
Insight on Infections in Diabetic Setting


Abstract
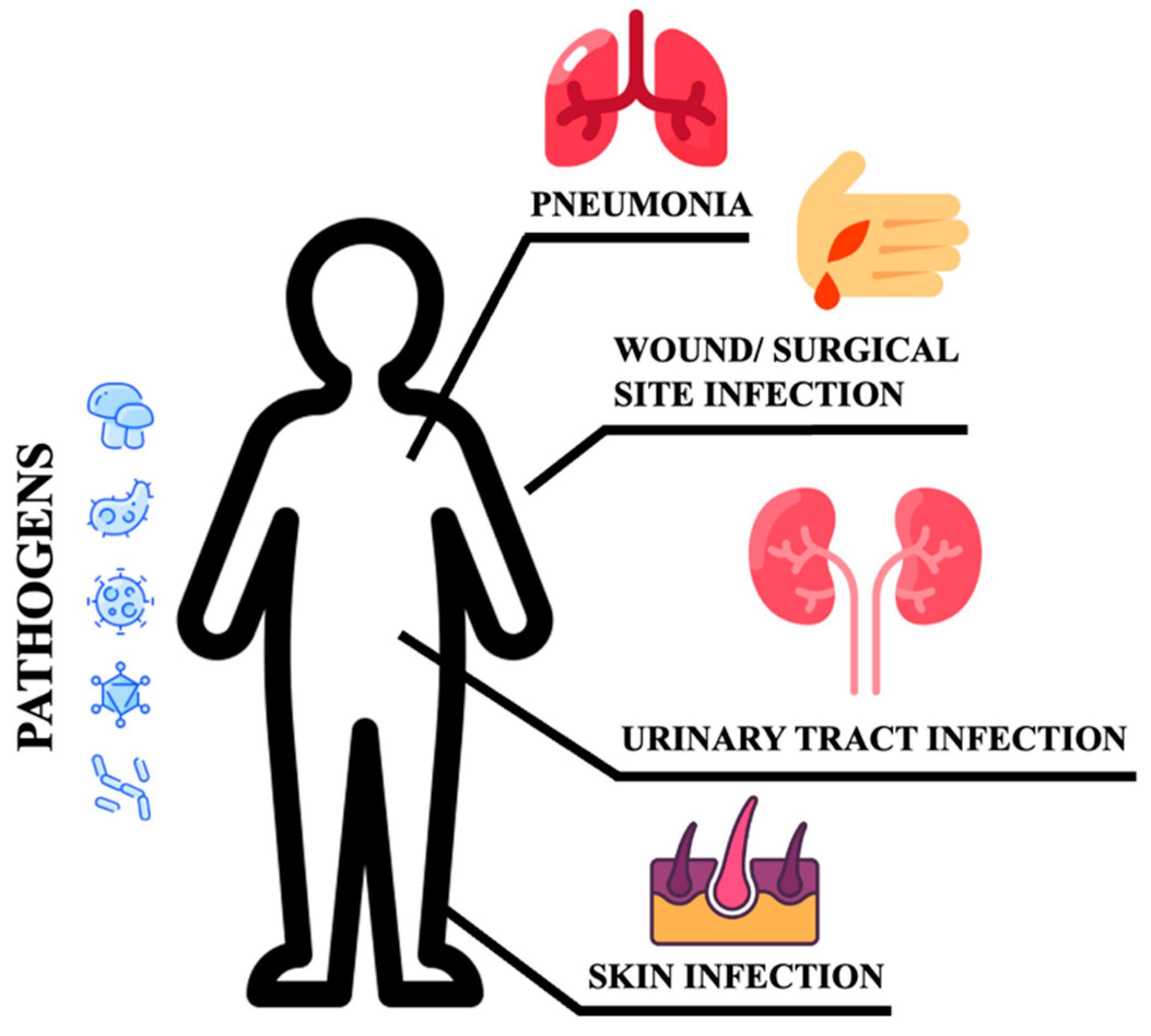
:1. Introduction
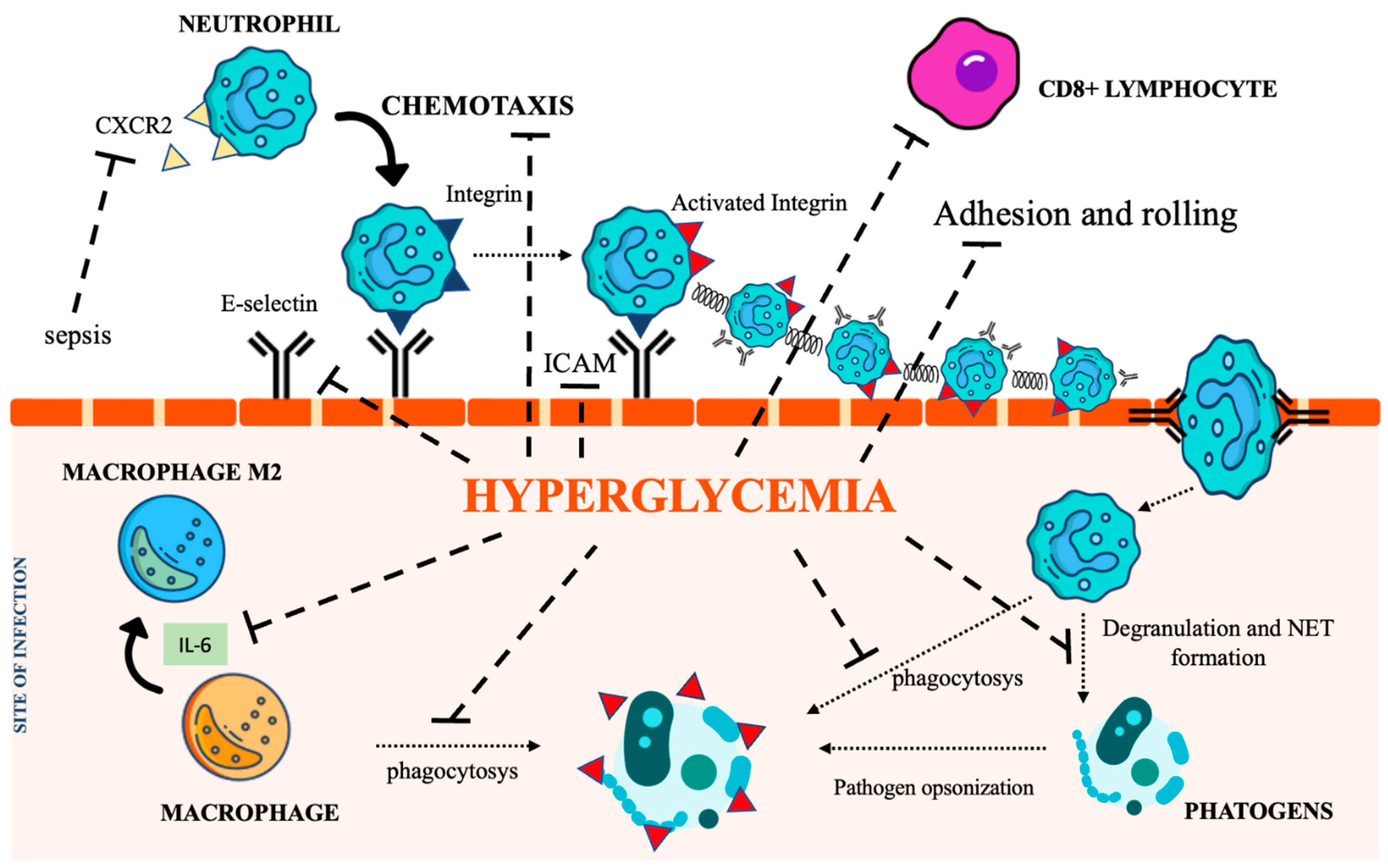
2. Immunity Impairment in DM
2.1. Neutrophils
2.2. Macrophages
2.3. Natural Killer Cells
2.4. Adaptive Immunity
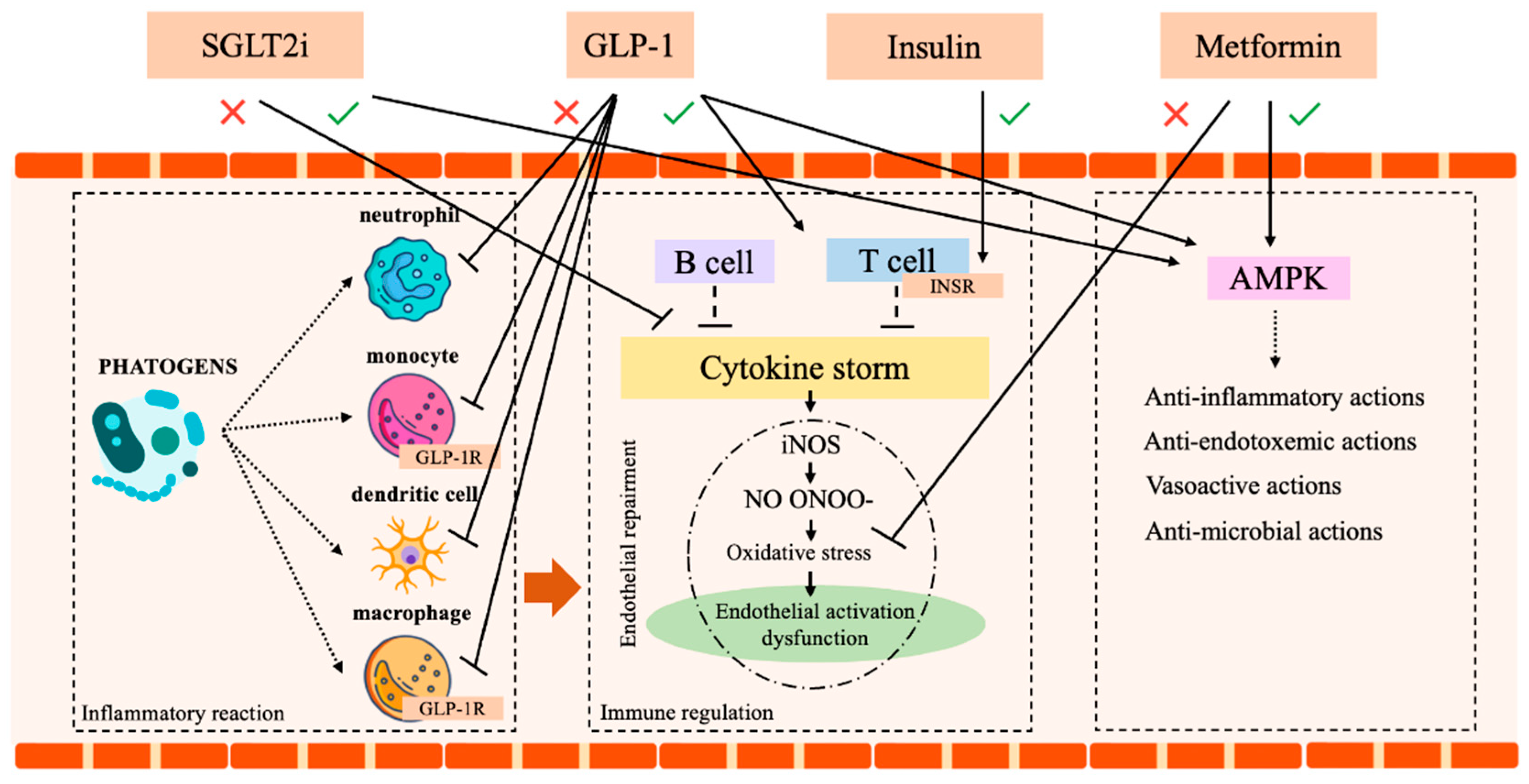
3. Treatment-Associated Infections
3.1. Metformin
3.2. Insulin
3.3. Glucagon-Like Peptide-1 Receptor Agonists (GLP-1) and Dipeptidyl Peptidase-4 Inhibitor (DPP4 Is)
3.4. SGLT2-Inhibitors (SGLT2i)
4. Diabetes and SARS-CoV-2 Infection
4.1. Diabetes and Increased Susceptibility to COVID-19 Infection
4.2. Antidiabetic Agents and SARS-CoV-2
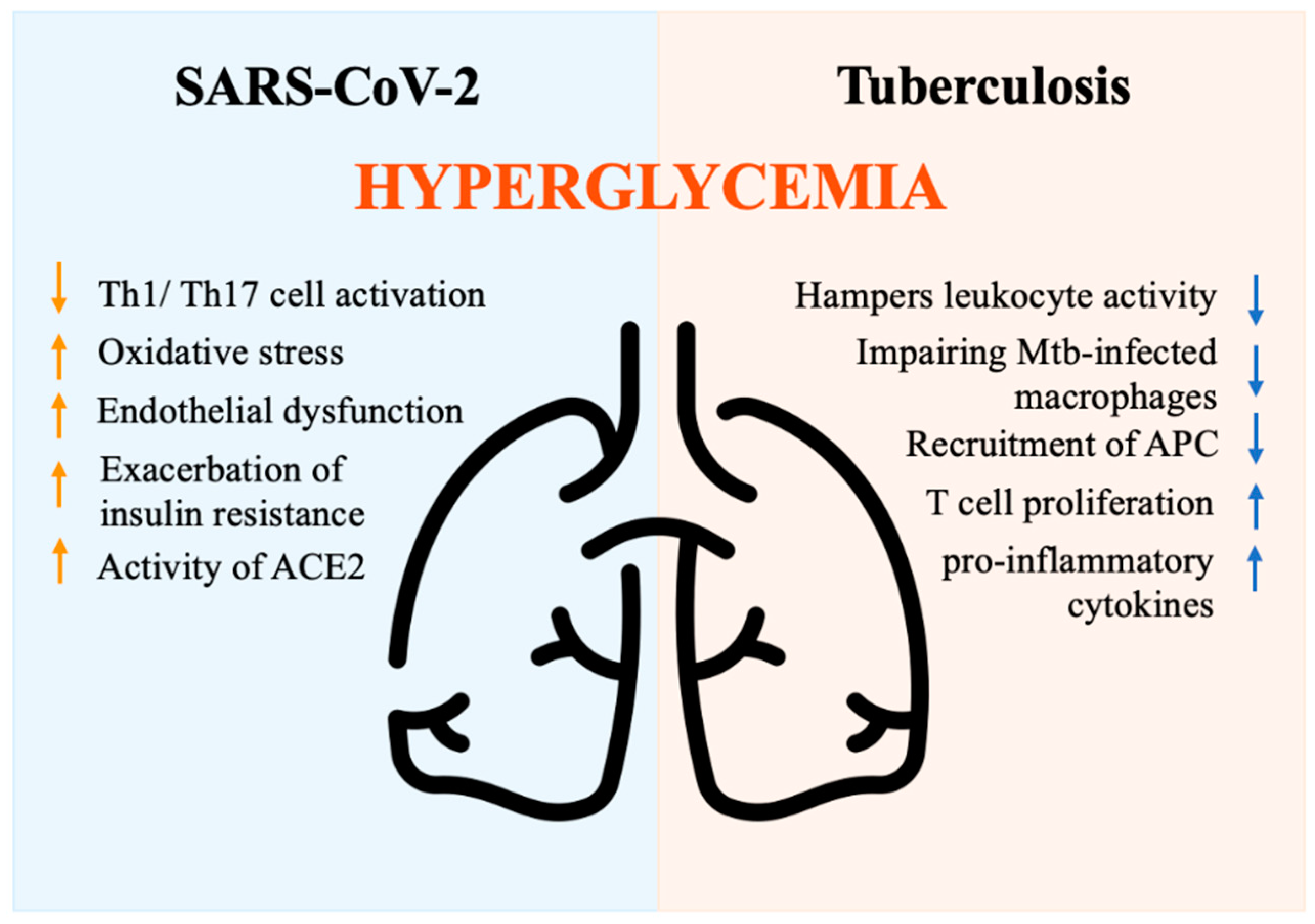
5. DM and Tuberculosis
5.1. Immune Mechanisms
5.2. Management of Tuberculosis in DM Patients
6. Conclusions and Future Perspective
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersmann, A.; Müller-Wieland, D.; Müller, U.A.; Landgraf, R.; Nauck, M.; Freckmann, G.; Heinemann, L.; Schleicher, E. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2019, 127, S1–S7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschner, P.; Basit, A.; Fawwad, A.; Guariguata, L.; James, S.; Karuranga, S.; Malanda, B.; Mbanya, J.C.; O’neill, S.; Ogle, G.; et al. IDF Guide for Diabetes Epidemiology Studies IDF Guide for Diabetes Epidemiology Studies i Acknowledgements Authors. Available online: https://diabetesatlas.org/idf-guide-for-epidemiology-studies/ (accessed on 28 January 2023).
- IDF Diabetes Atlas 10th Edition. Available online: www.diabetesatlas.org (accessed on 28 January 2023).
- Schuetz, P.; Castro, P.; Shapiro, N.I. Diabetes and Sepsis: Preclinical Findings and Clinical Relevance. Diabetes Care. 2011, 34, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erener, S. Diabetes, Infection Risk and COVID-19. Mol. Metab. 2020, 39, 101044. [Google Scholar] [CrossRef]
- Akinosoglou, K.; Kapsokosta, G.; Mouktaroudi, M.; Rovina, N.; Kaldis, V.; Stefos, A.; Kontogiorgi, M.; Giamarellos-Bourboulis, E.; Gogos, C. Diabetes on Sepsis Outcomes in Non-ICU Patients: A Cohort Study and Review of the Literature. J Diabetes Complicat. 2021, 35, 107765. [Google Scholar] [CrossRef]
- Jiang, L.; Cheng, M. Impact of Diabetes Mellitus on Outcomes of Patients with Sepsis: An Updated Systematic Review and Meta-Analysis. Diabetol. Metab. Syndr. 2022, 14, 1–17. [Google Scholar] [CrossRef]
- Costantini, E.; Carlin, M.; Porta, M.; Brizzi, M.F. Type 2 Diabetes Mellitus and Sepsis: State of the Art, Certainties and Missing Evidence. Acta Diabetol. 2021, 58, 1139–1151. [Google Scholar] [CrossRef]
- Akash, M.S.H.; Rehman, K.; Fiayyaz, F.; Sabir, S.; Khurshid, M. Diabetes-Associated Infections: Development of Antimicrobial Resistance and Possible Treatment Strategies. Arch. Microbiol. 2020, 202, 953–965. [Google Scholar] [CrossRef]
- Critchley, J.A.; Carey, I.M.; Harris, T.; DeWilde, S.; Hosking, F.J.; Cook, D.G. Glycemic Control and Risk of Infections among People with Type 1 or Type 2 Diabetes in a Large Primary Care Cohort Study. Diabetes Care 2018, 41, 2127–2135. [Google Scholar] [CrossRef] [Green Version]
- Burgess, J.L.; Wyant, W.A.; Abujamra, B.A.; Kirsner, R.S.; Jozic, I. Diabetic Wound-Healing Science. Medicina 2021, 57, 1072. [Google Scholar] [CrossRef]
- Shah, B.R.; Hux, J.E. Quantifying the Risk of Infectious Diseases for People with Diabetes. Available online: http://diabetesjournals.org/care/article-pdf/26/2/510/648543/dc0203000510.pdf (accessed on 28 January 2023).
- Toniolo, A.; Cassani, G.; Puggioni, A.; Rossi, A.; Colombo, A.; Onodera, T.; Ferrannini, E. The Diabetes Pandemic and Associated Infections: Suggestions for Clinical Microbiology. Rev. Res. Med. Microbiol. 2019, 30, 1–17. [Google Scholar] [CrossRef]
- Polk, C.; Sampson, M.M.; Roshdy, D.; Davidson, L.E. Skin and Soft Tissue Infections in Patients with Diabetes Mellitus. In Infectious Disease Clinics of North America; W.B. Saunders: Philadelphia, PA, USA, 2021; pp. 183–197. [Google Scholar] [CrossRef]
- Chowdhury, T.; Gousy, N.; Bellamkonda, A.; Dutta, J.; Zaman, C.F.; Zakia, U.B.; Tasha, T.; Dutta, P.; Deb Roy, P.; Gomez, A.M.; et al. Fournier’s Gangrene: A Coexistence or Consanguinity of SGLT-2 Inhibitor Therapy. Cureus 2022, 14, e27773. [Google Scholar] [CrossRef] [PubMed]
- Ellegård, L.; Prytz, M. Fournier’s Gangrene under SGLT-2 Inhibitor Therapy: A Literature Review and Case Report. Int. J. Surg. Case Rep. 2020, 77, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.L.; Zhu, Q.Q.; Chen, Y.H.; Li, X.L.; Chen, F.; Huang, J.A.; Xu, B. Cardiovascular Safety, Long-Term Noncardiovascular Safety, and Efficacy of Sodium-Glucose Cotransporter 2 Inhibitors in Patients with Type 2 Diabetes Mellitus: A Systemic Review and Meta-Analysis with Trial Sequential Analysis. J. Am. Heart Assoc. 2018, 7, e007165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamei, J.; Yamamoto, S. Complicated Urinary Tract Infections with Diabetes Mellitus. J. Infect. Chemother. 2021, 27, 1131–1136. [Google Scholar] [CrossRef]
- Nitzan, O.; Elias, M.; Chazan, B.; Saliba, W. Urinary Tract Infections in Patients with Type 2 Diabetes Mellitus: Review of Prevalence, Diagnosis, and Management. Diabetes Metab. Syndr. Obes. Targets Ther. 2015, 8, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Klekotka, R.B.; Mizgała, E.; Król, W. The Etiology of Lower Respiratory Tract Infections in People with Diabetes. Pneumonol. I Alergol. Pol. 2015, 83, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Knapp, S. Diabetes and Infection: Is There a Link?—A Mini-Review. Gerontology 2013, 59, 99–104. [Google Scholar] [CrossRef]
- Hua, J.; Huang, P.; Liao, H.; Lai, X.; Zheng, X. Prevalence and Clinical Significance of Occult Pulmonary Infection in Elderly Patients with Type 2 Diabetes Mellitus. Biomed. Res. Int. 2021, 2021, 3187388. [Google Scholar] [CrossRef]
- Jones, R.N. Microbial Etiologies of Hospital-Acquired Bacterial Pneumonia and Ventilator-Associated Bacterial Pneumonia. Clin. Infect. Dis. 2010, 51, S81–S87. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wang, R.; Di, X.; Liu, B.; Liu, Y. Different Microbiological and Clinical Aspects of Lower Respiratory Tract Infections between China and European/American Countries. J. Thorac. Dis. 2014, 6, 134–142. [Google Scholar] [CrossRef]
- Casqueiro, J.; Casqueiro, J.; Alves, C. Infections in Patients with Diabetes Mellitus: A Review of Pathogenesis. Indian J. Endocrinol. Metab. 2012, 16, 27. [Google Scholar] [CrossRef]
- Martin, E.T.; Kaye, K.S.; Knott, C.; Nguyen, H.; Santarossa, M.; Evans, R.; Bertran, E.; Jaber, L. Diabetes and Risk of Surgical Site Infection: A Systematic Review and Meta-Analysis. Infect. Control. Hosp. Epidemiol. 2016, 37, 88–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlos, D.; Spiller, F.; Souto, F.O.; Trevelin, S.C.; Borges, V.F.; de Freitas, A.; Alves-Filho, J.C.; Silva, J.S.; Ryffel, B.; Cunha, F.Q. Histamine H 2 Receptor Signaling in the Pathogenesis of Sepsis: Studies in a Murine Diabetes Model. J. Immunol. 2013, 191, 1373–1382. [Google Scholar] [CrossRef] [Green Version]
- Alba-Loureiro, T.C.; Munhoz, C.D.; Martins, J.O.; Cerchiaro, G.A.; Scavone, C.; Curi, R.; Sannomiya, P. Neutrophil Function and Metabolism in Individuals with Diabetes Mellitus. Volume 40. Available online: www.bjournal.com.br (accessed on 28 January 2023).
- Andersen, B.; Goldsmith, G.H.; Spagnuolo, P.J. Neutrophil Adhesive Dysfunction in Diabetes Mellitus: The Role of Cellular and Plasma Factors. J. Lab. Clin. Med. 1988, 111, 267–274. [Google Scholar]
- Delamaire, M.; Maugendre, D.; Moreno, M.; le Goff, M.C.; Allannic, H.; Genetet, B. Impaired Leucocyte Functions in Diabetic Patients. Diabet. Med. 1997, 14, 29–34. [Google Scholar] [CrossRef]
- Tater, D.; Tepaut, B.; Bercovici, J.P.; Youinou, P. Polymorphonuclear cell derangements in type i diabetes. Horm. Metab. Res. 1987, 19, 642–647. [Google Scholar] [CrossRef]
- Rios-Santos, F.; Alves-Filho, J.C.; Souto, F.O.; Spiller, F.; Freitas, A.; Lotufo, C.M.C.; Soares, M.B.P.; dos Santos, R.R.; Teixeira, M.M.; Cunha, F.D.Q. Down-Regulation of CXCR2 on Neutrophils in Severe Sepsis Is Mediated by Inducible Nitric Oxide Synthase-Derived Nitric Oxide. Am. J. Respir. Crit. Care Med. 2007, 175, 490–497. [Google Scholar] [CrossRef] [Green Version]
- Vieira, S.M.; Lemos, H.P.; Grespan, R.; Napimoga, M.H.; Dal-Secco, D.; Freitas, A.; Cunha, T.M.; Verri, W.A.; Souza, D.A.; Jamur, M.C.; et al. A Crucial Role for TNF-α in Mediating Neutrophil Influx Induced by Endogenously Generated or Exogenous Chemokines, KC/CXCL1 and LIX/CXCL5: RESEARCH PAPER. Br. J. Pharmacol. 2009, 158, 779–789. [Google Scholar] [CrossRef] [Green Version]
- Hair, P.S.; Echague, C.G.; Rohn, R.D.; Krishna, N.K.; Nyalwidhe, J.O.; Cunnion, K.M. Hyperglycemic Conditions Inhibit C3-Mediated Immunologic Control of Staphylococcus Aureus. J. Transl. Med. 2012, 10, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Chao, W.C.; Yen, C.L.; Wu, Y.H.; Chen, S.Y.; Hsieh, C.Y.; Chang, T.C.; Ou, H.Y.; Shieh, C.C. Increased Resistin May Suppress Reactive Oxygen Species Production and Inflammasome Activation in Type 2 Diabetic Patients with Pulmonary Tuberculosis Infection. Microbes Infect. 2015, 17, 195–204. [Google Scholar] [CrossRef]
- Shah, S.V.; Wallin, J.D.; Eilenj, S.D. Chemiluminescence and superoxide anion production by leukocytes from diabetic patients. J. Clin. Endocrinol. Metab. 1983, 57, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Stegenga, M.E.; van der Crabben, S.N.; Blümer, R.M.; Levi, M.; Meijers, J.C.; Serlie, M.J.; Tanck, M.W.; Sauerwein, H.P.; van der Poll, T. Hyperglycemia Enhances Coagulation and Reduces Neutrophil Degranulation, Whereas Hyperinsulinemia Inhibits Fibrinolysis during Human Endotoxemia. Blood J. Am. Soc. Hematol. 2008, 112, 82–89. [Google Scholar] [CrossRef]
- Joshi, M.B.; Lad, A.; Bharath Prasad, A.S.; Balakrishnan, A.; Ramachandra, L.; Satyamoorthy, K. High Glucose Modulates IL-6 Mediated Immune Homeostasis through Impeding Neutrophil Extracellular Trap Formation. FEBS Lett. 2013, 587, 2241–2246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Restrepo, B.I.; Twahirwa, M.; Rahbar, M.H.; Schlesinger, L.S. Phagocytosis via Complement or Fc-Gamma Receptors Is Compromised in Monocytes from Type 2 Diabetes Patients with Chronic Hyperglycemia. PLoS ONE 2014, 9, e92977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavlou, S.; Lindsay, J.; Ingram, R.; Xu, H.; Chen, M. Sustained High Glucose Exposure Sensitizes Macrophage Responses to Cytokine Stimuli but Reduces Their Phagocytic Activity. BMC Immunol. 2018, 19, 24. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.F.; Zhang, H.J.; Hu, Q.X.; Liu, X.Y.; Wang, Z.Q.; Fan, J.Y.; Zhan, M.; Chen, F.L. Altered Polarization, Morphology, and Impaired Innate Immunity Germane to Resident Peritoneal Macrophages in Mice with Long-Term Type 2 Diabetes. J. Biomed. Biotechnol. 2012, 2012, 867023. [Google Scholar] [CrossRef] [Green Version]
- Mauer, J.; Chaurasia, B.; Goldau, J.; Vogt, M.C.; Ruud, J.; Nguyen, K.D.; Theurich, S.; Hausen, A.C.; Schmitz, J.; Brönneke, H.S.; et al. Signaling by IL-6 Promotes Alternative Activation of Macrophages to Limit Endotoxemia and Obesity-Associated Resistance to Insulin. Nat. Immunol. 2014, 15, 423–430. [Google Scholar] [CrossRef]
- Zhang, K.; Kaufman, R.J. From Endoplasmic-Reticulum Stress to the Inflammatory Response. Nature 2008, 454, 455–462. [Google Scholar] [CrossRef] [Green Version]
- Whalen, M.M. Inhibition of Human Natural Killer Cell Function in Vitro by Glucose Concentrations Seen in Poorly Controlled Diabetes. Cell. Physiol. Biochem. 1997, 7, 53–60. [Google Scholar] [CrossRef]
- Kim, J.H.; Park, K.; Lee, S.B.; Kang, S.; Park, J.S.; Ahn, C.W.; Nam, J.S. Relationship between Natural Killer Cell Activity and Glucose Control in Patients with Type 2 Diabetes and Prediabetes. J. Diabetes Investig. 2019, 10, 1223–1228. [Google Scholar] [CrossRef] [Green Version]
- Kumar, M.; Roe, K.; Nerurkar, P.V.; Orillo, B.; Thompson, K.S.; Verma, S.; Nerurkar, V.R. Reduced Immune Cell Infiltration and Increased Pro-Inflammatory Mediators in the Brain of Type 2 Diabetic Mouse Model Infected with West Nile Virus. 2014. Available online: http://www.jneuroinflammation.com/content/11/1/80 (accessed on 28 January 2023).
- Lapolla, A.; Tonani, R.; Fedele, D.; Garbeglio, M.; Senesi, A.; Seraglia, R.; Favretto, D.; Traldi, P. Non-Enzymatic Glycation of IgG: An In Vivo Study. Horm. Metab. Res. 2002, 34, 260–264. [Google Scholar] [CrossRef]
- van Vught, L.A.; Scicluna, B.P.; Hoogendijk, A.J.; Wiewel, M.A.; Klein Klouwenberg, P.M.C.; Cremer, O.L.; Horn, J.; Nürnberg, P.; Bonten, M.M.J.; Schultz, M.J.; et al. Association of Diabetes and Diabetes Treatment with the Host Response in Critically Ill Sepsis Patients. Crit. Care 2016, 20, 252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiqiang, Z.; Yifen, Z.; Ziqi, R.; Wei, H.; Xiaoyun, F. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021, Interpretation and Expectation. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2021, 33, 1159–1164. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Zeng, F.; Luo, X.; Lei, Y.; Li, J.; Lu, S.; Huang, X.; Lan, Y.; Liu, R. GLP-1 Receptor: A New Target for Sepsis. Front. Pharmacol. 2021, 12, 706908. [Google Scholar] [CrossRef]
- Lu, Z.; Tao, G.; Sun, X.; Zhang, Y.; Jiang, M.; Liu, Y.; Ling, M.; Zhang, J.; Xiao, W.; Hua, T.; et al. Association of Blood Glucose Level and Glycemic Variability with Mortality in Sepsis Patients During ICU Hospitalization. Front. Public Health 2022, 10, 857368. [Google Scholar] [CrossRef]
- Bharath, L.P.; Nikolajczyk, B.S. The Intersection of Metformin and Inflammation. Am. J. Physiol. Cell Physiol. 2021, 320, C873–C879. [Google Scholar] [CrossRef]
- Gómez, H.; del Rio-Pertuz, G.; Priyanka, P.; Manrique-Caballero, C.L.; Chang, C.C.H.; Wang, S.; Liu, Q.; Zuckerbraun, B.S.; Murugan, R.; Angus, D.C.; et al. Association of Metformin Use During Hospitalization and Mortality in Critically Ill Adults with Type 2 Diabetes Mellitus and Sepsis. Crit. Care Med. 2022, 50, 935–944. [Google Scholar] [CrossRef]
- Montoya, C. Clarification of Key Points in a Study Evaluating the Association of Metformin and Mortality in Patients with Sepsis and Type 2 Diabetes. Crit. Care Med. 2023, 51, E60. [Google Scholar] [CrossRef]
- Yen, F.S.; Wei, J.C.C.; Shih, Y.H.; Pan, W.L.; Hsu, C.C.; Hwu, C.M. Role of Metformin in Morbidity and Mortality Associated with Urinary Tract Infections in Patients with Type 2 Diabetes. J. Pers. Med. 2022, 12, 702. [Google Scholar] [CrossRef]
- Li, Y.; Zhao, H.; Guo, Y.; Duan, Y.; Guo, Y.; Ding, X. Association of Preadmission Metformin Use and Prognosis in Patients with Sepsis and Diabetes Mellitus: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 811776. [Google Scholar] [CrossRef]
- Masadeh, M.M.; Alzoubi, K.H.; Masadeh, M.M.; Aburashed, Z.O. Metformin as a Potential Adjuvant Antimicrobial Agent against Multidrug Resistant Bacteria. Clin. Pharmacol. 2021, 13, 83–90. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- van Niekerk, G.; Davis, T.; Engelbrecht, A.M. Hyperglycaemia in Critically Ill Patients: The Immune System’s Sweet Tooth. Crit. Care 2017, 21, 202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, N.; Curtis, J.C.; Plotkin, B.J. Insulin Regulation of Escherichia Coli Abiotic Biofilm Formation: Effect of Nutrients and Growth Conditions. Antibiotics 2021, 10, 1349. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Zhang, Z.; Luo, J.; Kong, J.; Ding, Y.; Chen, Y.; Wang, K. Insulin Treatment Enhances Pseudomonas Aeruginosa Biofilm Formation by Increasing Intracellular Cyclic Di-GMP Levels, Leading to Chronic Wound Infection and Delayed Wound Healing. 2019, Volume 11. Available online: www.ajtr.org (accessed on 28 January 2023).
- Tsai, S.; Clemente-Casares, X.; Zhou, A.C.; Lei, H.; Ahn, J.J.; Chan, Y.T.; Choi, O.; Luck, H.; Woo, M.; Dunn, S.E.; et al. Insulin Receptor-Mediated Stimulation Boosts T Cell Immunity during Inflammation and Infection. Cell Metab. 2018, 28, 922–934.e4. [Google Scholar] [CrossRef] [Green Version]
- Steven, S.; Hausding, M.; Kröller-Schön, S.; Mader, M.; Mikhed, Y.; Stamm, P.; Zinßius, E.; Pfeffer, A.; Welschof, P.; Agdauletova, S.; et al. Gliptin and GLP-1 Analog Treatment Improves Survival and Vascular Inflammation/Dysfunction in Animals with Lipopolysaccharide-induced Endotoxemia. Basic Res. Cardiol. 2015, 110, 1–14. [Google Scholar] [CrossRef]
- Helmstädter, J.; Keppeler, K.; Aust, F.; Küster, L.; Frenis, K.; Filippou, K.; Vujacic-Mirski, K.; Tsohataridis, S.; Kalinovic, S.; Kröller-Schön, S.; et al. GLP-1 Analog Liraglutide Improves Vascular Function in Polymicrobial Sepsis by Reduction of Oxidative Stress and Inflammation. Antioxidants 2021, 10, 1175. [Google Scholar] [CrossRef]
- Steven, S.; Jurk, K.; Kopp, M.; Kröller-Schön, S.; Mikhed, Y.; Schwierczek, K.; Roohani, S.; Kashani, F.; Oelze, M.; Klein, T.; et al. Themed Section: Redox Biology and Oxidative Stress in Health and Disease. Br. J. Pharm. 2017, 174, 1620. [Google Scholar] [CrossRef] [Green Version]
- Kröller-Schön, S.; Knorr, M.; Hausding, M.; Oelze, M.; Schuff, A.; Schell, R.; Sudowe, S.; Scholz, A.; Daub, S.; Karbach, S.; et al. Glucose-Independent Improvement of Vascular Dysfunction in Experimental Sepsis by Dipeptidyl-Peptidase 4 Inhibition. Cardiovasc. Res. 2012, 96, 140–149. [Google Scholar] [CrossRef] [Green Version]
- al Zoubi, S.; Chen, J.; Murphy, C.; Martin, L.; Chiazza, F.; Collotta, D.; Yaqoob, M.M.; Collino, M.; Thiemermann, C. Linagliptin Attenuates the Cardiac Dysfunction Associated with Experimental Sepsis in Mice with Pre-Existing Type 2 Diabetes by Inhibiting NF-ΚB. Front. Immunol. 2018, 9, 2996. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.C.; Wang, X.Y.; Liu, C.T.; Chou, R.H.; Chen, Z.B.; Huang, P.H.; Lin, S.J. The Dipeptidyl Peptidase-4 Inhibitor Linagliptin Ameliorates Endothelial Inflammation and Microvascular Thrombosis in a Sepsis Mouse Model. Int. J. Mol. Sci. 2022, 23, 3065. [Google Scholar] [CrossRef] [PubMed]
- Brakenridge, S.C.; Moore, F.A.; Mercier, N.R.; Cox, M.; Wu, Q.; Moldawer, L.L.; Mohr, A.M.; Efron, P.A.; Smith, R.S. Persistently Elevated Glucagon-Like Peptide-1 Levels among Critically Ill Surgical Patients after Sepsis and Development of Chronic Critical Illness and Dismal Long-Term Outcomes. J. Am. Coll. Surg. 2019, 229, 58–67.e1. [Google Scholar] [CrossRef] [PubMed]
- Perl, S.H.; Bloch, O.; Zelnic-Yuval, D.; Love, I.; Mendel-Cohen, L.; Flor, H.; Rapoport, M.J. Sepsis-Induced Activation of Endogenous GLP-1 System Is Enhanced in Type 2 Diabetes. Diabetes/Metab. Res. Rev. 2018, 34, e2982. [Google Scholar] [CrossRef] [PubMed]
- Bloch, O.; Perl, S.H.; Lazarovitch, T.; Zelnik-Yovel, D.; Love, I.; Mendel-Cohen, L.; Goltsman, G.; Flor, H.; Rapoport, M.J. Hyper-Activation of Endogenous GLP-1 System to Gram-Negative Sepsis Is Associated with Early Innate Immune Response and Modulated by Diabetes. Shock 2021, 55, 796–805. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Bailey, C.J.; Day, C.; Bellary, S. Renal Protection with SGLT2 Inhibitors: Effects in Acute and Chronic Kidney Disease. Curr. Diabetes Rep. 2022, 22, 39–52. [Google Scholar] [CrossRef]
- Chen, G.; Li, X.; Cui, Q.; Zhou, Y.; Zhao, B.; Mei, D.; Xuemei. Acute Kidney Injury Following SGLT2 Inhibitors among Diabetic Patients: A Pharmacovigilance Study. Int. Urol. Nephrol. 2022, 54, 2949–2957. [Google Scholar] [CrossRef]
- Donnan, J.R.; Grandy, C.A.; Chibrikov, E.; Marra, C.A.; Aubrey-Bassler, K.; Johnston, K.; Swab, M.; Hache, J.; Curnew, D.; Nguyen, H.; et al. Comparative Safety of the Sodium Glucose Co-Transporter 2 (SGLT2) Inhibitors: A Systematic Review and Meta-Analysis. BMJ Open 2019, 9, e022577. [Google Scholar] [CrossRef] [Green Version]
- Dave, C.V.; Schneeweiss, S.; Kim, D.; Fralick, M.; Tong, A.; Patorno, E. Sodium-Glucose Cotransporter-2 Inhibitors and the Risk for Severe Urinary Tract Infections. Ann. Intern. Med. 2019, 171, 248–256. [Google Scholar] [CrossRef]
- Wiegley, N.; So, P.N. Sodium-Glucose Cotransporter 2 Inhibitors and Urinary Tract Infection: Is There Room for Real Concern? Kidney360 2022, 3, 1991–1993. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Liu, J.; Zhong, L.; Li, S.; Zhou, L.; Zhang, Q.; Li, M.; Xiao, X. The Effect of Sodium-Glucose Cotransporter 2 Inhibitors on Biomarkers of Inflammation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Pharm. 2022, 13, 4779. [Google Scholar] [CrossRef] [PubMed]
- Kıngır, Z.B.; Özdemir Kumra, Z.N.; Çam, M.E.; Çilingir, Ö.T.; Şekerler, T.; Ercan, F.; Özakpınar, Ö.B.; Özsavcı, D.; Sancar, M.; Okuyan, B. Effects of Dapagliflozin in Experimental Sepsis Model in Rats. Ulus. Travma Ve Acil Cerrahi Derg. 2019, 25, 213–221. [Google Scholar] [CrossRef]
- Chi, P.J.; Lee, C.J.; Hsieh, Y.J.; Lu, C.W.; Hsu, B.G. Dapagliflozin Ameliorates Lipopolysaccharide Related Acute Kidney Injury in Mice with Streptozotocin-Induced Diabetes Mellitus. Int. J. Med. Sci. 2022, 19, 729–739. [Google Scholar] [CrossRef] [PubMed]
- Maayah, Z.H.; Ferdaoussi, M.; Takahara, S.; Soni, S.; Dyck, J.R.B. Empagliflozin Suppresses Inflammation and Protects against Acute Septic Renal Injury. Inflammopharmacology 2021, 29, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-L.; Tse, Y.-K.; Chandramouli, C.; Hon, N.W.-L.; Cheung, C.-L.; Lam, L.-Y.; Wu, M.; Huang, J.-Y.; Yu, S.-Y.; Leung, K.-L.; et al. Sodium-Glucose Cotransporter 2 Inhibitors and the Risk of Pneumonia and Septic Shock. J. Clin. Endocrinol. Metab. 2022, 107, 3442–3451. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Organization. 2023. WHO Coronavirus (COVID-19) Dashboard. Available online: https://Covid19.Who.Int/ (accessed on 28 January 2023).
- Wang, B.; Li, R.; Lu, Z. Does Comorbidity Increase the Risk of Patients with COVID-19- Evidence from Meta-Analysis. Aging 2020, 12, 6049–6057. [Google Scholar] [CrossRef]
- Pranata, R.; Henrina, J.; Raffaello, W.M.; Lawrensia, S.; Huang, I. Diabetes and COVID-19: The Past, the Present, and the Future. In Metabolism: Clinical and Experimental; W.B. Saunders: Philadelphia, PA, USA, 2021. [Google Scholar] [CrossRef]
- McGurnaghan, S.J.; Weir, A.; Bishop, J.; Kennedy, S.; Blackbourn, L.A.K.; McAllister, D.A.; Hutchinson, S.; Caparrotta, T.M.; Mellor, J.; Jeyam, A.; et al. Risks of and Risk Factors for COVID-19 Disease in People with Diabetes: A Cohort Study of the Total Population of Scotland. Lancet Diabetes Endocrinol. 2021, 9, 82–93. [Google Scholar] [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and Diabetes Mellitus: From Pathophysiology to Clinical Management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef]
- Singh, A.K.; Khunti, K. COVID-19 and diabetes. Annu. Rev. Med. 2022, 73, 129–147. [Google Scholar] [CrossRef]
- Khunti, K.; del Prato, S.; Mathieu, C.; Kahn, S.E.; Gabbay, R.A.; Buse, J.B. COVID-19, Hyperglycemia, and New-Onset Diabetes. Diabetes Care 2021, 44, 2645–2655. [Google Scholar] [CrossRef] [PubMed]
- Jafar, N.; Edriss, H.; Nugent, K. The Effect of Short-Term Hyperglycemia on the Innate Immune System. Am. J. Med. Sci. 2016, 351, 201–211. [Google Scholar] [CrossRef]
- Coppelli, A.; Giannarelli, R.; Aragona, M.; Penno, G.; Falcone, M.; Tiseo, G.; Ghiadoni, L.; Barbieri, G.; Monzani, F.; Virdis, A.; et al. Hyperglycemia at Hospital Admission Is Associated with Severity of the Prognosis in Patients Hospitalized for COVID-19: The Pisa COVID-19 Study. Diabetes Care 2020, 43, 2345–2348. [Google Scholar] [CrossRef]
- Brooks, D.; Schulman-Rosenbaum, R.; Griff, M.; Lester, J.; Low Wang, C.C. Glucocorticoid-Induced Hyperglycemia Including Dexamethasone-Associated Hyperglycemia in COVID-19 Infection: A Systematic Review. Endocr. Pract. 2022, 28, 1166–1177. [Google Scholar] [CrossRef]
- Chai, C.; Chen, K.; Li, S.; Cheng, G.; Wang, W.; Wang, H.; Wei, D.; Peng, C.; Sun, Q.; Tang, Z. Effect of Elevated Fasting Blood Glucose Level on the 1-Year Mortality and Sequelae in Hospitalized COVID-19 Patients: A Bidirectional Cohort Study. J. Med. Virol. 2022, 94, 3240–3250. [Google Scholar] [CrossRef]
- Mifsud, S.; Schembri, E.L.; Gruppetta, M. Stress-Induced Hyperglycaemia. Br. J. Hosp. Med. 2018, 79, 634–639. [Google Scholar] [CrossRef]
- Kolahian, S.; Leiss, V.; Nürnberg, B. Diabetic Lung Disease: Fact or Fiction? In Endocrine and Metabolic Disorders; Springer: New York, NY, USA, 2019; pp. 303–319. [Google Scholar] [CrossRef]
- Cherney, D.Z.I.; Xiao, F.; Zimpelmann, J.; Har, R.L.H.; Lai, V.; Scholey, J.W.; Reich, H.N.; Burns, K.D. Urinary ACE2 in Healthy Adults and Patients with Uncomplicated Type 1 Diabetes. Can. J. Physiol. Pharmacol. 2014, 92, 703–706. [Google Scholar] [CrossRef]
- Rao, S.; Lau, A.; So, H.C. Exploring Diseases/Traits and Blood Proteins Causally Related to Expression of ACE2, the Putative Receptor of SARS-CoV-2: A Mendelian Randomization Analysis Highlights Tentative Relevance of Diabetes-Related Traits. Diabetes Care 2020, 43, 1416–1426. [Google Scholar] [CrossRef]
- Pugliese, G.; Vitale, M.; Resi, V.; Orsi, E. Is Diabetes Mellitus a Risk Factor for COronaVIrus Disease 19 (COVID-19)? Acta Diabetol. 2020, 57, 1275–1285. [Google Scholar] [CrossRef]
- Pal, R.; Bhansali, A. COVID-19, Diabetes Mellitus and ACE2: The Conundrum. Diabetes Res. Clin. Pract. 2020, 162, 108132. [Google Scholar] [CrossRef]
- South, A.M.; Tomlinson, L.; Edmonston, D.; Hiremath, S.; Sparks, M.A. Controversies of Renin–Angiotensin System Inhibition during the COVID-19 Pandemic. Nat. Rev. Nephrol. 2020, 16, 305–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelle, M.C.; Zaffina, I.; Provenzano, M.; Moirano, G.; Arturi, F. COVID-19 and Diabetes—Two Giants Colliding: From Pathophysiology to Management. Front. Endocrinol. 2022, 13, 974540. [Google Scholar] [CrossRef] [PubMed]
- Xia, C.; Rao, X.; Zhong, J. Role of T Lymphocytes in Type 2 Diabetes and Diabetes-Associated Inflammation. J. Diabetes Res. 2017, 2017, 6494795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scheen, A.J.; Marre, M.; Thivolet, C. Prognostic Factors in Patients with Diabetes Hospitalized for COVID-19: Findings from the CORONADO Study and Other Recent Reports. Diabetes Metab. 2020, 46, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Merino, J.; Joshi, A.D.; Nguyen, L.H.; Leeming, E.R.; Mazidi, M.; Drew, D.A.; Gibson, R.; Graham, M.S.; Lo, C.H.; Capdevila, J.; et al. Diet Quality and Risk and Severity of COVID-19: A Prospective Cohort Study. Gut 2021, 70, 2096–2104. [Google Scholar] [CrossRef]
- Li, Y.; Yang, X.; Yan, P.; Sun, T.; Zeng, Z.; Li, S. Metformin in Patients with COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 704666. [Google Scholar] [CrossRef]
- Scheen, A.J. Metformin and COVID-19: From Cellular Mechanisms to Reduced Mortality. Diabetes Metab. 2020, 46, 423–426. [Google Scholar] [CrossRef]
- Ursini, F.; Ciaffi, J.; Landini, M.P.; Meliconi, R. COVID-19 and Diabetes: Is Metformin a Friend or Foe? Diabetes Res. Clin. Pract. 2020, 164, 108167. [Google Scholar] [CrossRef]
- Narayanan, N.; Naik, D.; Sahoo, J.; Kamalanathan, S. Dipeptidyl Peptidase 4 Inhibitors in COVID-19: Beyond Glycemic Control. World J. Virol. 2022, 11, 399–410. [Google Scholar] [CrossRef]
- Nassar, M.; Abosheaishaa, H.; Singh, A.K.; Misra, A.; Bloomgarden, Z. Noninsulin-Based Antihyperglycemic Medications in Patients with Diabetes and COVID-19: A Systematic Review and Meta-Analysis. J. Diabetes 2023. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Dalan, R.; Hopkins, D.; Mingrone, G.; Boehm, B.O. Endocrine and Metabolic Link to Coronavirus Infection. Nat. Rev. Endocrinol. 2020, 16, 297–298. [Google Scholar] [CrossRef] [Green Version]
- Hariyanto, T.I.; Intan, D.; Hananto, J.E.; Putri, C.; Kurniawan, A. Pre-Admission Glucagon-like Peptide-1 Receptor Agonist (GLP-1RA) and Mortality from Coronavirus Disease 2019 (COVID-19): A Systematic Review, Meta-Analysis, and Meta-Regression. Diabetes Res. Clin. Pract. 2021, 179, 109031. [Google Scholar] [CrossRef]
- Nyland, J.E.; Raja-Khan, N.T.; Bettermann, K.; Haouzi, P.A.; Leslie, D.L.; Kraschnewski, J.L.; Parent, L.J.; Grigson, P.S. Diabetes, Drug Treatment, and Mortality in COVID-19: A Multinational Retrospective Cohort Study. Diabetes 2021, 70, 2903–2916. [Google Scholar] [CrossRef]
- Popovic, D.S.; Papanas, N.; Pantea Stoian, A.; Rizvi, A.A.; Janez, A.; Rizzo, M. Use of Novel Antidiabetic Agents in Patients with Type 2 Diabetes and COVID-19: A Critical Review. Diabetes Ther. 2021, 12, 3037–3054. [Google Scholar] [CrossRef]
- Bielka, W.; Przezak, A.; Pawlik, A. Therapy of Type 2 Diabetes in Patients with SARS-CoV-2 Infection. Int. J. Mol. Sci. 2021, 22, 7605. [Google Scholar] [CrossRef]
- Drucker, D.J. Coronavirus Infections and Type 2 Diabetes-Shared Pathways with Therapeutic Implications. Endocr. Rev. 2021, 41, 457–470. [Google Scholar] [CrossRef]
- Roca-Ho, H.; Riera, M.; Palau, V.; Pascual, J.; Soler, M.J. Characterization of ACE and ACE2 Expression within Different Organs of the NOD Mouse. Int. J. Mol. Sci. 2017, 18, 563. [Google Scholar] [CrossRef] [Green Version]
- Ricchio, M.; Tassone, B.; Pelle, M.C.; Mazzitelli, M.; Serapide, F.; Fusco, P.; Lionello, R.; Cancelliere, A.; Procopio, G.; Lio, E.; et al. Characteristics, Management, and Outcomes of Elderly Patients with Diabetes in a COVID-19 Unit: Lessons Learned from a Pilot Study. Medicina 2021, 57, 341. [Google Scholar] [CrossRef]
- Global Tuberculosis ReporT 2022. 2022. Available online: http://apps.who.int/bookorders (accessed on 28 January 2023).
- Mendenhall, E.; Kohrt, B.A.; Norris, S.A.; Ndetei, D.; Prabhakaran, D. Non-Communicable Disease Syndemics: Poverty, Depression, and Diabetes among Low-Income Populations. Lancet 2017, 389, 951–963. [Google Scholar] [CrossRef] [Green Version]
- Gakidou, E.; Mallinger, L.; Abbott-Klafter, J.; Guerrero, R.; Villalpando, S.; Ridaura, R.L.; Aekplakorn, W.; Naghavi, M.; Lim, S.; Lozano, R.; et al. Management of Diabetes and Associated Cardiovascular Risk Factors in Seven Countries: A Comparison of Data from National Health Examination Surveys. Bull. World Health Organ. 2011, 89, 172–183. [Google Scholar] [CrossRef]
- Riza, A.L.; Pearson, F.; Ugarte-Gil, C.; Alisjahbana, B.; van de Vijver, S.; Panduru, N.M.; Hill, P.C.; Ruslami, R.; Moore, D.; Aarnoutse, R.; et al. Clinical Management of Concurrent Diabetes and Tuberculosis and the Implications for Patient Services. Lancet Diabetes Endocrinol. 2014, 2, 740–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, C.Y.; Murray, M.B. Diabetes Mellitus Increases the Risk of Active Tuberculosis: A Systematic Review of 13 Observational Studies. PLoS Med. 2008, 5, 1091–1101. [Google Scholar] [CrossRef]
- Baker, M.A.; Harries, A.D.; Jeon, C.Y.; Hart, J.E.; Kapur, A.; Lönnroth, K.; Ottmani, S.E.; Goonesekera, S.D.; Murray, M.B. The Impact of Diabetes on Tuberculosis Treatment Outcomes: A Systematic Review. BMC Med. 2011, 9, 81. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Corona, M.E.; Cruz-Hervert, L.P.; García-García, L.; Ferreyra-Reyes, L.; Delgado-Sánchez, G.; Bobadilla-Del-Valle, M.; Canizales-Quintero, S.; Ferreira-Guerrero, E.; Báez-Saldaña, R.; Téllez-Vázquez, N.; et al. Association of Diabetes and Tuberculosis: Impact on Treatment and Post-Treatment Outcomes. Thorax 2013, 68, 214–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huangfu, P.; Ugarte-Gil, C.; Golub, J.; Pearson, F.; Critchley, J. The Effects of Diabetes on Tuberculosis Treatment Outcomes: An Updated Systematic Review and Meta-Analysis. Int. J. Tuberc. Lung Dis. 2019, 23, 783–796. [Google Scholar] [CrossRef] [PubMed]
- Tegegne, B.S.; Mengesha, M.M.; Teferra, A.A.; Awoke, M.A.; Habtewold, T.D. Association between Diabetes Mellitus and Multi-Drug-Resistant Tuberculosis: Evidence from a Systematic Review and Meta-Analysis 11 Medical and Health Sciences 1117 Public Health and Health Services. Syst. Rev. 2018, 7, 161. [Google Scholar] [CrossRef] [Green Version]
- Martinez, N.; Kornfeld, H. Diabetes and Immunity to Tuberculosis. In European Journal of Immunology; Wiley-VCH: Weinheim, Germany, 2014; pp. 617–626. [Google Scholar] [CrossRef] [Green Version]
- Vallerskog, T.; Martens, G.W.; Kornfeld, H. Diabetic Mice Display a Delayed Adaptive Immune Response to Mycobacterium Tuberculosis. J. Immunol. 2010, 184, 6275–6282. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.P.; Sridhar, R.; Banurekha, V.V.; Jawahar, M.S.; Nutman, T.B.; Babu, S. Expansion of Pathogen-Specific T-Helper 1 and T-Helper 17 Cells in Pulmonary Tuberculosis with Coincident Type 2 Diabetes Mellitus. J. Infect. Dis. 2013, 208, 739–748. [Google Scholar] [CrossRef] [Green Version]
- Martinez, N.; Vallerskog, T.; West, K.; Nunes-Alves, C.; Lee, J.; Martens, G.W.; Behar, S.M.; Kornfeld, H. Chromatin Decondensation and T Cell Hyperresponsiveness in Diabetes-Associated Hyperglycemia. J. Immunol. 2014, 193, 4457–4468. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.P.; Sridhar, R.; Banurekha, V.V.; Jawahar, M.S.; Fay, M.P.; Nutman, T.B.; Babu, S. Type 2 Diabetes Mellitus Coincident with Pulmonary Tuberculosis Is Associated with Heightened Systemic Type 1, Type 17, and Other Proinflammatory Cytokines. Ann. Am. Thorac. Soc. 2013, 10, 441–449. [Google Scholar] [CrossRef] [Green Version]
- Podell, B.K.; Ackart, D.F.; Obregon-Henao, A.; Eck, S.P.; Henao-Tamayo, M.; Richardson, M.; Orme, I.M.; Ordway, D.J.; Basaraba, R.J. Increased Severity of Tuberculosis in Guinea Pigs with Type 2 Diabetes: A Model of Diabetes-Tuberculosis Comorbidity. Am. J. Pathol. 2014, 184, 1104–1118. [Google Scholar] [CrossRef] [Green Version]
- Martens, G.W.; Arikan, M.C.; Lee, J.; Ren, F.; Greiner, D.; Kornfeld, H. Tuberculosis Susceptibility of Diabetic Mice. Am. J. Respir. Cell Mol. Biol. 2007, 37, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Jeon, C.Y.; Harries, A.D.; Baker, M.A.; Hart, J.E.; Kapur, A.; Lönnroth, K.; Ottmani, S.E.; Goonesekera, S.; Murray, M.B. Bi-Directional Screening for Tuberculosis and Diabetes: A Systematic Review. Trop. Med. Int. Health 2010, 15, 1300–1314. [Google Scholar] [CrossRef]
- Kumar, A.; Gupta, D.; Nagaraja, S.B.; Nair, A.; Satyanarayana, S.; Kumar, A.M.V.; Chadha, S.S.; Wilson, N.; Sharma, S.K.; Soneja, M.; et al. Screening of Patients with Diabetes Mellitus for Tuberculosis in India. Trop. Med. Int. Health 2013, 18, 646–654. [Google Scholar] [CrossRef]
- Lin, Y.; Li, L.; Mi, F.; Du, J.; Dong, Y.; Li, Z.; Qi, W.; Zhao, X.; Cui, Y.; Hou, F.; et al. Screening Patients with Diabetes Mellitus for Tuberculosis in China. Trop. Med. Int. Health 2012, 17, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Oluboyo, P.O.; Erasmus, R.T. The Significance of Glucose Intolerance in Pulmonary Tuberculosis. Tubercle 1990, 71, 135–138. [Google Scholar] [CrossRef]
- Adepoyibi, T.; Weigl, B.; Greb, H.; Neogi, T.; McGuire, H. New Screening Technologies for Type 2 Diabetes Mellitus Appropriate for Use in Tuberculosis Patients. Public Health Action 2013, 3, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Nijland, H.M.J.; Ruslami, R.; Stalenhoef, J.E.; Nelwan, E.J.; Alisjahbana, B.; Nelwan, R.H.H.; van der Ven, A.J.A.M.; Danusantoso, H.; Aarnoutse, R.E.; van Crevel, R. Exposure to Rifampicin Is Strongly Reduced in Patients with Tuberculosis and Type 2 Diabetes. Clin. Infect. Dis. 2006, 43, 848–854. [Google Scholar] [CrossRef]
- van Ingen, J.; Aarnoutse, R.E.; Donald, P.R.; Diacon, A.H.; Dawson, R.; Plemper Van Balen, G.; Gillespie, S.H.; Boeree, M.J. Why Do We Use 600 Mg of Rifampicin in Tuberculosis Treatment? Clin. Infect. Dis. 2011, 52, e194–e199. [Google Scholar] [CrossRef] [Green Version]
- Ruslami, R.; Ganiem, A.R.; Dian, S.; Apriani, L.; Achmad, T.H.; van der Ven, A.J.; Borm, G.; Aarnoutse, R.E.; van Crevel, R. Intensified Regimen Containing Rifampicin and Moxifloxacin for Tuberculous Meningitis: An Open-Label, Randomised Controlled Phase 2 Trial. Lancet Infect. Dis. 2013, 13, 27–35. [Google Scholar] [CrossRef]
- Mohan, V.; Saboo, B.; Khader, J.; Modi, K.D.; Jindal, S.; Wangnoo, S.K.; Amarnath, S. Position of Sulfonylureas in the Current ERA: Review of National and International Guidelines. In Clinical Medicine Insights: Endocrinology and Diabetes; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2022. [Google Scholar] [CrossRef]
- Cho, S.K.; Yoon, J.S.; Lee, M.G.; Lee, D.H.; Lim, L.A.; Park, K.; Park, M.S.; Chung, J.Y. Rifampin Enhances the Glucose-Lowering Effect of Metformin and Increases OCT1 MRNA Levels in Healthy Participants. Clin. Pharm. 2011, 89, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Tornio, A.; Niemi, M.; Neuvonen, P.J.; Backman, J.T. Drug Interactions with Oral Antidiabetic Agents: Pharmacokinetic Mechanisms and Clinical Implications. Trends Pharmacol. Sci. 2012, 33, 312–322. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drugs | Author (Year) | Article Typology | Key Outcomes |
|---|---|---|---|
| Metformin | Costantini et al. (2021) [8] | Review Article | Metformin may exert important pleiotropic effects, involving the regulation of lactate metabolism and adenosine monophosphate-activated protein kinase (AMPK) activation, and produce anti-inflammatory, anti-endotoxemic, vasoactive and antimicrobial actions |
| Bharath et al. (2021) [53] | Mini-Review | Metformin effect on mitochondrial function (inhibiting mitochondrial ROS and calcium-mediated activation of IL-6), autophagy, and immune modulation significantly impacts inflammation, independent of its role in blood glucose control. | |
| Gómez et al. * (2022) [54] | Retrospective cohort study | Exposure to metformin (n = 599) vs. not exposure (n = 2092) was associated with decreased 90-day mortality (71/599, 11.9% vs. 475/2092, 22.7%; OR, 0.46; 95% CI, 0.35–0.60), reduced severe acute kidney injury (50% vs. 57%; OR, 0.75; 95% CI, 0.62–0.90), lowered Major Adverse Kidney Events at 1 year (OR, 0.27; 95% CI, 0.22–0.68), and increased renal function recovery (95% vs. 86%; OR, 6.43; 95% CI, 3.42–12.1). | |
| Yen et al. (2022) [56] | Retrospective cohort study | In patients with DM, metformin displays no significant differences in the risks of UTI, recurrent UTI, or sepsis. However, it was associated with a lower risk of death due to UTI or sepsis than metformin non-user (p = 0.002). | |
| Li et al. (2021) [57] | Systematic Review and Meta-Analysis | At preadmission metformin use had lower mortality rate (OR, 0.74; 95% CIs, 0.62–0.88, p < 0.01) in patients with sepsis and DM. No statistically significant differences in the serum creatinine (p = 0.84) and lactic acid (p = 0.07) between preadmission metformin use and non-metformin use were reported. | |
| Masadeh et al. (2021) [58] | Pharmaceutical in vitro testing | In MRSA (ATCC 33,591) and MDR-Pseudomonas aeruginosa (ATCC BAA-2114) infection, combining metformin with the antibacterial agents had either synergetic or additive effects. | |
| Insulin | Van Niekerk (2017) [60] | Viewpoint Article | An increase glucose levels might be adaptive in the short term (maintaining biosynthetic activities, supporting immune response during an infection), but may exert negative effects (mitochondrial and innate immune cell dysfunctions) in chronic settings. Insulin can inhibit autophagy that plays a pivotal role in both host defense and cell survival. |
| Patel et al. (2021) [61] | Pharmaceutical in vitro testing | E. coli biofilm formation is insulin concentration dependent and is also influenced by oxygen concentration and temperature. | |
| Wei et al. (2019) [62] | Animal in vivo study/Pharmaceutical in vitro testing | Insulin did not promote the growth of P. aeruginosa. Insulin decreases the clearance of P. aeruginosa by inhibiting the Th1-type immune response and promoting biofilm formation by enhancing Th2-type polarization. | |
| Tsai et al. (2018) [63] | Review Article | Insulin receptor (INSR) on T cells supports cytokine production, effector cell differentiation, proliferation, nutrient uptake (and associated glycolytic and respiratory capacities), and boosts migration/recruitment to target organs. INSR deficiency compromises both CD4+ and CD8+ T cell compartments during influenza infection. | |
| GLP-1 Ras/DPP-4i | Steven et al. (2015) [64] | Animal in vivo study | Linagliptin, liraglutide (and to a minor extent sitagliptin) therapy suppress LPS-induced inflammatory pathways (e.g., iNOS induction and activation, leukocyte activation, DC maturation and biomarkers of inflammation) in endotoxemic rats, through a GLP-1-mediated decrease of iNOS expression as well as the activation of AMPK as central survival pathway. |
| Helmstädter et al. (2012) [65] | Animal in vivo study | Liraglutide displays both antioxidant and anti-inflammatory properties conferring vasoprotection in polymicrobial septic mice (lowering TNFα, IL-6, iNos and ICAM1 mRNA levels, attenuating elevated Nox2 protein) | |
| Steven et al. (2017) [66] | Animal in vivo study | GLP-1 receptor activation in platelets by linagliptin and liraglutide strongly attenuated endotoxemia-induced microvascular thrombosis and mortality by a cAMP/PKA-dependent mechanism, preventing systemic inflammation, vascular dysfunction, and end organ damage. | |
| Kröller-Schön et al. (2012) [67] | Animal in vivo study | Linagliptin, over all the other DDP-4i, demonstrated pleiotropic vasodilatory, antioxidant, and anti-inflammatory properties independent of its glucose-lowering properties. Linagliptin improved endothelial function by the reduction of leucocyte adhesion to endothelial cells in the presence of LPS. | |
| Al Zoubi et al. (2018) [68] | Animal in vivo study | Linagliptin significantly reduced sepsis-related cardiac, liver, kidney, and lung injury, by reducing NF-kB activation and iNOS expression in the heart, with lower serum inflammatory cytokine levels. Most notably, inhibition of NF-kB reduced organ dysfunction/injury associated with sepsis in mice with pre-existing T2DM. | |
| Wang et al. (2022) [69] | Animal in vivo study | Linagliptin exerted anti-inflammatory and anti-thrombotic effects independently of its effect on blood glucose level (inhibition of IL-1β and ICAM-1 expression, attenuation of tissue factor expression via the Akt/endothelial nitric oxide synthase phosphorylation) | |
| Yang et al. (2021) [51] | Review Article | GLP-1R is expressed in macrophages and monocytes and can inhibit the release of inflammatory factors. GLP-1R on can promote B- and T-cell proliferation, especially the expansion of Treg1, to inhibit systemic inflammatory response in sepsis patients. Thus, elevated endogenous GLP-1 levels are closely associated with worse outcomes. Therefore, since the GLP-1R is widely distributed in humans, GLP-1Ras have protective effects on multiple organs. | |
| SGLT2is | Donnan et al. (2019) [76] | Systematic review and meta-analysis | When compared with placebo, SGLT2 inhibitors were found to be significantly protective against AKI (RR = 0.59; 95% CI 0.39 to 0.89), while no difference was found for ketoacidosis or UTI. Subgroup analysis showed an increased risk of UTI with dapagliflozin only (RR 1.21; 95% CI 1.02 to 1.43). |
| Dave et al. (2019) [77] | Population-based cohort study | SGLT2is, when compared to DPP4i or a GLP-1RAs did not contribute to the severity of UTI events. | |
| Wiegley et al. (2022) [78] | Review Article | Despite SGLT2is-related glycosuria the increased urinary flow secondary to these medications’ osmotic effect has been proposed to explain the lack of clinically significant UTI. However, caution is required when SGLT2i agents are administered in patients with abnormal urinary flow (e.g., obstruction of urinary tract) | |
| Wang et al. (2022) [79] | Systematic review and meta-analysis | Compared to placebo or standard DM therapies, SGLT2is groups had reduced levels of ferritin (Standardized Mean Difference SMD −1.21; 95% CI: −1.91, −0.52, p < 0.001), C-reactive protein (SMD: 0.25; 95% CI: −0.47, −0.03, p = 0.02), leptin (SMD: −0.22; 95% CI:−0.43, −0.01, p = 0.04) and PAI-1 (SMD: −0.38; 95% CI: −0.61, −0.15, p = 0.001). | |
| Kıngır et al. (2019) [80] | Animal in vivo study | Dapagliflozin reduced oxidative stress (MDA), increased antioxidant levels (GSH), and reduced inflammation (MPO) in the kidney (p < 0.05). Dapagliflozin also decreased oxidative stress (MDA) in lung tissue and decreased inflammation (MPO) in lung and liver tissue (p < 0.05), although the effect was less relevant than in the kidney. | |
| Chi et al. (2021) [81] | Animal in vivo/in vitro study | Dapagliflozin attenuated endotoxin shock associated AKI and decreased the release of inflammatory cytokines in diabetic mice. | |
| Maayah et al. (2020) [82] | Animal in vivo study | Empagliflozin reduces mortality and inflammation in mice with established sepsis preventing renal injury, through the suppression of both local and systemic cytokine and chemokine release | |
| Li et al. (2022) [83] | Systematic review and meta-analysis | Compared with placebo, SGLT2is significantly reduced the risk of pneumonia (pooled RR 0.87, 95% CI 0.78–0.98) and septic shock (pooled RR 0.65, 95% CI 0.44–0.95). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pari, B.; Gallucci, M.; Ghigo, A.; Brizzi, M.F. Insight on Infections in Diabetic Setting. Biomedicines 2023, 11, 971. https://doi.org/10.3390/biomedicines11030971
Pari B, Gallucci M, Ghigo A, Brizzi MF. Insight on Infections in Diabetic Setting. Biomedicines. 2023; 11(3):971. https://doi.org/10.3390/biomedicines11030971
Chicago/Turabian StylePari, Bianca, Matteo Gallucci, Alberto Ghigo, and Maria Felice Brizzi. 2023. "Insight on Infections in Diabetic Setting" Biomedicines 11, no. 3: 971. https://doi.org/10.3390/biomedicines11030971