
Diagnostic Accuracy of Bone Scintigraphy for the Histopathological Diagnosis of Cardiac Transthyretin Amyloidosis—A Retrospective Austrian Multicenter Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. Bone Scintigraphy and FLC Assessment
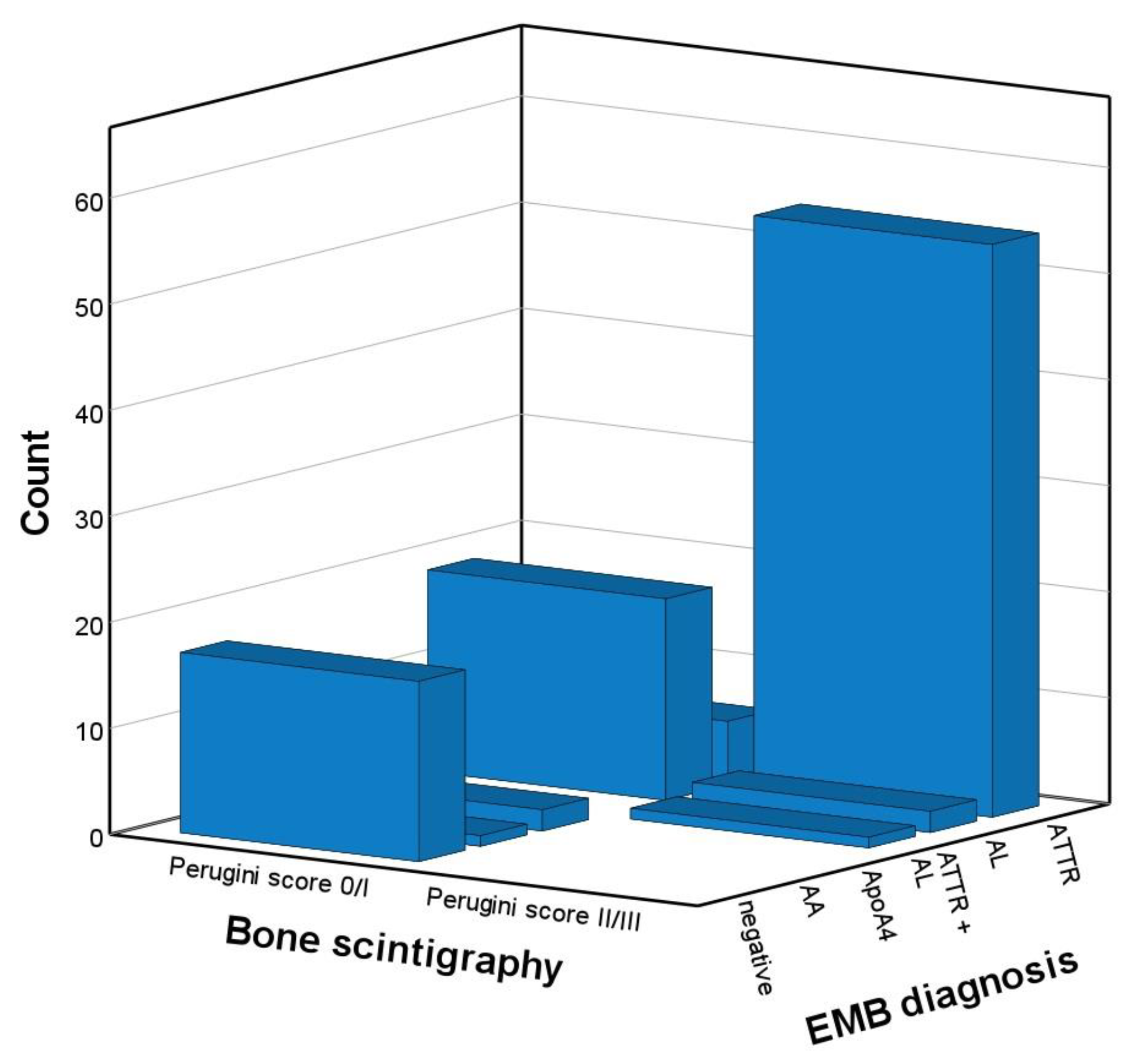
3.3. Diagnostic Accuracy Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ablasser, K.; Verheyen, N.; Glantschnig, T.; Agnetti, G.; Rainer, P.P. Unfolding Cardiac Amyloidosis -From Pathophysiology to Cure. Curr. Med. Chem. 2019, 26, 2865–2878. [Google Scholar] [CrossRef] [PubMed]
- Kocher, F.; Kaser, A.; Escher, F.; Doerler, J.; Zaruba, M.M.; Messner, M.; Mussner-Seeber, C.; Mayr, A.; Ulmer, H.; Schneiderbauer-Porod, S.; et al. Heart failure from ATTRwt amyloid cardiomyopathy is associated with poor prognosis. ESC Heart Fail. 2020, 7, 3919–3928. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Palladini, G.; Minnema, M.C.; Wechalekar, A.D.; Jaccard, A.; Lee, H.C.; Sanchorawala, V.; Gibbs, S.; Mollee, P.; Venner, C.P.; et al. Daratumumab-Based Treatment for Immunoglobulin Light-Chain Amyloidosis. N. Engl. J. Med. 2021, 385, 46–58. [Google Scholar] [CrossRef]
- Maurer, M.S.; Schwartz, J.H.; Gundapaneni, B.; Elliott, P.M.; Merlini, G.; Waddington-Cruz, M.; Kristen, A.V.; Grogan, M.; Witteles, R.; Damy, T.; et al. Tafamidis Treatment for Patients with Transthyretin Amyloid Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Grogan, M.; Dispenzieri, A.; Gertz, M.A. Light-chain cardiac amyloidosis: Strategies to promote early diagnosis and cardiac response. Heart 2017, 103, 1065–1072. [Google Scholar] [CrossRef] [Green Version]
- Gertz, M.A. Immunoglobulin light chain amyloidosis: 2022 update on diagnosis, prognosis, and treatment. Am. J. Hematol. 2022, 97, 818–829. [Google Scholar] [CrossRef]
- Gillmore, J.D.; Maurer, M.S.; Falk, R.H.; Merlini, G.; Damy, T.; Dispenzieri, A.; Wechalekar, A.D.; Berk, J.L.; Quarta, C.C.; Grogan, M.; et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation 2016, 133, 2404–2412. [Google Scholar] [CrossRef]
- Authors/Task Force, M.; McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Perugini, E.; Guidalotti, P.L.; Salvi, F.; Cooke, R.M.; Pettinato, C.; Riva, L.; Leone, O.; Farsad, M.; Ciliberti, P.; Bacchi-Reggiani, L.; et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J. Am. Coll. Cardiol. 2005, 46, 1076–1084. [Google Scholar] [CrossRef] [Green Version]
- Molina-Andujar, A.; Robles, P.; Cibeira, M.T.; Montagud-Marrahi, E.; Guillen, E.; Xipell, M.; Blasco, M.; Poch, E.; Rosinol, L.; Blade, J.; et al. The renal range of the kappa/lambda sFLC ratio: Best strategy to evaluate multiple myeloma in patients with chronic kidney disease. BMC Nephrol. 2020, 21, 111. [Google Scholar] [CrossRef]
- Hutt, D.F.; Fontana, M.; Burniston, M.; Quigley, A.M.; Petrie, A.; Ross, J.C.; Page, J.; Martinez-Naharro, A.; Wechalekar, A.D.; Lachmann, H.J.; et al. Prognostic utility of the Perugini grading of 99mTc-DPD scintigraphy in transthyretin (ATTR) amyloidosis and its relationship with skeletal muscle and soft tissue amyloid. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1344–1350. [Google Scholar] [CrossRef] [PubMed]
- Musumeci, M.B.; Cappelli, F.; Russo, D.; Tini, G.; Canepa, M.; Milandri, A.; Bonfiglioli, R.; Di Bella, G.; My, F.; Luigetti, M.; et al. Low Sensitivity of Bone Scintigraphy in Detecting Phe64Leu Mutation-Related Transthyretin Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Nativi-Nicolau, J.; Siu, A.; Dispenzieri, A.; Maurer, M.S.; Rapezzi, C.; Kristen, A.V.; Garcia-Pavia, P.; LoRusso, S.; Waddington-Cruz, M.; Lairez, O.; et al. Temporal Trends of Wild-Type Transthyretin Amyloid Cardiomyopathy in the Transthyretin Amyloidosis Outcomes Survey. JACC Cardio Oncol. 2021, 3, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Ruan, D.; Sun, L. Diagnostic efficacy of bone scintigraphy in transthyretin cardiac amyloidosis: An updated systematic review and Bayesian bivariate meta-analysis. Clin. Transl. Imaging 2022, 10, 85–98. [Google Scholar] [CrossRef]
- Hanna, M.; Ruberg, F.L.; Maurer, M.S.; Dispenzieri, A.; Dorbala, S.; Falk, R.H.; Hoffman, J.; Jaber, W.; Soman, P.; Witteles, R.M.; et al. Cardiac Scintigraphy With Technetium-99m-Labeled Bone-Seeking Tracers for Suspected Amyloidosis: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2020, 75, 2851–2862. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, C.; Mascherbauer, K.; Calabretta, R.; Koschutnik, M.; Dona, C.; Dannenberg, V.; Hofer, F.; Halavina, K.; Kammerlander, A.; Traub-Weidinger, T.; et al. Prevalence and outcomes of cardiac amyloidosis in all-comer referrals for bone scintigraphy. J. Nucl. Med. 2022, 42, ehab724-0280. [Google Scholar] [CrossRef] [PubMed]
- Zach, D.; Ablasser, K.; Kolesnik, E.; Hoeller, V.; Fruhwald, F.; Pruller, F.; Reiter, C.; Beham-Schmid, C.; Lipp, R.; Rainer, P.P.; et al. Advanced isolated light chain amyloid cardiomyopathy with negative immunofixation and normal free light chain ratio. ESC Heart Fail. 2021, 8, 3397–3402. [Google Scholar] [CrossRef]
- Palladini, G.; Russo, P.; Bosoni, T.; Verga, L.; Sarais, G.; Lavatelli, F.; Nuvolone, M.; Obici, L.; Casarini, S.; Donadei, S.; et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine. Clin. Chem. 2009, 55, 499–504. [Google Scholar] [CrossRef] [Green Version]
- Milani, P.; Valentini, V.; Ferraro, G.; Basset, M.; Russo, F.; Foli, A.; Palladini, G.; Merlini, G. A patient with AL amyloidosis with negative free light chain results. Clin. Chem. Lab. Med. 2016, 54, 1035–1037. [Google Scholar] [CrossRef]
- Wakfie-Corieh, C.G.; Ramos Lopez, N.; Saiz-Pardo Sanz, M.; Perez Castejon, M.J.; Vilacosta, I. Not All Heart Uptakes on 99mTc-DPD Scintigraphy Are Amyloidosis: Chloroquine-Induced Cardiomyopathy. Clin. Nucl. Med. 2021, 46, e188–e189. [Google Scholar] [CrossRef]
- Chang, I.C.Y.; Bois, J.P.; Bois, M.C.; Maleszewski, J.J.; Johnson, G.B.; Grogan, M. Hydroxychloroquine-Mediated Cardiotoxicity With a False-Positive (99m)Technetium-Labeled Pyrophosphate Scan for Transthyretin-Related Cardiac Amyloidosis. Circ. Cardiovasc. Imaging 2018, 11, e007059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makivic, N.; Stollberger, C.; Nakuz, T.; Schneider, B.; Schmid, C.; Hasun, M.; Weidinger, F. Reversible myocardial oedema due to acute myocardial infarction as differential diagnosis of cardiac transthyretin amyloidosis. ESC Heart Fail. 2020, 7, 1987–1991. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, C.; Alfarano, M.; Maestrini, V.; Galea, N.; De Vincentis, G.; Verardo, R.; Fedele, F.; Frustaci, A. False-positive bone scintigraphy denoting transthyretin amyloid in elderly hypertrophic cardiomyopathy. ESC Heart Fail. 2021, 8, 3387–3391. [Google Scholar] [CrossRef] [PubMed]
- Di Bella, G.; Pizzino, F.; Minutoli, F.; Zito, C.; Donato, R.; Dattilo, G.; Oreto, G.; Baldari, S.; Vita, G.; Khandheria, B.K.; et al. The mosaic of the cardiac amyloidosis diagnosis: Role of imaging in subtypes and stages of the disease. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1307–1315. [Google Scholar] [CrossRef] [Green Version]
- Mascia, G.; Arbelo, E.; Porto, I.; Brugada, R.; Brugada, J. The arrhythmogenic right ventricular cardiomyopathy in comparison to the athletic heart. J. Cardiovasc. Electrophysiol. 2020, 31, 1836–1843. [Google Scholar] [CrossRef]
- Mascia, G.; Crotti, L.; Groppelli, A.; Canepa, M.; Merlo, A.C.; Benenati, S.; Di Donna, P.; Della Bona, R.; Soranna, D.; Zambon, A.; et al. Syncope in hypertrophic cardiomyopathy (part I): An updated systematic review and meta-analysis. Int. J. Cardiol. 2022, 357, 88–94. [Google Scholar] [CrossRef]
- Milandri, A.; Farioli, A.; Gagliardi, C.; Longhi, S.; Salvi, F.; Curti, S.; Foffi, S.; Caponetti, A.G.; Lorenzini, M.; Ferlini, A.; et al. Carpal tunnel syndrome in cardiac amyloidosis: Implications for early diagnosis and prognostic role across the spectrum of aetiologies. Eur. J. Heart Fail. 2020, 22, 507–515. [Google Scholar] [CrossRef]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and treatment of cardiac amyloidosis: A position statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2021, 42, 1554–1568. [Google Scholar] [CrossRef]
- Baccouche, H.; Maunz, M.; Beck, T.; Gaa, E.; Banzhaf, M.; Knayer, U.; Fogarassy, P.; Beyer, M. Differentiating cardiac amyloidosis and hypertrophic cardiomyopathy by use of three-dimensional speckle tracking echocardiography. Echocardiography 2012, 29, 668–677. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Mirea, O.; Duchenne, J.; Van Cleemput, J.; Delforge, M.; Bogaert, J.; Kuznetsova, T.; Voigt, J.U. Echo Parameters for Differential Diagnosis in Cardiac Amyloidosis: A Head-to-Head Comparison of Deformation and Nondeformation Parameters. Circ. Cardiovasc. Imaging 2017, 10, e005588. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| All (N = 102) | Perugini Score | ||
|---|---|---|---|
| 0/1 (N = 45) | 2/3 (N = 57) | ||
| Age, years | 75 (68–78) | 70 (60–76) | 77 (73–80) ** |
| Women, n (%) | 22 (22%) | 16 (36%) | 6 (11%) * |
| NT-proBNP, pg/mL | 2652 (1580–5167) | 2966 (1322–5205) | 2578 (1624–5183) |
| eGFR MDRD, mL/min/1.73 m² | 60 ± 19 | 58 ± 18 | 61 ± 19 |
| Bone scintigraphy | |||
| SPECT | 57 (56%) | 29 (64%) | 28 (49%) |
| Tracer, n (%) | |||
| DPD | 87 (85%) | 35 (78%) | 52 (91%) |
| HDP | 6 (6%) | 3 (7%) | 3 (5%) |
| PYP | 9 (9%) | 7 (16%) | 2 (4%) |
| Perugini score, n (%) | |||
| 0 | 31 (30%) | 31 (69%) | 0 ** |
| 1 | 14 (14%) | 14 (31%) | 0 |
| 2 | 16 (16%) | 0 | 16 (28%) |
| 3 | 41 (40%) | 0 | 41 (72%) |
| FLC assessment | |||
| Monoclonal protein, n (%) | 62 (59%) | 31 (69%) | 31 (54%) |
| Monoclonal band | 48 (47%) | 29 (64%) | 19 (33%) * |
| serum | 46 (45%) | 28 (64%) | 18 (33%) * |
| urine | 26 (26%) | 14 (33%) | 12 (23%) |
| Abnormal FLC ratio | 51 (50%) | 26 (58%) | 25 (44%) |
| Serum FLC ratio | 1.50 (0.78–2.02) | 1.36 (0.185–2.37) | 1.64 (1.00–1.98) |
| EMB-derived diagnosis, n (%) | |||
| ATTR# | 60 (59%) | 6 (13%) | 54 (95%) |
| AL | 21 (21%) | 19 (42%) | 2 (4%) |
| ATTR + AL | 1 (1%) | 0 | 1 (2%) |
| ApoA4 | 2 (2%) | 2 (4%) | 0 |
| AA | 1 (1%) | 1 (2%) | 0 |
| negative | 17 (17%) | 17 (38%) | 0 |
| Perugini Score | ||||||
|---|---|---|---|---|---|---|
| 0 N = 31 | 1 N = 14 | 2 N = 16 | 3 N = 41 | |||
| EMB result | ATTR | 1 | 5 | 14 | 40 | Sensitivity 90% Specificity 95% PPV 96% NPV 87% |
| ATTR + AL | 0 | 0 | 1 * | 0 | ||
| AL | 14 | 5 | 1 | 1 | ||
| ApoA4 | 2 | 0 | 0 | 0 | ||
| AA | 1 | 0 | 0 | 0 | ||
| Negative | 13 | 4 | 0 | 0 | ||
| Perugini Score | ||||||
|---|---|---|---|---|---|---|
| 0 N = 9 | 1 N = 5 | 2 N = 7 | 3 N = 19 | |||
| EMB result | ATTR | 0 | 3 | 7 | 19 | Sensitivity 90% Specificity 100% PPV 100% NPV 79% |
| AL | 0 | 1 | 0 | 0 | ||
| ApoA4 | 1 | 0 | 0 | 0 | ||
| AA | 1 | 0 | 0 | 0 | ||
| Negative | 7 | 1 | 0 | 0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verheyen, N.; Ungericht, M.; Paar, L.; Danninger, K.; Schneiderbauer-Porod, S.; Duca, F.; Cherouny, B.; Hoeller, V.; Ablasser, K.; Zach, D.; et al. Diagnostic Accuracy of Bone Scintigraphy for the Histopathological Diagnosis of Cardiac Transthyretin Amyloidosis—A Retrospective Austrian Multicenter Study. Biomedicines 2022, 10, 3052. https://doi.org/10.3390/biomedicines10123052
Verheyen N, Ungericht M, Paar L, Danninger K, Schneiderbauer-Porod S, Duca F, Cherouny B, Hoeller V, Ablasser K, Zach D, et al. Diagnostic Accuracy of Bone Scintigraphy for the Histopathological Diagnosis of Cardiac Transthyretin Amyloidosis—A Retrospective Austrian Multicenter Study. Biomedicines. 2022; 10(12):3052. https://doi.org/10.3390/biomedicines10123052
Chicago/Turabian StyleVerheyen, Nicolas, Maria Ungericht, Lisa Paar, Kathrin Danninger, Stefanie Schneiderbauer-Porod, Franz Duca, Bernhard Cherouny, Viktoria Hoeller, Klemens Ablasser, David Zach, and et al. 2022. "Diagnostic Accuracy of Bone Scintigraphy for the Histopathological Diagnosis of Cardiac Transthyretin Amyloidosis—A Retrospective Austrian Multicenter Study" Biomedicines 10, no. 12: 3052. https://doi.org/10.3390/biomedicines10123052