
A Review of the Systemic Treatment of Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis

Abstract
:1. Introduction
2. Pathogenesis
3. Literature Review for Systemic Treatment for SJS/TEN
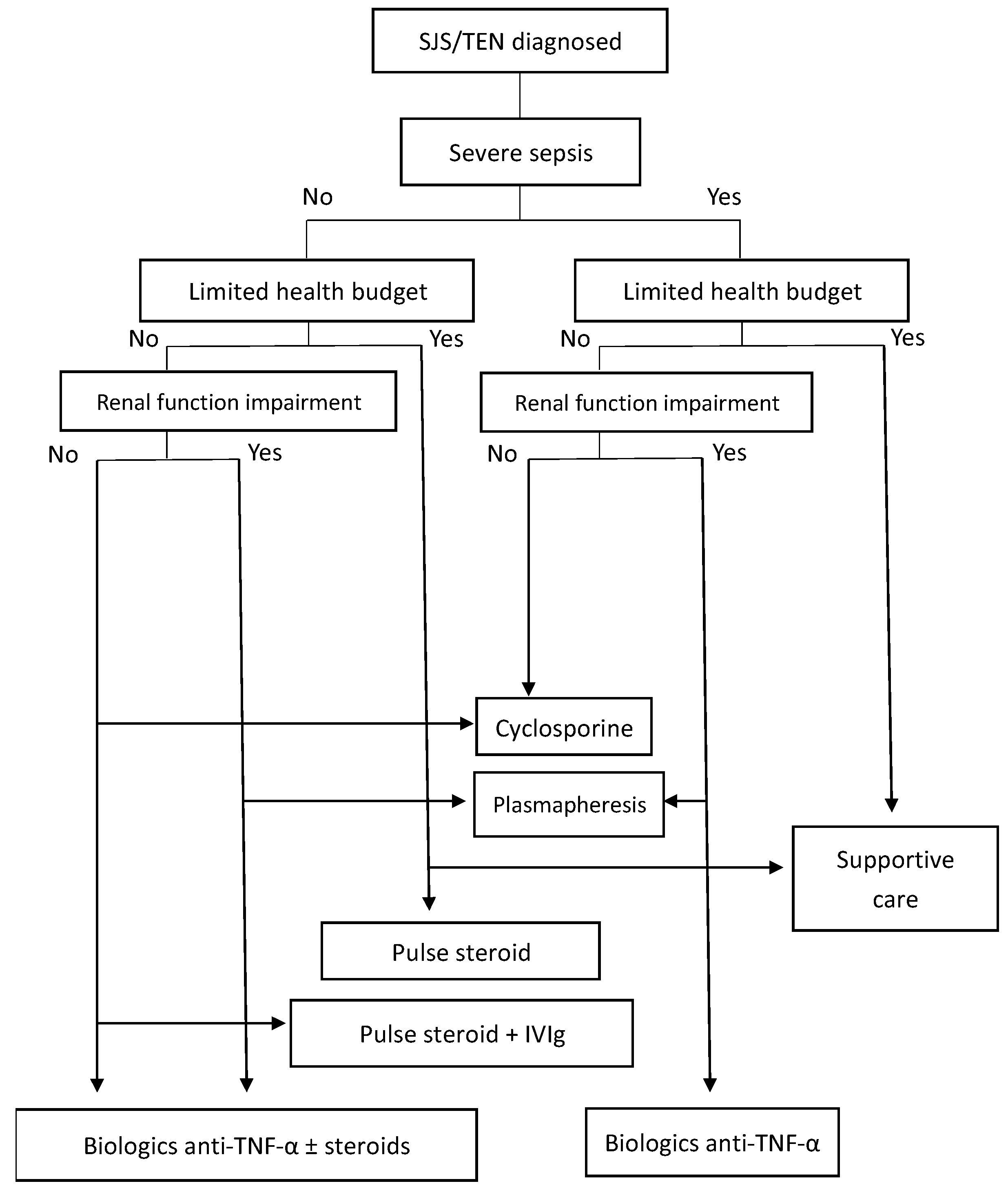
4. Management
4.1. Culprit Drugs Identification and Withdrawal
4.2. Severity-of-Illness Score for TEN (SCORTEN)
4.3. Supportive Therapy
4.4. Systemic Corticosteroids
4.5. Intravenous Immunoglobulin (IVIg)
4.6. Combination of Systemic Corticosteroids and IVIg
4.7. Cyclosporine A (CsA)
4.8. TNF-Alpha (TNF-α) Inhibitors
4.9. Combination of Biologic Anti-TNF-α and Corticosteroids
4.10. Combination of Biologic Anti-TNF-α with Other Treatments
4.11. Plasmapheresis
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dodiuk-Gad, R.P.; Chung, W.-H.; Valeyrie-Allanore, L.; Shear, N.H. Stevens-Johnson syndrome and toxic epidermal necrolysis: An update. Am. J. Clin. Dermatol. 2015, 16, 475–493. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.S.; Lee, J.Y.; Kim, J.; Kim, G.W.; Kim, B.K.; Kim, J.Y.; Park, H.W.; Cho, S.H.; Min, K.U.; Kang, H.R. Incidence of Stevens-Johnson Syndrome and Toxic Epi-dermal Necrolysis: A nationwide population-based study using National Health In-surance Database in Korea. PLoS ONE 2016, 11, e0165933. [Google Scholar] [CrossRef]
- Hsu, D.Y.; Brieva, J.; Silverberg, N.B.; Silverberg, J.I. Morbidity and Mortality of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in United States Adults. J. Investig. Dermatol. 2016, 136, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- Lerch, M.; Mainetti, C.; Beretta-Piccoli, B.T.; Harr, T. Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. Clin. Rev. Allergy Immunol. 2018, 54, 147–176. [Google Scholar] [CrossRef]
- Hoffman, M.; Chansky, P.B.; Bashyam, A.R.; Boettler, M.A.; Challa, N.; Dominguez, A.; Estupinan, B.; Gupta, R.; Hennessy, K.; Huckell, S.N.; et al. Long-term Physical and Psychological Outcomes of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. JAMA Dermatol. 2021, 157, 712–715. [Google Scholar] [CrossRef]
- Wei, C.Y.; Chung, W.H.; Huang, H.W.; Chen, Y.T.; Hung, S.I. Direct interaction between HLA-B and carbamazepine activates T cells in patients with Stevens-Johnson syndrome. J. Allergy Clin. Immunol. 2012, 129, 1562–1569.e5. [Google Scholar] [CrossRef]
- Tangamornsuksan, W.; Chaiyakunapruk, N.; Somkrua, R.; Lohitnavy, M.; Tassaneeyakul, W. Relationship between the HLA-B*1502 allele and carbamazepine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis: A systematic review and meta-analysis. JAMA Dermatol. 2013, 149, 1025–1032. [Google Scholar] [CrossRef]
- Viard, I.; Wehrli, P.; Bullani, R.; Schneider, P.; Holler, N.; Salomon, D.; Hunziker, T.; Saurat, J.H.; Tschopp, J.; French, L.E. Inhibition of toxic epidermal necrolysis by blockade of CD95 with human intravenous immunoglobulin. Science 1998, 282, 490–493. [Google Scholar] [CrossRef]
- Inachi, S.; Mizutani, H.; Shimizu, M. Epidermal apoptotic cell death in erythema multi-forme and Stevens-Johnson syndrome. Contribution of perforin-positive cell infiltration. Arch. Dermatol. 1997, 133, 845–849. [Google Scholar] [CrossRef]
- Nassif, A.; Bensussan, A.; Dorothée, G.; Mami-Chouaib, F.; Bachot, N.; Bagot, M.; Boumsell, L.; Roujeau, J.C. Drug Specific Cytotoxic T-Cells in the Skin Lesions of a Patient with Toxic Epidermal Necrolysis. J. Investig. Dermatol. 2002, 118, 728–733. [Google Scholar] [CrossRef] [Green Version]
- Nassif, A.; Bensussan, A.; Boumsell, L.; Deniaud, A.; Moslehi, H.; Wolkenstein, P.; Bagot, M.; Roujeau, J.C. Toxic epidermal necrolysis: Effector cells are drug-specific cytotoxic T cells. J. Allergy Clin. Immunol. 2004, 114, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Chung, W.H.; Hung, S.I.; Yang, J.Y.; Su, S.C.; Huang, S.P.; Wei, C.Y.; Chin, S.W.; Chiou, C.C.; Chu, S.C.; Ho, H.C.; et al. Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat. Med. 2008, 14, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Abe, R.; Yoshioka, N.; Murata, J.; Fujita, Y.; Shimizu, H. Granulysin as a marker for early diagnosis of the Stevens-Johnson syndrome. Ann. Intern. Med. 2009, 151, 514–515. [Google Scholar] [CrossRef] [PubMed]
- Nassif, A.; Moslehi, H.; Le Gouvello, S.; Bagot, M.; Lyonnet, L.; Michel, L.; Boumsell, L.; Bensussan, A.; Roujeau, J.C. Evaluation of the potential role of cytokines in toxic epidermal necrolysis. J. Investig. Dermatol. 2004, 123, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Su, S.C.; Mockenhaupt, M.; Wolkenstein, P.; Dunant, A.; Le Gouvello, S.; Chen, C.B.; Chosidow, O.; Valeyrie-Allanore, L.; Bellon, T.; Sekula, P.; et al. Interleukin-15 Is Associated with Severity and Mortality in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. J. Investig. Dermatol. 2017, 137, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.C.; Li, Y.C.; Chen, T.J. The efficacy of intravenous immunoglobulin for the treatment of toxic epidermal necrolysis: A systematic review and meta-analysis. Br. J. Dermatol. 2012, 167, 424–432. [Google Scholar] [CrossRef]
- Barron, S.J.; Del Vecchio, M.T.; Aronoff, S.C. Intravenous immunoglobulin in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis: A meta-analysis with meta-regression of observational studies. Int. J. Dermatol. 2015, 54, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.P.; Zhang, C.; Zhu, Q.X. The Effect of Intravenous Immunoglobulin Combined with Corticosteroid on the Progression of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Meta-Analysis. PLoS ONE 2016, 11, e0167120. [Google Scholar] [CrossRef]
- Huang, Y.C.; Chien, Y.N.; Chen, Y.T.; Li, Y.C.; Chen, T.J. Intravenous immunoglobulin for the treatment of toxic epidermal necrolysis: A systematic review and meta-analysis. G. Ital. Dermatol. Venereol. 2016, 151, 515–524. [Google Scholar] [CrossRef]
- Zimmermann, S.; Sekula, P.; Venhoff, M.; Motschall, E.; Knaus, J.; Schumacher, M.; Mockenhaupt, M. Systemic Immunomodulating Therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis. JAMA Dermatol. 2017, 153, 514–522. [Google Scholar] [CrossRef]
- Ng, Q.X.; De Deyn, M.L.Z.Q.; Venkatanarayanan, N.; Ho, C.Y.X.; Yeo, W.S. A meta-analysis of cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis. J. Inflamm. Res. 2018, 11, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Tang, S.; Li, S.; Pan, Y.; Ding, Y. Biologic TNF-alpha inhibitors in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis: A systemic review. J. Dermatolog. Treat. 2020, 31, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Patel, T.K.; Patel, P.B.; Thakkar, S. Comparison of effectiveness of interventions in reducing mortality in patients of toxic epidermal necrolysis: A network meta-analysis. Indian J. Dermatol. Venereol. Leprol. 2021, 87, 628–644. [Google Scholar] [CrossRef]
- Torres-Navarro, I.; Briz-Redón, Á.; Botella-Estrada, R. Systemic therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A SCORTEN-based systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 159–171. [Google Scholar] [CrossRef]
- Sachdeva, M.; Maliyar, K.; Ponzo, M.G. A Systematic Review of Efficacy and Safety of Monotherapy and Combination Therapy With Biologic for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. J. Cutan. Med. Surg. 2021, 25, 598–615. [Google Scholar] [CrossRef] [PubMed]
- Tsai, T.Y.; Huang, I.H.; Chao, Y.C.; Li, H.; Hsieh, T.S.; Wang, H.H.; Huang, Y.T.; Chen, C.Y.; Cheng, Y.C.; Kuo, P.H.; et al. Treating toxic epidermal necrolysis with systemic immunomodulating therapies: A systematic review and network meta-analysis. J. Am. Acad. Dermatol. 2021, 84, 390–397. [Google Scholar] [CrossRef]
- Krajewski, A.; Maciejewska-Markiewicz, D.; Jakubczyk, K.; Markowska, M.; Strużyna, J.; Mądry, R.; Mazurek, M.; Skonieczna-Żydecka, K. Impact of multiple medical interventions on mortality, length of hospital stay and reepithelialization time in Toxic Epidermal Necrolysis, Steven-Johnsons Syndrome, and TEN/SJS Overlap-Metanalysis and metaregression of observational studies. Burns 2021, 48, 263–280. [Google Scholar] [CrossRef]
- Houschyar, K.S.; Tapking, C.; Borrelli, M.R.; Puladi, B.; Ooms, M.; Wallner, C.; Duscher, D.; Pförringer, D.; Rein, S.; Reumuth, G.; et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: A systematic review and meta-analysis. J. Wound Care 2021, 30, 1012–1019. [Google Scholar] [CrossRef]
- Creamer, D.; Walsh, S.A.; Dziewulski, P.; Exton, L.S.; Lee, H.Y.; Dart, J.K.; Setterfield, J.; Bunker, C.B.; Ardern-Jones, M.R.; Watson, K.M.; et al. U.K. guidelines for the management of Stevens-Johnson syndrome/toxic epidermal necrolysis in adults 2016. Br. J. Dermatol. 2016, 174, 1194–1227. [Google Scholar] [CrossRef]
- Aihara, M.; Kano, Y.; Iijima, M.; Ikezawa, Z.; Shiohara, T.; Morita, E.; Kinoshita, S.; Aihara, Y.; Shirakata, Y.; Tohyama, M.; et al. Guidelines for the management of Stevens-Johnson syndrome and toxic epidermal necrolysis 2009, established by the Japanese research committee on Severe adverse reaction (J-SCAR) supported by the Ministry of Health, Labour and Welfare of Japan]. Jpn. J. Dermatol. 2009, 119, 2157–2163. (In Japanese) [Google Scholar]
- Sassolas, B.; Haddad, C.; Mockenhaupt, M.; Dunant, A.; Liss, Y.; Bork, K.; Haustein, U.F.; Vieluf, D.; Roujeau, J.C.; Le Louet, H. ALDEN, an algorithm for assessment of drug causality in Stevens-Johnson syndrome and toxic epidermal necrolysis: Comparison with case-control analysis. Clin. Pharmacol. Ther. 2010, 88, 60–68. [Google Scholar] [CrossRef]
- Roujeau, J.C.; Kelly, J.P.; Naldi, L.; Rzany, B.; Stern, R.S.; Anderson, T.; Auquier, A.; Bastuji-Garin, S.; Correia, O.; Locati, F.; et al. Medication use and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. N. Eng. J. Med. 1995, 333, 1600–1607. [Google Scholar] [CrossRef]
- Mockenhaupt, M.; Viboud, C.; Dunant, A.; Naldi, L.; Halevy, S.; Bouwes Bavinck, J.N.; Sidoroff, A.; Schneck, J.; Roujeau, J.C.; Flahault, A. Stevens-Johnson syndrome and toxic epidermal necrolysis: Assessment of medication risks with emphasis on recently marketed drugs: The EuroSCAR-study. J. Investig. Dermatol. 2008, 128, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Wolkenstein, P.; Chosidow, O.; Flechet, M.L.; Robbiola, O.; Paul, M.; Dumé, L.; Revuz, J.; Roujeau, J.C. Patch testing in severe cutaneous adverse drug reactions, including Stevens-Johnson syndrome and toxic epidermal necrolysis. Contact Dermat. 1996, 35, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Barbaud, A.; Collet, E.; Milpied, B.; Assier, H.; Staumont, D.; Avenel-Audran, M.; Grange, A.; Amarger, S.; Girardin, P.; Guinnepain, M.T.; et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br. J. Dermatol. 2013, 168, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.T.; Chang, Y.C.; Hui, R.C.; Yang, C.H.; Ho, H.C.; Hung, S.I.; Chung, W.H. A patch testing and cross-sensitivity study of carbamazepine-induced severe cutaneous adverse drug reactions. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 356–364. [Google Scholar] [CrossRef]
- Tang, Y.H.; Mockenhaupt, M.; Henry, A.; Bounoua, M.; Naldi, L.; Le Gouvello, S.; Bensussan, A.; Roujeau, J.C. Poor relevance of a lymphocyte proliferation assay in lamotrigine-induced Stevens-Johnson syndrome or toxic epidermal necrolysis. Clin. Exp. Allergy 2012, 42, 248–254. [Google Scholar] [CrossRef]
- Roujeau, J.C.; Albengres, E.; Moritz, S.; Piacentino, A.; Cuny, M.; Revuz, J.; Touraine, R. Lymphocyte transformation test in drug-induced toxic epidermal necrolysis. Int. Arch. Allergy Appl. Immunol. 1985, 78, 22–24. [Google Scholar] [CrossRef]
- Polak, M.E.; Belgi, G.; McGuire, C.; Pickard, C.; Healy, E.; Friedmann, P.S.; Ardern-Jones, M.R. In vitro diagnostic assays are effective during the acute phase of delayed-type drug hypersensitivity reactions. Br. J. Dermatol. 2013, 168, 539–549. [Google Scholar] [CrossRef]
- Porebski, G.; Pecaric-Petkovic, T.; Groux-Keller, M.; Bosak, M.; Kawabata, T.T.; Pichler, W.J. In vitro drug causality assessment in Stevens-Johnson syndrome—Alternatives for lymphocyte transformation test. Clin. Exp. Allergy 2013, 43, 1027–1037. [Google Scholar] [CrossRef]
- Fatangare, A.; Glässner, A.; Sachs, B.; Sickmann, A. Future perspectives on in-vitro diagnosis of drug allergy by the lymphocyte transformation test. J. Immunol. Methods 2021, 495, 113072. [Google Scholar] [CrossRef] [PubMed]
- Bastuji-Garin, S.; Fouchard, N.; Bertocchi, M.; Roujeau, J.C.; Revuz, J.; Wolkenstein, P. SCORTEN: A severity-of-illness score for toxic epidermal necrolysis. J. Investig. Dermatol. 2000, 115, 149–153. [Google Scholar] [PubMed]
- Shanbhag, S.S.; Chodosh, J.; Fathy, C.; Goverman, J.; Mitchell, C.; Saeed, H.N. Multidisciplinary care in Stevens-Johnson syndrome. Ther. Adv. Chronic. Dis. 2020, 11, 2040622319894469. [Google Scholar] [CrossRef] [PubMed]
- Valeyrie-Allanore, L.; Ingen-Housz-Oro, S.; Chosidow, O.; Wolkenstein, P. French referral center management of Stevens–Johnson syndrome/toxic epidermal necrolysis. Dermatol. Sin. 2013, 31, 191–195. [Google Scholar] [CrossRef]
- Mockenhaupt, M. The current understanding of Stevens-Johnson syndrome and toxic epidermal necrolysis. Expert Rev. Clin. Immunol. 2011, 7, 803–813. [Google Scholar] [CrossRef]
- Ginsburg, C.M. Stevens-Johnson syndrome in children. Pediatr. Infect. Dis. J. 1982, 1, 155–158. [Google Scholar] [CrossRef]
- Halebian, P.H.; Corder, V.J.; Madden, M.R.; Finklestein, J.L.; Shires, G.T. Improved Burn Center Survival of Patients with Toxic Epidermal Necrolysis Managed without Corticosteroids. Ann. Surg. 1986, 204, 503–512. [Google Scholar] [CrossRef]
- Kelemen, J.J., 3rd; Cioffi, W.G.; McManus, W.F.; Mason, A.D., Jr.; Pruitt, B.A., Jr. Burn center care for patients with toxic epidermal necrolysis. J. Am. Coll. Surg. 1995, 180, 273–278. [Google Scholar]
- Schneck, J.; Fagot, J.P.; Sekula, P.; Sassolas, B.; Roujeau, J.C.; Mockenhaupt, M. Effects of treatments on the mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis: A retrospective study on patients included in the prospective EuroSCAR Study. J. Am. Acad. Dermatol. 2008, 58, 33–40. [Google Scholar] [CrossRef]
- Kardaun, S.H.; Jonkman, M.F. Dexamethasone pulse therapy for Stevens-Johnson syndrome/toxic epidermal necrolysis. Acta Derm. Venereol. 2007, 87, 144–148. [Google Scholar] [CrossRef]
- Araki, Y.; Sotozono, C.; Inatomi, T.; Ueta, M.; Yokoi, N.; Ueda, E.; Kishimoto, S.; Kinoshita, S. Successful treatment of Stevens-Johnson syndrome with steroid pulse therapy at disease onset. Am. J. Oph. Thalmol. 2009, 147, 1004–1011.e1. [Google Scholar] [CrossRef] [PubMed]
- Hirahara, K.; Kano, Y.; Sato, Y.; Horie, C.; Okazaki, A.; Ishida, T.; Aoyama, Y.; Shiohara, T. Methylprednisolone pulse therapy for Stevens-Johnson syn-drome/toxic epidermal necrolysis: Clinical evaluation and analysis of biomarkers. J. Am. Acad. Dermatol. 2013, 69, 496–498. [Google Scholar] [CrossRef]
- Das, S.; Roy, A.K.; Biswas, I. A six-month prospective study to find out the treatment outcome, prognosis and offending drugs in toxic epidermal necrolysis from an urban institution in kolkata. Indian J. Dermatol. 2013, 58, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Mieno, H.; Ueta, M.; Kinoshita, F.; Teramukai, S.; Kinoshita, S.; Sotozono, C. Corticosteroid Pulse Therapy for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis Patients with Acute Ocular Involvement. Am. J. Ophthalmol. 2021, 231, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Nie, X.; Zhang, L. A retrospective analysis of Stevens-Johnson syndrome/toxic epidermal necrolysis treated with corticosteroids. Int. J. Dermatol. 2016, 55, 1408–1413. [Google Scholar] [CrossRef]
- Jarczak, D.; Kluge, S.; Nierhaus, A. Use of Intravenous Immunoglobulins in Sepsis Therapy-A Clinical View. Int. J. Mol. Sci. 2020, 21, 5543. [Google Scholar] [CrossRef]
- Amato, G.M.; Travia, A.; Ziino, O. The use of intravenous high-dose immunoglobulins (IGIV) in a case of Stevens-Johnson syndrome. Pediatr. Med. Chir. 1992, 14, 555–556. [Google Scholar]
- Prins, C.; Vittorio, C.; Padilla, R.S.; Hunziker, T.; Itin, P.; Förster, J.; Bröcker, E.B.; Saurat, J.H.; French, L.E. Effect of high-dose intravenous immunoglobulin therapy in Stevens-Johnson syndrome: A retrospective, multicenter study. Dermatology 2003, 207, 96–99. [Google Scholar] [CrossRef]
- Ai-Mutairi, N.; Arun, J.; Osama, N.E.; Amr, Z.; Mazen, A.S.; Ibtesam, E.-A.; Nazeha, E.-B. Prospective, noncomparative open study from Kuwait of the role of intravenous immunoglobulin in the treatment of toxic epidermal necrolysis. Int. J. Dermatol. 2004, 43, 847–851. [Google Scholar] [CrossRef]
- Tristani-Firouzi, P.; Petersen, M.J.; Saffle, J.R.; Morris, S.E.; Zone, J.J. Treatment of toxic epidermal necrolysis with intravenous immunoglobulin in children. J. Am. Acad. Dermatol. 2002, 47, 548–552. [Google Scholar] [CrossRef]
- Firoz, B.F.; Henning, J.S.; Zarzabal, L.A.; Pollock, B.H. Toxic epidermal necrolysis: Five years of treatment experience from a burn unit. J. Am. Acad. Dermatol. 2012, 67, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Bachot, N.; Revuz, J.; Roujeau, J.C. Intravenous immunoglobulin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis: A prospective noncomparative study showing no benefit on mortality or progression. Arch. Dermatol. 2003, 139, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.; Davidovici, B. Severe cutaneous adverse drug reactions: Who should treat, where and how?: Facts and controversies. Clin. Dermatol. 2010, 28, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Mittmann, N.; Chan, B.; Knowles, S.; Cosentino, L.; Shear, N. Intravenous immunoglobulin use in patients with toxic epidermal necrolysis and Stevens-Johnson syndrome. Am. J. Clin. Dermatol. 2006, 7, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Prins, C.; Kerdel, F.A.; Padilla, R.S.; Hunziker, T.; Chimenti, S.; Viard, I.; Mauri, D.N.; Flynn, K.; Trent, J.; Margolis, D.J.; et al. Treatment of toxic epidermal necrolysis with high-dose intravenous immunoglobulins: Multicenter retrospective analysis of 48 consecutive cases. Arch. Dermatol. 2003, 139, 26–32. [Google Scholar] [CrossRef]
- Trent, J.T.; Kirsner, R.S.; Romanelli, P.; Kerdel, F.A. Analysis of intravenous immuno-globulin for the treatment of toxic epidermal necrolysis using SCORTEN: The University of Miami experience. Arch. Dermatol. 2003, 139, 39–43. [Google Scholar] [CrossRef]
- Reipert, B.M.; Stellamor, M.T.; Poell, M.; Ilas, J.; Sasgary, M.; Reipert, S.; Zimmermann, K.; Ehrlich, H.; Schwarz, H.P. Variation of anti-Fas antibodies in different lots of intravenous immunoglobulin. Vox Sang 2008, 94, 334–341. [Google Scholar] [CrossRef]
- Yang, Y.; Xu, J.; Li, F.; Zhu, X. Combination therapy of intravenous immunoglobulin and cortico-steroid in the treatment of toxic epidermal necrolysis and Stevens-Johnson syndrome: A retrospective comparative study in China. Int. J. Dermatol. 2009, 48, 1122–1128. [Google Scholar] [CrossRef]
- Chen, J.; Wang, B.; Zeng, Y.; Xu, H. High-dose intravenous immunoglobulins in the treatment of Stevens-Johnson syndrome and toxic epidermal necrolysis in Chinese patients: A retrospective study of 82 cases. Eur. J. Dermatol. 2010, 20, 743–747. [Google Scholar] [CrossRef]
- Jagadeesan, S.; Sobhanakumari, K.; Sadanandan, S.M.; Ravindran, S.; Divakaran, M.V.; Skaria, L.; Kurien, G. Low dose intravenous immunoglobulins and steroids in toxic epidermal necrolysis: A prospective comparative open-labelled study of 36 cases. Indian J. Dematol. Venereol. Leprol. 2013, 79, 506–511. [Google Scholar] [CrossRef]
- Micheletti, R.G.; Chiesa-Fuxench, Z.; Noe, M.H.; Stephen, S.; Aleshin, M.; Agarwal, A.; Boggs, J.; Cardones, A.R.; Chen, J.K.; Cotliar, J.; et al. Stevens-Johnson syndrome/toxic epidermal necrolysis: A multi-center retrospective study of 377 adult patients from the United States. J. Investig. Dermatol. 2018, 138, 2315–2321. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.; Scherrer, L.A. Efficacy and safety of cyclosporine in Stevens-Johnson syn-drome and toxic epidermal necrolysis. Dermatol. Ther. 2019, 32, e12758. [Google Scholar] [CrossRef] [PubMed]
- Arevalo, J.M.; Lorente, J.A.; Gonzalez-Herrada, C.; Jimenez-Reyes, J. Treatment of toxic epidermal necrolysis with cyclosporine A. J. Trauma 2000, 48, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Valeyrie-Allanore, L.; Wolkenstein, P.; Brochard, L.; Ortonne, N.; Maître, B.; Revuz, J.; Bagot, M.; Roujeau, J.C. Open trial of ciclosporin treatment for Stevens-Johnson syndrome and toxic epidermal necrolysis. Br. J. Dermatol. 2010, 163, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Chatteljee, M.; Verma, R. Cyclosporine in Stevens-Johnson syndrome and toxic epidermal necrolysis and retrospective comparison with systemic corticosteroid. Indian J. Dermatol. Venereol. Leprol. 2013, 79, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, M.G.; Miliszewski, M.A.; Sikora, S.; Papp, A.; Dutz, J.P. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J. Am. Acad. Dermatol. 2014, 71, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Mckenzie, E.; Owen, C.; Callen, J. The use of cyclosporine for Stevens-Johnson syndrome and toxic epidermal necrolysis: The University of Louisville experience. J. Am. Acad. Dermatol. 2016, 74, AB175. [Google Scholar]
- Mohanty, S.; Das, A.; Ghosh, A.; Sil, A.; Gharami, R.C.; Bandyopadhyay, D.; Das, N.K. Effectiveness, safety and to1erabi1ity of cyclosporine versus supportive treatment in Stevens-Johnson syndrome/toxic epidermal necrolysis: A record-based study. Indian J. Dermatol. Venereol. Leprol. 2017, 83, 312–316. [Google Scholar] [CrossRef]
- Lee, H.Y.; Fook-Chong, S.; Koh, H.Y.; Thirumoorthy, T.; Pang, S.M. Cyclosporine treatment for Stevens-Johnson syndrome/toxic epidermal necrolysis: Retrospective analysis of a cohort treated in a specialized referral center. J. Am. Acad. Dermatol. 2017, 76, 106–113. [Google Scholar] [CrossRef]
- González-Herrada, C.; Rodríguez-Martín, S.; Cachafeiro, L.; Lerma, V.; González, O.; Lorente, J.A.; Rodríguez-Miguel, A.; González-Ramos, J.; Roustan, G.; Ramírez, E.; et al. Cyclosporine use in epidermal necrolysis is associated with an important mortality reduction: Evidence from three different approaches. J. Investig. Dermatol. 2017, 137, 2092–2100. [Google Scholar] [CrossRef]
- Poizeau, F.; Gaudin, O.; Le Cleach, L.; Duong, T.A.; Hua, C.; Hotz, C.; Ingen-Housz-Oro, S.; Sbidian, E.; Zehou, O.; Colin, A.; et al. Cyclosporine for Epidermal Necrolysis: Absence of Beneficial Effect in a Retrospective Cohort of 174 Patients-Exposed/Unexposed and Propensity Score-Matched Analyses. J. Investig. Dermatol. 2018, 138, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Noe, M.H.; Mostaghimi, A.; Rosenbach, M.; Shinkai, K.; Micheletti, R.G. Selective Use of Cyclosporine for Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis May Exclude Patients with Poor Prognostic Factors. J. Investig. Dermatol. 2018, 138, 2068–2072. [Google Scholar] [CrossRef] [PubMed]
- Kuijper, E.C.; French, L.E.; Tensen, C.P.; Vermeer, M.H.; Bavinck, B.J.N. Clinical and pathogenic aspects of the severe cutaneous adverse reaction epidermal necrolysis (EN). J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1957–1971. [Google Scholar] [CrossRef] [PubMed]
- Caproni, M.; Torchia, D.; Schincaglia, E.; Volpi, W.; Frezzolini, A.; Schena, D.; Marzano, A.; Quaglino, P.; De Simone, C.; Parodi, A.; et al. Expression of cytokines and chemokine receptors in the cutaneous lesions of erythema multiforme and Stevens-Johnson syndrome/toxic epidermal necrolysis. Br. J. Dermatol. 2006, 155, 722–728. [Google Scholar] [CrossRef]
- Wolkenstein, P.; Latarjet, J.; Roujeau, J.C.; Duguet, C.; Boudeau, S.; Vaillant, L.; Maignan, M.; Schuhmacher, M.H.; Milpied, B.; Pilorget, A.; et al. Randomised comparison of thalidomide versus placebo in toxic epidermal necrolysis. Lancet 1998, 352, 1586–1589. [Google Scholar] [CrossRef]
- Fischer, M.; Fiedler, E.; Marsch, W.C.; Wohlrab, J. Antitumour necrosis factor-alpha antibodies (infliximab) in the treatment of a patient with toxic epidermal necrolysis. Br. J. Dermatol. 2002, 146, 707–709. [Google Scholar] [CrossRef]
- Hunger, R.E.; Hunziker, T.; Buettiker, U.; Braathen, L.R.; Yawalkar, N. Rapid resolution of toxic epidermal necrolysis with anti-TNF-alpha treatment. J. Allergy Clin. Immunol. 2005, 116, 923–924. [Google Scholar] [CrossRef]
- Al-Shouli, S.; Abouchala, N.; Bogusz, M.J.; Al Tufail, M.; Thestrup-Pedersen, K. Toxic epidermal necrolysis associated with high intake of sildenafil and its response to infliximab. Acta Derm. Venereol. 2005, 85, 534–535. [Google Scholar] [CrossRef]
- Wojtkiewicz, A.; Wysocki, M.; Fortuna, J.; Chrupek, M.; Matczuk, M.; Koltan, A. Beneficial and rapid effect of infliximab on the course of toxic epidermal necrolysis. Acta Derm. Venereol. 2008, 88, 420–421. [Google Scholar]
- Patmanidis, K.; Sidiras, A.; Dolianitis, K.; Simelidis, D.; Solomonidis, C.; Gaitanis, G.; Bassukas, I.D. Combination of infliximab and high-dose intravenous immunoglobulin for toxic epidermal necrolysis: Successful treatment of an elderly patient. Case Rep. Dermatol. Med. 2012, 2012, 915314. [Google Scholar] [CrossRef]
- Zárate-Correa, L.C.; Carrillo-Gómez, D.C.; Ramírez-Escobar, A.F.; Serrano-Reyes, C. Toxic epi-dermal necrolysis successfully treated with infliximab. J. Investig. Allergol. Clin. Immunol. 2013, 23, 61–63. [Google Scholar] [PubMed]
- Scott-Lang, V.; Tidman, M.; McKay, D. Toxic Epidermal Necrolysis in a Child Successfully Treated with Infliximab. Pediatr. Dermatol. 2014, 31, 532–534. [Google Scholar] [CrossRef] [PubMed]
- Paradisi, A.; Abeni, D.; Bergamo, F.; Ricci, F.; Didona, D.; Didona, B. Etanercept therapy for toxic epidermal necrolysis. J. Am. Acad. Dermatol. 2014, 71, 278–283. [Google Scholar] [CrossRef]
- Famularo, G.; Di Dona, B.; Canzona, F.; Girardelli, C.R.; Cruciani, G. Etanercept for toxic epidermal necrolysis. Ann. Pharmacother. 2007, 41, 1083–1084. [Google Scholar] [CrossRef] [PubMed]
- Gubinelli, E.; Canzona, F.; Tonanzi, T.; Raskovic, D.; Didona, B. Toxic epidermal necrolysis successfully treated with etanercept. J. Dermatol. 2009, 36, 150–153. [Google Scholar] [CrossRef]
- Wang, C.W.; Yang, L.Y.; Chen, C.B.; Ho, H.C.; Hung, S.I.; Yang, C.H.; Chang, C.J.; Su, S.C.; Hui, R.C.; Chin, S.W.; et al. Randomized, controlled trial of TNF-α antagonist in CTL-mediated severe cutaneous adverse reactions. J. Clin. Investig. 2018, 128, 985–996. [Google Scholar] [CrossRef]
- Gaitanis, G.; Spyridonos, P.; Patmanidis, K.; Koulouras, V.; Nakos, G.; Tzaphlidou, M.; Bassukas, I.D. Treatment of toxic epidermal necrolysis with the combination of infliximab and high-dose intravenous immunoglobulin. Dermatology 2012, 224, 134–139. [Google Scholar] [CrossRef]
- Chong, I.; Chao, A. Stevens-Johnson syndrome/toxic epidermal necrolysis and treatment with a biologic: A case report. Perm. J. 2017, 21, 16–60. [Google Scholar] [CrossRef]
- Vivar, K.L.; Deschaine, M.; Messina, J.; Divine, J.M.; Rabionet, A.; Patel, N.; Harrington, M.A.; Seminario-Vidal, L. Epidermal programmed cell death-ligand 1 expression in TEN associated with nivolumab therapy. J. Cutan. Pathol. 2017, 44, 381–384. [Google Scholar] [CrossRef]
- Jiang, Y.-Y.; Nguyen, G.H.; Jin, H.-Z.; Zeng, Y.-P. Methazolamide-induced toxic epidermal necrolysis in a man carrying HLA-B*59:01: Successful treatment with infliximab and glucocorticoid. Int. J. Dermatol. 2018, 57, 494–496. [Google Scholar] [CrossRef]
- Wang, F.; Gao, X.; Chen, X.; Tang, X.; Chen, H.; Han, J. Successful treatment of interstitial lung disease related to Stevens-Johnson syndrome/toxic epidermal necrolysis overlap with etanercept: A case report and published work review. J. Dermatol. 2019, 46, 1035–1038. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.-H.; Liu, M.-T.; Chung, W.-H.; Lu, C.-W. Toxic epidermal necrolysis induced by human herpes virus 7 treated with a tumor necrosis factor-α inhibitor. J. Dermatol. 2020, 47, 1179–1181. [Google Scholar] [CrossRef] [PubMed]
- Estébanez, A.; Såez-Martin, L.C.; Muöoz, J.I.; Silva, E.; Monrabal, A.; Monteagudo, C.; Ramón, M.D. Levetiracetam-induced pediatric toxic epidermal necrolysis successfully treated with etanercept. Pediatr. Dermatol. 2020, 37, 701–705. [Google Scholar] [CrossRef]
- Ao, S.; Gao, X.; Zhan, J.; Ai, L.; Li, M.; Su, H.; Tang, X.; Chu, C.; Han, J.; Wang, F. Inhibition of tumor necrosis factor improves conventional steroid therapy for Stevens-Johnson syndrome/toxic epidermal necrolysis in a cohort of patients. J. Am. Acad. Dermatol. 2022, 86, 1236–1245. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, C.-W.; Chen, C.-B.; Wang, C.-W.; Chen, W.-T.; Cheng, B.; Ji, C.; Chung, W.-H. Evaluation of Combination Therapy with Etanercept and Systemic Corticosteroids for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Multicenter Observational Study. J. Allergy Clin. Immunol. Pract. 2022, 10, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Kreft, B.; Lieser, U.; Haase, R.; Marsch, W.C.; Wohlrab, J. Extensive hypertrophic scarring after toxic epidermal necrolysis in a child. Pediatr. Dermatol. 2014, 31, 527–528. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhong, S.; Tu, P.; Li, R.; Wang, M. Rapid remission of Stevens-Johnson syndrome by combination therapy using etanercept and intravenous immunoglobulin and a review of the literature. Dermatol. Ther. 2019, 32, e12832. [Google Scholar] [CrossRef]
- Pham, C.H.; Gillenwater, T.J.; Nagengast, E.; McCullough, M.C.; Peng, D.H.; Garner, W.L. Combination therapy: Etanercept and intravenous immunoglobulin for the acute treatment of Stevens-Johnson syndrome/toxic epidermal necrolysis. Burns 2019, 45, 1634–1638. [Google Scholar] [CrossRef]
- López-Gómez, V.; Yarza, R.; Muñoz-González, H.; Revilla, E.; Enrech, S.; González-Valle, O.; Tolosa, P.; Ciruelos, E. Ribociclib-Related Stevens-Johnson Syndrome: Oncologic Awareness, Case Report, and Literature Review. J. Breast Cancer 2019, 22, 661–666. [Google Scholar] [CrossRef]
- Gavigan, G.M.; Kanigsberg, N.D.; Ramien, M.L. Pediatric Stevens-Johnson syndrome/toxic epidermal necrolysis halted by etanercept. J. Cutan. Med. Surg. 2018, 22, 514–515. [Google Scholar] [CrossRef]
- Coulombe, J.; Belzile, E.; Duhamel, A.; Rault, P.; Buteau, C.; DeBruycker, J.J.; Bussières, J.F. Pediatric SJS/TEN subdued by a combination of dexamethasone, cyclosporine, and etanercept. J. Cutan. Med. Surg. 2019, 23, 547–550. [Google Scholar] [CrossRef]
- Sibbald, C.; Putteman, E.; Micheletti, R.; Treat, J.; Castelo-Soccio, L. Retrospective review of drug-induced Stevens-Johnson syndrome and toxic epidermal necrolysis cases at a pediatric tertiary care institution. Pediatr. Dermatol. 2020, 37, 461–466. [Google Scholar] [CrossRef]
- Holtz, M.; Grimstad, F.; Strickland, J.; Dowlut-McElroy, T. Vulvovaginal involvement in pediatric Stevens-Johnsons syndrome: A case series. J. Pediatr. Adolesc. Gynecol. 2019, 32, 233–234. [Google Scholar] [CrossRef]
- Paquet, P.; Jennes, S.; Rousseau, A.F.; Libon, F.; Delvenne, P.; Piérard, G.E. Effect of N-acetylcysteine combined with infliximab on toxic epidermal necrolysis. A proof-of-concept study. Burns 2014, 40, 1707–1712. [Google Scholar] [CrossRef] [PubMed]
- Kamanabroo, D.; Schmitz-Landgraf, W.; Czarnetzki, B.M. Plasmapheresis in Severe Drug-Induced Toxic Epidermal Necrolysis. Arch. Dermatol. 1985, 121, 1548–1549. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, G.; Koukoudis, P.; Karpouzas, J.; Alexopoulos, E.; Papadopoulou, D.; Chrisomalis, F.; Skenteris, N.; Tsakaris, D.; Papadimitriou, M. Plasma Exchange (Pe) Treatment in Drug-Induced Toxic Epidermal Necrolysis (Ten). Int. J. Artif. Organs. 1991, 14, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Chaidemenos, G.C.; Chrysomallis, F.; Sombolos, K.; Mourellou, O.; Ioannides, D.; Papakonstantinou, M. Plasmapheresis in toxic epidermal necrolysis. Int. J. Dermatol. 1997, 36, 218–221. [Google Scholar] [CrossRef]
- Yamada, H.; Takamori, K.; Yaguchi, H.; Ogawa, H. A Study of the Efficacy of Plasmapheresis for the Treatment of Drug Induced Toxic Epidermal Necrolysis. Ther. Apher. 1998, 2, 153–156. [Google Scholar] [CrossRef]
- Egan, C.A.; Grant, W.J.; Morris, S.E.; Saffle, J.R.; Zone, J.J. Plasmapheresis as an adjunct treatment in toxic epidermal necrolysis. J. Am. Acad. Dermatol. 1999, 40, 458–461. [Google Scholar] [CrossRef]
- Bamichas, G.; Natse, T.; Christidou, F.; Stangou, M.; Karagianni, A.; Koukourikos, S.; Chaidemenos, G.; Chrysomallis, F.; Sombolos, K. Plasma exchange in patients with toxic epidermal necrolysis. Ther. Apher. 2002, 6, 225–228. [Google Scholar] [CrossRef]
- Narita, Y.M.; Hirahara, K.; Mizukawa, Y.; Kano, Y.; Shiohara, T. Efficacy of plasmapheresis for the treatment of severe toxic epidermal necrolysis: Is cytokine expression analysis useful in predicting its therapeutic efficacy? J. Dermatol. 2011, 38, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Zhang, J.; Guo, Q.; Feng, Y.; Gao, Y.; Guo, L.; Hou, Y.; An, J.; Wang, X.; Yan, B.; et al. Successful treatment of toxic epidermal necrolysis using plasmapheresis: A prospective observational study. J. Crit. Care 2017, 42, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Furubacke, A.; Berlin, G.; Anderson, C.; Sjöberg, F. Lack of significant treatment effect of plasma exchange in the treatment of drug-induced toxic epidermal necrolysis? Intensive Care Med. 1999, 25, 1307–1310. [Google Scholar] [CrossRef] [PubMed]
- Giudice, G.; Maggio, G.; Bufano, L.; Memeo, G.; Vestita, M. Management of toxic epidermal necrolysis with plasmapheresis and cyclosporine A: Our10 years’ experience. Plast. Reconstr. Surg. Glob. Open 2017, 5, e1221. [Google Scholar] [CrossRef]
- Krajewski, A.; Mazurek, M.J.; Mlynska-Krajewska, E.; Piorun, K.; Knakiewicz, M.; Markowska, M. Toxic Epidermal Necrolysis Therapy with TPE and IVIG-10 Years of Experience of the Burns Treatment Center. J. Burn. Care Res. 2019, 40, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Lissia, M.; Figus, A.; Rubino, C. Intravenous immunoglobulins and plasmapheresis combined treatment in patients with severe toxic epidermal necrolysis: Preliminary report. Br. J. Plast. Surg. 2005, 58, 504–510. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Included Studies/Treatment | Summary of Potential Treatments with Benefits |
|---|---|---|
| Huang et al., 2012 [16] | 17 studies/IVIg | Both high-dose and low-dose IVIg were not associated with survival benefit. |
| Barron et al., 2015 [17] | 13 studies/IVIg | Increasing dose of IVIg was associated with decreased mortality. |
| Ye et al., 2016 [18] | 26 studies/IVIg + corticosteroid | Combination of IVIg and corticosteroid markedly reduced recovery time but not mortality. |
| Huang et al., 2016 [19] | 11 studies/IVIg | IVIg was ineffective in reducing mortality in TEN patients, even at high-dose. |
| Zimmermann et al., 2017 [20] | 96 studies/multiple | Glucocorticoids and cyclosporine were the most promising treatment. |
| Ng et al., 2018 [21] | 9 studies/cyclosporine | Cyclosporine significantly reduced mortality. |
| Zhang et al., 2019 [22] | 27 studies/TNF-α inhibitors | Biologic TNF-α inhibitors (infliximab and etanercept) are safe and effective treatments. |
| Patel et al., 2021 [23] | 24 studies/multiple | Cyclosporine reduced mortality in TEN patients. Etanercept and combination of IVIg and corticosteroid and were also promising. |
| Torres-Navarro et al., 2021 [24] | 38 studies/multiple | The meta-regression analysis confirmed that cyclosporine and combination of IVIg and corticosteroid were associated with less deaths than predicted by SCORTEN. |
| Sachdeva et al., 2021 [25] | 38 studies/biologics | TNF-α inhibitors monotherapy improved outcomes and may be safer compared to combination therapy. |
| Tsai et al., 2021 [26] | 66 studies/multiple | Combination of IVIg and corticosteroid was the only treatment with significant survival benefits. |
| Krajewski et al., 2022 [27] | 42 studies/multiple | The lowest mortality was found in etanercept group followed by cyclosporine. |
| Houschyar et al., 2021 [28] | 16 studies/multiple | Systemic glucocorticoids showed a survival benefit. Cyclosporine also showed promising results. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.-C.; Wang, T.-J.; Lin, M.-H.; Chen, T.-J. A Review of the Systemic Treatment of Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis. Biomedicines 2022, 10, 2105. https://doi.org/10.3390/biomedicines10092105
Chang H-C, Wang T-J, Lin M-H, Chen T-J. A Review of the Systemic Treatment of Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis. Biomedicines. 2022; 10(9):2105. https://doi.org/10.3390/biomedicines10092105
Chicago/Turabian StyleChang, Hua-Ching, Tsung-Jen Wang, Ming-Hsiu Lin, and Ting-Jui Chen. 2022. "A Review of the Systemic Treatment of Stevens–Johnson Syndrome and Toxic Epidermal Necrolysis" Biomedicines 10, no. 9: 2105. https://doi.org/10.3390/biomedicines10092105