
Evidence of Improvement of Lower Limb Functioning Using Hydrotherapy on Spinal Cord Injury Patients
 ,
,
Abstract
:1. Introduction
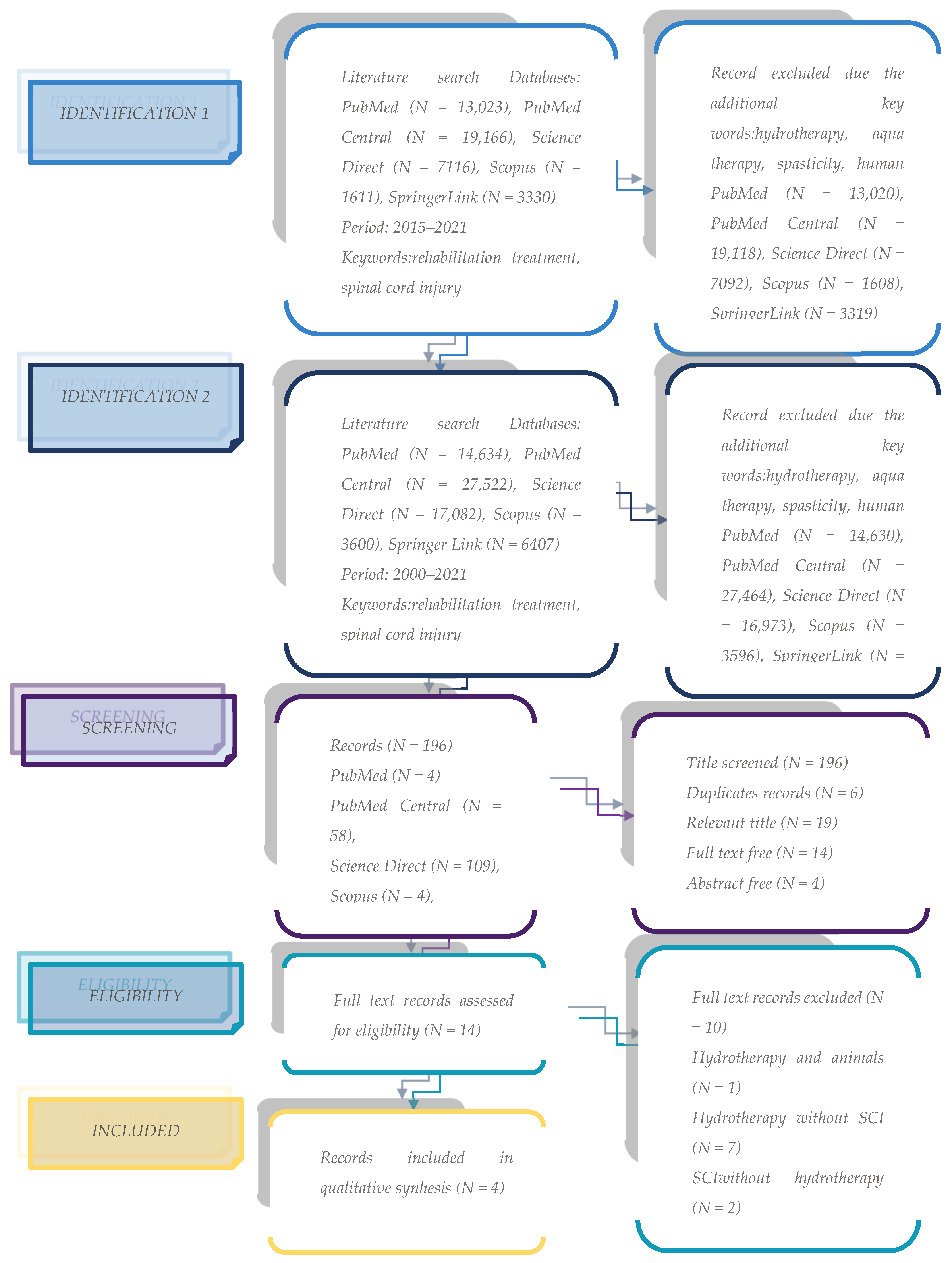
2. Methods
- (1)
- Population (patients with neuromotor or neuromuscular deficits due to spinal cord injury);
- (2)
- Intervention (hydrotherapy/aqua therapy).
3. Results

{kind=link}
| Downs and Black Appraisal | ||||||
|---|---|---|---|---|---|---|
| Authors | Reporting (n = 5) | External Validity (n = 3) | Internal Validity (n = 3) | Power (n = 5) | Total (n =16) | Grading % = x/16 × 100 |
| N. Kesiktas, N. Paker, N. Erdogan, G. Gülsen, D. Biçki, and H. Yilmaz (2004) [1] | 5 | 3 | 2 | 4 | 14 | 87.5 % (very good) |
| C. Li, S. Khoo, A. Adnan (2017) [19] | 5 | 3 | 3 | 4 | 15 | 93.75% (very good) |
| T. J. Ellapen, H. V. Hammill, M. Swanepoel, G. L. Strydom (2018) [20] | 5 | 3 | 3 | 4 | 15 | 93.75% (very good) |
| A. R. Marinho-Buzelli, A. J. Zaluski, A. Mansfield, A. M. Bonnyman, K. E. Musselman (2019) [22] | 5 | 1 | 3 | 3 | 11 | 68.75% (fair) |
| Characteristics of the Study | ||||
|---|---|---|---|---|
| Authors | Type of Study | Sample | Method | Findings |
| N. Kesiktas, N. Paker, N. Erdogan, G. Gülsen, D. Biçki, and H. Yilmaz (2004) [1] | Experimental non-randomised control | Hydrotherapy group: 10, mean age 32.13 ± 8.34, gender: 2 females and 8 males, injury time (months): 8.6 ± 5.5, FIM: 52 ± 14.13, Ashworth Score 3 ± 0.92, Oral Baclofen (mg) 96 ± 12, Etiology (accident) 50%. Control group: 10, mean age 33.10 ± 10.71, gender: 3 females and 7 males, injury time (months): 7.70 ± 6.06, FIM: 54.70 ± 18.8, Ashworth Score 2.50 ± 1.18, Oral Baclogen (mg) 100 ± 0, Etiology (accident) 50%. | The hydrotherapy group received 20 min of underwater exercises at 71 º F (21.6 º C) 3 times/week, and also participated in the usual rehabilitation, which included passive range of motion 2 times/day, psychotherapy and oral baclofen for 10 weeks. The control group were able to maintain their usual activities through the conventional rehabilitation program. | The hydrotherapeutic intervention successfully reduced spasticity and oral baclofen doses and raised FIM scores compared to control group. |
| C. Li, S. Khoo, A. Adnan (2017) [19] | Systematic review | A total of 143 participants with SCI were reported and the sample size of each study ranged from 1 to 60. More male participants were reported than female (male = 91, female = 52). Participants were adults aged between 18 and 63 years. A total of seven of eight studies reported participants’ injury levels on the spinal cord (the study by Pachalski and Mekarski did not report the specific injury level). Only 4 studies provided the grade of ASIA impairment scale. There was a big range in terms of postinjury time from 7 months to 28 years. In terms of study design, 3 were controlled clinical trials, 2 single group test–retest designs, 1 randomized controlled trial, 1 single-subject design, and 1 case study. | Eight of 276 studies met the inclusion criteria, of which none showed high research quality. Four studies assessed physical function outcomes and 4 studies evaluated aerobic fitness as outcome measures. Significant improvements on these 2 outcomes were generally found. Other physical or fitness outcomes including body composition, muscular strength, and balance were rarely reported. | There is insufficient evidence to support the efficacy of aquatic exercise on increasing physical function and aerobic fitness among SCI patients. We cannot yet draw any conclusion about the effectiveness of underwater training on body composition, muscular strength, and balance among the study population. |
| T. J. Ellapen, H. V. Hammill, M. Swanepoel, G. L. Strydom (2018) [20] | Systematic review | A total of 142 participants were reported (but 83 PWSCI), with sample sizes varying from 1 to 30 and participant age varying from 5 to 70 years. Five studies provided kinanthropometric characteristics, whereas 5 studies considered the number of years injured, and 10 studies described the aquatic exercise intervention. The overall quality of the studies was rated as fair (62.0%). | A literature surveillance was conducted between 1998 and 2017, through the Crossref meta-database and Google Scholar, according to the PRISMA procedures. Key search words were water-therapy, aquatic-therapy, hydrotherapy, spinal cord injury, rehabilitation, human, kinematics, underwater gait, cardiorespiratory, thermoregulation and spasticity. The quality of each paper was evaluated using a modified Downs and Black Appraisal Scale. The participants were recorded pertaining to SCI and hydrotherapy. The outcomes of interest were hydrotherapy interventions, the impact of hydrotherapy on gait kinematics, thermoregulation during water submersion, and cardiorespiratory function of PWSCI. | Hydrotherapy increases PWSCI underwater gait kinematics, cardiorespiratory and thermoregulatory responses and reduces spasticity. |
| A. R. Marinho-Buzelli, A. J. Zaluski, A. Mansfield, A. M. Bonnyman, K. E. Musselman (2019) [22] | Individual semi-structured interviews | None mentioned. | Six PT (2 male, 4 female), three PTA (female) and 1 KIN (female) participated. The following four themes were identified: (1) multi-system benefits from AT (e.g., from impairment to function, confidence, and enjoyment); (2) application of AT; (3) perceived barriers to implementing AT; and (4) water as an enabler to function on land. All were interviewed regarding their clinical findings while working with SCI patients in aquatic environment. | The participants reported AT was a unique and fickle approach that benefits the multi-dimensional aspects of the health of individuals with SCI/D. They inserted AT very well into their clinical practice despite the barriers professionals and clients face. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kesiktas, N.; Paker, N.; Erdogan, N.; Gülsen, G.; Biçki, D.; Yilmaz, H.G. The use of hydrotherapy for the management of spasticity. Neurorehabil. Neural Repair 2004, 18, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Priebe, M.M.; Sherwood, A.M.; Thornby, J.I.; Kharas, N.F.; Markowski, J. Clinical assessment of spasticity in spinal cord injury: A multidimensional problem. Arch. Phys. Med. Rehabil. 1996, 77, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Hippocrates. On Airs, Waters, and Places. 400 BC. Available online: http://classics.mit.edu/Hippocrates/airwatpl.html (accessed on 11 January 2022).
- Kneipp, S. My Water Cure, as Tested through more than Thirty Years, and Described for the Healing of Diseases and the Preservation of Health, 30th ed.; William Blackwood&Sons: Edinburgh, UK, 1894. [Google Scholar]
- Hall, J.; Swinkels, A.; Briddon, J.; McCabe, C.S. Does aquatic exercisere lieve pain in adults with neurologic or musculoskeletal disease? A systematic reviewand meta-analysis of randomized controlled trials. ArchPhys. Med. Rehabil. 2008, 89, 873–883. [Google Scholar] [CrossRef]
- Bender, T.; Karaglle, Z.; Balint, G.P.; Gutenbrunner, C.; Balint, P.V.; Sukenik, S. Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatol. Int. 2005, 25, 220–224. [Google Scholar] [CrossRef]
- Yamazaki, F.; Endo, Y.; Torii, S.; Sagawa, S.; Shiraki, K. Continuous monitoring of change in hemodilution during water immersion in humans: Effect of water temperature. Aviat. Space Environ. Med. 2000, 71, 632–639. [Google Scholar] [PubMed]
- Gabrielsen, A.; Ek, V.A.; Johansen, L.B.; Warberg, J.; Christensen, N.J.; Pump, B.; Norsk, P. Forearm vascular and neuroendocrine responses to graded water immersion in humans. Acta PhysioScand 2000, 169, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Fam, A.G. Spa treatment in arthritis: A rheumarologist’s view. J. Rheumatol. 1991, 18, 1775–1777. [Google Scholar] [PubMed]
- Giesecke, C. Aquatic rehabilitation of clients with spinal cord injury. In Aquatic Rehabilitation; Ruoti, R.G., Morris, D.M., Cole, A.J., Eds.; Lippincott, Williams andWilkins: Hagerstown, MD, USA, 1997; pp. 125–150. [Google Scholar]
- Stiens, S.A.; Biener-Bergman, S.; Goetz, L.L. Neurogenic boweldys function after spinal cord injury: Clinical evaluation and rehabilitation management. ArchPhys. Med. Rehab. 1997, 78, S86–S102. [Google Scholar] [CrossRef]
- Recio, A.C.; Cabahug, P. Safety of aquatic therapy for adults with complex medical conditions among chronic spinal cord injury. In Proceedings of the ASCIP Annual Meeting, Nashville, TN, USA, 4–7 September 2016; pp. 568–569. [Google Scholar]
- Stiens, S.A.; Shamberg, S.; Shamberg, A.; Guistini, A. Environ mental barriers: Solutions to participation, collaboration and to getherness. In Physical Medicine and Rehabilitation Secrets, 3rd ed.; O’Young, B.J., Young, M.A., Stiens, S.A., Eds.; Mosby: St. Louis, MI, USA, 2007; pp. 76–85. [Google Scholar]
- Stiens, S.A.; O’Young, B.J.; Young, M.A. Person-centered rehabilitation: Interdisciplinary intervention to enhance patient enablement, physical medicine and rehabilitation secrets. In Physical Medicine and Rehabilitation Secrets, 3rd ed.; O’Young, B.J., Young, M.A., Stiens, S.A., Eds.; Mosby: St. Louis, MI, USA, 2007; pp. 118–125. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomized and nonrandomized studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Machado, M.; Bajcar, J.; Guzzo, G.C.; Einarson, T.R. Sensitivity of patient out comes to pharmacist interventions. Part II: Systematic reviewand meta-analysis in hypertension management. Ann. Pharmacother. 2007, 41, 1770–1781. [Google Scholar] [CrossRef] [PubMed]
- Kamioka, H.; Tsutani, K.; Okuizumi, H.; Mutoh, Y.; Ohta, M.; Handa, S.; Okada, S.; Kitayuguchi, J.; Kamada, M.; Shiozawa, N.; et al. A systematic review of nonrandomized controlled trials on the curative effects of aquatic exercise. Int. J. Gen. Med. 2011, 4, 239–260. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Khoo, S.; Adnan, A. Effects of aquatic exercise on physical function and fitness among people with spinal cord injury. Medicine 2017, 96, e6328. [Google Scholar] [CrossRef] [PubMed]
- Ellapen, T.J.; Hammill, H.V.; Swanepoel, M.; Strydom, G.L. Strydom, The benefits of hydrotherapy to patients with spinal cord injuries. Afr. J. Disabil. 2018, 7, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamparo, P.; Pagliaro, P. The energy cost of level walking before and after hydro-kinesi therapy in patients with spastic paresis. Scand. Med. Sci. Sport 2007, 8, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Marinho-Buzelli, A.R.; Zaluski, A.J.; Mansfield, A.; Bonnyman, A.M.; Musselman, K.E. The use of aquatic therapy among rehabilitation professionals for individuals with spinal cord injury or disorde. J. Spinal. Cord. Med. 2019, 42 (Suppl. 1), 158–165. [Google Scholar] [CrossRef] [PubMed]
- Wall, T.; Falvo, L.; Kesten, A. Activity-specific aquatic therapy targeting gait for a patient with incomplete spinal cord injury. Physiother. Theory Pract. 2017, 33, 331–344. [Google Scholar] [CrossRef]
- Munteanu, C. Therapeutic Mineral Waters; Balneary: Bucharest, Romania, 2013; ISBN 978-606-93550-6-0. [Google Scholar]
- Rekand, T.; Hagen, E.; Grønning, M. Marit Grønning, Spasticity following spinal cord injury. Tidsskr. Nor. Legeforen. 2012, 132, 970–973. [Google Scholar] [CrossRef] [Green Version]
- Adams, M.M.; Hicks, A.L. Spasticity after Spinal Cord Injury. Spinal Cord 2005, 43, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Holtz, K.A.; Lipson, R.; Noonan, V.K.; Kwon, B.K.; Mills, P.B. The prevalence and Effect of Problematic Spasticity After Traumatic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2017, 98, 1132–1138. [Google Scholar] [CrossRef]
- Cragg, J.J.; Noonan, V.K.; Krassioukov, A.; Borisoff, J. Cardiovascular disease and spinal cord injury. Neurology 2013, 81, 723–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myers, J.; Lee, M.; Kiratli, J. Cardiovascular Disease in Spinal Cord Injury An Overview of Prevalence, Risk, Evaluation, and Management. Am. J. Phys. Med. Rehabil. 2007, 86, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Dulberg, C.; Wells, G. Statistical power, sample size and their reporting in randomized controlled trials. J. Am. Med. Assoc. 1994, 272, 122Y124. [Google Scholar] [CrossRef]
- Schulz, K. Randomized trials, human nature, and reporting guidelines. Lancet 1996, 348, 562. [Google Scholar] [CrossRef] [PubMed]
- Day, S.; Altman, D. Blinding to clinical trials and other studies. Br. Med. J. 2000, 321, 504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gasmi, A.; Bjorklund, G.; Mujawdiya, P.K.; Semenova, Y.; Peana, M.; Dosa, A.; Piscopo, S.; Benahmed, A.G.; Costea, D.O. Micronutrients deficiencies in patients after bariatric surgery. Eur. J. Nutr. 2021, 61, 55–67. [Google Scholar] [CrossRef]
- Głowiński, S.; Ptak, M. A kinematic model of a humanoid lower limb exoskeleton with pneumatic actuators. Acta Bioeng. Biomech. 2022, 24, 145–157. [Google Scholar] [CrossRef]
- Pons, J.L. Wearable Robots; John Wiley & Sons, Ltd.: Chichester, UK, 2008; ISBN 9780470987667. [Google Scholar]
- Stevenson, V.L. Rehabilitation in practice: Spasticity management. Clin. Rehabil. 2010, 24, 293–304. [Google Scholar] [CrossRef]
- Little, J.W.; Micklesen, P.; Umlauf, R.; Britell, C. Lower extremitiy manifestations in spasticity in chronic spinal cord injury. Am. J. Phys. Med. Rehabil. 1989, 68, 32–36. [Google Scholar] [CrossRef]
- Horga Parte, J.F.; Pareés, M.I. Toxina botulínica: Origen, estructura, actividad farmacológica y cinética. In Toxina Botulínica; López, d.V.L.J., Castor, G.A., Eds.; Elsevier España: Barcelona, Spain, 2010; pp. 3–17. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanciu, L.E.; Iliescu, M.G.; Vlădăreanu, L.; Ciota, A.E.; Ionescu, E.-V.; Mihailov, C.I. Evidence of Improvement of Lower Limb Functioning Using Hydrotherapy on Spinal Cord Injury Patients. Biomedicines 2023, 11, 302. https://doi.org/10.3390/biomedicines11020302
Stanciu LE, Iliescu MG, Vlădăreanu L, Ciota AE, Ionescu E-V, Mihailov CI. Evidence of Improvement of Lower Limb Functioning Using Hydrotherapy on Spinal Cord Injury Patients. Biomedicines. 2023; 11(2):302. https://doi.org/10.3390/biomedicines11020302
Chicago/Turabian StyleStanciu, Liliana Elena, Madalina Gabriela Iliescu, Liliana Vlădăreanu, Alexandra Ecaterina Ciota, Elena-Valentina Ionescu, and Claudia Ileana Mihailov. 2023. "Evidence of Improvement of Lower Limb Functioning Using Hydrotherapy on Spinal Cord Injury Patients" Biomedicines 11, no. 2: 302. https://doi.org/10.3390/biomedicines11020302