
Fetal Fibroblast Transplantation via Ablative Fractional Laser Irradiation Reduces Scarring

Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Experiment
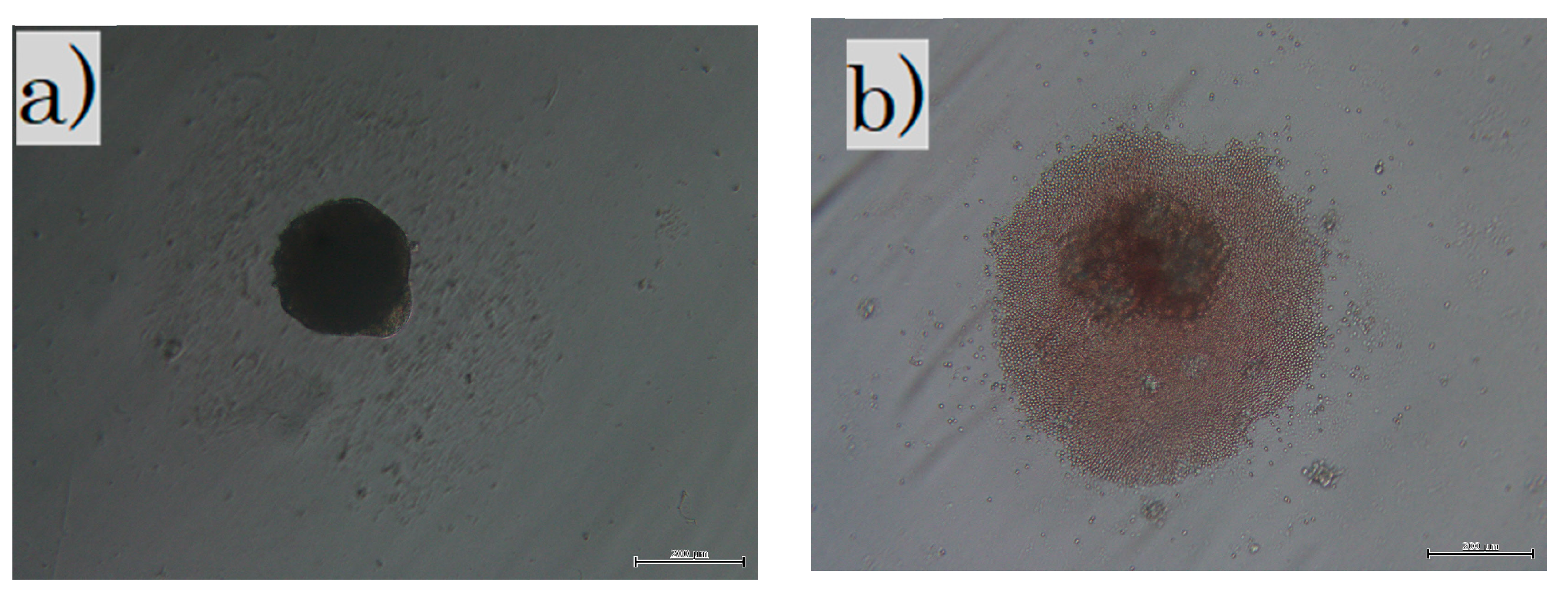
2.2. Fibroblast Culture and Transplantation
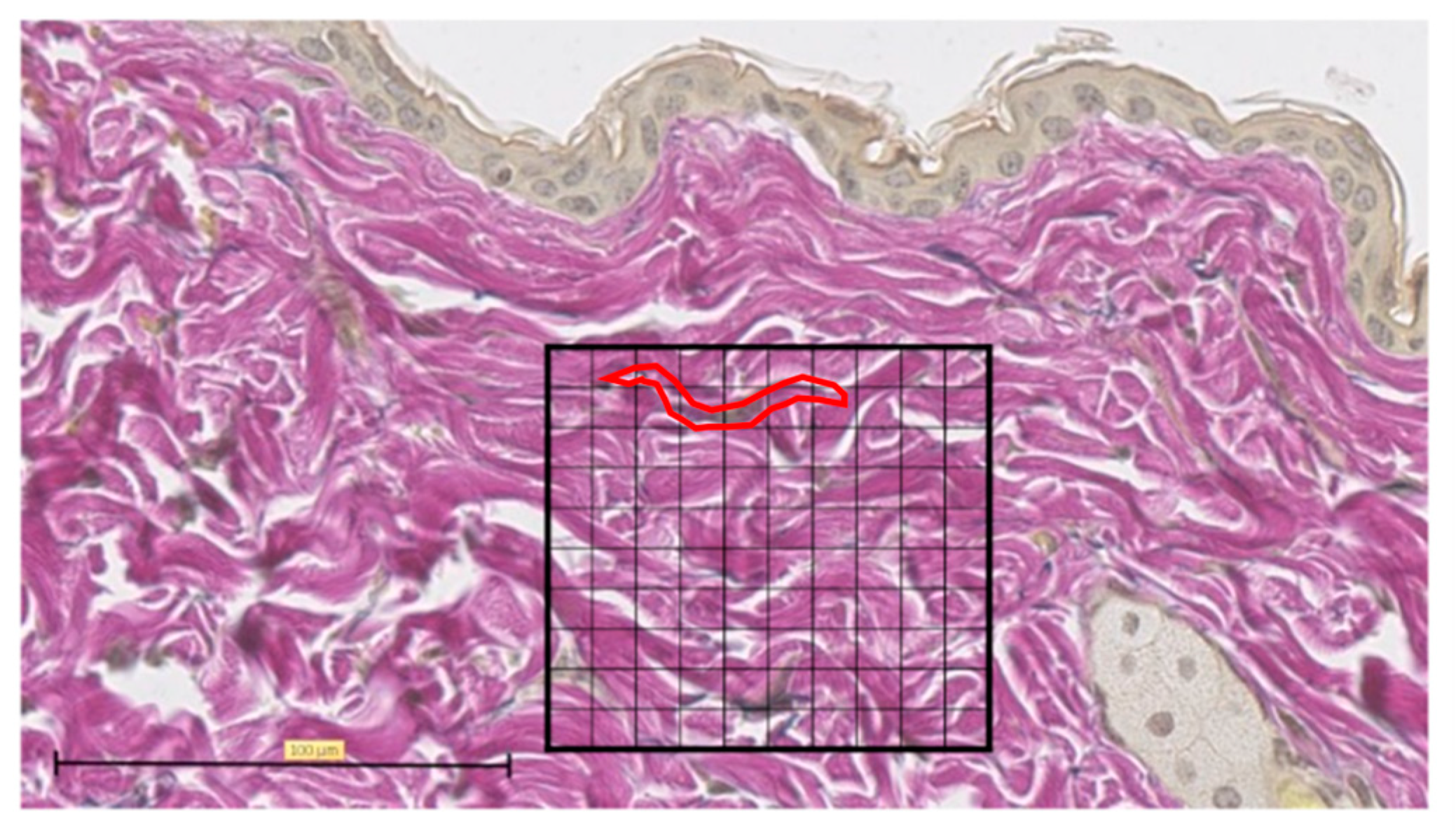
2.3. MMTSS
2.4. Immunofluorescence Staining and Immunohistochemistry
3. Results
3.1. Fractional Laser for Scars
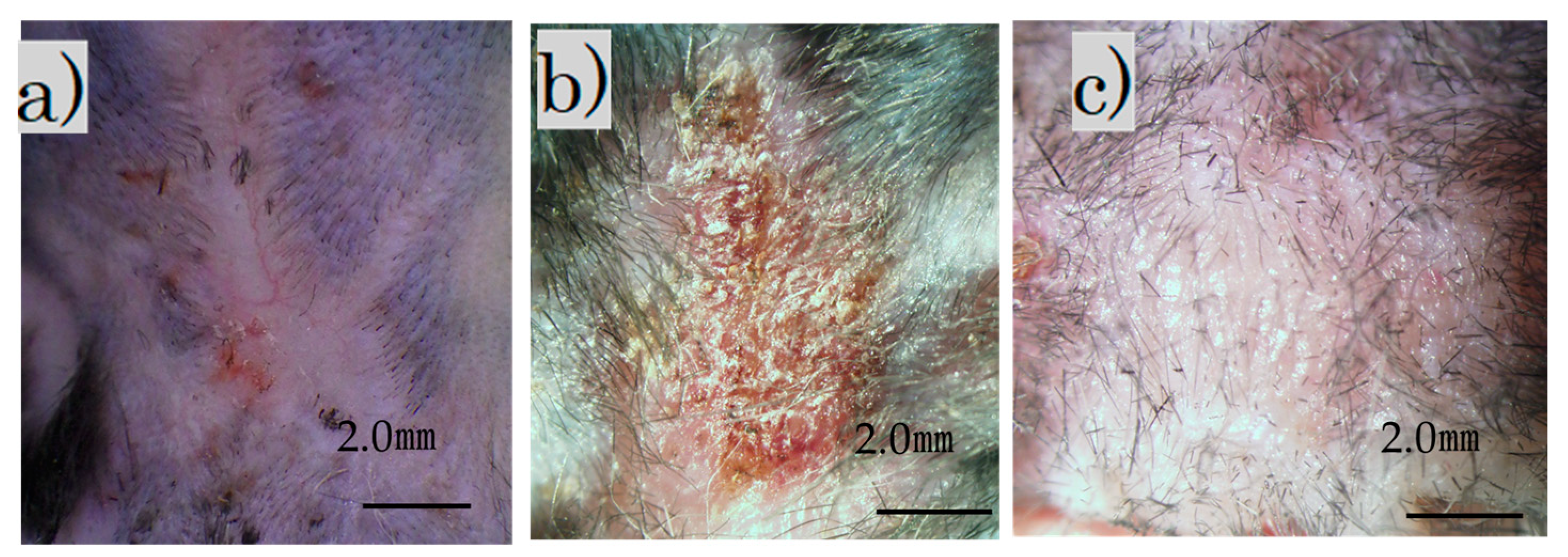
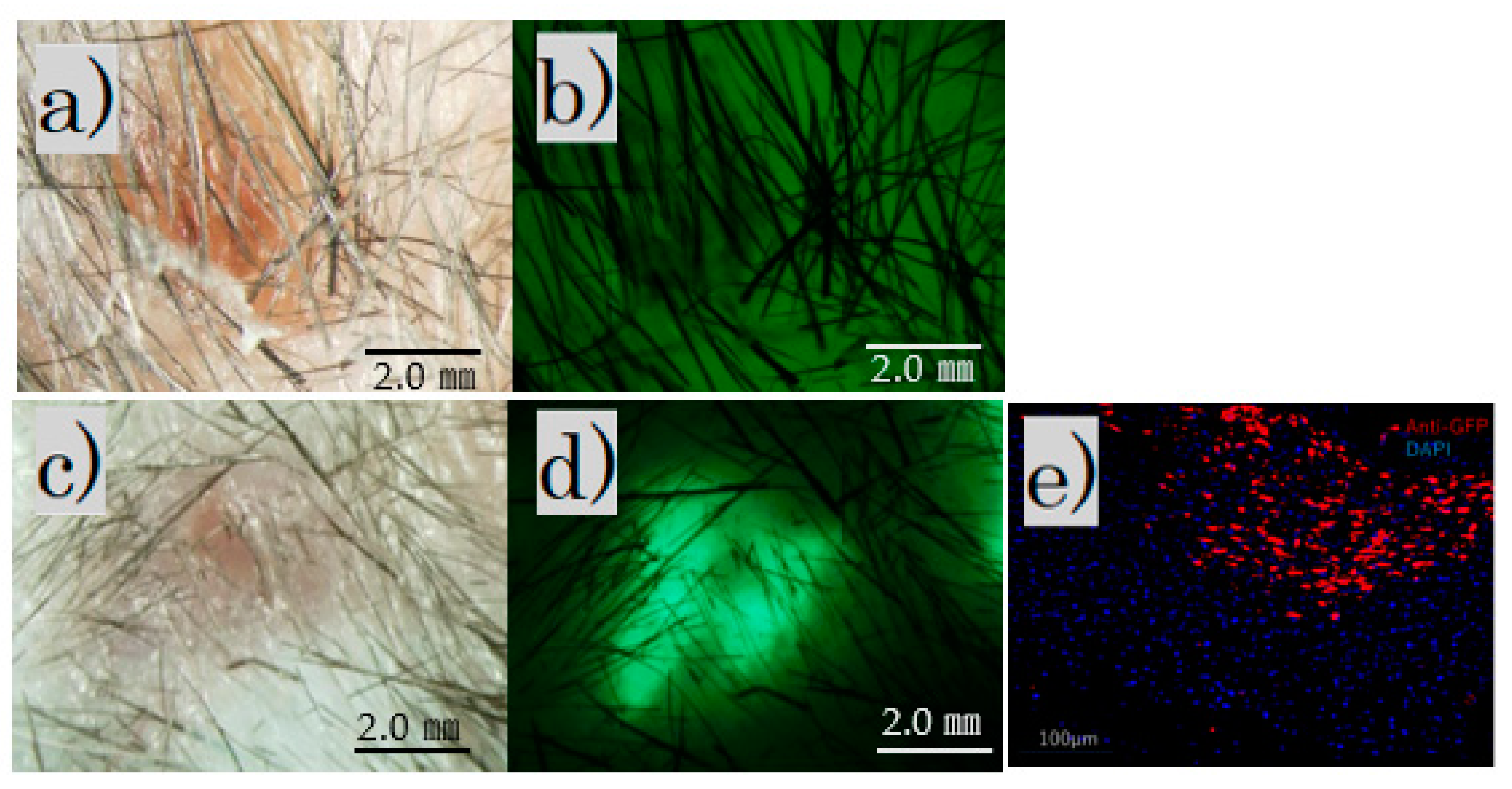
3.1.1. Transplanted Cells Took Well after Ablative CO2 Laser Treatment
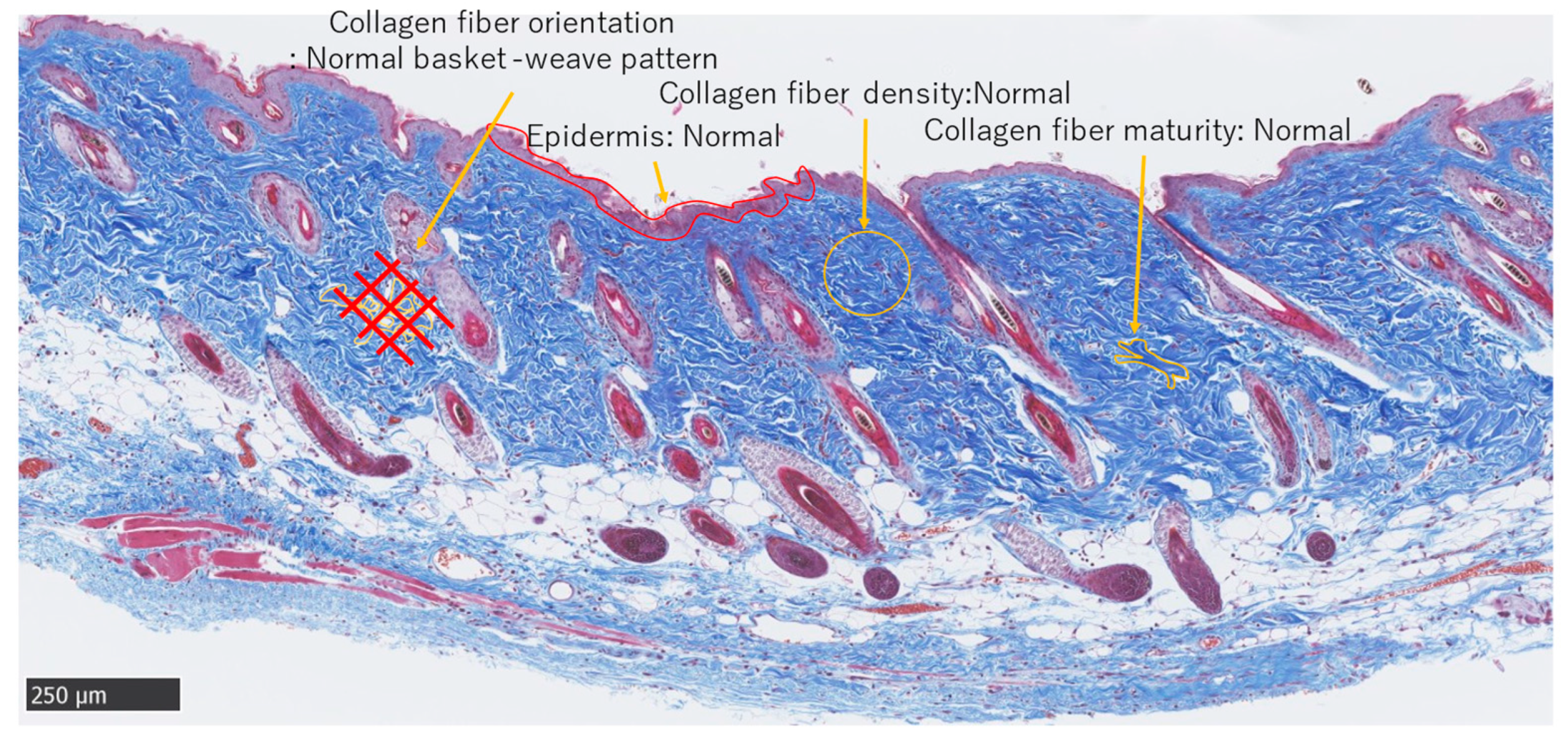
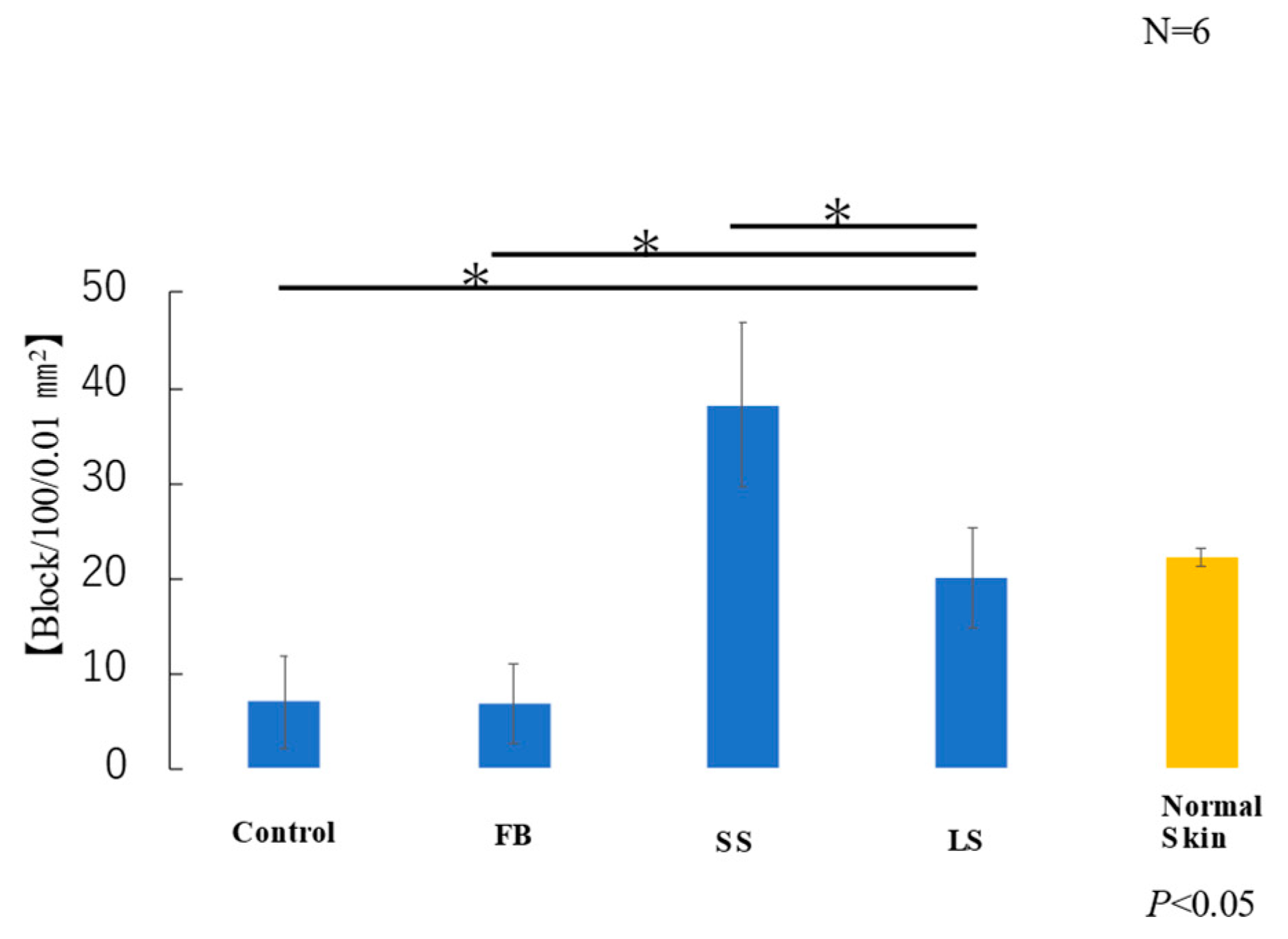
3.1.2. MT-Stained and MMTSS
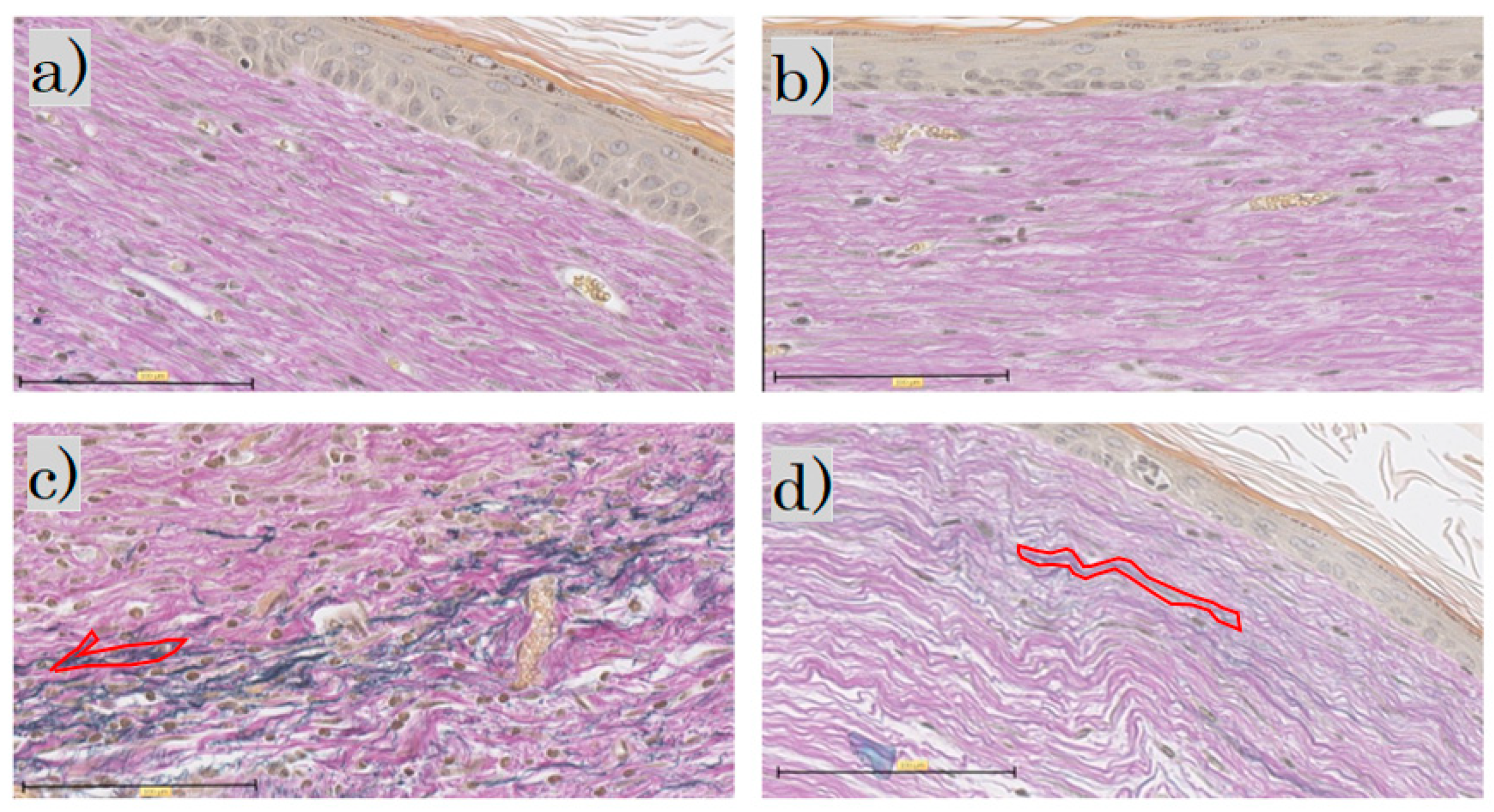
3.1.3. EVG Stained
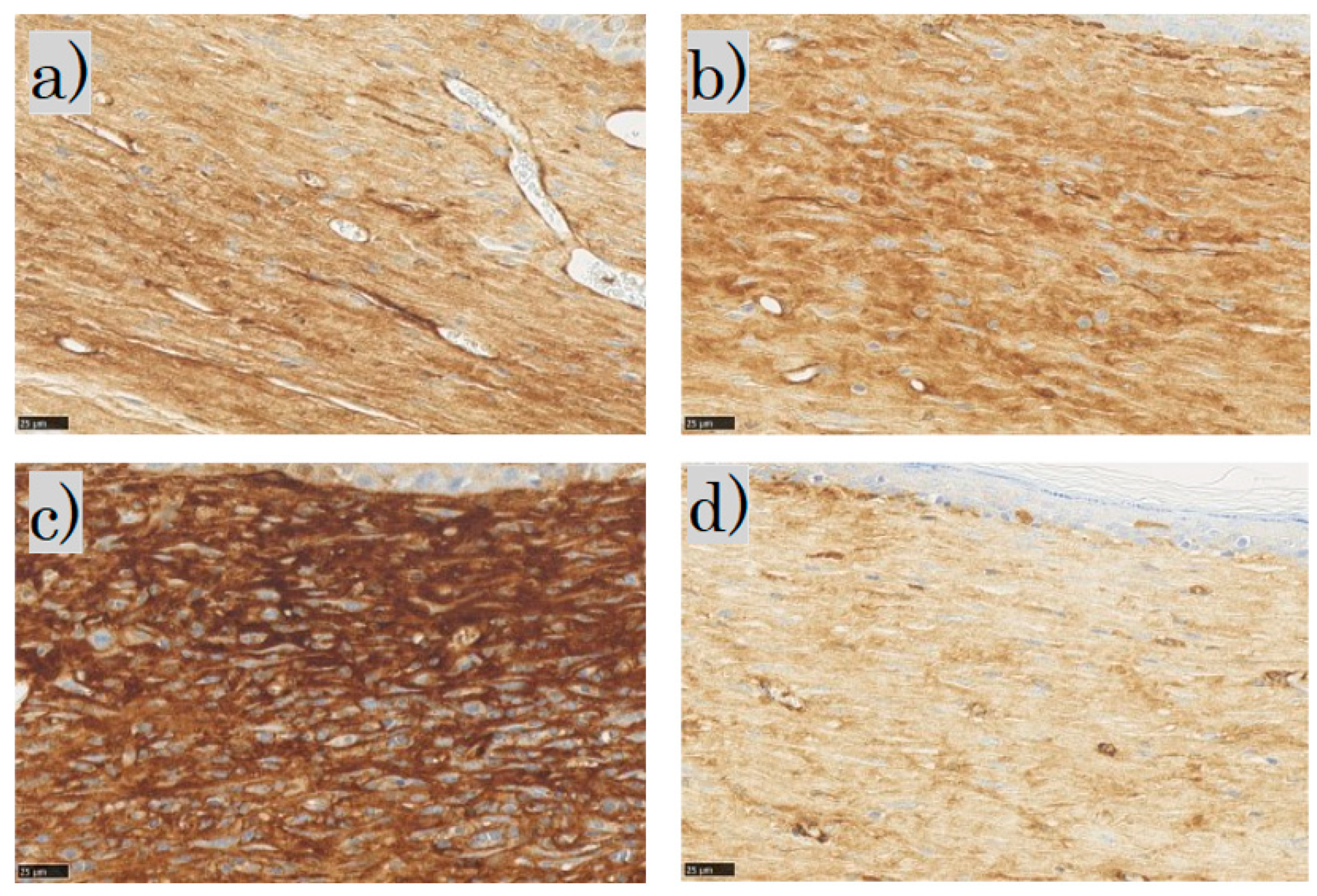
3.1.4. Immunohistochemical Staining of α-SMA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takaya, K.; Okabe, K.; Ishigami, A.; Imbe, Y.; Kanazawa, H.; Sakai, S.; Aramaki-Hattori, N.; Kishi, K. Actin cable formation and epidermis-dermis positional relationship during complete skin regeneration. Sci. Rep. 2022, 12, 15913. [Google Scholar] [CrossRef] [PubMed]
- Ishii, T.; Takashimizu, I.; Casco-Robles, M.M.; Taya, Y.; Yuzuriha, S.; Toyama, F.; Maruo, F.; Kishi, K.; Chiba, C. Skin wound healing of the adult newt, Cynopspyrrhogaster: A unique re-epithelialization and scarless model. Biomedicines 2021, 9, 1892. [Google Scholar] [CrossRef] [PubMed]
- Thangapazham, R.L.; Darling, T.N.; Meyerle, J. Alteration of skin properties with autologous dermal fibroblasts. Int. J. Mol. Sci. 2014, 15, 8407–8427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takaya, K.; Aramaki-Hattori, N.; Sakai, S.; Okabe, K.; Asou, T.; Kishi, K. Decorin inhibits dermal mesenchymal cell migration and induces scar formation. Plast. Reconstr. Surg. 2022, 10, e4245. [Google Scholar] [CrossRef]
- Kishi, K.; Katsube, K.; Satoh, H.; Imanishi, N.; Nakajima, H.; Nakajima, T. The fetal dermal but not loose fascial mesenchymal cells possess regenerative activity of dermal structure. Cell Transplant. 2005, 14, 709–714. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, R.; Okabe, K.; Kubota, Y.; Nakamura-Ishizu, A.; Nakajima, H.; Kishi, K. Sphere formation restores and confers hair-inducing capacity in cultured mesenchymal cells. Exp. Dermatol. 2011, 20, 679–681. [Google Scholar] [CrossRef]
- Miwa, T.; Idiris, A.; Kumagai, H. High-throughput 3D spheroid formation and effective cardiomyocyte differentiation from human iPS cells using the microfabric vessels EZSPHERETM. Bio-Protocol 2021, 11, e4203. [Google Scholar] [CrossRef]
- Koudan, E.V.; Zorina, A.I.; Levin, A.A.; Pereira, F.D.A.S.; Petrov, S.V.; Karshieva, S.S.; Kasyanov, V.A.; Manturova, N.E.; Ustyugov, A.Y.; Potekaev, N.N.; et al. Correlation of the regenerative potential of dermal fibroblasts in 2D culture with the biological properties of fibroblast-derived tissue spheroids. Cell Tissue Res. 2022, 390, 453–464. [Google Scholar] [CrossRef]
- Beausang, E.M.D.; Floyd, H.; Dunn, K.W.; Orton, C.I.F.D.S.; Ferguson, M.W. A new quantitative scale for clinical scar assessment. Plast. Reconstr. Surg. 1998, 102, 1954–1961. [Google Scholar] [CrossRef]
- Smitha, G.P.; Shenoy, S.; Narayan, T.V.; Jayaram, R. Comparison of myofibroblasts between solid/multicystic ameloblastoma and unicystic ameloblastoma: An immunohistochemical analysis. J. Clin. Diagn. Res. 2016, 10, ZC52–ZC57. [Google Scholar] [CrossRef]
- Maninder, K.; Richa, R.; Dinesh, A.P.; Suman, P. Factors affecting the outcome of fractional carbon dioxide laser resurfacing of various types of scars in skin of color. J. Cosmet. Dermatol. 2022, 21, 3842–3847. [Google Scholar] [CrossRef] [PubMed]
- Asilian, A.; Salimi, E.; Faghihi, G.; Dehghani, F.; Tajmirriahi, N.; Hosseini, S.M. Comparison of Q-Switched 1064-nm Nd: YAG laser and fractional CO2 laser efficacies on improvement of atrophic facial acne scar. J. Res. Med. Sci. 2011, 16, 1189–1195. [Google Scholar] [PubMed]
- Gazitaeva, Z.I.; Drobintseva, A.O.; Prokopov, A.Y.; Sidorina, A.N.; Leonteva, D.O.; Kvetnoy, I.M. Signaling Molecules of Human Skin Cells as the Targets for Injection Cosmetology. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1473–1480. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Yang, J.; Guan, Y.; Zhang, J.; Zhang, Q. A new treatment for static forehead rhytides: Autologous fibroblast and keratin injection. J. Cosmet. Dermatol. 2021, 20, 3308–3314. [Google Scholar] [CrossRef]
- Zou, Q.; Zhang, M.; Yuan, R.; Wang, Y.; Gong, Z.; Shi, R.; Li, Y.; Fei, K.; Luo, C.; Xiong, Y.; et al. Small extracellular vesicles derived from dermal fibroblasts promote fibroblast activity and skin development through carrying miR-218 and ITGBL1. J. Nanobiotechnol. 2022, 20, 296. [Google Scholar] [CrossRef]
- Hu, S.; Li, Z.; Cores, J.; Huang, K.; Su, T.; Dinh, P.U.; Cheng, K. Needle-free injection of exosomes derived from human dermal fibroblast spheroids ameliorates skin photoaging. ACS Nano 2019, 13, 11273–11282. [Google Scholar] [CrossRef]
- Smith, S.R.; Munavalli, G.; Weiss, R.; Maslowski, J.M.; Hennegan, K.P.; Novak, J.M. A multicenter, double-blind, placebo-controlled trial of autologous fibroblast therapy for the treatment of nasolabial fold wrinkles. Dermatol. Surg. 2012, 38 Pt 2, 1234–1243. [Google Scholar] [CrossRef]
- Rodriguez-Menocal, L.; Salgado, M.; Davis, S.; Waibel, J.; Shabbir, A.; Cox, A.; Badiavas, E.V. Percutaneous bone marrow transplantation using fractional ablative Erbium: YAG laser. PLoS ONE 2014, 9, e93004. [Google Scholar] [CrossRef]
- Feng, C.; Shan, M.; Xia, Y.; Zheng, Z.; He, K.; Wei, Y.; Song, K.; Meng, T.; Liu, H.; Hao, Y.; et al. Single-cell RNA sequencing reveals distinct immunology profiles in human keloid. Front. Immunol. 2022, 13, 940645. [Google Scholar] [CrossRef]
- Neveux, Y.; Rives, J.M.; Le Breton, C.; Gentilhomme, E.; Saint-Blancar, P.; Carsin, H. Clinical interest of cutaneous models reproduced in vitro for severe burn treatment: Histopathological and ultrastructural study. Cell Biol. Toxicol. 1995, 11, 173–178. [Google Scholar] [CrossRef]
- Higgins, C.A.; Chen, J.C.; Cerise, J.E.; Jahoda, C.A.; Christiano, A.M. Microenvironmental reprogramming by three-dimensional culture enables dermal papilla cells to induce de novo human hair-follicle growth. Proc. Natl. Acad. Sci. USA 2013, 110, 19679–19688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadoya, K.; Amano, S.; Inomata, S.; Tsunenaga, M.; Matsuzaki, K.; Oshima, H.; Tanabe, M.; Kumagai, N.; Nishiyama, T. Evaluation of autologous cultured epithelium as replacement skin after tattoo excision: Correlation between skin texture and histological features. Br. J. Dermatol. 2003, 149, 377–380. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Epidermis | B. Collagen fiber density |
| Collagen fiber orientation | 0 = normal fiber bundle density |
| 0 = Normal | 1 ≤ 25% abnormal |
| 1 = Some restoration of rete ridges | 2 = 26–50% abnormal |
| 2 = No restoration of rete ridges | 3 = 51–75% abnormal |
| Dermis | 4 = 76–100% abnormal |
| A. Collagen fiber orientation | C. Collagen fiber maturity |
| 0 = Normal basket-weave pattern | 0 = normal fiber maturity |
| 1 ≤ 25% abnormal | 1 ≤ 25% abnormal |
| 2 = 26–50% abnormal | 2 = 26–50% abnormal |
| 3 = 51–75% abnormal | 3 = 51–75% abnormal |
| 4 = 76–100% abnormal | 4 = 76–100% abnormal |
| Total score range: 0–14 |
| Mouse No. | No. 1 | No. 2 | No. 3 | No. 4 | No. 5 | No. 6 | Total Average |
|---|---|---|---|---|---|---|---|
| Control | 5 | 8.3 | 2.3 | 4.6 | 10 | 3.6 | 5.6 |
| FB | 6.3 | 5 | 6.3 | 3.3 | 4.6 | 4.3 | 5 |
| SS | 4 | 3 | 10.6 | 2.6 | 2.3 | 7.3 | 5 |
| LS | 3.6 | 2.3 | 3 | 5.6 | 2.3 | 4 | 3.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, S.; Aramaki-Hattori, N.; Kishi, K. Fetal Fibroblast Transplantation via Ablative Fractional Laser Irradiation Reduces Scarring. Biomedicines 2023, 11, 347. https://doi.org/10.3390/biomedicines11020347
Sakai S, Aramaki-Hattori N, Kishi K. Fetal Fibroblast Transplantation via Ablative Fractional Laser Irradiation Reduces Scarring. Biomedicines. 2023; 11(2):347. https://doi.org/10.3390/biomedicines11020347
Chicago/Turabian StyleSakai, Shigeki, Noriko Aramaki-Hattori, and Kazuo Kishi. 2023. "Fetal Fibroblast Transplantation via Ablative Fractional Laser Irradiation Reduces Scarring" Biomedicines 11, no. 2: 347. https://doi.org/10.3390/biomedicines11020347