
Ovarian Clear Cell Carcinoma and Mature Cystic Teratoma Transformed to PNET and Carcinosarcoma: A Case Report with an Immunohistochemical Investigation

 , and
, and 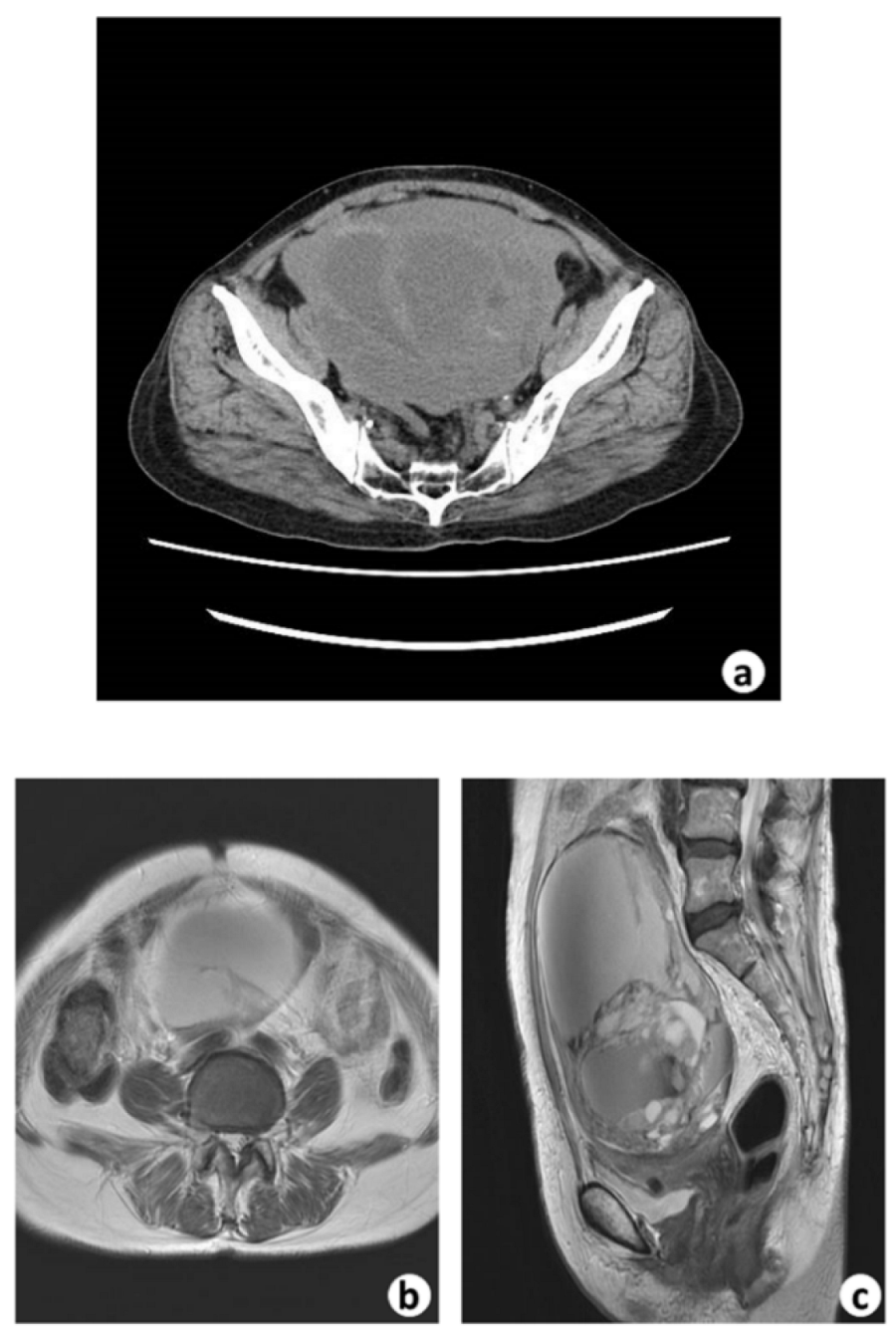{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
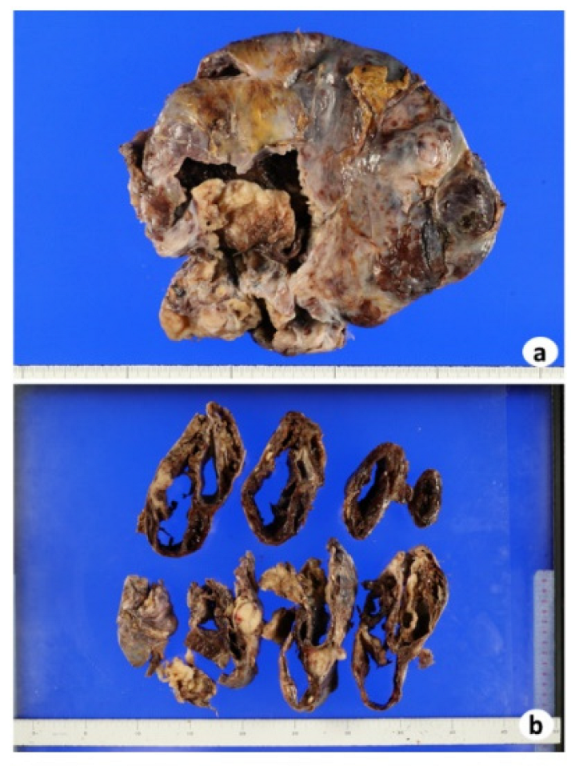
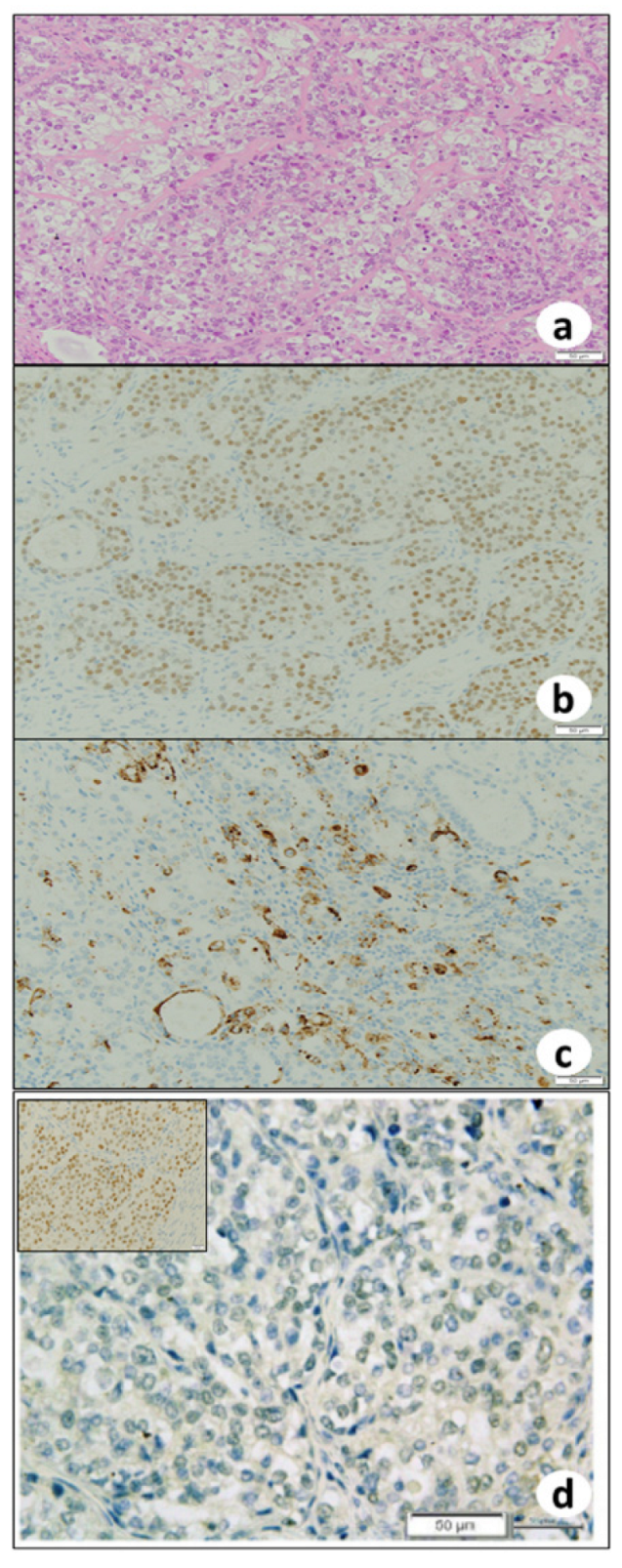
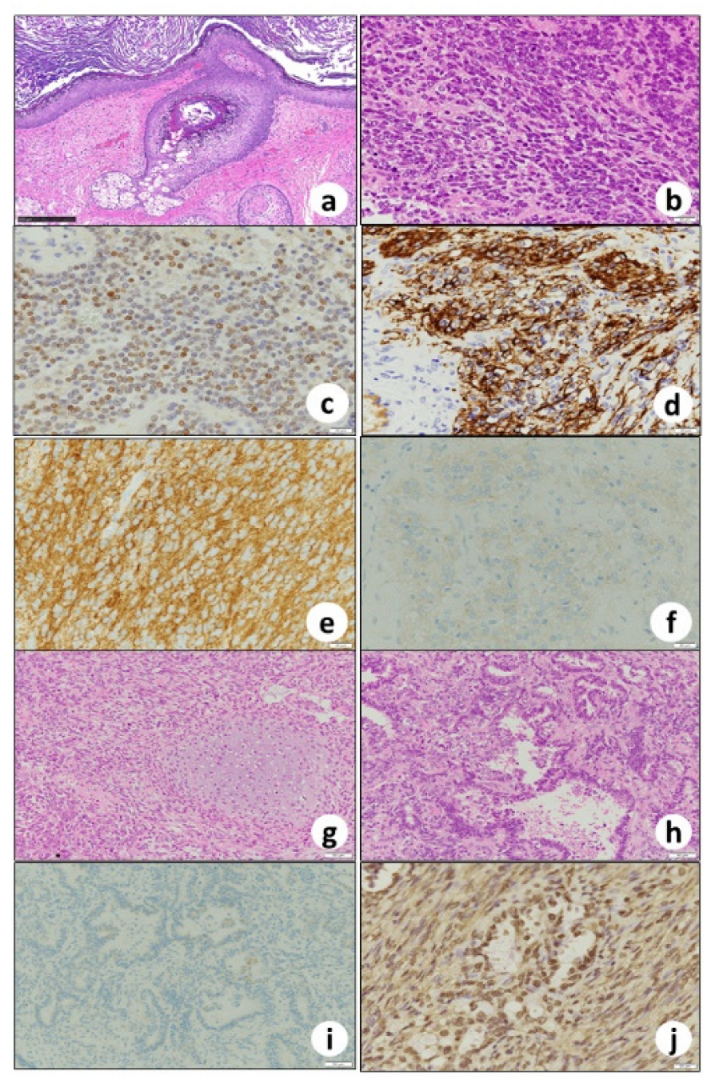
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cheung, A.N.; Ellenson, L.H.; Gilks, C.B.; Kim, K.-R.; Kong, C.S.; Lax, S.F.; Longacre, T.A.; Malpica, A.; McCluggage, W.G.; Oliva, E.; et al. Tumours of the ovary. In Female Genital Tumours; Board WCoTE; IARC Press: Lyon, France, 2020; pp. 31–167. [Google Scholar]
- Berton-Rigaud, D.; Devouassoux-Shisheboran, M.; Ledermann, J.A.; Leitao, M.M.; Powell, M.A.; Poveda, A.; Beale, P.; Glasspool, R.M.; Creutzberg, C.L.; Harter, P.; et al. Gynecologic Cancer InterGroup (GCIG) consensus review for uterine and ovarian carcinosarcoma. Int. J. Gynecol. Cancer 2014, 24, S55–S60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niwa, K.; Mori, S.; Kuwabara, K.; Nagata, K.; Takenaka, M.; Shiga, T.; Yamaguchi, Y.; Niwa, K.; Tanaka, T. Primary Ovarian Carcinosarcoma: Cytological, Pathological, Immunocytochemical, and Immunohistochemical Features. Open J. Pathol. 2021, 11, 22–31. [Google Scholar] [CrossRef]
- Ehrmann, R.L.; Weidner, N.; Welch, W.R.; Gleiberman, I. Malignant mixed mullerian tumor of the ovary with prominent neuroectodermal differentiation (teratoid carcinosarcoma). Int. J. Gynecol. Pathol. 1990, 9, 272–282. [Google Scholar] [CrossRef]
- Tanimoto, A.; Arima, N.; Hayashi, R.; Hamada, T.; Matsuki, Y.; Sasaguri, Y. Teratoid carcinosarcoma of the ovary with prominent neuroectodermal differentiation. Pathol. Int. 2001, 51, 829–832. [Google Scholar] [CrossRef]
- Heffner, D.K.; Hyams, V.J. Teratocarcinosarcoma (malignant teratoma?) of the nasal cavity and paranasal sinuses A clinicopathologic study of 20 cases. Cancer 1984, 53, 2140–2154. [Google Scholar] [CrossRef]
- Dunne, R.F.; Sahasrabudhe, D.M.; Messing, E.M.; Jean-Gilles, J.; Fung, C. A case series of transformation of teratoma to primitive neuroectodermal tumor: Evolving management of a rare malignancy. Rare Tumors 2014, 6, 5268. [Google Scholar] [CrossRef]
- Arora, D.S.; Haldane, S. Carcinosarcoma arising in a dermoid cyst of the ovary. J. Clin. Pathol. 1996, 49, 519–521. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Norquist, B.; Lacchetti, C.; Armstrong, D.; Grisham, R.N.; Goodfellow, P.J.; Kohn, E.C.; Levine, D.A.; Liu, J.F.; Lu, K.H.; et al. Germline and Somatic Tumor Testing in Epithelial Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 1222–1245. [Google Scholar] [CrossRef]
- Ulbright, T.M. Germ cell tumors of the gonads: A selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues. Mod. Pathol. 2005, 18 (Suppl. 2), S61–S79. [Google Scholar] [CrossRef]
- Wiegand, K.C.; Shah, S.P.; Al-Agha, O.M.; Zhao, Y.; Tse, K.; Zeng, T.; Senz, J.; McConechy, M.K.; Anglesio, M.S.; Kalloger, S.E.; et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N. Engl. J. Med. 2010, 363, 1532–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rorke, L.B. The cerebellar medulloblastoma and its relationship to primitive neuroectodermal tumors. J. Neuropathol. Exp. Neurol. 1983, 42, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaramillo-Huff, A.; Bakkar, R.; McKee, J.Q.; Sokkary, N. Primary Primitive Neuroectodermal Tumor Arising from an Ovarian Mature Cystic Teratoma in a 12-Year-Old Girl: A Case Report. J. Pediatr. Adolesc. Gynecol. 2017, 30, 511–512. [Google Scholar] [CrossRef] [PubMed]
- Cabibi, D.; Martorana, A.; Cappello, F.; Barresi, E.; Di Gangi, C.; Rodolico, V. Carcinosarcoma of monoclonal origin arising in a dermoid cyst of ovary: A case report. BMC Cancer 2006, 6, 47. [Google Scholar] [CrossRef] [Green Version]
- Allam-Nandyala, P.; Bui, M.M.; Caracciolo, J.T.; Hakam, A. Squamous cell carcinoma and osteosarcoma arising from a dermoid cyst--a case report and review of literature. Int. J. Clin. Exp. Pathol. 2010, 3, 313–318. [Google Scholar]
- Laury, A.R.; Perets, R.; Piao, H.; Krane, J.F.; Barletta, J.A.; French, C.; Chirieac, L.R.; Lis, R.; Loda, M.; Hornick, J.L.; et al. A comprehensive analysis of PAX8 expression in human epithelial tumors. Am. J. Surg. Pathol. 2011, 35, 816–826. [Google Scholar] [CrossRef] [Green Version]
- Tong, G.X.; Devaraj, K.; Hamele-Bena, D.; Yu, W.M.; Turk, A.; Chen, X.; Wright, J.D.; Greenebaum, E. Pax8: A marker for carcinoma of Mullerian origin in serous effusions. Diagn. Cytopathol. 2011, 39, 567–574. [Google Scholar] [CrossRef]
- Yachida, N.; Yoshihara, K.; Suda, K.; Nakaoka, H.; Ueda, H.; Sugino, K.; Yamaguchi, M.; Mori, Y.; Yamawaki, K.; Tamura, R.; et al. ARID1A protein expression is retained in ovarian endometriosis with ARID1A loss-of-function mutations: Implication for the two-hit hypothesis. Sci. Rep. 2020, 10, 14260. [Google Scholar] [CrossRef]
- Mathur, R. ARID1A loss in cancer: Towards a mechanistic understanding. Pharm. Ther. 2018, 190, 15–23. [Google Scholar] [CrossRef]
- Jones, S.; Wang, T.L.; Shih Ie, M.; Mao, T.L.; Nakayama, K.; Roden, R.; Glas, R.; Slamon, D.; Diaz, L.A., Jr.; Vogelstein, B.; et al. Frequent mutations of chromatin remodeling gene ARID1A in ovarian clear cell carcinoma. Science 2010, 330, 228–231. [Google Scholar] [CrossRef] [Green Version]
- Takeda, T.; Banno, K.; Okawa, R.; Yanokura, M.; Iijima, M.; Irie-Kunitomi, H.; Nakamura, K.; Iida, M.; Adachi, M.; Umene, K.; et al. ARID1A gene mutation in ovarian and endometrial cancers (Review). Oncol. Rep. 2016, 35, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollis, R.L.; Thomson, J.P.; Stanley, B.; Churchman, M.; Meynert, A.M.; Rye, T.; Bartos, C.; Iida, Y.; Croy, I.; Mackean, M.; et al. Molecular stratification of endometrioid ovarian carcinoma predicts clinical outcome. Nat. Commun. 2020, 11, 4995. [Google Scholar] [CrossRef] [PubMed]
- Leskela, S.; Romero, I.; Cristobal, E.; Perez-Mies, B.; Rosa-Rosa, J.M.; Gutierrez-Pecharroman, A.; Caniego-Casas, T.; Santon, A.; Ojeda, B.; Lopez-Reig, R.; et al. Mismatch Repair Deficiency in Ovarian Carcinoma: Frequency, Causes, and Consequences. Am. J. Surg. Pathol. 2020, 44, 649–656. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuo, M.; Saigo, C.; Takeuchi, T.; Onogi, A.; Watanabe, N.; Aikyo, S.; Toyoki, H.; Yanai, H.; Tanaka, T. Ovarian Clear Cell Carcinoma and Mature Cystic Teratoma Transformed to PNET and Carcinosarcoma: A Case Report with an Immunohistochemical Investigation. Biomedicines 2022, 10, 547. https://doi.org/10.3390/biomedicines10030547
Matsuo M, Saigo C, Takeuchi T, Onogi A, Watanabe N, Aikyo S, Toyoki H, Yanai H, Tanaka T. Ovarian Clear Cell Carcinoma and Mature Cystic Teratoma Transformed to PNET and Carcinosarcoma: A Case Report with an Immunohistochemical Investigation. Biomedicines. 2022; 10(3):547. https://doi.org/10.3390/biomedicines10030547
Chicago/Turabian StyleMatsuo, Mikiko, Chiemi Saigo, Tamotsu Takeuchi, Akane Onogi, Naoki Watanabe, Shinsuke Aikyo, Hiroshi Toyoki, Hiroyuki Yanai, and Takuji Tanaka. 2022. "Ovarian Clear Cell Carcinoma and Mature Cystic Teratoma Transformed to PNET and Carcinosarcoma: A Case Report with an Immunohistochemical Investigation" Biomedicines 10, no. 3: 547. https://doi.org/10.3390/biomedicines10030547