
Early Diagnosis in Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS) by Focusing on Major Clinical Clues: Beyond Ataxia and Vestibular Impairment

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Genetic Testing
2.3. Other Laboratory Testing
2.4. Skin Biopsy
2.5. Nerve Biopsy
3. Results
3.1. Main Clinical Findings
3.2. Initial Diagnosis and Course
3.3. Laboratory Investigations
3.4. Molecular Analysis
3.5. Skin and Nerve Biopsy Findings
3.5.1. Skin Biopsy
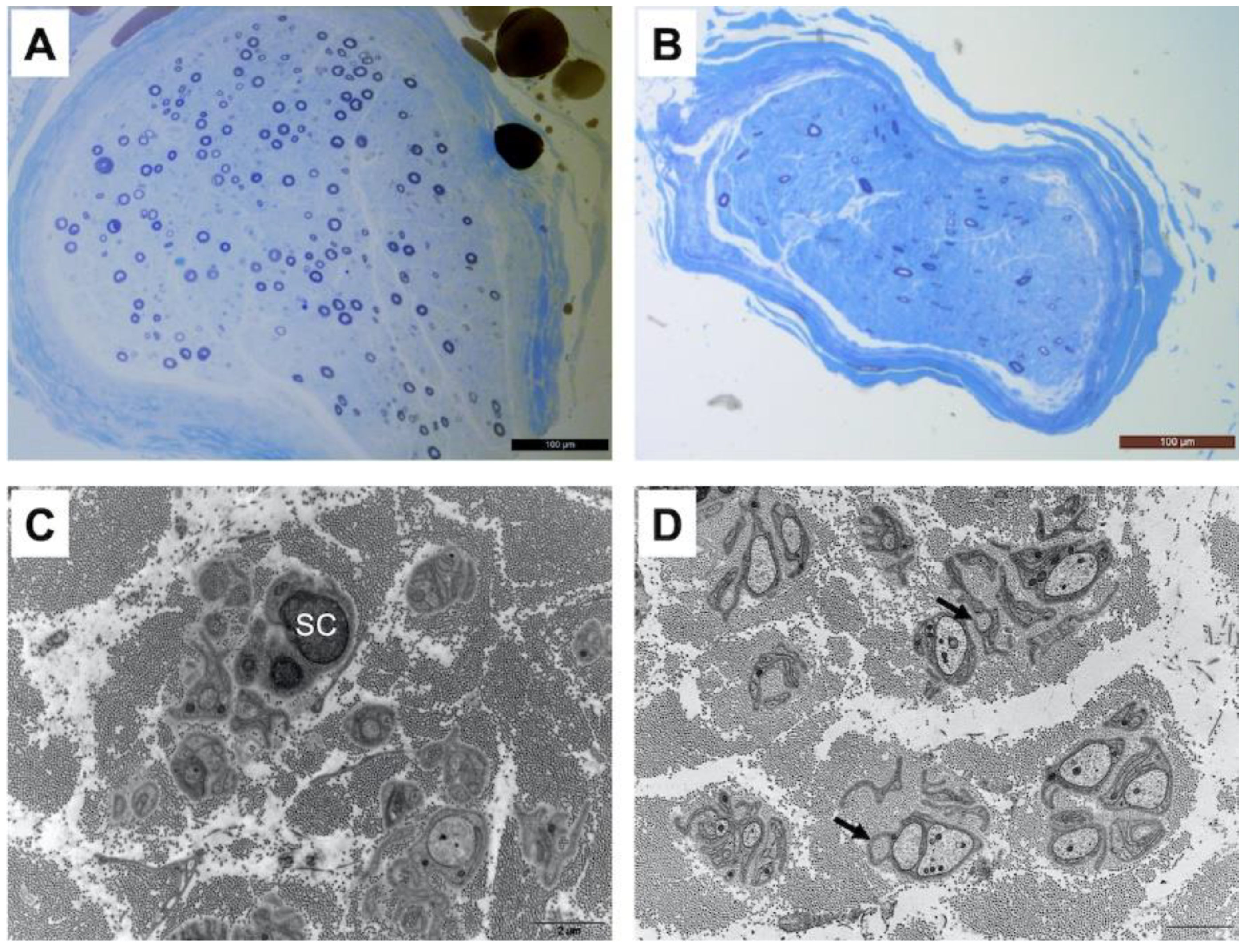
3.5.2. Nerve Biopsy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cortese, A.; Simone, R.; Sullivan, R.; Vandrovcova, J.; Tariq, H.; Yau, W.Y.; Humphrey, J.; Jaunmuktane, Z.; Sivakumar, P.; Polke, J.; et al. Biallelic expansion of an intronic repeat in RFC1 is a common cause of late-onset ataxia. Nat Genet. 2019, 51, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Szmulewicz, D.J.; Seiderer, L.; Halmagyi, G.M.; Storey, E.; Roberts, L. Neurophysiological evidence for generalized sensory neuronopathy in cerebellar ataxia with neuropathy and bilateral vestibular areflexia syndrome. Muscle Nerve 2014, 51, 600–603. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, A.; Halmagyi, G.M.; McGarvie, L.A.; Cremer, P.D. Cerebellar ataxia with bilateral vestibulopathy: Description of a syndrome and its characteristic clinical sign. Brain 2004, 127, 280–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szmulewicz, D.J.; Waterston, J.A.; Halmagyi, G.M.; Mossman, S.; Chancellor, A.M.; McLean, C.A.; Storey, E. Sensory neuropathy as part of the cerebellar ataxia neuropathy vestibular areflexia syndrome. Neurology 2011, 76, 1903–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortese, A.; Tozza, S.; Yau, W.Y.; Rossi, S.; Beecroft, S.J.; Jaunmuktane, Z.; Dyer, Z.; Ravenscroft, G.; Lamont, P.J.; Mossman, S.; et al. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome due to RFC1 repeat expansion. Brain 2020, 143, 480–490. [Google Scholar] [CrossRef]
- Mazzone, S.B.; Farrell, M.J. Heterogeneity of cough neurobiology: Clinical implications. Pulm. Pharmacol. Ther. 2019, 55, 62–66. [Google Scholar] [CrossRef]
- Akçimen, F.; Ross, J.P.; Bourassa, C.V.; Liao, C.; Rochefort, D.; Gama, M.T.D.; Dicaire, M.-J.; Barsottini, O.G.; Brais, B.; Pedroso, J.L.; et al. Investigation of the RFC1 Repeat Expansion in a Canadian and a Brazilian Ataxia Cohort: Identification of Novel Conformations. Front. Genet. 2019, 10, 1219. [Google Scholar] [CrossRef] [Green Version]
- Boukhris, S.; Magy, L.; Kabore, R.; Mabrouk, T.; Li, Y.; Sindou, P.; Tabaraud, F.; Vallat, J.-M. Atypical electrophysiologic findings in chronic inflammatory demyelinating polyneuropathy (CIDP)—Diagnosis confirmed by nerve biopsy. Neurophysiol. Clin. 2004, 34, 71–79. [Google Scholar] [CrossRef]
- Lauria, G.; Cornblath, D.R.; Johansson, O.; McArthur, J.C.; Mellgren, S.I.; Nolano, M.; Rosenberg, N.; Sommer, C. EFNS guidelines on the use of skin biopsy in the diagnosis of peripheral neuropathy. Eur. J. Neurol. 2005, 12, 747–758. [Google Scholar] [CrossRef]
- Duchesne, M.; Danigo, A.; Richard, L.; Vallat, J.-M.; Attarian, S.; Gonnaud, P.-M.; Lacour, A.; Péréon, Y.; Stojkovic, T.; Nave, K.-A.; et al. Skin Biopsy Findings in Patients with CMT1A: Baseline Data From the CLN-PXT3003-01 Study Provide New Insights into the Pathophysiology of the Disorder. J. Neuropathol. Exp. Neurol. 2018, 77, 274–281. [Google Scholar] [CrossRef]
- Vallat, J.-M.; Funalot, B.; Magy, L. Nerve biopsy: Requirements for diagnosis and clinical value. Acta Neuropathol. 2011, 121, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Gorson, K.C.; Herrmann, D.N.; Thiagarajan, R.; Brannagan, T.H.; Chin, R.L.; Kinsella, L.J.; Ropper, A.H. Non-length dependent small fibre neuropathy/ganglionopathy. J. Neurol. Neurosurg. Psychiatry 2008, 79, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Provitera, V.; Gibbons, C.H.; Wendelschafer-Crabb, G.; Donadio, V.; Vitale, D.F.; Loavenbruck, A.; Stancanelli, A.; Caporaso, G.; Liguori, R.; Wang, N.; et al. The role of skin biopsy in differentiating small-fiber neuropathy from ganglionopathy. Eur. J. Neurol. 2018, 25, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Szmulewicz, D.J.; Waterston, J.A.; MacDougall, H.; Mossman, S.; Chancellor, A.M.; McLean, C.A.; Merchant, S.; Patrikios, P.; Halmagyi, G.M.; Storey, E. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS): A review of the clinical features and video-oculographic diagnosis. Ann. N. Y. Acad. Sci. 2011, 1233, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mathis, S.; Duval, F.; Soulages, A.; Solé, G.; Le Masson, G. The ataxic neuropathies. J. Neurol. 2020, 268, 3675–3689. [Google Scholar] [CrossRef]
- Burke, D.; Halmagyi, G.M. Normal tendon reflexes despite absent sensory nerve action potentials in CANVAS: A neurophysiological study. J. Neurol. Sci. 2018, 387, 75–79. [Google Scholar] [CrossRef]
- Dominik, N.; Deforie, V.G.; Cortese, A.; Houlden, H. CANVAS: A late onset ataxia due to biallelic intronic AAGGG expansions. J. Neurol. 2020, 268, 1119–1126. [Google Scholar] [CrossRef]
- Umeh, C.C.; Polydefkis, M.; Chaudhry, V.; Zee, D.S. Sweat Gland Denervation in Cerebellar Ataxia with Neuropathy and Vestibular Areflexia Syndrome (CANVAS). Mov. Disord. Clin. Pract. 2017, 4, 46–48. [Google Scholar] [CrossRef]
- Szmulewicz, D.J.; McLean, C.A.; MacDougall, H.G.; Roberts, L.; Storey, E.; Halmagyi, G.M. CANVAS an update: Clinical presentation, investigation and management. J. Vestib. Res. 2014, 24, 465–474. [Google Scholar] [CrossRef] [Green Version]
- Bakkers, M.; Faber, C.G.; Hoeijmakers, J.G.; Lauria, G.; Merkies, I.S. Small fibers, large impact: Quality of life in small-fiber neuropathy. Muscle Nerve 2013, 49, 329–336. [Google Scholar] [CrossRef]
- Infante, J.; García, A.; Serrano-Cárdenas, K.M.; González-Aguado, R.; Gazulla, J.; de Lucas, E.M.; Berciano, J. Cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS) with chronic cough and preserved muscle stretch reflexes: Evidence for selective sparing of afferent Ia fibres. J. Neurol. 2018, 265, 1454–1462. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, S.B.; Chung, K.F.; McGarvey, L. The heterogeneity of chronic cough: A case for endotypes of cough hypersensitivity. Lancet Respir. Med. 2018, 6, 636–646. [Google Scholar] [CrossRef]
- Chung, K.F.; McGarvey, L.; Mazzone, S.B. Chronic cough as a neuropathic disorder. Lancet Respir. Med. 2013, 1, 414–422. [Google Scholar] [CrossRef]
- Canning, B.J.; Mazzone, S.B.; Meeker, S.N.; Mori, N.; Reynolds, S.M.; Undem, B.J. Identification of the tracheal and laryngeal afferent neurones mediating cough in anaesthetized guinea-pigs. J. Physiol. 2004, 557, 543–558. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient | Age at Referral | Family History | Duration of Sensory Symptoms (Years) | Initial Suspected Diagnosis | Pain | Duration of Unexplained Cough before Neurological Presentation (Years) | Ataxia at Referral | Cerebellar Atrophy | NCS Pattern | IEFND at the Thigh/Leg (Fibers/mm) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 62 | Yes | 5 | Immune-mediated | Yes | 20 | No | ND | SNN | 0.25/0.49 |
| 2 | 57 | Yes | 5 | CANVAS | Yes | 10 | Mild | ND | SNN | 0/0.53 |
| 3 | 52 | Yes | 3 | Immune-mediated | Yes | 10 | Mild | Slight | SNN | 0/0 |
| 4 | 52 | Yes | 3 | CANVAS | Yes | 20 | No | Slight | SNN | 0/0 |
| 5 | 61 | No | 7 | Immune-mediated | Yes | 20 | Mild | Slight | SNN | 0.34/0 |
| 6 | 58 | No | 3 | Immune-mediated | Yes | 15 | Moderate | ND | SNN | 0/0.17 |
| 7 | 62 | No | 8 | Immune-mediated | Yes | NA | Moderate | Slight | SNN | 0.51/0.37 |
| 8 | 55 | No | NA | CANVAS | No | 15 | Mild | ND | SNN | ND |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magy, L.; Chazelas, P.; Richard, L.; Deschamps, N.; Frachet, S.; Vallat, J.-M.; Magdelaine, C.; Favreau, F.; Bessaguet, F.; Lia, A.-S.; et al. Early Diagnosis in Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS) by Focusing on Major Clinical Clues: Beyond Ataxia and Vestibular Impairment. Biomedicines 2022, 10, 2046. https://doi.org/10.3390/biomedicines10082046
Magy L, Chazelas P, Richard L, Deschamps N, Frachet S, Vallat J-M, Magdelaine C, Favreau F, Bessaguet F, Lia A-S, et al. Early Diagnosis in Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS) by Focusing on Major Clinical Clues: Beyond Ataxia and Vestibular Impairment. Biomedicines. 2022; 10(8):2046. https://doi.org/10.3390/biomedicines10082046
Chicago/Turabian StyleMagy, Laurent, Pauline Chazelas, Laurence Richard, Nathalie Deschamps, Simon Frachet, Jean-Michel Vallat, Corinne Magdelaine, Frédéric Favreau, Flavien Bessaguet, Anne-Sophie Lia, and et al. 2022. "Early Diagnosis in Cerebellar Ataxia, Neuropathy, Vestibular Areflexia Syndrome (CANVAS) by Focusing on Major Clinical Clues: Beyond Ataxia and Vestibular Impairment" Biomedicines 10, no. 8: 2046. https://doi.org/10.3390/biomedicines10082046