
Patisiran Enhances Muscle Mass after Nine Months of Treatment in ATTRv Amyloidosis: A Study with Bioelectrical Impedance Analysis and Handgrip Strength

 ,
,  ,
,  , , , , , , , , and
, , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Procedures
2.2. Patient Demographics and Clinical Features
2.3. Coutinho Stage
2.4. Neuropathy Impairment Score (NIS)
2.5. Karnofsky Performance Status (KPS)
2.6. Norfolk QOL Questionnaire
2.7. Six-Minute Walking Test (6MWT)
2.8. Nerve Conduction Studies (NCSs)
2.9. Handgrip Test
2.10. Bioelectrical Impedance Analysis (BIA)
2.11. Statistical Analysis
3. Results
3.1. Clinical and Neurophysiological Evaluation
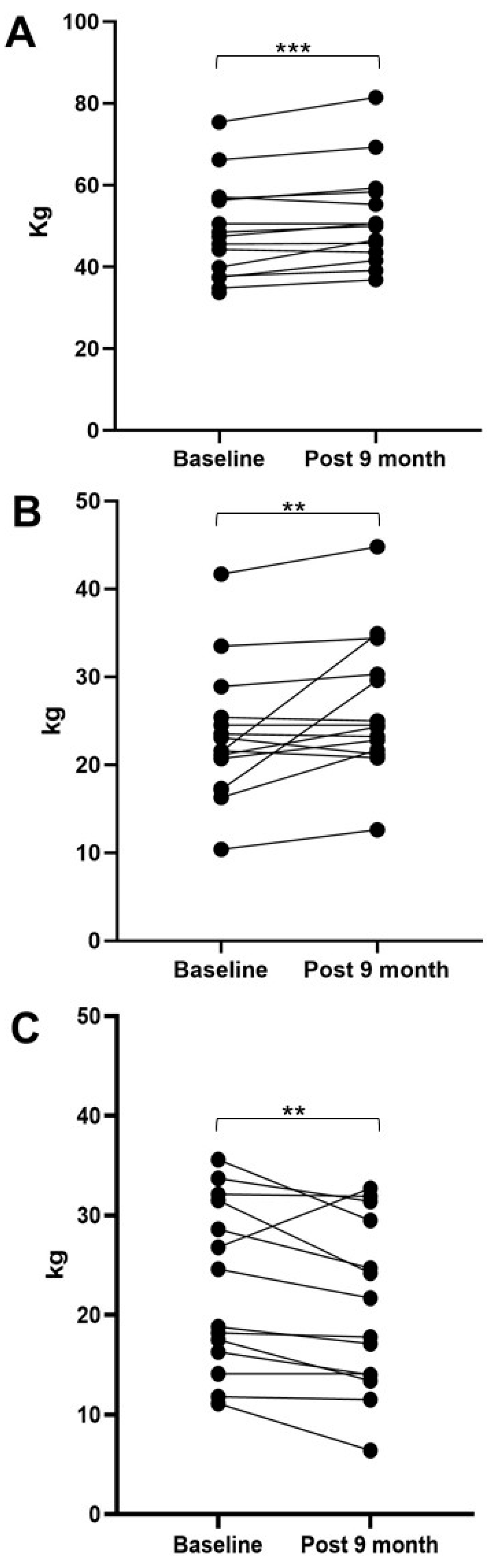
3.2. Bioelectrical Impedance Analysis (BIA)
3.3. Handgrip Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adams, D.; Ando, Y.; Beirão, J.M.; Coelho, T.; Gertz, M.A.; Gillmore, J.D.; Hawkins, P.N.; Lousada, I.; Suhr, O.B. Expert consensus recommendations to improve diagnosis of ATTR amyloidosis with polyneuropathy. J. Neurol. 2021, 268, 2109–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waddington-Cruz, M.; Schmidt, H.; Botteman, M.F.; Carter, J.A.; Stewart, M.; Hopps, M.; Fallet, S.; Amass, L. Epidemiological and clinical characteristics of symptomatic hereditary transthyretin amyloid polyneuropathy: A global case series. Orphanet J. Rare Dis. 2019, 14, 34. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.H.; Waddington-Cruz, M.; Botteman, M.F.; Carter, J.; Chopra, A.S.; Hopps, M.; Stewart, M.; Fallet, S.; Amass, L. Estimating the global prevalence of transthyretin familial amyloid polyneuropathy. Muscle Nerve 2018, 57, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Adyan, T.A.; Polyakov, A.V. Hereditary transthyretin amyloidosis. Nervn.-Myshechnye Bolezni. 2019, 9, 12–25. [Google Scholar] [CrossRef] [Green Version]
- Koike, H.; Iguchi, Y.; Sahashi, K.; Katsuno, M. Significance of Oligomeric and Fibrillar Species in Amyloidosis: Insights into Pathophysiology and Treatment. Molecules 2021, 26, 5091. Available online: https://pubmed.ncbi.nlm.nih.gov/34443678/ (accessed on 22 December 2022). [CrossRef]
- Russo, M.; Obici, L.; Bartolomei, I.; Cappelli, F.; Luigetti, M.; Fenu, S.; Cavallaro, T.; Chiappini, M.G.; Gemelli, C.; Pradotto, L.G.; et al. ATTRv amyloidosis Italian Registry: Clinical and epidemiological data. Amyloid 2020, 27, 259–265. Available online: https://pubmed.ncbi.nlm.nih.gov/32696671/ (accessed on 22 December 2022). [CrossRef]
- Mazzeo, A.; Russo, M.; Di Bella, G.; Minutoli, F.; Stancanelli, C.; Gentile, L.; Baldari, S.; Carerj, S.; Toscano, A.; Vita, G. Transthyretin-Related Familial Amyloid Polyneuropathy (TTR-FAP): A Single-Center Experience in Sicily, an Italian Endemic Area. J. Neuromuscul. Dis. 2015, 2, S39–S48. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27858761 (accessed on 22 December 2022). [CrossRef] [Green Version]
- Koike, H.; Misu, K.I.; Ikeda, S.I.; Ando, Y.; Nakazato, M.; Ando, E.; Yamamoto, M.; Hattori, N.; Sobue, G. Type I (transthyretin Met30) familial amyloid polyneuropathy in Japan: Early-vs. late-onset form. Arch. Neurol. 2002, 59, 1771–1776. Available online: https://pubmed.ncbi.nlm.nih.gov/12433265/ (accessed on 22 December 2022). [CrossRef] [Green Version]
- Rintell, D.; Heath, D.; Mendendez, F.B.; Cross, E.; Cross, T.; Knobel, V.; Gagnon, B.; Turtle, C.; Cohen, A.; Kalmykov, E.; et al. Patient and family experience with transthyretin amyloid cardiomyopathy (ATTR-CM) and polyneuropathy (ATTR-PN) amyloidosis: Results of two focus groups. Orphanet J. Rare Dis. 2021, 16, 70. [Google Scholar] [CrossRef]
- Russo, M.; Gentile, L.; Di Stefano, V.; Di Bella, G.; Minutoli, F.; Toscano, A.; Brighina, F.; Vita, G.; Mazzeo, A. Use of Drugs for ATTRv Amyloidosis in the Real World: How Therapy Is Changing Survival in a Non-Endemic Area. Brain Sci. 2021, 11, 545. [Google Scholar] [CrossRef]
- Adams, D.; Polydefkis, M.; González-Duarte, A.; Wixner, J.; Kristen, A.V.; Schmidt, H.H.; Berk, J.L.; López, I.A.L.; Dispenzieri, A.; Quan, D.; et al. Long-term safety and efficacy of patisiran for hereditary transthyretin-mediated amyloidosis with polyneuropathy: 12-month results of an open-label extension study. Lancet Neurol. 2021, 20, 49–59. Available online: https://pubmed.ncbi.nlm.nih.gov/33212063/ (accessed on 22 December 2022). [CrossRef] [PubMed]
- Di Stefano, V.; Fava, A.; Gentile, L.; Guaraldi, P.; Leonardi, L.; Poli, L.; Tagliapietra, M.; Vastola, M.; Fanara, S.; Ferrero, B.; et al. Italian Real-Life Experience of Patients with Hereditary Transthyretin Amyloidosis Treated with Patisiran. Pharmgenomics Pers. Med. 2022, 15, 499–514. Available online: https://pubmed.ncbi.nlm.nih.gov/35592550/ (accessed on 22 December 2022). [CrossRef] [PubMed]
- Dohrn, M.F.; Auer-Grumbach, M.; Baron, R.; Birklein, F.; Escolano-Lozano, F.; Geber, C.; Grether, N.; Hagenacker, T.; Hund, E.; Sachau, J.; et al. Chance or challenge, spoilt for choice? New recommendations on diagnostic and therapeutic considerations in hereditary transthyretin amyloidosis with polyneuropathy: The German/Austrian position and review of the literature. J. Neurol. 2021, 268, 3610–3625. [Google Scholar] [CrossRef] [PubMed]
- Ando, Y.; Adams, D.; Benson, M.D.; Berk, J.L.; Planté-Bordeneuve, V.; Coelho, T.; Conceição, I.; Ericzon, B.G.; Obici, L.; Rapezzi, C.; et al. Guidelines and new directions in the therapy and monitoring of ATTRv amyloidosis. Amyloid. 2022, 29, 143–155. [Google Scholar] [CrossRef]
- Luigetti, M.; Di Paolantonio, A.; Guglielmino, V.; Romano, A.; Rossi, S.; Sabino, A.; Servidei, S.; Sabatelli, M.; Primiano, G. Neurofilament light chain as a disease severity biomarker in ATTRv: Data from a single-centre experience. Neurol. Sci. 2022, 43, 2845–2848. Available online: https://pubmed.ncbi.nlm.nih.gov/35094171/ (accessed on 22 December 2022). [CrossRef]
- Stefano, V.D.; Thomas, E.; Giustino, V.; Iacono, S.; Torrente, A.; Pillitteri, G.; Gagliardo, A.; Lupica, A.; Palma, A.; Battaglia, G.; et al. Motor Conduction Studies and Handgrip in Hereditary TTR Amyloidosis: Simple Tools to Evaluate the Upper Limbs. Front. Neurol. 2022, 13, 835812. Available online: https://pubmed.ncbi.nlm.nih.gov/35295833/ (accessed on 22 December 2022). [CrossRef]
- Ribom, E.L.; Mellström, D.; Ljunggren, Ö.; Karlsson, M.K. Population-based reference values of handgrip strength and functional tests of muscle strength and balance in men aged 70–80 years. Arch. Gerontol. Geriatr. 2011, 53, e114–e117. [Google Scholar] [CrossRef]
- Lee, S.H.; Gong, H.S. Measurement and Interpretation of Handgrip Strength for Research on Sarcopenia and Osteoporosis. J. Bone Metab. 2020, 27, 85–96. Available online: https://pubmed.ncbi.nlm.nih.gov/32572369/ (accessed on 22 December 2022). [CrossRef]
- Oh, T.J.; Kang, S.; Lee, J.-E.; Moon, J.H.; Choi, S.H.; Lim, S.; Jang, H.C. Association between deterioration in muscle strength and peripheral neuropathy in people with diabetes. J. Diabetes its Complicat. 2019, 33, 598–601. Available online: https://pubmed.ncbi.nlm.nih.gov/31129004/ (accessed on 22 December 2022). [CrossRef]
- Thevarajah, N.; Sadagatullah, A.N.; Anbarasan, A. The Functional Outcome of Mini Carpal Tunnel Release. J. Hand Microsurg. 2017, 09, 006–010. Available online: https://pubmed.ncbi.nlm.nih.gov/28442855/ (accessed on 22 December 2022). [CrossRef]
- Piscosquito, G.; Reilly, M.M.; Schenone, A.; Fabrizi, G.M.; Cavallaro, T.; Santoro, L.; Manganelli, F.; Vita, G.; Quattrone, A.; Padua, L.; et al. Responsiveness of clinical outcome measures in Charcot−Marie−Tooth disease. Eur. J. Neurol. 2015, 22, 1556–1563. Available online: https://pubmed.ncbi.nlm.nih.gov/26227902/ (accessed on 22 December 2022). [CrossRef] [PubMed]
- Gertz, M.; Adams, D.; Ando, Y.; Beirão, J.M.; Bokhari, S.; Coelho, T.; Comenzo, R.L.; Damy, T.; Dorbala, S.; Drachman, B.M.; et al. Avoiding misdiagnosis: Expert consensus recommendations for the suspicion and diagnosis of transthyretin amyloidosis for the general practitioner. BMC Fam. Pract. 2020, 21, 198. [Google Scholar] [CrossRef] [PubMed]
- Luigetti, M.; Tortora, A.; Romano, A.; Di Paolantonio, A.; Guglielmino, V.; Bisogni, G.; Gasbarrini, A.; Calabresi, P.; Sabatelli, M. Gastrointestinal Manifestations in Hereditary Transthyretin Amyloidosis: A Single-Centre Experience. J. Gastrointest. Liver Dis. 2020, 29, 339–343. Available online: https://pubmed.ncbi.nlm.nih.gov/32919418/ (accessed on 22 December 2022). [CrossRef] [PubMed]
- Rezk, T.; Davenport, A.; Gan, J.J.; Lachmann, H.J.; Fontana, M.; Martinez-Naharro, A.; Sachchithanantham, S.; Guillotte, C.; Mahmood, S.; Petrie, A.; et al. Bioimpedance vector analysis for the detection of extracellular volume overload and sarcopenia in systemic AL amyloidosis. Br. J. Haematol. 2019, 185, 977–980. Available online: https://pubmed.ncbi.nlm.nih.gov/30450572/ (accessed on 22 December 2022). [CrossRef] [Green Version]
- Yasemin, Ö.; Seydahmet, A.; Özcan, K. Relationship between diabetic neuropathy and sarcopenia. Prim. Care Diabetes 2019, 13, 521–528. Available online: https://pubmed.ncbi.nlm.nih.gov/31126745/ (accessed on 22 December 2022). [CrossRef]
- Gentile, L.; Russo, M.; Luigetti, M.; Bisogni, G.; Di Paolantonio, A.; Romano, A.; Guglielmino, V.; Arimatea, I.; Sabatelli, M.; Toscano, A.; et al. Patisiran in hATTR Amyloidosis: Six-Month Latency Period before Efficacy. Brain Sci. 2021, 11, 515. Available online: https://pubmed.ncbi.nlm.nih.gov/33921571/ (accessed on 22 December 2022). [CrossRef]
- Mundayat, R.; Stewart, M.; Alvir, J.; Short, S.; Ong, M.-L.; Keohane, D.; Rill, D.; Sultan, M.B. Positive Effectiveness of Tafamidis in Delaying Disease Progression in Transthyretin Familial Amyloid Polyneuropathy up to 2 Years: An Analysis from the Transthyretin Amyloidosis Outcomes Survey (THAOS). Neurol. Ther. 2018, 7, 87–101. Available online: https://pubmed.ncbi.nlm.nih.gov/29633228/ (accessed on 22 December 2022). [CrossRef]
- Vinik, E.J.; Hayes, R.P.; Oglesby, A.; Bastyr, E.; Barlow, P.; Ford-Molvik, S.L.; Vinik, A.I. The development and validation of the Norfolk QOL-DN, a new measure of patients’ perception of the effects of diabetes and diabetic neuropathy. Diabetes Technol. Ther. 2005, 7, 497–508. Available online: https://pubmed.ncbi.nlm.nih.gov/15929681/ (accessed on 22 December 2022). [CrossRef]
- Merkies, I.S. Tafamidis for transthyretin familial amyloid polyneuropathy: A randomized, controlled trial. Neurology 2013, 80, 1444–1445. Available online: https://pubmed.ncbi.nlm.nih.gov/23569001/ (accessed on 22 December 2022). [CrossRef] [Green Version]
- Benson, M.D.; Waddington-Cruz, M.; Berk, J.L.; Polydefkis, M.; Dyck, P.J.; Wang, A.K.; Planté-Bordeneuve, V.; Barroso, F.A.; Merlini, G.; Obici, L.; et al. Inotersen Treatment for Patients with Hereditary Transthyretin Amyloidosis. N. Engl. J. Med. 2018, 379, 22–31. Available online: https://pubmed.ncbi.nlm.nih.gov/29972757/ (accessed on 22 December 2022). [CrossRef]
- Obici, L.; Berk, J.L.; González-Duarte, A.; Coelho, T.; Gillmore, J.; Schmidt, H.H.-J.; Schilling, M.; Yamashita, T.; Labeyrie, C.; Iii, T.H.B.; et al. Quality of life outcomes in APOLLO, the phase 3 trial of the RNAi therapeutic patisiran in patients with hereditary transthyretin-mediated amyloidosis. Amyloid 2020, 27, 153–162. Available online: https://pubmed.ncbi.nlm.nih.gov/32131641/ (accessed on 22 December 2022). [CrossRef] [PubMed] [Green Version]
- Adams, D.; Tournev, I.L.; Taylor, M.S.; Coelho, T.; Planté-Bordeneuve, V.; Berk, J.L.; González-Duarte, A.; Gillmore, J.D.; Low, S.-C.; Sekijima, Y.; et al. Efficacy and safety of vutrisiran for patients with hereditary transthyretin-mediated amyloidosis with polyneuropathy: A randomized clinical trial. Amyloid 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. Available online: https://pubmed.ncbi.nlm.nih.gov/31689414/ (accessed on 22 December 2022). [CrossRef] [PubMed]
- Tomás, M.T.; Santa-Clara, M.H.; Monteiro, E.; Baynard, T.; Carnero, E.A.; Bruno, P.M.; Barroso, E.; Sardinha, L.B.; Fernhall, B. Body composition, muscle strength, functional capacity, and physical disability risk in liver transplanted familial amyloidotic polyneuropathy patients. Clin. Transplant. 2011, 25, E406–E414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vita, G.L.; Stancanelli, C.; Gentile, L.; Barcellona, C.; Russo, M.; Di Bella, G.; Vita, G.; Mazzeo, A. 6MWT performance correlates with peripheral neuropathy but not with cardiac involvement in patients with hereditary transthyretin amyloidosis (hATTR). Neuromuscul. Disord. 2019, 29, 213–220. Available online: https://pubmed.ncbi.nlm.nih.gov/30718023/ (accessed on 22 December 2022). [CrossRef] [PubMed] [Green Version]
- Crapo, R.O.; Casaburi, R.; Coates, A.L.; Enright, P.L.; MacIntyre, N.R.; McKay, R.T. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. Available online: https://pubmed.ncbi.nlm.nih.gov/12091180/ (accessed on 22 December 2022).
- Di Stefano, V.; Gagliardo, A.; Barbone, F.; Vitale, M.; Ferri, L.; Lupica, A.; Iacono, S.; Di Muzio, A.; Brighina, F. Median-to-Ulnar Nerve Communication in Carpal Tunnel Syndrome: An Electrophysiological Study. Neurol. Int. 2021, 13, 304–314. [Google Scholar] [CrossRef]
- Spijkerman, D.C.; Snijders, C.J.; Stijnen, T.; Lankhorst, G.J. Standardization of grip strength measurements. Effects on repeatability and peak force. Scand. J. Rehabilitation Med. 1991, 23, 203–206. Available online: https://pubmed.ncbi.nlm.nih.gov/1785029/ (accessed on 22 December 2022).
- Bonaventura, R.E.; Giustino, V.; Chiaramonte, G.; Giustiniani, A.; Smirni, D.; Battaglia, G.; Messina, G.; Oliveri, M. Investigating prismatic adaptation effects in handgrip strength and in plantar pressure in healthy subjects. Gait Posture 2020, 76, 264–269. Available online: https://pubmed.ncbi.nlm.nih.gov/31881480/ (accessed on 22 December 2022). [CrossRef]
- Aleixo, G.F.; Shachar, S.S.; Nyrop, K.A.; Muss, H.B.; Battaglini, C.L.; Williams, G.R. Bioelectrical Impedance Analysis for the Assessment of Sarcopenia in Patients with Cancer: A Systematic Review. Oncologist 2019, 25, 170–182. Available online: https://pubmed.ncbi.nlm.nih.gov/32043785/ (accessed on 22 December 2022). [CrossRef]
- Kim, W.; Park, S.-H.; Kim, W.-S.; Jang, W.Y.; Park, E.J.; Kang, D.O.; Park, Y.; Na, J.O.; Kim, J.W.; Kim, E.J.; et al. Handgrip Strength as a Predictor of Exercise Capacity in Coronary Heart Disease. J. Cardiopulm. Rehabilitation Prev. 2020, 40, E10–E13. Available online: https://pubmed.ncbi.nlm.nih.gov/32118655/ (accessed on 22 December 2022). [CrossRef] [PubMed]


{kind=link}
| Baseline | Post 9 Month | p | |
|---|---|---|---|
| Age (years) | 66.4 ± 7.8 | 66.9 ± 7.7 | ns |
| Height (cm) | 163.0 ± 10.9 | 163.0 ± 10.9 | ns |
| Weight (kg) | 70.3 ± 19.8 | 73.1 ± 21.1 | 0.044 |
| Baseline | Post 9 Month | p | |
|---|---|---|---|
| Clinical evaluation | |||
| FAP stage | 1.13 ± 0.5 | 1.13 ± 0.5 | ns |
| Karnofski performance status | 72.7 ± 13.8 | 75.3 ± 14.1 | ns |
| NIS | 30.9 ± 29.2 | 31.4 ± 25.6 | ns |
| NIS-W | 14.6 ± 17.8 | 14.7 ± 14.5 | ns |
| Norfolk | 51.0 ± 31.6 | 47.8 ± 29.5 | ns |
| COMPASS-31 | 18.9 ± 9.1 | 19.8 ± 9.2 | ns |
| 6MWT (m) | 229.6 ± 72.6 | 260.9 ± 69.8 | 0.033 |
| Body Composition | |||
| FFM (kg) | 48.8 ± 11.9 | 52.0 ± 12.1 | 0.005 |
| BCM (kg) | 23.1 ± 7.5 | 26.4 ± 7.8 | 0.014 |
| FM (kg) | 21.5 ± 9.8 | 20.7 ± 8.5 | 0.012 |
| TBW (l) | 36.5 ± 9.2 | 38.4 ± 9.1 | ns |
| ECW (l) | 19.0 ± 4.9 | 18.7 ± 4.5 | ns |
| Strength | |||
| HG R | 20.6 ± 13.8 | 21.4 ± 13.9 | ns |
| HG L | 22.5 ± 11.8 | 22.1 ± 10.9 | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, V.; Thomas, E.; Alonge, P.; Giustino, V.; Pillitteri, G.; Leale, I.; Torrente, A.; Pignolo, A.; Norata, D.; Iacono, S.; et al. Patisiran Enhances Muscle Mass after Nine Months of Treatment in ATTRv Amyloidosis: A Study with Bioelectrical Impedance Analysis and Handgrip Strength. Biomedicines 2023, 11, 62. https://doi.org/10.3390/biomedicines11010062
Di Stefano V, Thomas E, Alonge P, Giustino V, Pillitteri G, Leale I, Torrente A, Pignolo A, Norata D, Iacono S, et al. Patisiran Enhances Muscle Mass after Nine Months of Treatment in ATTRv Amyloidosis: A Study with Bioelectrical Impedance Analysis and Handgrip Strength. Biomedicines. 2023; 11(1):62. https://doi.org/10.3390/biomedicines11010062
Chicago/Turabian StyleDi Stefano, Vincenzo, Ewan Thomas, Paolo Alonge, Valerio Giustino, Guglielmo Pillitteri, Ignazio Leale, Angelo Torrente, Antonia Pignolo, Davide Norata, Salvatore Iacono, and et al. 2023. "Patisiran Enhances Muscle Mass after Nine Months of Treatment in ATTRv Amyloidosis: A Study with Bioelectrical Impedance Analysis and Handgrip Strength" Biomedicines 11, no. 1: 62. https://doi.org/10.3390/biomedicines11010062