
Quantitative Autofluorescence in Non-Neovascular Age Related Macular Degeneration
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Participants
2.3. Study Assessments
2.4. Image Acquisition
2.5. Image Analysis
2.6. Definition of Various AMD Categories
2.7. Statistical Analysis
3. Results
3.1. Participant and Imaging Characteristics
3.2. Comparison of qAF8 Levels in AMD versus Control Eyes Aged ≥50 Years
3.3. Comparison of qAF8 Levels in AMD Categories Based on Beckman Classification versus Control Eyes from Participants Aged ≥50 Years
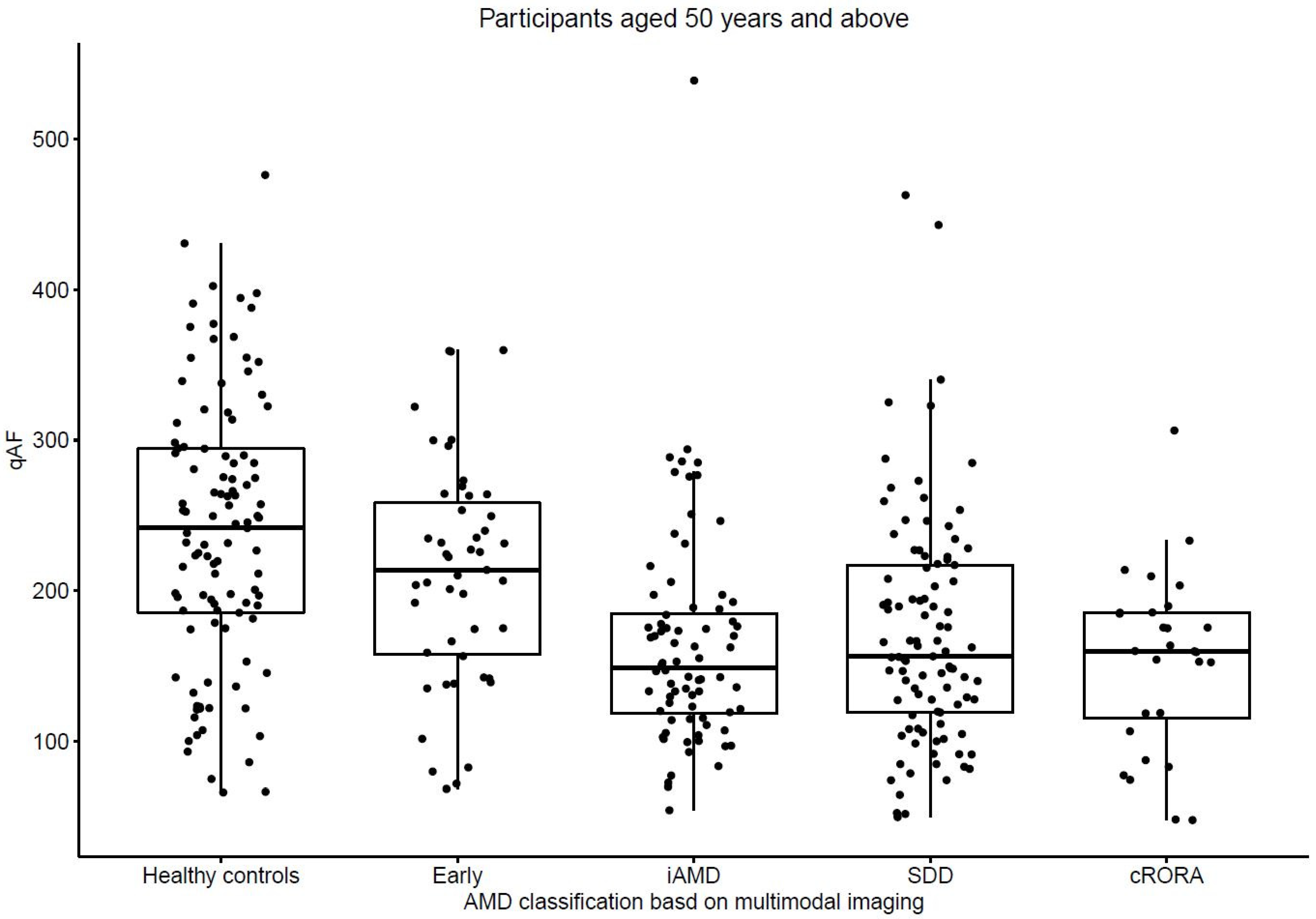
3.4. Comparison of qAF8 Levels in AMD Categories Based on MMI versus Control Eyes from Participants Aged ≥50 Years
3.5. Comparison of qAF8 Levels in AMD Eyes with and without Risk Factors of Progression to Geographic Atrophy or cRORA
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Okubo, A. The relationships of age changes in retinal pigment epithelium and Bruch’s membrane. Investig. Ophthalmol. Vis. Sci. 1999, 40, 443–449. [Google Scholar] [PubMed]
- Delori, F.C.; Goger, D.G.; Dorey, C.K. Age-related accumulation and spatial distribution of lipofuscin in RPE of normal subjects. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1855–1866. [Google Scholar]
- Moreno-García, A.; Kun, A.; Calero, O.; Medina, M.; Calero, M. An overview of the role of lipofuscin in age-related neurodegeneration. Front. Neurosci. 2018, 12, 464. [Google Scholar] [CrossRef] [Green Version]
- Young, R.W. Pathophysiology of age-related macular degeneration. Surv. Ophthalmol. 1987, 31, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Delori, F.C.; Fleckner, M.R.; Goger, D.G.; Weiter, J.J.; Dorey, C.K. Autofluorescence distribution associated with drusen in age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2000, 41, 496–504. [Google Scholar]
- Pollreisz, A.; Messinger, J.D.; Sloan, K.R.; Mittermueller, T.J.; Weinhandl, A.S.; Benson, E.K.; Kidd, G.; Schmidt-Erfurth, U.; Curcio, C.A. Visualizing melanosomes, lipofuscin, and melanolipofuscin in human retinal pigment epithelium using serial block face scanning electron microscopy. Exp. Eye Res. 2018, 166, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Brunk, U.T.; Terman, A. Lipofuscin: Mechanisms of age-related accumulation and influence on cell function. Free Radic. Biol. Med. 2002, 33, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Holz, F.G. Patterns of increased in vivo fundus autofluorescence in the junctional zone of geographic atrophy of the retinal pig-ment epithelium associated with age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 1999, 237, 145–152. [Google Scholar] [CrossRef]
- Sparrow, J.R.; Duncker, T. Fundus autofluorescence and RPE lipofuscin in age-related macular degeneration. J. Clin. Med. 2014, 3, 1302–1321. [Google Scholar] [CrossRef]
- Sparrow, J.R.; Duncker, T.; Schuerch, K.; Paavo, M.; de Carvalho, J.R.L., Jr. Lessons learned from quantitative fundus autofluorescence. Prog. Retin. Eye Res. 2020, 74, 100774. [Google Scholar] [CrossRef]
- Burke, T.R.; Duncker, T.; Woods, R.L.; Greenberg, J.P.; Zernant, J.; Tsang, S.H.; Smith, R.T.; Allikmets, R.; Sparrow, J.R.; Delori, F.C. Quantitative fundus autofluorescence in recessive Stargardt disease. Investig. Ophthalmol. Vis. Sci. 2014, 55, 2841–2852. [Google Scholar] [CrossRef] [Green Version]
- Gliem, M.; Müller, P.L.; Finger, R.P.; McGuinness, M.B.; Holz, F.G.; Issa, P.C. Quantitative fundus autofluorescence in early and intermediate age-related macular degeneration. JAMA Ophthalmol. 2016, 134, 817–824. [Google Scholar] [CrossRef]
- Greenberg, J.P.; Duncker, T.; Woods, R.L.; Smith, R.T.; Sparrow, J.R.; Delori, F.C. Quantitative fundus autofluorescence in healthy eyes. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5684–5693. [Google Scholar] [CrossRef] [Green Version]
- Reiter, G.S.; Schwarzenbacher, L.; Schartmüller, D.; Röggla, V.; Leydolt, C.; Menapace, R.; Schmidt-Erfurth, U.; Sacu, S. Influence of lens opacities and cataract severity on quantitative fundus autofluorescence as a secondary outcome of a randomized clinical trial. Sci. Rep. 2021, 11, 12685. [Google Scholar] [CrossRef]
- Wang, Y.; Tran, T.; Firl, K.; Huang, N.; Yasin, O.; van Kuijk, F.J.; Montezuma, S.R. Quantitative fundus autofluorescence in smokers compared to non-smokers. Exp. Eye Res. 2019, 184, 48–55. [Google Scholar] [CrossRef]
- Ach, T.; Huisingh, C.; McGwin, G., Jr.; Messinger, J.D.; Zhang, T.; Bentley, M.J.; Gutierrez, D.B.; Ablonczy, Z.; Smith, R.T.; Sloan, K.R.; et al. Quantitative autofluorescence and cell density maps of the human retinal pigment epithelium. Investig. Ophthalmol. Vis. Sci. 2014, 55, 4832–4841. [Google Scholar] [CrossRef] [Green Version]
- Mata, N.L.; Lichter, J.B.; Vogel, R.; Han, Y.; Bui, T.V.; Singerman, L.J. Investigation of oral fenretinide for treatment of geographic atrophy in age-related macular degeneration. Retina 2013, 33, 498–507. [Google Scholar] [CrossRef]
- Petrukhin, K. Pharmacological inhibition of lipofuscin accumulation in the retina as a therapeutic strategy for dry AMD treatment. Drug Discov. Today Ther. Strat. 2013, 10, e11–e20. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, P.J. Emixustat hydrochloride for geographic atrophy secondary to age-related macular degeneration: A randomized clinical trial. Ophthalmology 2018, 125, 1556–1567. [Google Scholar] [CrossRef] [Green Version]
- Sadda, S.R. Consensus definition for atrophy associated with age-related macular degeneration on OCT: Classification of atrophy report 3. Ophthalmology 2018, 125, 537–548. [Google Scholar] [CrossRef] [Green Version]
- von der Emde, L. Natural history of quantitative autofluorescence in intermediate age-related macular de-generation. Retina 2021, 41, 694–700. [Google Scholar] [CrossRef]
- van de Kraats, J.; van Norren, D. Optical density of the aging human ocular media in the visible and the UV. J. Opt. Soc. Am. A. Opt. Image Sci. Vis. 2007, 24, 1842–1857. [Google Scholar] [CrossRef]
- Ferris, F.L., 3rd; Wilkinson, C.P.; Bird, A.; Chakravarthy, U.; Chew, E.; Csaky, K.; Sadda, S.R. Clinical classification of age-related macular degeneration. Ophthalmology 2013, 120, 844–851. [Google Scholar] [CrossRef]
- Spaide, R.F.; Ooto, S.; Curcio, C.A. Subretinal drusenoid deposits AKA pseudodrusen. Surv. Ophthalmol. 2018, 63, 782–815. [Google Scholar] [CrossRef]
- Kim, D.Y. Comparison of single drusen size on color fundus photography and spectral-domain optical coherence tomography. Retina 2021, 41, 1715–1722. [Google Scholar] [CrossRef]
- Spaide, R.F.; Curcio, C.A. Drusen characterization with multimodal imaging. Retina 2010, 30, 1441–1454. [Google Scholar] [CrossRef] [Green Version]
- Hardin, J.W.; Hilbe, J.M. Generalized Estimating Equations, 1st ed.; Chapman and Hall/CRC: Boca Raton, FL, USA, 2002. [Google Scholar]
- Liang, K.-Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Shih, J.H.; Fay, M.P. Pearson’s chi-square test and rank correlation inferences for clustered data. Biometrics 2017, 73, 822–834. [Google Scholar] [CrossRef]
- Orellana-Rios, J.; Yokoyama, S.; Agee, J.M.; Challa, N.; Freund, K.B.; Yannuzzi, L.A.; Smith, R.T. Quantitative fundus autofluorescence in non-neovascular age-related macular degeneration. Ophthalmic Surg. Lasers Imaging Retin. 2018, 49, S34–S42. [Google Scholar] [CrossRef]
- Armenti, S.T.; Greenberg, J.P.; Smith, R.T. Quantitative fundus autofluorescence for the evaluation of retinal diseases. J. Vis. Exp. 2016, 11, 53577. [Google Scholar] [CrossRef]
- Sparrow, J.R.; Gregory-Roberts, E.; Yamamoto, K.; Blonska, A.; Ghosh, S.K.; Ueda, K.; Zhou, J. The bisretinoids of retinal pigment epithelium. Prog. Retin. Eye Res. 2012, 31, 121–135. [Google Scholar] [CrossRef] [Green Version]
- Ferrington, D.A.; Sinha, D.; Kaarniranta, K. Defects in retinal pigment epithelial cell proteolysis and the pathology associated with age-related macular degeneration. Prog. Retin. Eye Res. 2016, 51, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, G.J. Imaging features associated with progression to geographic atrophy in age-related macular degeneration: Classification of atrophy meeting report 5. Ophthalmol. Retina 2021, 5, 855–867. [Google Scholar] [CrossRef] [PubMed]
- Balaratnasingam, C. Cuticular drusen: Clinical phenotypes and natural history defined using multimodal imaging. Ophthalmology 2018, 125, 100–118. [Google Scholar] [CrossRef] [Green Version]
- Bird, A. Role of retinal pigment epithelium in age-related macular disease: A systematic review. Br. J. Ophthalmol. 2021, 105, 1469–1474. [Google Scholar] [CrossRef]
- Reiter, G.S.; Told, R.; Schlanitz, F.G.; Bogunovic, H.; Baumann, L.; Sacu, S.; Schmidt-Erfurth, U.; Pollreisz, A. Impact of drusen volume on quantitative fundus autofluorescence in early and intermediate age-related macular degeneration. Investig. Opthalmol. Vis. Sci. 2019, 60, 1937–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt-Erfurth, U.; Bogunovic, H.; Grechenig, C.; Bui, P.; Fabianska, M.; Waldstein, S.; Reiter, G.S. Role of deep learning—Quantified hyperreflective foci for the prediction of geographic atrophy progression. Am. J. Ophthalmol. 2020, 216, 257–270. [Google Scholar] [CrossRef]
- Owsley, C.; Clark, M.E.; McGwin, G. Natural history of rod-mediated dark adaptation over 2 years in intermediate age-related macular degeneration. Transl. Vis. Sci. Technol. 2017, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Ablonczy, Z.; Higbee, D.; Anderson, D.M.; Dahrouj, M.; Grey, A.; Gutierrez, D.; Koutalos, Y.; Schey, K.L.; Hanneken, A.; Crouch, R.K. Lack of correlation between the spatial distribution of A2E and lipofuscin fluorescence in the human retinal pigment epithelium. Investig. Ophthalmol. Vis. Sci. 2013, 54, 5535–5542. [Google Scholar] [CrossRef]
- Kleefeldt, N.; Bermond, K.; Tarau, I.-S.; Hillenkamp, J.; Berlin, A.; Sloan, K.R.; Ach, T. Quantitative fundus autofluorescence: Advanced analysis tools. Transl. Vis. Sci. Technol. 2020, 9, 2. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| AMD vs. Controls | |||
|---|---|---|---|
| Variable | Overall, N = 353 Eyes of 231 Participants | Controls, N = 105 Eyes of 63 Participants | AMD, N = 248 Eyes of 176 Participants |
| Participant level a | |||
| Number of participants with bilateral eyes | 122 (52.8%) | 42 (66.7%) | 72 (40.9%) |
| Age, years | 70.3 (8.5) | 64.2 (8.2) | 72.4 (7.5) |
| Age, years | |||
| <60 | 30 (13.0%) | 20 (31.8%) | 11 (6.3%) |
| 60–69 | 65 (28.1%) | 24 (38.1%) | 44 (25.0%) |
| 70–79 | 104 (45.0%) | 15 (23.8%) | 92 (52.3%) |
| ≥80 | 32 (13.9%) | 4 (6.3%) | 29 (16.5%) |
| Gender | |||
| M | 93 (40.3%) | 28 (44.4%) | 68 (38.6%) |
| F | 138 (59.7%) | 35 (55.6%) | 108 (61.4%) |
| Eye level b | |||
| Pseudophakic eyes | 60 (17.0%) | 7 (6.7%) | 53 (21.4%) |
| Beckman AMD classification | |||
| Normal | 105 (29.7%) | 105 (100.0%) | 0 (0.0%) |
| Early | 59 (16.7%) | 0 (0.0%) | 59 (23.8%) |
| iAMD | 161 (45.6%) | 0 (0.0%) | 161 (64.9%) |
| GA | 28 (7.9%) | 0 (0.0%) | 28 (11.3%) |
| AMD classification based on multimodal imaging | |||
| Normal | 105 (29.7%) | 105 (100.0%) | 0 (0.0%) |
| Early | 47 (13.3%) | 0 (0.0%) | 47 (19.0%) |
| iAMD | 76 (21.5%) | 0 (0.0%) | 76 (30.6%) |
| SDD | 97 (27.5%) | 0 (0.0%) | 97 (39.1%) |
| cRORA | 28 (7.9%) | 0 (0.0%) | 28 (11.3%) |
| Median qAF8 (IQR) | 184.0 (132.2, 246.4) | 241.6 (185.4, 294.4) | 163.5 (122.6, 216.6) |
| Analysis in AMD eyes c; n (%) | |||
| Stage of SDD | |||
| 0 | 151/248 (60.9%) | 0 (NA%) | 151/248 (60.9%) |
| 1 | 5/248 (2.0%) | 0 (NA%) | 5/248 (2.0%) |
| 2 | 15/248 (6.0%) | 0 (NA%) | 15/248 (6.0%) |
| 3 | 77/248 (31.0%) | 0 (NA%) | 77/248 (31.0%) |
| Indicators of RPE integrity | |||
| Absence of HRF, iRORA or cRORA | 153/248 (61.7%) | 0 (NA%) | 153/248 (61.7%) |
| Presence of HRF without evidence of iRORA or cRORA | 16/248 (6.5%) | 0 (NA%) | 16/248 (6.5%) |
| Presence of iRORA without any evidence of cRORA | 51/248 (20.6%) | 0 (NA%) | 51/248 (20.6%) |
| Presence of cRORA | 28/248 (11.3%) | 0 (NA%) | 28/248 (11.3%) |
| Drusen volume in those without cRORA (N = 220 eyes) | 0.44 (0.36, 0.54) | NA | 0.44 (0.36, 0.54) |
| Characteristics | N | Coefficient in Log-qAF8 Units | qAF8 Difference in % | p-Value |
|---|---|---|---|---|
| Controls vs. AMD | 353 | |||
| Controls | - | - | ||
| AMD | −0.22 (−0.34–−0.11) | −19.7% (−28.8%, −10.4%) | <0.001 | |
| Beckman classification | 353 | |||
| Normal | - | - | ||
| Early | −0.14 (−0.28–−0.01) | −13.1% (−24.4%, −1%) | 0.04 | |
| iAMD | −0.26 (−0.39–−0.14) | −22.9% (−32.3%, −13.1%) | <0.001 | |
| GA | −0.29 (−0.48–−0.11) | −25.2% (−38.1%, −10.4%) | 0.002 | |
| AMD classification based on multimodal imaging | 353 | |||
| Normal | - | |||
| Early without SDD | −0.06 (−0.21–0.08) | −5.8% (−18.9%, 8.3%) | 0.40 | |
| iAMD without SDD | −0.31 (−0.45–−0.17) | −26.7% (−36.2%, −15.6%) | <0.001 | |
| SDD | −0.27 (−0.41–−0.13) | −23.7% (−33.6%, −12.2%) | <0.001 | |
| cRORA | −0.31 (−0.50–−0.12) | −26.7% (−39.3%, −11.3%) | 0.001 | |
| Stage of SDD in those with SDD | 97 | |||
| Stage 1 or 2 | - | |||
| Stage 3 | −0.05 (−0.28−0.18) | −4.9% (−24.4%, 19.7%) | 0.67 | |
| Stage of SDD | 248 | |||
| 0 | - | |||
| 1 | 0.01 (−0.17–0.19) | 1% (−15.6%, 20.9%) | 0.88 | |
| 2 | 0.05 (−0.22–0.33) | 5.1% (−19.7%, 39.1%) | 0.71 | |
| 3 | −0.05 (−0.17–0.07) | −4.9% (−15.6%, 7.3%) | 0.38 | |
| Drusen volume in those without cRORA, per 0.1-unit increase | 220 | −0.01 (−0.05–0.02) | −1.4% (−4.6%, 1.9%) | 0.40 |
| Indicators of RPE integrity | 248 | |||
| Absence of HRF without evidence of iRORA or cRORA | - | |||
| Presence of HRF without evidence of iRORA or cRORA | −0.18 (−0.43–0.07) | −16.5% (−34.9%, 7.25%) | 0.16 | |
| Presence of iRORA without any evidence of cRORA | −0.16 (−0.28–−0.03) | −14.8% (−24.4%, −3.0%) | 0.01 | |
| Presence of cRORA | −0.13 (−0.30–0.05) | −12.2% (−25.9%, 5.1%) | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandra, S.; Grewal, M.K.; Gurudas, S.; Sondh, R.; Bird, A.; Jeffery, G.; Chong, V.; Sivaprasad, S. Quantitative Autofluorescence in Non-Neovascular Age Related Macular Degeneration. Biomedicines 2023, 11, 560. https://doi.org/10.3390/biomedicines11020560
Chandra S, Grewal MK, Gurudas S, Sondh R, Bird A, Jeffery G, Chong V, Sivaprasad S. Quantitative Autofluorescence in Non-Neovascular Age Related Macular Degeneration. Biomedicines. 2023; 11(2):560. https://doi.org/10.3390/biomedicines11020560
Chicago/Turabian StyleChandra, Shruti, Manjot K. Grewal, Sarega Gurudas, Rajan Sondh, Alan Bird, Glen Jeffery, Victor Chong, and Sobha Sivaprasad. 2023. "Quantitative Autofluorescence in Non-Neovascular Age Related Macular Degeneration" Biomedicines 11, no. 2: 560. https://doi.org/10.3390/biomedicines11020560