
Erectile Dysfunction: Pharmacological Pathways with Understudied Potentials
{kind=link}
Abstract
:1. Introduction
1.1. Epidemiology
1.2. Risk Factors
1.3. Etiology
1.4. Pathophysiology
2. Assessment
2.1. Animal Models
2.2. Human Subjects
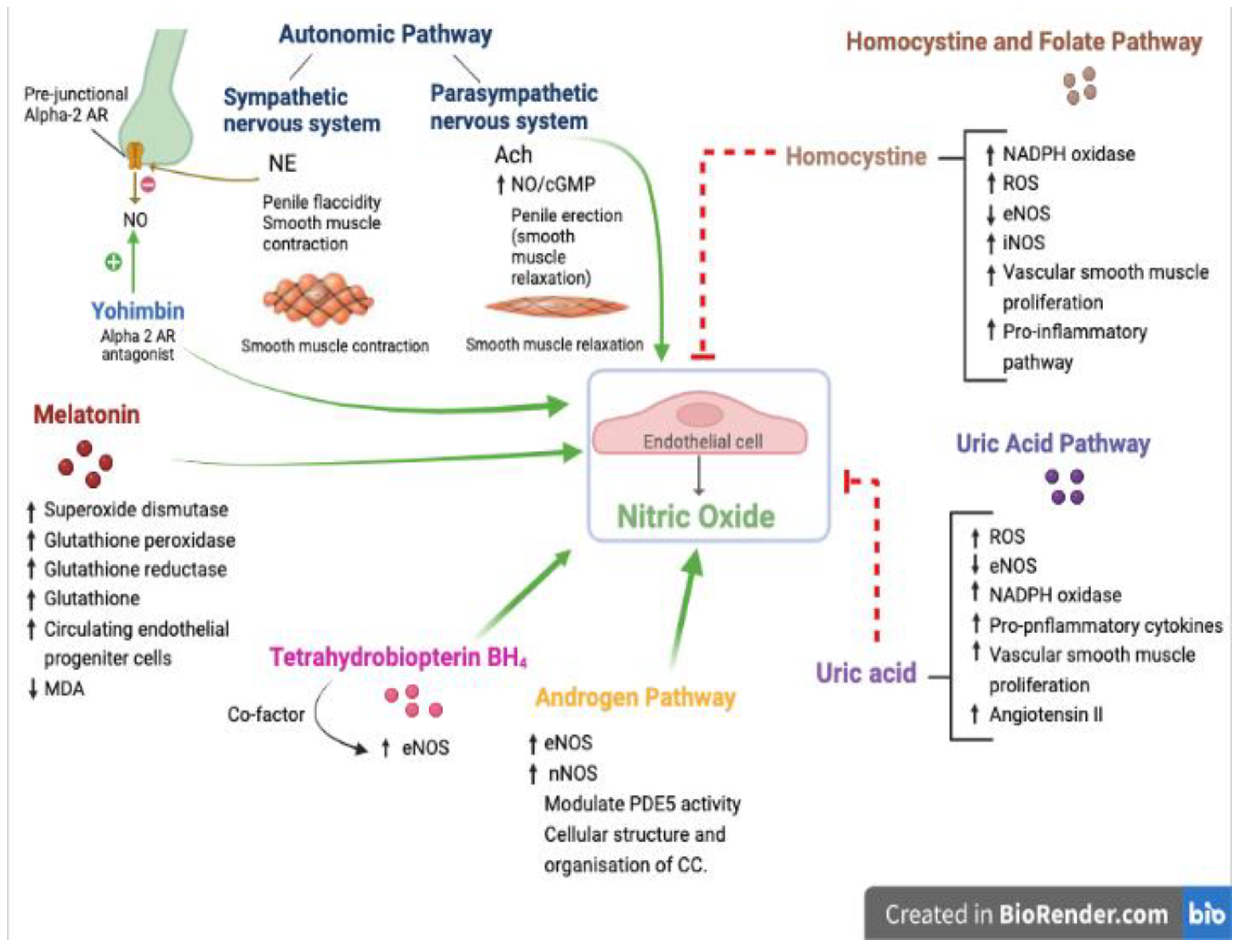
3. Pharmacological Pathways
3.1. Oxidant–Antioxidant Pathway
3.1.1. Tetrahydrobiopterin (BH4)
3.1.2. Melatonin
3.2. Homocysteine and Folate Pathway
3.3. Uric Acid Pathway
3.4. Androgen Pathway
3.5. Autonomic Pathway
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Montorsi, F.; Adaikan, G.; Becher, E.; Giuliano, F.; Khoury, S.; Lue, T.F.; Sharlip, I.; Althof, S.E.; Andersson, K.E.; Brock, G.; et al. Summary of the recommendations on sexual dysfunctions in men. J. Sex Med. 2010, 7, 3572–3588. [Google Scholar] [CrossRef] [PubMed]
- Pyrgidis, N.; Mykoniatis, I.; Haidich, A.B.; Tirta, M.; Talimtzi, P.; Kalyvianakis, D.; Ouranidis, A.; Hatzichristou, D. The Effect of Phosphodiesterase-type 5 Inhibitors on Erectile Function: An Overview of Systematic Reviews. Front. Pharm. 2021, 12, 735708. [Google Scholar] [CrossRef] [PubMed]
- Kloner, R.A.; Goldstein, I.; Kirby, M.G.; Parker, J.D.; Sadovsky, R. Cardiovascular Safety of Phosphodiesterase Type 5 Inhibitors After Nearly 2 Decades on the Market. Sex Med. Rev. 2018, 6, 583–594. [Google Scholar] [CrossRef] [PubMed]
- Sagban, T.H.; Ismail, K. Formulation and evaluation of orodispersible film of sildenafilcitrate. Int. J. Pharm. Pharm. Sci. 2014, 6, 81–86. [Google Scholar]
- Burnett, A.L.; Nehra, A.; Breau, R.H.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.; Khera, M.; McVary, K.T.; Miner, M.M.; et al. Erectile Dysfunction: AUA Guideline. J. Urol. 2018, 200, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Stridh, A.; Ponten, M.; Arver, S.; Kirsch, I.; Abe, C.; Jensen, K.B. Placebo Responses Among Men With Erectile Dysfunction Enrolled in Phosphodiesterase 5 Inhibitor Trials: A Systematic Review and Meta-analysis. JAMA Netw. Open. 2020, 3, e201423. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, B.G.; Kloner, R.A. Drug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertension. Circulation 2010, 122, 88–95. [Google Scholar] [CrossRef] [Green Version]
- McMahon, C.N.; Smith, C.J.; Shabsigh, R. Treating erectile dysfunction when PDE5 inhibitors fail. BMJ 2006, 332, 589–592. [Google Scholar] [CrossRef] [Green Version]
- Fagelman, E.; Fagelman, A.; Shabsigh, R. Efficacy, safety, and use of sildenafil in urologic practice. Urology 2001, 57, 1141–1144. [Google Scholar] [CrossRef]
- Kessler, A.; Sollie, S.; Challacombe, B.; Briggs, K.; Van Hemelrijck, M. The global prevalence of erectile dysfunction: A review. BJU Int. 2019, 124, 587–599. [Google Scholar] [CrossRef]
- Ayta, I.A.; McKinlay, J.B.; Krane, R.J. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 1999, 84, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.E.; Keoghane, S.R.; Miller, M.A. Vascular risk factors and erectile dysfunction. BJU Int. 2001, 87, 838–845. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, D.K.; Campbell, I.W.; Wu, F.C.; Prescott, R.J.; Clarke, B.F. The prevalence of diabetic impotence. Diabetologia 1980, 18, 279–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virag, R.; Bouilly, P.; Frydman, D. Is impotence an arterial disorder? A study of arterial risk factors in 440 impotent men. Lancet 1985, 1, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Macera, C.A.; Davis, D.R.; Hornung, C.A.; Nankin, H.R.; Blair, S.N. Total cholesterol and high density lipoprotein cholesterol as important predictors of erectile dysfunction. Am. J. Epidemiol. 1994, 140, 930–937. [Google Scholar] [CrossRef]
- Shabsigh, R.; Fishman, I.J.; Schum, C.; Dunn, J.K. Cigarette smoking and other vascular risk factors in vasculogenic impotence. Urology 1991, 38, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Araujo, A.B.; Hall, S.A.; Ganz, P.; Chiu, G.R.; Rosen, R.C.; Kupelian, V.; Travison, T.G.; McKinlay, J.B. Does erectile dysfunction contribute to cardiovascular disease risk prediction beyond the Framingham risk score? J. Am. Coll. Cardiol. 2010, 55, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Romano, L.; Pellegrino, R.; Sciorio, C.; Barone, B.; Gravina, A.G.; Santonastaso, A.; Mucherino, C.; Astretto, S.; Napolitano, L.; Aveta, A.; et al. Erectile and sexual dysfunction in male and female patients with celiac disease: A cross-sectional observational study. Andrology 2022, 10, 910–918. [Google Scholar] [CrossRef]
- McMahon, C.G. Current diagnosis and management of erectile dysfunction. Med. J. Aust. 2019, 210, 469–476. [Google Scholar] [CrossRef]
- Nickel, J.C.; Morales, A.; Condra, M.; Fenemore, J.; Surridge, D.H. Endocrine dysfunction in impotence: Incidence, significance and cost-effective screening. J. Urol. 1984, 132, 40–43. [Google Scholar] [CrossRef]
- Dean, R.C.; Lue, T.F. Physiology of penile erection and pathophysiology of erectile dysfunction. Urol. Clin. N. Am. 2005, 32, 379–395. [Google Scholar] [CrossRef]
- Jung, D.C.; Park, S.Y.; Lee, J.Y. Penile Doppler ultrasonography revisited. Ultrasonography 2018, 37, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Luscher, T.F.; Barton, M. Biology of the endothelium. Clin. Cardiol. 1997, 20 (Suppl. S2), II-3-10. [Google Scholar] [CrossRef] [PubMed]
- Mudau, M.; Genis, A.; Lochner, A.; Strijdom, H. Endothelial dysfunction: The early predictor of atherosclerosis. Cardiovasc. J. Afr. 2012, 23, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Ludmer, P.L.; Selwyn, A.P.; Shook, T.L.; Wayne, R.R.; Mudge, G.H.; Alexander, R.W.; Ganz, P. Paradoxical vasoconstriction induced by acetylcholine in atherosclerotic coronary arteries. N. Engl. J. Med. 1986, 315, 1046–1051. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Sorensen, K.E.; Bull, C.; Robinson, J.; Deanfield, J.E. Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J. Am. Coll. Cardiol. 1994, 24, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Azadzoi, K.M.; Goldstein, I. Erectile dysfunction due to atherosclerotic vascular disease: The development of an animal model. J. Urol. 1992, 147, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Levine, F.J.; Greenfield, A.J.; Goldstein, I. Arteriographically determined occlusive disease within the hypogastric-cavernous bed in impotent patients following blunt perineal and pelvic trauma. J. Urol. 1990, 144, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Garban, H.; Vernet, D.; Freedman, A.; Rajfer, J.; Gonzalez-Cadavid, N. Effect of aging on nitric oxide-mediated penile erection in rats. Am. J. Physiol. 1995, 268 Pt 2, H467–H475. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.A.; Seftel, A.D.; Razmjouei, K.; Ganz, M.B.; Hampel, N.; Ferguson, K. Erectile dysfunction in aging: Upregulation of endothelial nitric oxide synthase. Urology 1998, 51, 516–522. [Google Scholar] [CrossRef]
- Rajfer, J.; Aronson, W.J.; Bush, P.A.; Dorey, F.J.; Ignarro, L.J. Nitric oxide as a mediator of relaxation of the corpus cavernosum in response to nonadrenergic, noncholinergic neurotransmission. N. Engl. J. Med. 1992, 326, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Saenz de Tejada, I.; Goldstein, I.; Azadzoi, K.; Krane, R.J.; Cohen, R.A. Impaired neurogenic and endothelium-mediated relaxation of penile smooth muscle from diabetic men with impotence. N. Engl. J. Med. 1989, 320, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Pickard, R.S.; Powell, P.H.; Zar, M.A. Nitric oxide and cyclic GMP formation following relaxant nerve stimulation in isolated human corpus cavernosum. Br. J. Urol. 1995, 75, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Kaya, C.; Uslu, Z.; Karaman, I. Is endothelial function impaired in erectile dysfunction patients? Int. J. Impot. Res. 2006, 18, 55–60. [Google Scholar] [CrossRef] [Green Version]
- Yao, F.; Huang, Y.; Zhang, Y.; Dong, Y.; Ma, H.; Deng, C.; Lin, H.; Liu, D.; Lu, K. Subclinical endothelial dysfunction and low-grade inflammation play roles in the development of erectile dysfunction in young men with low risk of coronary heart disease. Int. J. Androl. 2012, 35, 653–659. [Google Scholar] [CrossRef]
- Pizzino, G.; Irrera, N.; Cucinotta, M.; Pallio, G.; Mannino, F.; Arcoraci, V.; Squadrito, F.; Altavilla, D.; Bitto, A. Oxidative Stress: Harms and Benefits for Human Health. Oxid. Med. Cell Longev. 2017, 2017, 8416763. [Google Scholar] [CrossRef] [Green Version]
- Guzik, T.J.; Mussa, S.; Gastaldi, D.; Sadowski, J.; Ratnatunga, C.; Pillai, R.; Channon, K.M. Mechanisms of increased vascular superoxide production in human diabetes mellitus: Role of NAD(P)H oxidase and endothelial nitric oxide synthase. Circulation 2002, 105, 1656–1662. [Google Scholar] [CrossRef] [Green Version]
- Cosentino, F.; Luscher, T.F. Tetrahydrobiopterin and endothelial function. Eur. Heart J. 1998, 19 (Suppl. G), G3–G8. [Google Scholar]
- Ohara, Y.; Peterson, T.E.; Harrison, D.G. Hypercholesterolemia increases endothelial superoxide anion production. J. Clin. Investig. 1993, 91, 2546–2551. [Google Scholar] [CrossRef] [Green Version]
- Hernanz, R.; Briones, A.M.; Salaices, M.; Alonso, M.J. New roles for old pathways? A circuitous relationship between reactive oxygen species and cyclo-oxygenase in hypertension. Clin. Sci. 2014, 126, 111–121. [Google Scholar] [CrossRef]
- Murphy, M.P. How mitochondria produce reactive oxygen species. Biochem. J. 2009, 417, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzkaya, N.; Weissmann, N.; Harrison, D.G.; Dikalov, S. Interactions of peroxynitrite, tetrahydrobiopterin, ascorbic acid, and thiols: Implications for uncoupling endothelial nitric-oxide synthase. J. Biol. Chem. 2003, 278, 22546–22554. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M. Oxidant stress and atherosclerosis. Curr. Opin. Pharmacol. 2004, 4, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Sommer, F.; Klotz, T.; Steinritz, D.; Bloch, W. Evaluation of tetrahydrobiopterin (BH4) as a potential therapeutic agent to treat erectile dysfunction. Asian J. Androl. 2006, 8, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, P.; Nandakumar, N.; Rengarajan, T.; Palaniswami, R.; Gnanadhas, E.N.; Lakshminarasaiah, U.; Gopas, J.; Nishigaki, I. Antioxidants and human diseases. Clin. Chim. Acta 2014, 436, 332–347. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.D.; Xin, Z.C.; Choi, H.K. Effect of Korean red ginseng on the rabbit corpus cavernosal smooth muscle. Int. J. Impot. Res. 1998, 10, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.S.; Lee, Y.J.; Chung, Y.H.; Lee, M.Y.; Kim, S.T.; Ko, S.K.; Momoi, M.; Kondoh, Y.; Sasaki, F.; Jeong, J.H. In vitro and in vivo evaluation of tissue-cultured mountain ginseng on penile erection. J. Ginseng Res. 2016, 40, 334–343. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.C.; Cappelleri, J.C.; Gendrano, N., 3rd. The International Index of Erectile Function (IIEF): A state-of-the-science review. Int. J. Impot. Res. 2002, 14, 226–244. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Pena, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Althof, S.E.; Corty, E.W.; Levine, S.B.; Levine, F.; Burnett, A.L.; McVary, K.; Stecher, V.; Seftel, A.D. EDITS: Development of questionnaires for evaluating satisfaction with treatments for erectile dysfunction. Urology 1999, 53, 793–799. [Google Scholar] [CrossRef]
- Costa, P.; Arnould, B.; Cour, F.; Boyer, P.; Marrel, A.; Jaudinot, E.O.; Solesse de Gendre, A. Quality of Sexual Life Questionnaire (QVS): A reliable, sensitive and reproducible instrument to assess quality of life in subjects with erectile dysfunction. Int. J. Impot. Res. 2003, 15, 173–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grover, S.; Shouan, A. Assessment Scales for Sexual Disorders—A Review. J. Psychosexual Health 2020, 2, 121–138. [Google Scholar] [CrossRef]
- Opladen, T.; Lopez-Laso, E.; Cortes-Saladelafont, E.; Pearson, T.S.; Sivri, H.S.; Yildiz, Y.; Assmann, B.; Kurian, M.A.; Leuzzi, V.; Heales, S.; et al. Consensus guideline for the diagnosis and treatment of tetrahydrobiopterin (BH4) deficiencies. Orphanet J. Rare Dis. 2020, 15, 126. [Google Scholar] [CrossRef] [PubMed]
- Bendall, J.K.; Douglas, G.; McNeill, E.; Channon, K.M.; Crabtree, M.J. Tetrahydrobiopterin in cardiovascular health and disease. Antioxid. Redox Signal 2014, 20, 3040–3077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitzer, T.; Krohn, K.; Albers, S.; Meinertz, T. Tetrahydrobiopterin improves endothelium-dependent vasodilation by increasing nitric oxide activity in patients with Type II diabetes mellitus. Diabetologia 2000, 43, 1435–1438. [Google Scholar] [CrossRef] [Green Version]
- Heitzer, T.; Brockhoff, C.; Mayer, B.; Warnholtz, A.; Mollnau, H.; Henne, S.; Meinertz, T.; Munzel, T. Tetrahydrobiopterin improves endothelium-dependent vasodilation in chronic smokers: Evidence for a dysfunctional nitric oxide synthase. Circ. Res. 2000, 86, E36–E41. [Google Scholar] [CrossRef] [Green Version]
- Stroes, E.; Kastelein, J.; Cosentino, F.; Erkelens, W.; Wever, R.; Koomans, H.; Luscher, T.; Rabelink, T. Tetrahydrobiopterin restores endothelial function in hypercholesterolemia. J. Clin. Investig. 1997, 99, 41–46. [Google Scholar] [CrossRef]
- Higashi, Y.; Sasaki, S.; Nakagawa, K.; Fukuda, Y.; Matsuura, H.; Oshima, T.; Chayama, K. Tetrahydrobiopterin enhances forearm vascular response to acetylcholine in both normotensive and hypertensive individuals. Am. J. Hypertens. 2002, 15 Pt 1, 326–332. [Google Scholar] [CrossRef] [Green Version]
- Ohashi, A.; Saeki, Y.; Harada, T.; Naito, M.; Takahashi, T.; Aizawa, S.; Hasegawa, H. Tetrahydrobiopterin Supplementation: Elevation of Tissue Biopterin Levels Accompanied by a Relative Increase in Dihydrobiopterin in the Blood and the Role of Probenecid-Sensitive Uptake in Scavenging Dihydrobiopterin in the Liver and Kidney of Rats. PLoS ONE 2016, 11, e0164305. [Google Scholar] [CrossRef] [Green Version]
- Un, O.; Yilmaz, D.; Bayatli, N.; Kaya, E.; Gur, S. L-arginine and tetrahydrobiopterin, but not sodium nitrite partially restored erectile dysfunction in aged rats. Aging Male 2014, 17, 248–255. [Google Scholar] [CrossRef]
- Claustrat, B.; Leston, J. Melatonin: Physiological effects in humans. Neurochirurgie 2015, 61, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.X.; Manchester, L.C.; Terron, M.P.; Flores, L.J.; Reiter, R.J. One molecule, many derivatives: A never-ending interaction of melatonin with reactive oxygen and nitrogen species? J. Pineal. Res. 2007, 42, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Galano, A.; Tan, D.X.; Reiter, R.J. Melatonin as a natural ally against oxidative stress: A physicochemical examination. J. Pineal Res. 2011, 51, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Barlow-Walden, L.R.; Reiter, R.J.; Abe, M.; Pablos, M.; Menendez-Pelaez, A.; Chen, L.D.; Poeggeler, B. Melatonin stimulates brain glutathione peroxidase activity. Neurochem. Int. 1995, 26, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Antolin, I.; Rodriguez, C.; Sainz, R.M.; Mayo, J.C.; Uria, H.; Kotler, M.L.; Rodriguez-Colunga, M.J.; Tolivia, D.; Menendez-Pelaez, A. Neurohormone melatonin prevents cell damage: Effect on gene expression for antioxidant enzymes. FASEB J. 1996, 10, 882–890. [Google Scholar] [CrossRef]
- Drago, F.; Busa, L. Acute low doses of melatonin restore full sexual activity in impotent male rats. Brain Res. 2000, 878, 98–104. [Google Scholar] [CrossRef]
- Paskaloglu, K.; Sener, G.; Ayangolu-Dulger, G. Melatonin treatment protects against diabetes-induced functional and biochemical changes in rat aorta and corpus cavernosum. Eur. J. Pharm. 2004, 499, 345–354. [Google Scholar] [CrossRef]
- Qiu, X.F.; Li, X.X.; Chen, Y.; Lin, H.C.; Yu, W.; Wang, R.; Dai, Y.T. Mobilisation of endothelial progenitor cells: One of the possible mechanisms involved in the chronic administration of melatonin preventing erectile dysfunction in diabetic rats. Asian J. Androl. 2012, 14, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Tavukcu, H.H.; Sener, T.E.; Tinay, I.; Akbal, C.; Ersahin, M.; Cevik, O.; Cadirci, S.; Reiter, R.J.; Sener, G. Melatonin and tadalafil treatment improves erectile dysfunction after spinal cord injury in rats. Clin. Exp. Pharm. Physiol. 2014, 41, 309–316. [Google Scholar] [CrossRef]
- Tang, Z.; Song, J.; Yu, Z.; Cui, K.; Ruan, Y.; Wang, T.; Yang, J.; Wang, S.; Liu, J. Melatonin Treatment Ameliorates Hyperhomocysteinemia-Induced Impairment of Erectile Function in a Rat Model. J. Sex. Med. 2019, 16, 1506–1517. [Google Scholar] [CrossRef]
- Bozkurt, A.; Karabakan, M.; Aktas, B.K.; Gunay, M.; Keskin, E.; Hirik, E. Low serum melatonin levels are associated with erectile dysfunction. Int. Braz. J. Urol. 2018, 44, 794–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blom, H.J.; Smulders, Y. Overview of homocysteine and folate metabolism. With special references to cardiovascular disease and neural tube defects. J. Inherit. Metab. Dis. 2011, 34, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.; Arheart, K.; Refsum, H.; Brattstrom, L.; Boers, G.; Ueland, P.; Rubba, P.; Palma-Reis, R.; Meleady, R.; Daly, L.; et al. Low circulating folate and vitamin B6 concentrations: Risk factors for stroke, peripheral vascular disease, and coronary artery disease. European COMAC Group. Circulation 1998, 97, 437–443. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, E.G.; Stehouwer, C.D.; Twisk, J.W.; van den Berg, M.; de Jong, S.C.; Mackaay, A.J.; van Campen, C.M.; Visser, F.C.; Jakobs, C.A.; Bulterjis, E.J.; et al. Effect of homocysteine-lowering treatment with folic acid plus vitamin B6 on progression of subclinical atherosclerosis: A randomised, placebo-controlled trial. Lancet 2000, 355, 517–522. [Google Scholar] [CrossRef]
- Cheng, S.W.; Ting, A.C.; Wong, J. Fasting total plasma homocysteine and atherosclerotic peripheral vascular disease. Ann. Vasc. Surg. 1997, 11, 217–223. [Google Scholar] [CrossRef]
- Vasan, R.S.; Beiser, A.; D’Agostino, R.B.; Levy, D.; Selhub, J.; Jacques, P.F.; Rosenberg, I.H.; Wilson, P.W. Plasma homocysteine and risk for congestive heart failure in adults without prior myocardial infarction. JAMA 2003, 289, 1251–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayer, E.L.; Jacobsen, D.W.; Robinson, K. Homocysteine and coronary atherosclerosis. J. Am. Coll. Cardiol. 1996, 27, 517–527. [Google Scholar] [CrossRef] [Green Version]
- Moselhy, S.S.; Demerdash, S.H. Plasma homocysteine and oxidative stress in cardiovascular disease. Dis. Markers 2003, 19, 27–31. [Google Scholar] [CrossRef] [Green Version]
- Tyagi, N.; Sedoris, K.C.; Steed, M.; Ovechkin, A.V.; Moshal, K.S.; Tyagi, S.C. Mechanisms of homocysteine-induced oxidative stress. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H2649–H2656. [Google Scholar] [CrossRef] [Green Version]
- Papatheodorou, L.; Weiss, N. Vascular oxidant stress and inflammation in hyperhomocysteinemia. Antioxid. Redox Signal. 2007, 9, 1941–1958. [Google Scholar] [CrossRef]
- Giovannone, R.; Busetto, G.M.; Antonini, G.; De Cobelli, O.; Ferro, M.; Tricarico, S.; Del Giudice, F.; Ragonesi, G.; Conti, S.L.; Lucarelli, G.; et al. Hyperhomocysteinemia as an Early Predictor of Erectile Dysfunction: International Index of Erectile Function (IIEF) and Penile Doppler Ultrasound Correlation With Plasma Levels of Homocysteine. Medicine 2015, 94, e1556. [Google Scholar] [CrossRef]
- Stabler, S.P.; Marcell, P.D.; Podell, E.R.; Allen, R.H.; Savage, D.G.; Lindenbaum, J. Elevation of total homocysteine in the serum of patients with cobalamin or folate deficiency detected by capillary gas chromatography-mass spectrometry. J. Clin. Investig. 1988, 81, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zhang, W.; Dai, Y.; Jiang, H.; Zhang, X. Serum Folic Acid and Erectile Dysfunction: A Systematic Review and Meta-Analysis. Sex. Med. 2021, 9, 100356. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.S.; Rosenson, R.S. Analytic Approaches for the Treatment of Hyperhomocysteinemia and Its Impact on Vascular Disease. Cardiovasc. Drugs Ther. 2018, 32, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Agostini, R.; Rossi, F.; Pajalich, R. Myoinositol/folic acid combination for the treatment of erectile dysfunction in type 2 diabetes men: A double-blind, randomized, placebo-controlled study. Eur. Rev. Med. Pharm. Sci. 2006, 10, 247–250. [Google Scholar]
- Hamidi Madani, A.; Asadolahzade, A.; Mokhtari, G.; Shahrokhi Damavand, R.; Farzan, A.; Esmaeili, S. Assessment of the efficacy of combination therapy with folic acid and tadalafil for the management of erectile dysfunction in men with type 2 diabetes mellitus. J. Sex Med. 2013, 10, 1146–1150. [Google Scholar] [CrossRef]
- Elshahid, A.R.M.; Shahein, I.M.; Mohammed, Y.F.; Ismail, N.F.; Zakarria, H.B.A.E.-R.; Gamal El Din, S.F. Folic acid supplementation improves erectile function in patients with idiopathic vasculogenic erectile dysfunction by lowering peripheral and penile homocysteine plasma levels: A case-control study. Andrology 2020, 8, 148–153. [Google Scholar] [CrossRef]
- Yu, W.; Cheng, J.D. Uric Acid and Cardiovascular Disease: An Update From Molecular Mechanism to Clinical Perspective. Front. Pharmacol. 2020, 11, 582680. [Google Scholar] [CrossRef]
- Battelli, M.G.; Polito, L.; Bortolotti, M.; Bolognesi, A. Xanthine Oxidoreductase-Derived Reactive Species: Physiological and Pathological Effects. Oxid. Med. Cell Longev. 2016, 2016, 3527579. [Google Scholar] [CrossRef] [Green Version]
- Mishima, M.; Hamada, T.; Maharani, N.; Ikeda, N.; Onohara, T.; Notsu, T.; Ninomiya, H.; Miyazaki, S.; Mizuta, E.; Sugihara, S.; et al. Effects of Uric Acid on the NO Production of HUVECs and its Restoration by Urate Lowering Agents. Drug Res. 2016, 66, 270–274. [Google Scholar] [CrossRef] [Green Version]
- Sautin, Y.Y.; Nakagawa, T.; Zharikov, S.; Johnson, R.J. Adverse effects of the classic antioxidant uric acid in adipocytes: NADPH oxidase-mediated oxidative/nitrosative stress. Am. J. Physiol. Cell Physiol. 2007, 293, C584–C596. [Google Scholar] [CrossRef] [PubMed]
- Cai, W.; Duan, X.M.; Liu, Y.; Yu, J.; Tang, Y.L.; Liu, Z.L.; Jiang, S.; Zhang, C.P.; Liu, J.Y.; Xu, J.X. Uric Acid Induces Endothelial Dysfunction by Activating the HMGB1/RAGE Signaling Pathway. Biomed. Res. Int. 2017, 2017, 4391920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, P.T.; Jamar, F.; Harrison, A.A.; Schofield, J.B.; Peters, A.M.; Binns, R.M.; Haskard, D.O. Characterization of E-selectin expression, leucocyte traffic and clinical sequelae in urate crystal-induced inflammation: An insight into gout. Br. J. Rheumatol. 1996, 35, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Haskard, D.O.; Landis, R.C. Interactions between leukocytes and endothelial cells in gout: Lessons from a self-limiting inflammatory response. Arthritis Res. 2002, 4 (Suppl. S3), S91–S97. [Google Scholar] [CrossRef]
- Sansone, A.; Reisman, Y.; Jannini, E.A. Relationship between hyperuricemia with deposition and sexual dysfunction in males and females. J. Endocrinol. Investig. 2022, 45, 691–703. [Google Scholar] [CrossRef]
- Wang, W.; Jing, Z.; Liu, W.; Zhu, L.; Ren, H.; Hou, X. Hyperuricaemia is an important risk factor of the erectile dysfunction: A systematic review and meta-analysis. Andrologia 2022, 54, e14384. [Google Scholar] [CrossRef]
- Luo, L.; Xiang, Q.; Deng, Y.; Zhao, S.; Zhu, Z.; Liu, Y.; Wang, J.; Zhao, Z. Gout is associated with elevated risk of erectile dysfunction: A systematic review and meta-analysis. Rheumatol. Int. 2019, 39, 1527–1535. [Google Scholar] [CrossRef]
- Chen, Y.-F.; Lin, H.-H.; Lu, C.-C.; Hung, C.-T.; Lee, M.-H.; Hsu, C.-Y.; Chung, W.-S. Gout and a Subsequent Increased Risk of Erectile Dysfunction in Men Aged 64 and Under: A Nationwide Cohort Study in Taiwan. J. Rheumatol. 2015, 42, 1898–1905. [Google Scholar] [CrossRef]
- Abdul Sultan, A.; Mallen, C.; Hayward, R.; Muller, S.; Whittle, R.; Hotston, M.; Roddy, E. Gout and subsequent erectile dysfunction: A population-based cohort study from England. Arthritis. Res. Ther. 2017, 19, 123. [Google Scholar] [CrossRef] [Green Version]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; Gelber, A.C.; Harrold, L.R.; Khanna, D.; King, C.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020, 72, 744–760. [Google Scholar] [CrossRef]
- Alem, M.M. Allopurinol and endothelial function: A systematic review with meta-analysis of randomized controlled trials. Cardiovasc. Ther. 2018, 36, e12432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farquharson, C.A.; Butler, R.; Hill, A.; Belch, J.J.; Struthers, A.D. Allopurinol improves endothelial dysfunction in chronic heart failure. Circulation 2002, 106, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Doehner, W.; Schoene, N.; Rauchhaus, M.; Leyva-Leon, F.; Pavitt, D.V.; Reaveley, D.A.; Schuler, G.; Coats, A.J.; Anker, S.D.; Hambrecht, R. Effects of xanthine oxidase inhibition with allopurinol on endothelial function and peripheral blood flow in hyperuricemic patients with chronic heart failure: Results from 2 placebo-controlled studies. Circulation 2002, 105, 2619–2624. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Deng, S.B.; She, Q.; Li, J.; Kao, G.Y.; Wang, J.S.; Ma, Y. Allopurinol ameliorates cardiac function in non-hyperuricaemic patients with chronic heart failure. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 756–761. [Google Scholar]
- Jain, P.; Rademaker, A.W.; McVary, K.T. Testosterone supplementation for erectile dysfunction: Results of a meta-analysis. J. Urol. 2000, 164, 371–375. [Google Scholar] [CrossRef]
- Sulcova, J.; Hill, M.; Hampl, R.; Starka, L. Age and sex related differences in serum levels of unconjugated dehydroepiandrosterone and its sulphate in normal subjects. J. Endocrinol. 1997, 154, 57–62. [Google Scholar] [CrossRef]
- Gray, A.; Feldman, H.A.; McKinlay, J.B.; Longcope, C. Age, disease, and changing sex hormone levels in middle-aged men: Results of the Massachusetts Male Aging Study. J. Clin. Endocrinol. Metab. 1991, 73, 1016–1025. [Google Scholar] [CrossRef]
- Feldman, H.A.; Goldstein, I.; Hatzichristou, D.G.; Krane, R.J.; McKinlay, J.B. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol. 1994, 151, 54–61. [Google Scholar] [CrossRef]
- Reiter, W.J.; Pycha, A.; Schatzl, G.; Pokorny, A.; Gruber, D.M.; Huber, J.C.; Marberger, M. Dehydroepiandrosterone in the treatment of erectile dysfunction: A prospective, double-blind, randomized, placebo-controlled study. Urology 1999, 53, 590–594; discussion 594–595. [Google Scholar] [CrossRef]
- Reiter, W.J.; Schatzl, G.; Mark, I.; Zeiner, A.; Pycha, A.; Marberger, M. Dehydroepiandrosterone in the treatment of erectile dysfunction in patients with different organic etiologies. Urol. Res. 2001, 29, 278–281. [Google Scholar] [CrossRef]
- Morales, A.; Black, A.; Emerson, L.; Barkin, J.; Kuzmarov, I.; Day, A. Androgens and sexual function: A placebo-controlled, randomized, double-blind study of testosterone vs. dehydroepiandrosterone in men with sexual dysfunction and androgen deficiency. Aging Male 2009, 12, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Dillon, J.S. Dehydroepiandrosterone stimulates nitric oxide release in vascular endothelial cells: Evidence for a cell surface receptor. Steroids 2004, 69, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Simoncini, T.; Mannella, P.; Fornari, L.; Varone, G.; Caruso, A.; Genazzani, A.R. Dehydroepiandrosterone modulates endothelial nitric oxide synthesis via direct genomic and nongenomic mechanisms. Endocrinology 2003, 144, 3449–3455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, M.R.; Ling, S.; Dawood, T.; Hashimura, K.; Dai, A.; Li, H.; Liu, J.P.; Funder, J.W.; Sudhir, K.; Komesaroff, P.A. Dehydroepiandrosterone inhibits human vascular smooth muscle cell proliferation independent of ARs and ERs. J. Clin. Endocrinol. Metab. 2002, 87, 176–181. [Google Scholar] [CrossRef]
- Clark, B.J.; Prough, R.A.; Klinge, C.M. Mechanisms of Action of Dehydroepiandrosterone. Vitam. Horm. 2018, 108, 29–73. [Google Scholar] [CrossRef] [PubMed]
- Traish, A.; Kim, N.N.; Moreland, R.B.; Goldstein, I. Role of alpha adrenergic receptors in erectile function. Int. J. Impot. Res. 2000, 12 (Suppl. S1), S48–S63. [Google Scholar] [CrossRef] [Green Version]
- Traish, A.M.; Kim, N.N.; Goldstein, I.; Moreland, R.B. Alpha-adrenergic receptors in the penis: Identification, characterization, and physiological function. J. Androl. 1999, 20, 671–682. [Google Scholar]
- Cohen, P.A.; Wang, Y.H.; Maller, G.; DeSouza, R.; Khan, I.A. Pharmaceutical quantities of yohimbine found in dietary supplements in the USA. Drug Test. Anal. 2016, 8, 357–369. [Google Scholar] [CrossRef] [Green Version]
- Simonsen, U.; Prieto, D.; Hernandez, M.; Saenz de Tejada, I.; Garcia-Sacristan, A. Prejunctional alpha 2-adrenoceptors inhibit nitrergic neurotransmission in horse penile resistance arteries. J. Urol. 1997, 157, 2356–2360. [Google Scholar] [CrossRef]
- Clark, J.T.; Smith, E.R.; Davidson, J.M. Evidence for the modulation of sexual behavior by alpha-adrenoceptors in male rats. Neuroendocrinology 1985, 41, 36–43. [Google Scholar] [CrossRef]
- Papeschi, R.; Sourkes, T.L.; Youdim, M.B. The effect of yohimbine on brain serotonin metabolism, motor behavior and body temperature of the rat. Eur. J. Pharmacol. 1971, 15, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Brannan, T.; Martinez-Tica, J.; Yahr, M.D. Effect of yohimbine on brain monoamines: An in vivo study. J. Neural. Transm. Park. Dis. Dement. Sect. 1991, 3, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; McCarley, A. Yohimbine treatment of sexual side effects induced by serotonin reuptake blockers. J. Clin. Psychiatry 1992, 53, 207–209. [Google Scholar] [PubMed]
- Wibowo, D.; Soebadi, D.M.; Soebadi, M.A. Yohimbine as a treatment for erectile dysfunction: A systematic review and meta-analysis. Turk. J. Urol. 2021, 47, 482–488. [Google Scholar] [CrossRef] [PubMed]
- Stief, C.G.; Wetterauer, U. Erectile responses to intracavernous papaverine and phentolamine: Comparison of single and combined delivery. J. Urol. 1988, 140, 1415–1416. [Google Scholar] [CrossRef]
- Juenemann, K.P.; Lue, T.F.; Fournier, G.R., Jr.; Tanagho, E.A. Hemodynamics of papaverine- and phentolamine-induced penile erection. J. Urol. 1986, 136, 158–161. [Google Scholar] [CrossRef]
- Marquer, C.; Bressolle, F. Moxisylyte: A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic use in impotence. Fundam. Clin. Pharmacol. 1998, 12, 377–387. [Google Scholar] [CrossRef]
- Giraldi, A.; Wyllie, M.; Wagner, G. Abanoquil, a new alpha-1 adrenoceptor antagonist. In vitro and in vivo effect on erectile tissue. Int. J. Impot. Res. 2000, 12, S37–S40. [Google Scholar] [CrossRef] [Green Version]
- Matés, J.M.; Pérez-Gómez, C.; Núñez de Castro, I. Antioxidant enzymes and human diseases. Clin. Biochem. 1999, 32, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Khosla, U.M.; Zharikov, S.; Finch, J.L.; Nakagawa, T.; Roncal, C.; Mu, W.; Krotova, K.; Block, E.R.; Prabhakar, S.; Johnson, R.J. Hyperuricemia induces endothelial dysfunction. Kidney Int. 2005, 67, 1739–1742. [Google Scholar] [CrossRef] [Green Version]
- Chávez, M.D.; Lakshmanan, N.; Kavdia, M. Impact of superoxide dismutase on nitric oxide and peroxynitrite levels in the microcirculation--a computational model. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2007, 2007, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Traish, A.M.; Goldstein, I.; Kim, N.N. Testosterone and erectile function: From basic research to a new clinical paradigm for managing men with androgen insufficiency and erectile dysfunction. Eur. Urol. 2007, 52, 54–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corry, D.B.; Eslami, P.; Yamamoto, K.; Nyby, M.D.; Makino, H.; Tuck, M.L. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system. J. Hypertens. 2008, 26, 269–275. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adam, D.R.; Alem, M.M. Erectile Dysfunction: Pharmacological Pathways with Understudied Potentials. Biomedicines 2023, 11, 46. https://doi.org/10.3390/biomedicines11010046
Adam DR, Alem MM. Erectile Dysfunction: Pharmacological Pathways with Understudied Potentials. Biomedicines. 2023; 11(1):46. https://doi.org/10.3390/biomedicines11010046
Chicago/Turabian StyleAdam, Doaa R., and Manal M. Alem. 2023. "Erectile Dysfunction: Pharmacological Pathways with Understudied Potentials" Biomedicines 11, no. 1: 46. https://doi.org/10.3390/biomedicines11010046