
Sarcoidosis and COVID-19: At the Cross-Road between Immunopathology and Clinical Manifestation

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Immunopathology of Sarcoidosis and COVID-19, Shared Mechanisms
2.1. Adaptive and Innate Immunity in COVID-19 and Sarcoidosis
2.2. Fibrosis
3. Clinical Features of Sarcoidosis and COVID-19
3.1. Clinical Manifestation of Sarcoidosis
3.2. Clinical Manifestations of COVID-19
3.3. Clinical Features of Sarcoid Patients Infected by SARS-CoV2
4. Diagnosis of Sarcoidosis and COVID-19, the Role of Imaging
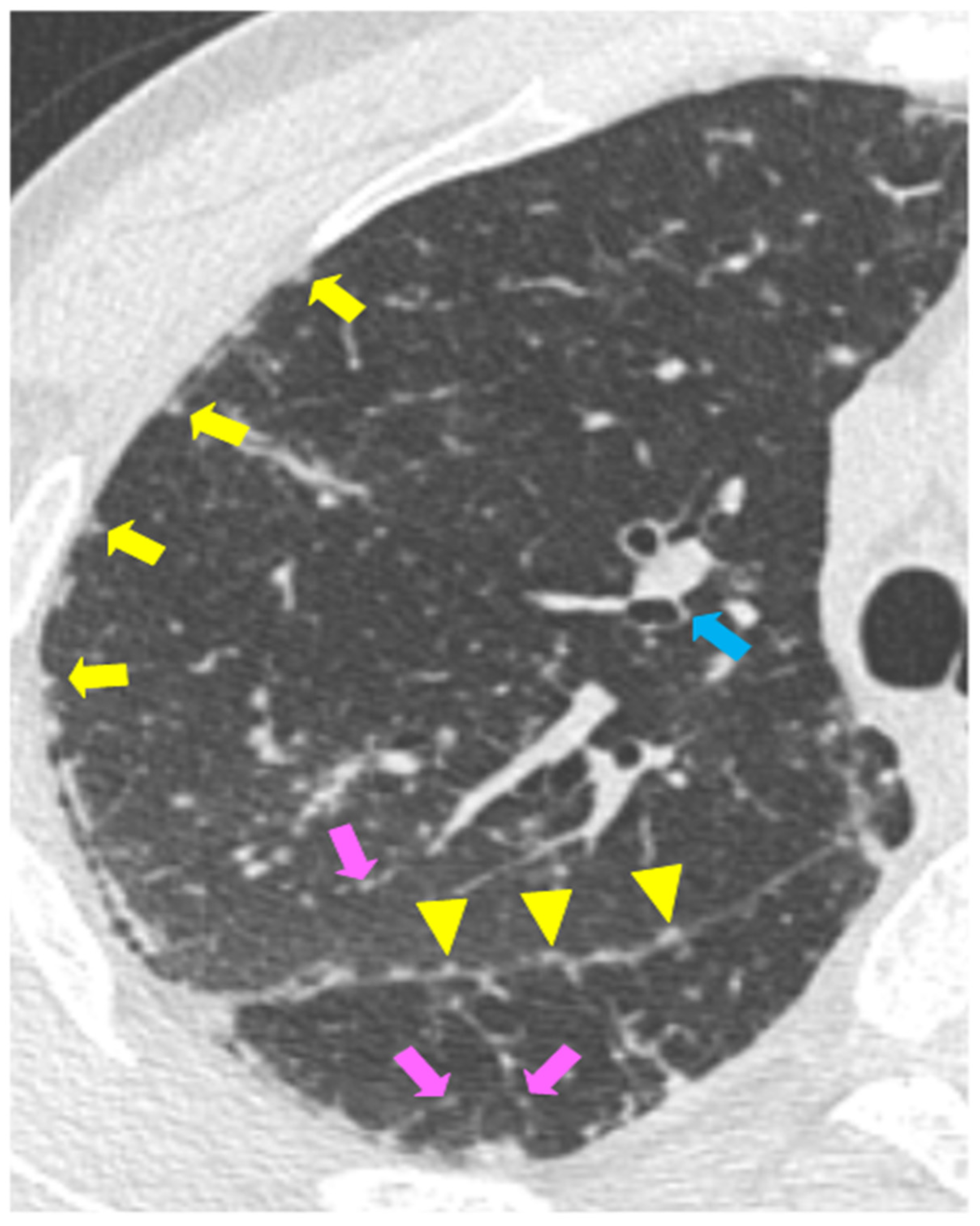
4.1. High Resolution Computed Tomography Findings (HRCT) of Pulmonary Sarcoidosis
- Obstructive physiology: characterized by bronchiectasis featuring air trapping or central bronchial distortion.
- Restrictive physiology with low DLCO: characterized by subpleural honeycombing.
- Mild effect on respiratory function: characterized by diffuse linear fibrotic pattern, with typical distribution more from hila to all directions [82].
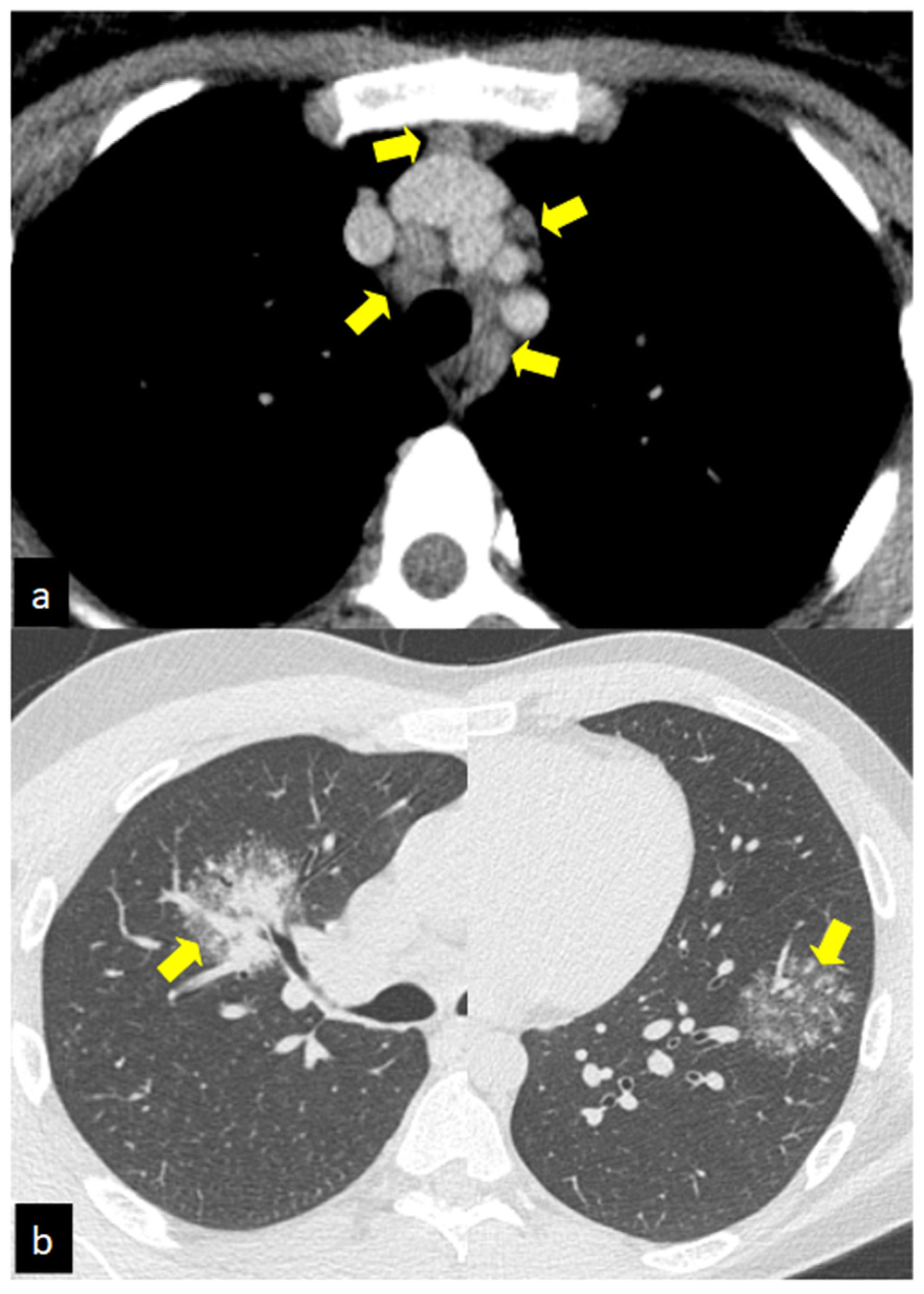
4.2. HRCT Findings of Lung Involvement from COVID-19
4.3. Differences and Similarities between HRCT Findings of Pulmonary Sarcoidosis and COVID-19
5. Treatment Approaches, Algorithms for Suppression of Sarcoidosis during the COVID-19 Pandemic
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Renda, G.; Ricci, F.; Spinoni, E.G.; Grisafi, L.; D’Ardes, D.; Mennuni, M.; Tana, C.; Rognoni, A.; Bellan, M.; Sainaghi, P.P.; et al. Predictors of Mortality and Cardiovascular Outcome at 6 Months after Hospitalization for COVID-19. J. Clin. Med. 2022, 11, 729. [Google Scholar] [CrossRef] [PubMed]
- Polverino, F.; Stern, D.A.; Ruocco, G.; Balestro, E.; Bassetti, M.; Candelli, M.; Cirillo, B.; Contoli, M.; Corsico, A.; D’Amico, F.; et al. Comorbidities, Cardiovascular Therapies, and COVID-19 Mortality: A Nationwide, Italian Observational Study (ItaliCO). Front. Cardiovasc. Med. 2020, 7, 585866. [Google Scholar] [CrossRef] [PubMed]
- Bajema, K.L.; Dahl, R.M.; Prill, M.M.; Meites, E.; Rodriguez-Barradas, M.C.; Marconi, V.C.; Beenhouwer, D.O.; Brown, S.T.; Holodniy, M.; Lucero-Obusan, C.; et al. Effectiveness of COVID-19 mRNA Vaccines Against COVID-19-Associated Hospitalization—Five Veterans Affairs Medical Centers, United States, 1 February–6 August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1294–1299. [Google Scholar] [CrossRef]
- Tana, C.; Drent, M.; Nunes, H.; Kouranos, V.; Cinetto, F.; Jessurun, N.T.; Spagnolo, P. Comorbidities of sarcoidosis. Ann. Med. 2022, 54, 1014–1035. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Schiavone, C. The Chameleon Behavior of Sarcoidosis. J. Clin. Med. 2021, 10, 2780. [Google Scholar] [CrossRef] [PubMed]
- Chokoeva, A.A.; Tchernev, G.; Tana, M.; Tana, C. Exclusion criteria for sarcoidosis: A novel approach for an ancient disease? Eur. J. Intern. Med. 2014, 25, e120. [Google Scholar] [CrossRef] [PubMed]
- Tchernev, G.; Chokoeva, A.A.; Tana, M.; Tana, C. Transcriptional blood signatures of sarcoidosis, sarcoid-like reactions and tuberculosis and their diagnostic implications. Sarcoidosis Vasc. Diffus. Lung Dis. 2016, 33, 5030. [Google Scholar]
- Esteves, T.; Aparicio, G.; Garcia-Patos, V. Is there any association between Sarcoidosis and infectious agents?: A systematic review and meta-analysis. BMC Pulm. Med. 2016, 16, 165. [Google Scholar] [CrossRef] [Green Version]
- Tana, C.; Giamberardino, M.A.; Di Gioacchino, M.; Mezzetti, A.; Schiavone, C. Immunopathogenesis of sarcoidosis and risk of malignancy: A lost truth? Int. J. Immunopathol. Pharmacol. 2013, 26, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Capaccione, K.M.; McGroder, C.; Garcia, C.K.; Fedyna, S.; Saqi, A.; Salvatore, M.M. COVID-19-induced pulmonary sarcoid: A case report and review of the literature. Clin. Imaging 2022, 83, 152–158. [Google Scholar] [CrossRef]
- Behbahani, S.; Baltz, J.O.; Droms, R.; Deng, A.C.; Amano, S.U.; Levin, N.A.; O’Brien, M.C.; Wiss, K. Sarcoid-like reaction in a patient recovering from coronavirus disease 19 pneumonia. JAAD Case Rep. 2020, 6, 915–917. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, A.P.; Buyukbabani, N.; Mese, S.; Pehlivan, G.; Okomuş, N.G.; Ağaçfidan, A.; Özkaya, E. COVID-19-triggered sarcoid granulomas mimicking scar sarcoidosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e477–e480. [Google Scholar]
- Stukalov, A.; Girault, V.; Grass, V.; Karayel, O.; Bergant, V.; Urban, C.; Haas, D.A.; Huang, Y.; Oubraham, L.; Wang, A.; et al. Multilevel proteomics reveals host perturbations by SARS-CoV-2 and SARS-CoV. Nature 2021, 594, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Stravalaci, M.; Pagani, I.; Paraboschi, E.M.; Pedotti, M.; Doni, A.; Scavello, F.; Mapelli, S.N.; Sironi, M.; Perucchini, C.; Varani, L.; et al. Recognition and inhibition of SARS-CoV-2 by humoral innate immunity pattern recognition molecules. Nat. Immunol. 2022, 23, 275–286. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.S.; Atif, S.M.; Falta, M.T.; Fontenot, A.P. Innate and Adaptive Immunity in Noninfectious Granulomatous Lung Disease. J. Immunol. 2022, 208, 1835–1843. [Google Scholar] [CrossRef]
- Vagts, C.; Ascoli, C.; Fraidenburg, D.R.; Baughman, R.P.; Huang, Y.; Edafetanure-Ibeh, R.; Ahmed, S.; Levin, B.; Lu, Y.; Perkins, D.L.; et al. Unsupervised Clustering Reveals Sarcoidosis Phenotypes Marked by a Reduction in Lymphocytes Relate to Increased Inflammatory Activity on 18FDG-PET/CT. Front. Med. 2021, 8, 595077. [Google Scholar] [CrossRef]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Wang, Y.; Li, J.; Han, H.; Xia, Z.; Liu, F.; Wu, K.; Yang, L.; Liu, X.; Zhu, C. Decreased T cell populations contribute to the increased severity of COVID-19. Clin. Chim. Acta 2020, 508, 110–114. [Google Scholar] [CrossRef]
- Maeda, K.; Baba, Y.; Nagai, Y.; Miyazaki, K.; Malykhin, A.; Nakamura, K.; Kincade, P.W.; Sakaguchi, N.; Coggeshall, K.M. IL-6 blocks a discrete early step in lymphopoiesis. Blood 2005, 106, 879–885. [Google Scholar] [CrossRef] [Green Version]
- Tortorici, M.A.; Walls, A.C.; Lang, Y.; Wang, C.; Li, Z.; Koerhuis, D.; Boons, G.J.; Bosch, B.J.; Rey, F.A.; de Groot, R.J.; et al. Structural basis for human coronavirus attachment to sialic acid receptors. Nat. Struct. Mol. Biol. 2019, 26, 481–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lieberman, J. The specificity and nature of serum-angiotensin-converting enzyme (serum ace) elevations in sarcoidosis. Ann. N. Y. Acad. Sci. 1976, 278, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Silverstein, E.; Friedland, J.; Lyons, H.A.; Gourin, A. Markedly elevated angiotensin converting enzyme in lymph nodes containing non-necrotizing granulomas in sarcoidosis. Proc. Natl. Acad. Sci. USA 1976, 73, 2137–2141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouser, E.D.; Maier, L.A.; Wilson, K.C.; Bonham, C.A.; Morgenthau, A.S.; Patterson, K.C.; Abston, E.; Bernstein, R.C.; Blankstein, R.; Chen, E.S.; et al. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2020, 201, e26–e51. [Google Scholar] [CrossRef] [PubMed]
- Hemnes, A.R.; Rathinasabapathy, A.; Austin, E.A.; Brittain, E.L.; Carrier, E.J.; Chen, X.; Fessel, J.P.; Fike, C.D.; Fong, P.; Fortune, N.; et al. A potential therapeutic role for angiotensin-converting enzyme 2 in human pulmonary arterial hypertension. Eur. Respir. J. 2018, 51, 1702638. [Google Scholar] [CrossRef]
- Fung, T.S.; Liu, D.X. Human Coronavirus: Host-Pathogen Interaction. Annu. Rev. Microbiol. 2019, 73, 529–557. [Google Scholar] [CrossRef] [Green Version]
- Xiao, R.; Zhao, H.-C.; Yan, T.-T.; Zhang, Q.; Huang, Y.S. Angiotensin II and hypoxia induce autophagy in cardiomyocytes via activating specific protein kinase C subtypes. Cardiovasc. Diagn. Ther. 2021, 11, 744–759. [Google Scholar] [CrossRef]
- Ibrahim, I.M.; Abdelmalek, D.H.; Elshahat, M.E.; Elfiky, A.A. COVID-19 spike-host cell receptor GRP78 binding site prediction. J. Infect. 2020, 80, 554–562. [Google Scholar] [CrossRef]
- Linke, M.; Pham, H.T.; Katholnig, K.; Schnöller, T.; Miller, A.; Demel, F.; Schütz, B.; Rosner, M.; Kovacic, B.; Sukhbaatar, N.; et al. Chronic signaling via the metabolic checkpoint kinase mTORC1 induces macrophage granuloma formation and marks sarcoidosis progression. Nat. Immunol. 2017, 18, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Lockstone, H.E.; Sanderson, S.; Kulakova, N.; Baban, D.; Leonard, A.; Kok, W.L.; McGowan, S.; McMichael, A.J.; Ho, L.P. Gene set analysis of lung samples provides insight into pathogenesis of progressive, fibrotic pulmonary sarcoidosis. Am. J. Respir. Crit. Care Med. 2010, 181, 1367–1375. [Google Scholar] [CrossRef]
- Cinetto, F.; Scarpa, R.; Dell’Edera, A.; Jones, M.G. Immunology of sarcoidosis: Old companions, new relationships. Curr. Opin. Pulm. Med. 2020, 26, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Brunetta, E.; Folci, M.; Bottazzi, B.; De Santis, M.; Gritti, G.; Protti, A.; Mapelli, S.N.; Bonovas, S.; Piovani, D.; Leone, R.; et al. Macrophage expression and prognostic significance of the long pentraxin PTX3 in COVID-19. Nat. Immunol. 2021, 22, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Dubaniewicz, A.; Typiak, M.; Wybieralska, M.; Szadurska, M.; Nowakowski, S.; Staniewicz-Panasik, A.; Rogoza, K.; Sternau, A.; Deeg, P.; Trzonkowski, P. Changed phagocytic activity and pattern of Fcgamma and complement receptors on blood monocytes in sarcoidosis. Hum. Immunol. 2012, 73, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Gonçales, R.A.; Bastos, H.N.; Duarte-Oliveira, C.; Antunes, D.; Sokhatska, O.; Jacob, M.; Rolo, R.; Campos, C.F.; Sasaki, S.D.; Donato, A.; et al. PTX3 Inhibits Complement-Driven Macrophage Activation to Restrain Granuloma Formation in Sarcoidosis. Am. J. Resp. Crit. Care Med. 2022, in press. [Google Scholar] [CrossRef]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Annunziato, F.; Cosmi, L. Hallmarks of immune response in COVID-19: Exploring dysregulation and exhaustion. Semin. Immunol. 2021, 55, 101508. [Google Scholar] [CrossRef]
- Webb, B.J.; Peltan, I.D.; Jensen, P.; Hoda, D.; Hunter, B.; Silver, A.; Starr, N.; Buckel, W.; Grisel, N.; Hummel, E.; et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: A cohort study. Lancet Rheumatol. 2020, 2, e754–e763. [Google Scholar] [CrossRef]
- Sims, J.T.; Krishnan, V.; Chang, C.Y.; Engle, S.M.; Casalini, G.; Rodgers, G.H.; Bivi, N.; Nickoloff, B.J.; Konrad, R.J.; de Bono, S.; et al. Characterization of the cytokine storm reflects hyperinflammatory endothelial dysfunction in COVID-19. J. Allergy Clin. Immunol. 2021, 147, 107–111. [Google Scholar] [CrossRef]
- Locke, L.W.; Crouser, E.D.; White, P.; Julian, M.W.; Caceres, E.G.; Papp, A.C.; Le, V.T.; Sadee, W.; Schlesinger, L.S. IL-13–regulated Macrophage Polarization during Granuloma Formation in an In Vitro Human Sarcoidosis Model. Am. J. Respir. Cell Mol. Biol. 2019, 60, 84–95. [Google Scholar] [CrossRef]
- Zhou, T.; Casanova, N.; Pouladi, N.; Wang, T.; Lussier, Y.; Knox, K.S.; Garcia, J.G.N. Identification of Jak-STAT signaling involvement in sarcoidosis severity via a novel microRNA-regulated peripheral blood mononuclear cell gene signature. Sci. Rep. 2017, 7, 4237. [Google Scholar] [CrossRef] [Green Version]
- Damsky, W.; Wang, A.; Kim, D.J.; Young, B.D.; Singh, K.; Murphy, M.J.; Daccache, J.; Clark, A.; Ayasun, R.; Ryu, C.; et al. Inhibition of type 1 immunity with tofacitinib is associated with marked improvement in longstanding sarcoidosis. Nat. Commun. 2022, 13, 3140. [Google Scholar] [CrossRef]
- Della-Torre, E.; Lanzillotta, M.; Campochiaro, C.; Cavalli, G.; De Luca, G.; Tomelleri, A.; Boffini, N.; De Lorenzo, R.; Ruggeri, A.; Rovere-Querini, P.; et al. Respiratory Impairment Predicts Response to IL-1 and IL-6 Blockade in COVID-19 Patients with Severe Pneumonia and Hyper-Inflammation. Front. Immunol. 2021, 12, 675678. [Google Scholar] [CrossRef] [PubMed]
- Bertoni, A.; Penco, F.; Mollica, H.; Bocca, P.; Prigione, I.; Corcione, A.; Cangelosi, D.; Schena, F.; Del Zotto, G.; Amaro, A.; et al. Spontaneous NLRP3 inflammasome-driven IL1-beta secretion is induced in severe COVID-19 patients and responds to anakinra treatment. J. Allergy Clin. Immunol. 2022, in press. [Google Scholar] [CrossRef]
- Kalil, A.C.; Patterson, T.F.; Mehta, A.K.; Tomashek, K.M.; Wolfe, C.R.; Ghazaryan, V.; Marconi, V.C.; Ruiz-Palacios, G.M.; Hsieh, L.; Kline, S.; et al. Baricitinib plus Remdesivir for Hospitalized Adults with COVID-19. N. Engl. J. Med. 2021, 384, 795–807. [Google Scholar] [CrossRef]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; de Cassia Pellegrini, R.; et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir. Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Chen, C.-C.; Yang, Y.-P.; Tsai, H.-L.; Thun, T.H. Effects of Tocilizumab on Adults With COVID-19 Pneumonia: A Meta-Analysis. Front. Med. 2022, 9, 838904. [Google Scholar] [CrossRef] [PubMed]
- Kirkil, G.; Lower, E.E.; Baughman, R.P. Predictors of Mortality in Pulmonary Sarcoidosis. Chest 2018, 153, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Celada, L.J.; Kropski, J.A.; Herazo-Maya, J.D.; Luo, W.; Creecy, A.; Abad, A.T.; Chioma, O.S.; Lee, G.; Hassell, N.E.; Shaginurova, G.I.; et al. PD-1 up-regulation on CD4+ T cells promotes pulmonary fibrosis through STAT3-mediated IL-17A and TGF-β1 production. Sci. Transl. Med. 2018, 10, eaar8356. [Google Scholar] [CrossRef] [Green Version]
- Pan, Y.; Guan, H.; Zhou, S.; Wang, Y.; Li, Q.; Zhu, T.; Hu, Q.; Xia, L. Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): A study of 63 patients in Wuhan, China. Eur. Radiol. 2020, 30, 3306–3309. [Google Scholar] [CrossRef] [Green Version]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef] [Green Version]
- Jeny, F.; Bernaudin, J.F.; Valeyre, D.; Kambouchner, M.; Pretolani, M.; Nunes, H.; Planès, C.; Besnard, V. Hypoxia Promotes a Mixed Inflammatory-Fibrotic Macrophages Phenotype in Active Sarcoidosis. Front. Immunol. 2021, 12, 719009. [Google Scholar] [CrossRef]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. ATS/ERS/WASOG statement on sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc. Diffus. Lung Dis. 1999, 16, 149–173. [Google Scholar]
- Tana, C.; Donatiello, I.; Caputo, A.; Tana, M.; Naccarelli, T.; Mantini, C.; Ricci, F.; Ticinesi, A.; Meschi, T.; Cipollone, F.; et al. Clinical Features, Histopathology and Differential Diagnosis of Sarcoidosis. Cells 2021, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Bernardinello, N.; Petrarulo, S.; Balestro, E.; Cocconcelli, E.; Veltkamp, M.; Spagnolo, P. Pulmonary Sarcoidosis: Diagnosis and Differential Diagnosis. Diagnostics 2021, 11, 1558. [Google Scholar] [CrossRef] [PubMed]
- Sève, P.; Pacheco, Y.; Durupt, F.; Jamilloux, Y.; Gerfaud-Valentin, M.; Isaac, S.; Boussel, L.; Calender, A.; Androdias, G.; Valeyre, D.; et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells 2021, 10, 766. [Google Scholar] [CrossRef]
- Drent, M.; Strookappe, B.; Hoitsma, E.; De Vries, J. Consequences of Sarcoidosis. Clin. Chest Med. 2015, 36, 727–737. [Google Scholar] [CrossRef]
- Tavee, J.; Culver, D. Sarcoidosis and Small-fiber Neuropathy. Curr. Pain Headache Rep. 2011, 15, 201–206. [Google Scholar] [CrossRef]
- Hoitsma, E.; Marziniak, M.; Faber, C.G.; Reulen, J.P.; Sommer, C.; De Baets, M.; Drent, M. Small fibre neuropathy in sarcoidosis. Lancet 2002, 359, 2085–2086. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Adil, M.T.; Rahman, R.; Whitelaw, D.; Jain, V.; Al-Taan, O.; Rashid, F.; Munasinghe, A.; Jambulingam, P. SARS-CoV-2 and the pandemic of COVID-19. Postgrad. Med. J. 2021, 97, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.R.; Martin, M.R.; Martin, J.D.; Kuhn, P.; Hicks, J.B. Modeling the Onset of Symptoms of COVID-19. Front. Public Health 2020, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J. Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Abrams, R.M.C.; Simpson, D.M.; Navis, A.; Jette, N.; Zhou, L.; Shin, S.C. Small fiber neuropathy associated with SARS-CoV-2 infection. Muscle Nerve 2022, 65, 440–443. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Gracia-Tello, B.; Robles, A.; Alguacil, A.; Bonet, M.; De-Escalante, B.; Noblejas-Mosso, A.; Gómez-de-la-Torre, R.; Akasbi, M.; Pérez-de-Lis, M.; et al. Characterization and Outcomes of SARS-CoV-2 Infection in Patients with Sarcoidosis. Viruses 2021, 13, 1000. [Google Scholar] [CrossRef]
- Manansala, M.; Ascoli, C.; Alburquerque, A.G.; Perkins, D.; Mirsaedi, M.; Finn, P.; Sweiss, N.J. Case Series: COVID-19 in African American Patients with Sarcoidosis. Front. Med. 2020, 7, 588527. [Google Scholar] [CrossRef]
- Baughman, R.P.; Lower, E.E. COVID-19 infections in sarcoidosis: A prospective single-centre study of 886 sarcoidosis patients. Sarcoidosis Vasc. Diffus. Lung Dis. 2021, 38, e2021029. [Google Scholar]
- Desbois, A.C.; Marques, C.; Lefèvre, L.; Barmo, S.; Lorenzo, C.; Leclercq, M.; Leroux, G.; Comarmond, C.; Chapelon-Abric, C.; Domont, F.; et al. Prevalence and clinical features of COVID-19 in a large cohort of 199 patients with sarcoidosis. Clin. Exp. Rheumatol. 2022, 40, 195–196. [Google Scholar] [CrossRef]
- Hadi, Y.B.; Lakhani, D.A.; Naqvi, S.F.Z.; Singh, S.; Kupec, J.T. Outcomes of SARS-CoV-2 infection in patients with pulmonary sarcoidosis: A multicenter retrospective research network study. Respir. Med. 2021, 187, 106538. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.P.; Lower, E.E.; Buchanan, M.; Rottoli, P.; Drent, M.; Sellares, J.; Terwiel, M.; Elfferich, M.; Francesqui, J.; Barriuso Cabrerizo, M.R.; et al. Risk and outcome of COVID-19 infection in sarcoidosis patients: Results of a self-reporting questionnaire. Sarcoidosis Vasc. Diffus. Lung Dis. 2020, 37, e2020009. [Google Scholar]
- Palones, E.; Pajares, V.; López, L.; Castillo, D.; Torrego, A. Sarcoidosis following SARS-CoV-2 infection: Cause or consequence? Respirol. Case Rep. 2022, 10, e0955. [Google Scholar] [CrossRef] [PubMed]
- Muller, N.L.; Miller, R.R. Ground-glass attenuation, nodules, alveolitis, and sarcoid granulomas. Radiology 1993, 189, 31–32. [Google Scholar] [CrossRef]
- Tana, C.; Ricci, F.; Coppola, M.G.; Mantini, C.; Lauretani, F.; Campanozzi, D.; Renda, G.; Gallina, S.; Lugará, M.; Cipollone, F.; et al. Prognostic Significance of Chest Imaging by LUS and CT in COVID-19 Inpatients: The ECOVID Multicenter Study. Respiration 2021, 101, 122–131. [Google Scholar] [CrossRef]
- Tana, C.; Donatiello, I.; Coppola, M.G.; Ricci, F.; Maccarone, M.T.; Ciarambino, T.; Cipollone, F.; Giamberardino, M.A. CT Findings in Pulmonary and Abdominal Sarcoidosis. Implications for Diagnosis and Classification. J. Clin. Med. 2020, 9, 3028. [Google Scholar] [CrossRef]
- Reich, J.M. Mortality of intrathoracic sarcoidosis in referral vs population-based settings: Influence of stage, ethnicity, and corticosteroid therapy. Chest 2002, 121, 32–39. [Google Scholar] [CrossRef]
- Tana, C.; Mantini, C.; Cipollone, F.; Giamberardino, M.A. Chest Imaging of Patients with Sarcoidosis and SARS-CoV-2 Infection. Current Evidence and Clinical Perspectives. Diagnostics 2021, 11, 183. [Google Scholar] [CrossRef]
- Arar, O.; Boni, F.; Meschi, T.; Tana, C. Pulmonary Sarcoidosis Presenting with Miliary Opacities. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2018, 15, 81–83. [Google Scholar] [CrossRef]
- Chokoeva, A.A.; Tchernev, G.; Tana, C.; Ananiev, J.; Wollina, U. Sarcoid-like pattern in a patient with tuberculosis. J. Biol. Regul. Homeost. Agents 2015, 28, 783–788. [Google Scholar]
- Tana, C.; Tchernev, G.; Chokoeva, A.A.; Wollina, U.; Lotti, T.; Fioranelli, M.; Roccia, M.G.; Maximov, G.K.; Silingardi, M. Pulmonary and abdominal sarcoidosis, the great imitators on imaging? J. Biol. Regul. Homeost. Agents 2016, 30, 45–48. [Google Scholar] [PubMed]
- Ganeshan, D.; Menias, C.O.; Lubner, M.G.; Pickhardt, P.J.; Sandrasegaran, K.; Bhalla, S. Sarcoidosis from Head to Toe: What the Radiologist Needs to Know. Radiographics 2018, 38, 1180–1200. [Google Scholar] [CrossRef] [PubMed]
- D’Ardes, D.; Tana, C.; Salzmann, A.; Ricci, F.; Guagnano, M.T.; Giamberardino, M.A.; Cipollone, F. Ultrasound assessment of SARS-CoV-2 pneumonia: A literature review for the primary care physician. Ann. Med. 2022, 54, 1140–1149. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Yakar, D.; Hope, M.D.; Kwee, R.M. Chest CT Imaging Signature of Coronavirus Disease 2019 Infection: In Pursuit of the Scientific Evidence. Chest 2020, 158, 1885–1895. [Google Scholar] [CrossRef] [PubMed]
- Infante, M.; Lutman, R.F.; Imparato, S.; Di Rocco, M.; Ceresoli, G.L.; Torri, V.; Morenghi, E.; Minuti, F.; Cavuto, S.; Bottoni, E.; et al. Differential diagnosis and management of focal ground-glass opacities. Eur. Respir. J. 2009, 33, 821–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsakok, M.T.; Watson, R.A.; Saujani, S.J.; Kong, M.; Xie, C.; Peschl, H.; Wing, L.; MacLeod, F.K.; Shine, B.; Talbot, N.P.; et al. Chest CT and Hospital Outcomes in Patients with Omicron Compared with Delta Variant SARS-CoV-2 Infection. Radiology 2022, 21, 220533. [Google Scholar] [CrossRef]
- Tana, C.; Mantini, C.; Donatiello, I.; Mucci, L.; Tana, M.; Ricci, F.; Cipollone, F.; Giamberardino, M.A. Clinical Features and Diagnosis of Cardiac Sarcoidosis. J. Clin. Med. 2021, 10, 1941. [Google Scholar] [CrossRef]
- Ricci, F.; Mantini, C.; Grigoratos, C.; Bianco, F.; Bucciarelli, V.; Tana, C.; Mastrodicasa, D.; Caulo, M.; Donato Aquaro, G.; Raffaele Cotroneo, A.; et al. The Multi-modality Cardiac Imaging Approach to Cardiac Sarcoidosis. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2018, 15, 10–20. [Google Scholar] [CrossRef]
- Di Dedda, E.A.; Barison, A.; Aquaro, G.D.; Ismail, T.F.; Hua, A.; Mantini, C.; Ricci, F.; Pontone, G.; Volpe, A.; Secchi, F.; et al. Cardiac magnetic resonance imaging of myocarditis and pericarditis following COVID-19 vaccination: A multicenter collection of 27 cases. Eur. Radiol. 2022, 32, 4352–4360. [Google Scholar] [CrossRef]
- Siripanthong, B.; Asatryan, B.; Hanff, T.C.; Chatha, S.R.; Khanji, M.Y.; Ricci, F.; Muser, D.; Ferrari, V.A.; Nazarian, S.; Santangeli, P.; et al. The Pathogenesis and Long-Term Consequences of COVID-19 Cardiac Injury. JACC Basic Transl. Sci. 2022, 7, 294–308. [Google Scholar] [CrossRef]
- Bisaccia, G.; Ricci, F.; Recce, V.; Serio, A.; Iannetti, G.; Chahal, A.A.; Ståhlberg, M.; Khanji, M.Y.; Fedorowski, A.; Gallina, S. Post-Acute Sequelae of COVID-19 and Cardiovascular Autonomic Dysfunction: What Do We Know? J. Cardiovasc. Dev. Dis. 2021, 8, 156. [Google Scholar] [CrossRef] [PubMed]
- Aveyard, P.; Gao, M.; Lindson, N.; Hartmann-Boyce, J.; Watkinson, P.; Young, D.; Coupland, C.A.C.; Tan, P.S.; Clift, A.K.; Harrison, D.; et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: A population cohort study. Lancet Respir. Med. 2021, 9, 909–923. [Google Scholar] [CrossRef]
- Morgenthau, A.S.; Levin, M.A.; Freeman, R.; Reich, D.L.; Klang, E. Moderate or Severe Impairment in Pulmonary Function is Associated with Mortality in Sarcoidosis Patients Infected with SARS-CoV-2. Lung 2020, 198, 771–775. [Google Scholar] [CrossRef]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.I.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Sweiss, N.J.; Korsten, P.; Syed, H.J.; Syed, A.; Baughman, R.P.; Yee, A.M.F.; Culver, D.A.; Sosenko, T.; Azuma, A.; Bonella, F.; et al. When the Game Changes: Guidance to Adjust Sarcoidosis Management During the Coronavirus Disease 2019 Pandemic. Chest 2020, 158, 892–895. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, M.; Rabe, K.F.; Taube, C.; Joest, M.; Kreuter, M.; Wirtz, H.; Blum, T.G.; Kolditz, M.; Geerdes-Fenge, H.; Otto-Knapp, R.; et al. Risk Assessment for Patients with Chronic Respiratory Conditions in the Context of the SARS-CoV-2 Pandemic Statement of the German Respiratory Society with the support of the German Association of Chest Physicians. Respiration 2022, 101, 307–320. [Google Scholar] [CrossRef]
- Tana, C.; Schiavone, C.; Cipollone, F.; Giamberardino, M.A. Management Issues of Sarcoidosis in the Time of Coronavirus Disease 2019. Chest 2021, 159, 1306–1307. [Google Scholar] [CrossRef]
- Kahlmann, V.; Manansala, M.; Moor, C.C.; Shahrara, S.; Wijsenbeek, M.S.; Sweiss, N.J. COVID-19 infection in patients with sarcoidosis: Susceptibility and clinical outcomes. Curr. Opin. Pulm. Med. 2021, 27, 463–471. [Google Scholar] [CrossRef]
- Manansala, M.; Baughman, R.; Novak, R.; Judson, M.; Sweiss, N. Management of immunosuppressants in the era of coronavirus disease-2019. Curr. Opin. Pulm. Med. 2021, 27, 176–183. [Google Scholar] [CrossRef]
- Wagner, C.; Griesel, M.; Mikolajewska, A.; Mueller, A.; Nothacker, M.; Kley, K.; Metzendorf, M.I.; Fischer, A.L.; Kopp, M.; Stegemann, M.; et al. Systemic corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014963. [Google Scholar]
- Griesel, M.; Wagner, C.; Mikolajewska, A.; Stegemann, M.; Fichtner, F.; Metzendorf, M.I.; Nair, A.A.; Daniel, J.; Fischer, A.L.; Skoetz, N. Inhaled corticosteroids for the treatment of COVID-19. Cochrane Database Syst. Rev. 2022, 3, CD015125. [Google Scholar] [PubMed]
- Geriatric Medicine Research Collaborative; Covid Collaborative; Welch, C. Age and frailty are independently associated with increased COVID-19 mortality and increased care needs in survivors: Results of an international multi-centre study. Age Ageing 2021, 50, 617–630. [Google Scholar] [PubMed]
- Ticinesi, A.; Nouvenne, A.; Cerundolo, N.; Parise, A.; Prati, B.; Guerra, A.; Meschi, T. Trends of COVID-19 Admissions in an Italian Hub during the Pandemic Peak: Large Retrospective Study Focused on Older Subjects. J. Clin. Med. 2021, 10, 1115. [Google Scholar] [CrossRef]
- Kondle, S.; Hou, T.; Manansala, M.; Ascoli, C.; Novak, R.M.; Sweiss, N. Treatment of COVID-19 in Patients with Sarcoidosis. Front. Med. 2021, 8, 689539. [Google Scholar] [CrossRef] [PubMed]
- Manansala, M.; Chopra, A.; Baughman, R.P.; Novak, R.; Lower, E.E.; Culver, D.A.; Korsten, P.; Drake, W.P.; Judson, M.A.; Sweiss, N. COVID-19 and Sarcoidosis, Readiness for Vaccination: Challenges and Opportunities. Front. Med. 2021, 8, 672028. [Google Scholar] [CrossRef]
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; Arasaratnam, R.J.; Baden, L.R.; Bass, A.R.; Calabrese, C.; Gravallese, E.M.; Harpaz, R.; Kroger, A.; et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients with Rheumatic and Musculoskeletal Diseases: Version 4. Arthritis Rheumatol. 2022, 74, e21–e36. [Google Scholar] [CrossRef]
- Simon, D.; Tascilar, K.; Fagni, F.; Krönke, G.; Kleyer, A.; Meder, C.; Atreya, R.; Leppkes, M.; Kremer, A.E.; Ramming, A.; et al. SARS-CoV-2 vaccination responses in untreated, conventionally treated and anticytokine-treated patients with immune-mediated inflammatory diseases. Ann. Rheum. Dis. 2021, 80, 1312–1316. [Google Scholar] [CrossRef]
- Tavana, S.; Argani, H.; Gholamin, S.; Razavi, S.M.; Keshtkar-Jahromi, M.; Talebian, A.S.; Moghaddam, K.G.; Sepehri, Z.; Azad, T.M.; Keshtkar-Jahromi, M. Influenza vaccination in patients with pulmonary sarcoidosis: Efficacy and safety. Influ. Other Respir. Viruses 2011, 6, 136–141. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Country | Spain [67] | US [68] | US [69] | France [70] | US [71] | All over the world [72] |
| Initial cohort | 882 (calculated) sarcoidosis patients | 236 sarcoidosis patients | 899 sarcoidosis patients | 199 sarcoidosis patients | 278,271 COVID patients, of which 954 with pulmonary sarcoidosis | 5200 sarcoidosis patients (self-reported questionnaire) |
| Time | 2020 | 12 March to 30 April 2020 | 2nd semester 2020 | Feb–May 2020 | Jan–Oct 2020 | |
| Prevalence of infection | 5.1% (45 patients) | 2.1% (5 patients) | 8.9% (77 patients) | 4.02% (8 patients) | N/A | 2.23% (116 patients) |
| Symptomatic | 36/45 (80%) | 5/5 (100%) | Not specified | 8 (100%) | N/A | |
| Hospitalized | 14/45 (31%) | 2/5 (40%) | 19 (25%) | 3/8 (37.5%) | 181/954 (18.87%) | 18/116 (15.8%) |
| ICU | 2/45 (4.4%) | 2/5 (40%) | 6/19 (31%) | 2/8 (25%) | 66/954 (6.9%) | Unknown |
| Died | 4/45 (9%) | 1/5 (20%) | 1/77 (1%) | 1/8 (12.5%) | 41/954 (4.29%) | N/A |
| Relation treatment-severity? | Not evaluated | Not evaluated | Not evaluated | Not evaluated | Not evaluated | None |
| N/A = not applicable |
| Clinical Scenario | Management during the COVID-19 Pandemic |
|---|---|
| Stable disease not requiring drug treatment | No treatment |
| Stable disease under glucocorticoids only | Reduction to the lowest effective dose |
| Stable disease under DMASD | Reduction of doses, prolongation of intervals, possible drug holiday |
| Stable disease under biologicals | Reduction of doses, prolongation of intervals |
| Non-life-threatening disease flare | Increase glucocorticoid doses to the lowest effective dose |
| Active disease under glucocorticoids only | Reduction to the lowest effective dose |
| Active disease under DMASD | Continuation of DMASD only if benefits outweigh risks of severe COVID-19 |
| Active disease under biologicals | Continuation of treatment (different routes are possible during lockdowns) |
| Continued active disease | Consideration of alternative treatments |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tana, C.; Cinetto, F.; Mantini, C.; Bernardinello, N.; Tana, M.; Ricci, F.; Ticinesi, A.; Meschi, T.; Scarpa, R.; Cipollone, F.; et al. Sarcoidosis and COVID-19: At the Cross-Road between Immunopathology and Clinical Manifestation. Biomedicines 2022, 10, 2525. https://doi.org/10.3390/biomedicines10102525
Tana C, Cinetto F, Mantini C, Bernardinello N, Tana M, Ricci F, Ticinesi A, Meschi T, Scarpa R, Cipollone F, et al. Sarcoidosis and COVID-19: At the Cross-Road between Immunopathology and Clinical Manifestation. Biomedicines. 2022; 10(10):2525. https://doi.org/10.3390/biomedicines10102525
Chicago/Turabian StyleTana, Claudio, Francesco Cinetto, Cesare Mantini, Nicol Bernardinello, Marco Tana, Fabrizio Ricci, Andrea Ticinesi, Tiziana Meschi, Riccardo Scarpa, Francesco Cipollone, and et al. 2022. "Sarcoidosis and COVID-19: At the Cross-Road between Immunopathology and Clinical Manifestation" Biomedicines 10, no. 10: 2525. https://doi.org/10.3390/biomedicines10102525