
Influence of DNA Mismatch Repair (MMR) System in Survival and Response to Immune Checkpoint Inhibitors (ICIs) in Non-Small Cell Lung Cancer (NSCLC): Retrospective Analysis


 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Collection and Construction of the Cohort
- Patients diagnosed with advanced or metastatic NSCLC.
- The patients must have received treatment with ICIs (Nivolumab) between 2015 and 2021.
- The existence of adequate samples from each patient in the Pathology Department of de University Hospital of Salamanca for IHC analysis.
- Patients over 18 years with full mental faculties who received and signed the informed consent for inclusion in the research project. After the age of 18, there is no age limit.
- Patients had to present an Eastern Cooperative Oncology Group (ECOG) 0-1.
- Refusal for inclusion in the research project by the patient or if age under 18 years old.
- Small cell lung cancer.
- First-line treatment with immunotherapy.
- No sample of primary tumor.
- ECOG ≥ 2
2.2. Analysis of MMR System Expression by IHC
2.3. Statistical Analysis
3. Results
3.1. General Analysis of the Sample
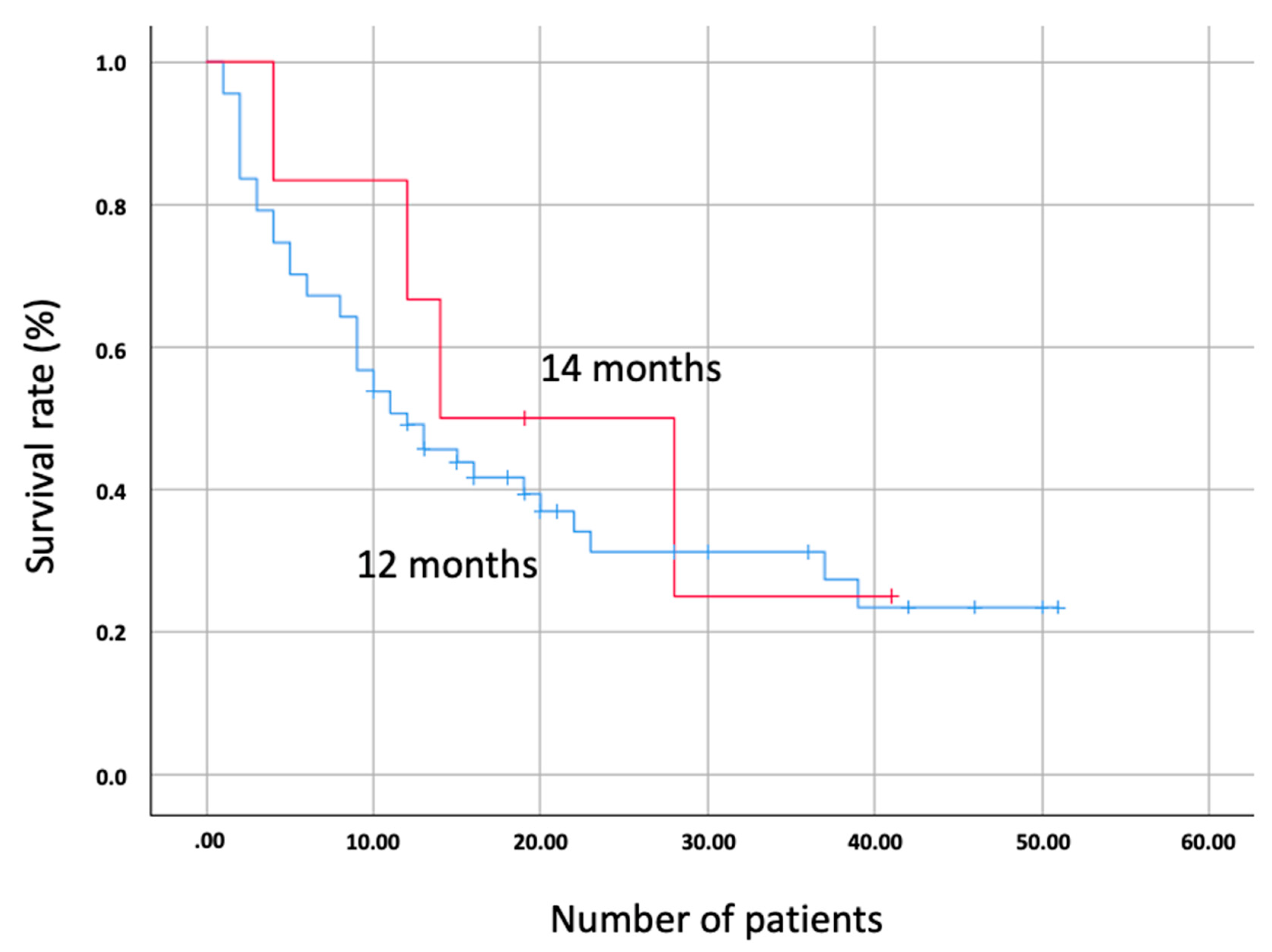
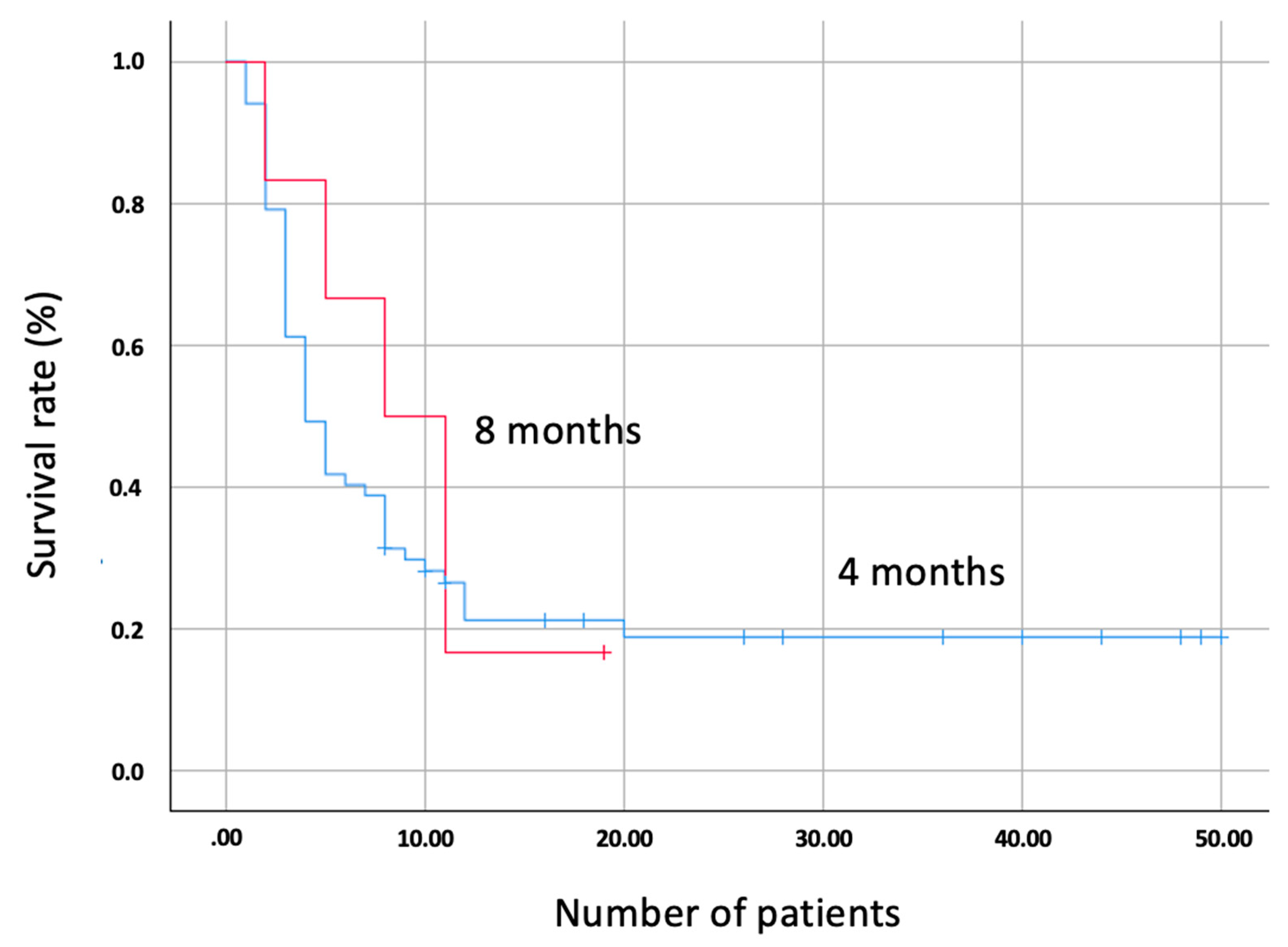
3.2. Survival Analysis by Expression of the MMR System
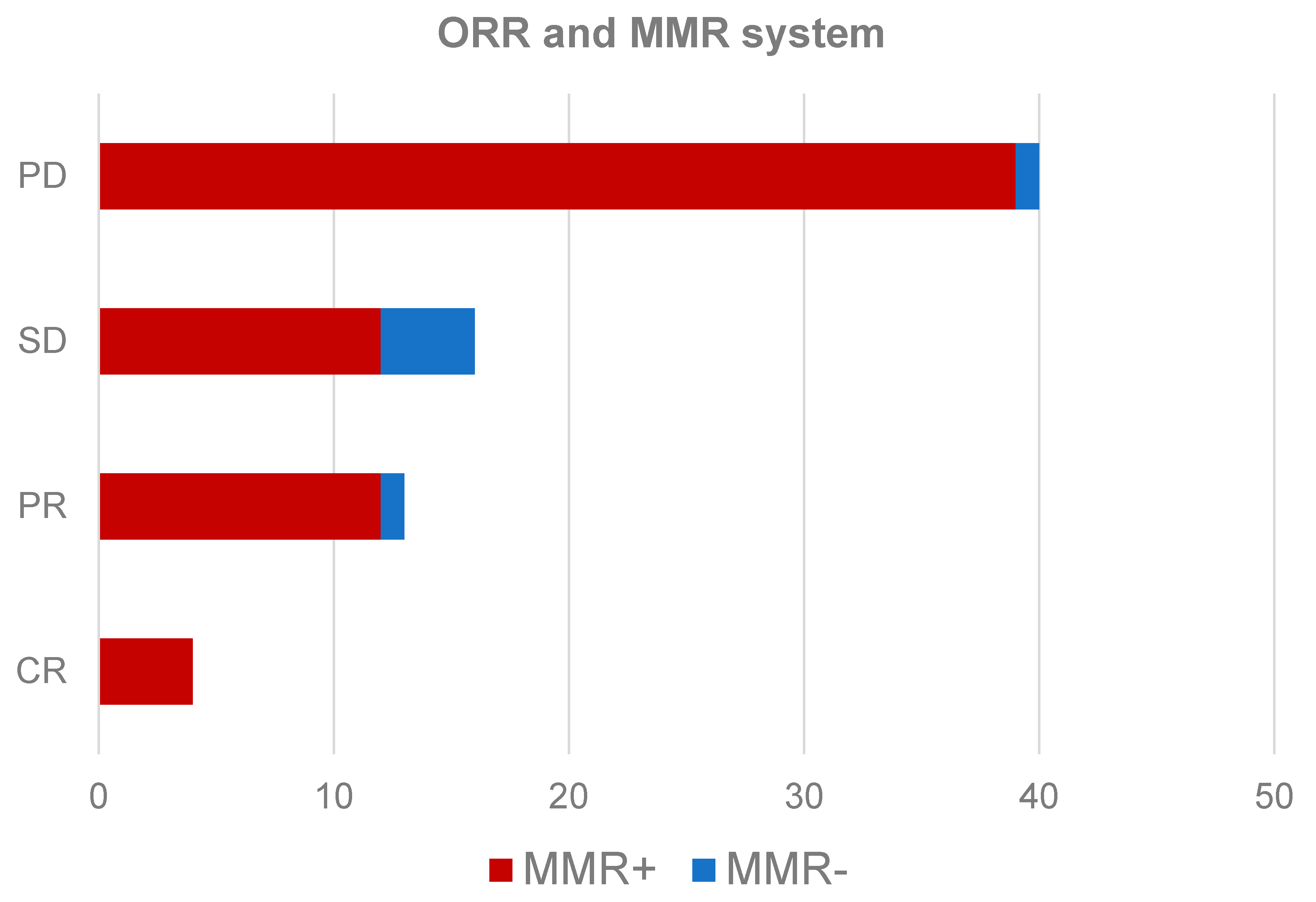
3.3. Analysis of Response by Expression of the MMR System
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with Ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Amanam, I.; Mambetsariev, I.; Gupta, R.; Achuthan, S.; Wang, Y.; Pharaon, R.; Massarelli, E.; Koczywas, M.; Reckamp, K.; Salgia, R. Role of immunotherapy and co-mutations on KRAS-mutant non-small cell lung cancer survival. J. Thorac. Dis. 2020, 12, 5086–5095. [Google Scholar] [CrossRef] [PubMed]
- Assoun, S.; Theou-Anton, N.; Nguenang, M.; Cazes, A.; Danel, C.; Abbar, B.; Pluvy, J.; Gounant, V.; Khalil, A.; Namour, C.; et al. Association of TP53 mutations with response and longer survival under immune checkpoint inhibitors in advanced non-small-cell lung cancer. Lung Cancer 2019, 132, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.D.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 mutations and PD-1 Inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, P.; Li, L.; Jiang, X.; Li, Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J. Hematol. Oncol. 2019, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Jiricny, J. The multifaceted mismatch-repair system. Nat. Rev. Mol. Cell. Biol. 2006, 7, 335–346. [Google Scholar] [CrossRef]
- Sahin, I.H.; Akce, M.; Alese, O.; Shaib, W.; Lesinsko, G.B.; El-Rayes, B.; Wu, C. Immune checkpoint inhibitors for the treatment of MSI-H/MMR-D colorectal cancer and a perspective on resistance mechanisms. Br. J. Cancer. 2019, 121, 809–818. [Google Scholar] [CrossRef]
- Viale, G.; Trapani, D.; Curigliano, G. Mismatch Repair Deficiency as a Predictive Biomarker for Immunotherapy Efficacy. Biomed. Res. Int. 2017, 2017, 4719194. [Google Scholar] [CrossRef]
- Lahtz, C.; Pfeifer, G.P. Epigenetic changes of DNA repair genes in cancer. J. Mol. Cell Biol. 2011, 3, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Warth, A.; Körner, S.; Penzel, R.; Muley, T.; Dienemann, H.; Schirmacher, P.; Von Knebel-Doeberitz, M.; Weichert, W.; Kloor, M. Microsatellite instability in pulmonary adenocarcinomas: A comprehensive study of 480 cases. Virchows Arch. 2016, 468, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Nojadeh, J.N.; Sharif, S.B.; Sakhinia, E. Microsatellite instability in colorectal cancer. EXCLI J. 2018, 17, 159–168. [Google Scholar] [PubMed]
- Brahmer, J.; Karen, L.R.; Baas, P.; Crinó, L.; Eberhardt, W.E.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non–small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non–small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Wang, X.; Tian, L.; Che, G. Microsatellite alteration in multiple primary lung cancer. J. Thorac. Dis. 2014, 6, 1499–1505. [Google Scholar]
- Xinarianos, G.; Scott, F.M.; Liloglou, T.; Prime, W.; Callaghan, J.; Gosney, J.R.; Field, J.K. Telomerase activity in non-small cell lung carcinomas correlates with smoking status. Int. J. Oncol. 1999, 15, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.H.; Ho, C.C.; Hsia, T.C.; Tseng, J.S.; Su, K.Y.; Wu, M.F.; Chiu, K.L.; Yang, T.Y.; Chen, K.C.; Ooi, H.; et al. Identification of five driver gene mutations in patients with treatment-naïve lung adenocarcinoma in Taiwan. PLoS ONE. 2015, 10, e0120852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doukas, S.G.; Vageli, D.P.; Nikolouzakis, T.K.; Falzone, L.; Docea, A.O.; Lazopoulos, G.; Kalbakis, K.; Tsatsakis, A. Role of DNA mismatch repair genes in lung and head and neck cancer (Review). World Acad. Sci. J. 2019, 1, 184–191. [Google Scholar] [CrossRef]
- André, T.; Shiu, K.K.; Kim, T.W.; Vittrup, B.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in microsatellite-instability–high advanced colorectal cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non–small cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüs, M.; Maziéres, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus chemotherapy for squamous non-small cell lung cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Garon, E.B.; Rizvi, N.A.; Hui, R.; Leighl, N.; Balmanoukian, A.S.; Eder, J.P.; Patnaik, A.; Aggarwal, C.; Gubens, M.; Horn, L.; et al. Pembrolizumab for the treatment of non–small-cell lung cancer. N. Engl. J. Med. 2015, 372, 2018–2028. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.X.; Qu, C.H.; Gao, Y.H.; Ding, P.R.; Yun, H.P.; Xie, D.; Cai, M.-Y. The degree of microsatellite instability predicts response to PD-1 blockade immunotherapy in mismatch repair-deficient/microsatellite instability-high colorectal cancers. Exp. Hematol. Oncol. 2021, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Raab, S.S. The cost-effectiveness of immunohistochemistry. Arch. Pathol. Lab. Med. 2000, 124, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Johnson, D.B. Immune-related adverse events and anti-tumour efficacy of immune checkpoint inhibitors. J. Immunother. Cancer. 2019, 7, 306. [Google Scholar] [CrossRef] [PubMed]
- Osipov, A.; Lim, S.J.; Popovic, A.; Azad, N.S.; Laheru, D.A.; Zheng, L.; Jaffee, E.M.; Wang, H.; Yarchoan, M. Tumor mutational burden, toxicity, and response of immune checkpoint inhibitors targeting PD(L)1, CTLA-4, and combination: A meta-regression analysis. Clin. Cancer Res. 2020, 26, 4842–4851. [Google Scholar] [CrossRef] [PubMed]
- Weinmann, S.C.; Pisetsky, D.S. Mechanisms of immune-related adverse events during the treatment of cancer with immune checkpoint inhibitors. Rheumatology 2019, 58 (Suppl. 7), viii59–vii67. [Google Scholar] [CrossRef] [Green Version]
- Sehgal, R.; Sheahan, K.; O’Connell, P.R.; Hanly, A.M.; Martin, S.T.; Winter, D.C. Lynch syndrome: An updated review. Genes 2014, 5, 497–507. [Google Scholar] [CrossRef] [Green Version]
- Warren, G.W.; Cummings, K.M. Tobacco and lung cancer: Risks, trends, and outcomes in patients with cancer. Am. Soc. Clin. Oncol. Educ. Book 2013, 33, 359–364. [Google Scholar] [CrossRef]
- Griffin, R.; Ramirez, R.A. Molecular targets in non–small cell lung cancer. Oschsner J. 2017, 17, 388–392. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Sample | Overall, 73 (100%) | MMR Present, 67 (91.8%) | MMR Deficiency, 6 (8.2%) |
|---|---|---|---|
| Age | 68 (44–84) | 68 (44–84) | 67 (54–79) |
| Sex (M/W) | 59/14 (80.8/19.2%) | 53/14 (79.1/20.9%) | 6/0 (100/0%) |
| Subtype | |||
| 36 (49.3%) | 32 (47.8%) | 4 (66.7%) |
| 34 (46.6%) | 32 (47.8%) | 2 (33.3%) | |
| 3 (4.1%) | 3 (4.5%) | 0 (0%) | |
| PD-L1 | |||
| 27 (37%) | 25 (37.3%) | 3 (50%) |
| 46 (63%) | 42 (62.7%) | 3 (50%) | |
| Driver mutations | |||
| 0 (0%) | 0 (0%) | 0 (0%) |
| Survival (months) | |||
| 13 (95% CI 8.2–17.8) | 12 (95% CI 4–20) | 14 (95% CI 4.5−23.5) |
| 5 (95% CI 3.8–6.2) | 4 (95% CI 3–5) | 8 (95% CI 2–14) | |
| Response | |||
| 40 (54.8%) | 39 (58.2%) | 1 (16.7%) |
| 16 (21.9%) | 12 (17.9%) | 4 (66.7%) | |
| 13 (17.8%) | 12 (17.9%) | 1 (16.7%) | |
| 4 (5.4%) | 4 (6%) | 0 (0%) | |
| Toxicity | |||
| 47 (64.4%) | 45 (67.2%) | 2 (33.3%) |
| 12 (16.4%) | 11 (16.4%) | 1 (16.7%) | |
| 4 (5.8%) | 2 (3%) | 2 (33.3%) | |
| 2 (2.7%) | 1 (1.5%) | 1 (16.7%) | |
| 4 (5.8%) | 3 (4.5%) | 1 (16.7%) | |
| 4 (5.8%) | 2 (3%) | 2 (33.3%) | |
| 7 (9.6%) | 5 (7.5%) | 2 (33.3%) | |
| 1 (1.4%) | 1 (1.5%) | 0 (0%) | |
| 1 (1.4%) | 1 (1.5%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olivares-Hernández, A.; del Barco Morillo, E.; Parra Pérez, C.; Miramontes-González, J.P.; Figuero-Pérez, L.; Martín-Gómez, T.; Escala-Cornejo, R.; Bellido Hernández, L.; González Sarmiento, R.; Cruz-Hernández, J.J.; et al. Influence of DNA Mismatch Repair (MMR) System in Survival and Response to Immune Checkpoint Inhibitors (ICIs) in Non-Small Cell Lung Cancer (NSCLC): Retrospective Analysis. Biomedicines 2022, 10, 360. https://doi.org/10.3390/biomedicines10020360
Olivares-Hernández A, del Barco Morillo E, Parra Pérez C, Miramontes-González JP, Figuero-Pérez L, Martín-Gómez T, Escala-Cornejo R, Bellido Hernández L, González Sarmiento R, Cruz-Hernández JJ, et al. Influence of DNA Mismatch Repair (MMR) System in Survival and Response to Immune Checkpoint Inhibitors (ICIs) in Non-Small Cell Lung Cancer (NSCLC): Retrospective Analysis. Biomedicines. 2022; 10(2):360. https://doi.org/10.3390/biomedicines10020360
Chicago/Turabian StyleOlivares-Hernández, Alejandro, Edel del Barco Morillo, Carmen Parra Pérez, José Pablo Miramontes-González, Luis Figuero-Pérez, Teresa Martín-Gómez, Roberto Escala-Cornejo, Lorena Bellido Hernández, Rogelio González Sarmiento, Juan Jesús Cruz-Hernández, and et al. 2022. "Influence of DNA Mismatch Repair (MMR) System in Survival and Response to Immune Checkpoint Inhibitors (ICIs) in Non-Small Cell Lung Cancer (NSCLC): Retrospective Analysis" Biomedicines 10, no. 2: 360. https://doi.org/10.3390/biomedicines10020360