
Arginine Availability in Reamed Intramedullary Aspirate as Predictor of Outcome in Nonunion Healing
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Inclusion
2.2. High-Performance Liquid Chromatography Amino Acid Analysis
2.3. RNA Isolation and qPCR
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
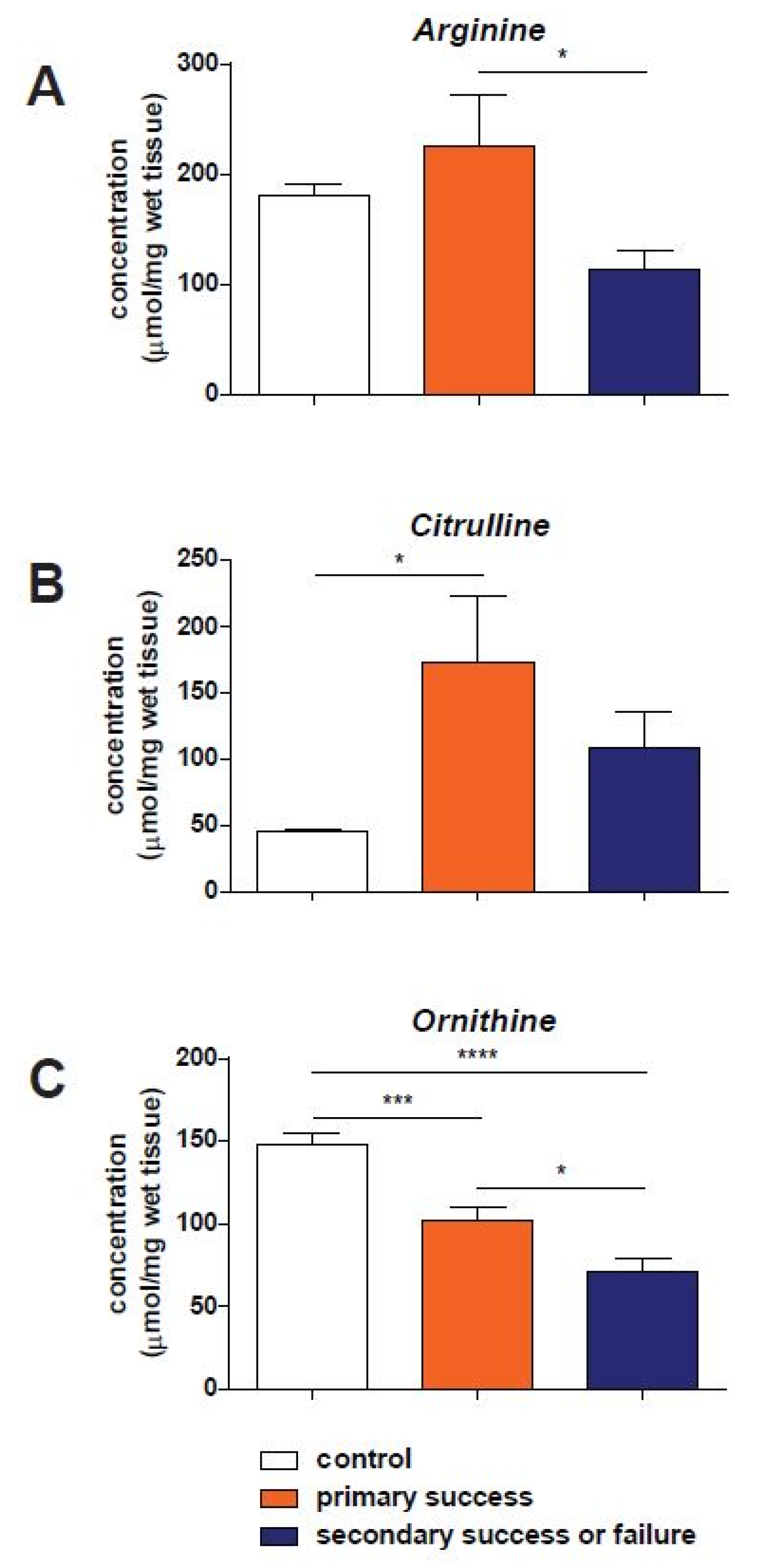
3.2. Amino Acid Concentrations
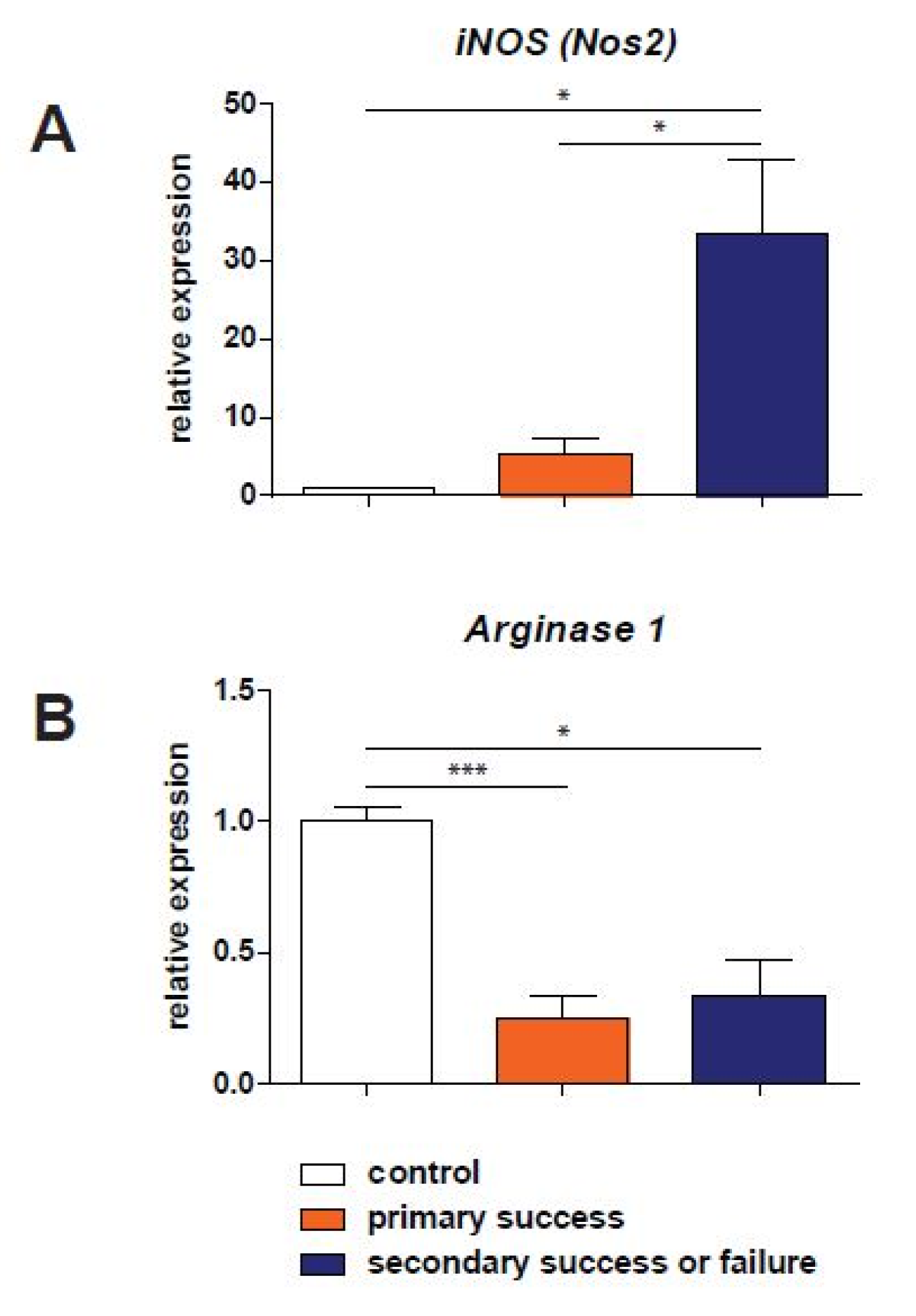
3.3. qPCR Analysis
3.4. Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mills, L.A.; Aitken, S.A.; Simpson, A. The risk of non-union per fracture: Current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, J.A.; Palanca, A.A.; Bellino, M.J.; Lowenberg, D.W. Assessment of compromised fracture healing. J. Am. Acad. Orthop. Surg. 2012, 20, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Karladani, A.H.; Granhed, H.; Karrholm, J.; Styf, J. The influence of fracture etiology and type on fracture healing: A review of 104 consecutive tibial shaft fractures. Arch. Orthop. Trauma Surg. 2001, 121, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Kanakaris, N.K.; Giannoudis, P.V. The health economics of the treatment of long-bone non-unions. Injury 2007, 38 (Suppl. S2), S77–S84. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Einhorn, T.A.; Marsh, D. Fracture healing: The diamond concept. Injury 2007, 38 (Suppl. S4), S3–S6. [Google Scholar] [CrossRef]
- Masquelet, A.C.; Begue, T. The concept of induced membrane for reconstruction of long bone defects. Orthop. Clin. N. Am. 2010, 41, 27–37. [Google Scholar] [CrossRef]
- Dawson, J.; Kiner, D.; Gardner, W., 2nd; Swafford, R.; Nowotarski, P.J. The reamer-irrigator-aspirator as a device for harvesting bone graft compared with iliac crest bone graft: Union rates and complications. J. Orthop. Trauma 2014, 28, 584–590. [Google Scholar] [CrossRef]
- Belthur, M.V.; Conway, J.D.; Jindal, G.; Ranade, A.; Herzenberg, J.E. Bone graft harvest using a new intramedullary system. Clin. Orthop. Relat. Res. 2008, 466, 2973–2980. [Google Scholar] [CrossRef] [Green Version]
- Stafford, P.R.; Norris, B.L. Reamer-irrigator-aspirator bone graft and bi Masquelet technique for segmental bone defect nonunions: A review of 25 cases. Injury 2010, 41 (Suppl. S2), S72–S77. [Google Scholar] [CrossRef]
- Wijnands, K.A.; Brink, P.R.; Weijers, P.H.; Dejong, C.H.; Poeze, M. Impaired fracture healing associated with amino acid disturbances. Am. J. Clin. Nutr. 2012, 95, 1270–1277. [Google Scholar] [CrossRef]
- Chae, H.J.; Park, R.K.; Chung, H.T.; Kang, J.S.; Kim, M.S.; Choi, D.Y.; Bang, B.G.; Kim, H.R. Nitric oxide is a regulator of bone remodelling. J. Pharm. Pharmacol. 1997, 49, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Corbett, S.A.; McCarthy, I.D.; Batten, J.; Hukkanen, M.; Polak, J.M.; Hughes, S.P. Nitric oxide mediated vasoreactivity during fracture repair. Clin. Orthop. Relat. Res. 1999, 365, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Vittur, F.; Lunazzi, G.; Moro, L.; Stagni, N.; de Bernard, B.; Moretti, M.; Stanta, G.; Bacciottini, F.; Orlandini, G.; Reali, N.; et al. A possible role for polyamines in cartilage in the mechanism of calcification. Biochim. Biophys. Acta 1986, 881, 38–45. [Google Scholar] [CrossRef]
- Xia, W.; Szomor, Z.; Wang, Y.; Murrell, G.A. Nitric oxide enhances collagen synthesis in cultured human tendon cells. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2006, 24, 159–172. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Murrell, G.A.; Lin, J.; Gardiner, E.M.; Diwan, A.D. Localization of nitric oxide synthases during fracture healing. J. Bone Miner. Res. 2002, 17, 1470–1477. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.; Diwan, A.D.; Lin, J.H.; Murrell, G.A. Nitric oxide synthase isoforms during fracture healing. J. Bone Miner. Res. 2001, 16, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Meesters, D.M.; Neubert, S.; Wijnands, K.A.; Heyer, F.L.; Zeiter, S.; Ito, K.; Brink, P.R.; Poeze, M. Deficiency of inducible and endothelial nitric oxide synthase results in diminished bone formation and delayed union and nonunion development. Bone 2016, 83, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Diwan, A.D.; Wang, M.X.; Jang, D.; Zhu, W.; Murrell, G.A. Nitric oxide modulates fracture healing. J. Bone Miner. Res. 2000, 15, 342–351. [Google Scholar] [CrossRef]
- van Eijk, H.M.; Rooyakkers, D.R.; Deutz, N.E. Rapid routine determination of amino acids in plasma by high-performance liquid chromatography with a 2–3 microns Spherisorb ODS II column. J. Chromatogr. 1993, 620, 143–148. [Google Scholar] [CrossRef]
- Mills, L.A.; Simpson, A.H. The relative incidence of fracture non-union in the Scottish population (5.17 million): A 5-year epidemiological study. BMJ Open 2013, 3, e002276. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Gudipati, S.; Harwood, P.; Kanakaris, N.K. Long bone non-unions treated with the diamond concept: A case series of 64 patients. Injury 2015, 46 (Suppl. S8), S48–S54. [Google Scholar] [CrossRef]
- Pountos, I.; Georgouli, T.; Pneumaticos, S.; Giannoudis, P.V. Fracture non-union: Can biomarkers predict outcome? Injury 2013, 44, 1725–1732. [Google Scholar] [CrossRef] [PubMed]
- Wildemann, B.; Ignatius, A.; Leung, F.; Taitsman, L.A.; Smith, R.M.; Pesantez, R.; Stoddart, M.J.; Richards, R.G.; Jupiter, J.B. Non-union bone fractures. Nat. Rev. Dis. Primers 2021, 7, 57. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Einhorn, T.A.; Schmidmaier, G.; Marsh, D. The diamond concept--open questions. Injury 2008, 39 (Suppl. S2), S5–S8. [Google Scholar] [CrossRef]
- Ramamurthy, C.; Cutler, L.; Nuttall, D.; Simison, A.J.; Trail, I.A.; Stanley, J.K. The factors affecting outcome after non-vascular bone grafting and internal fixation for nonunion of the scaphoid. J. Bone Joint Surg. Br. 2007, 89, 627–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calori, G.M.; Phillips, M.; Jeetle, S.; Tagliabue, L.; Giannoudis, P.V. Classification of non-union: Need for a new scoring system? Injury 2008, 39 (Suppl. S2), S59–S63. [Google Scholar] [CrossRef]
- Zura, R.; Della Rocca, G.J.; Mehta, S.; Harrison, A.; Brodie, C.; Jones, J.; Steen, R.G. Treatment of chronic (>1 year) fracture nonunion: Heal rate in a cohort of 767 patients treated with low-intensity pulsed ultrasound (LIPUS). Injury 2015, 46, 2036–2041. [Google Scholar] [CrossRef] [Green Version]
- Granchi, D.; Gomez-Barrena, E.; Rojewski, M.; Rosset, P.; Layrolle, P.; Spazzoli, B.; Donati, D.M.; Ciapetti, G. Changes of Bone Turnover Markers in Long Bone Nonunions Treated with a Regenerative Approach. Stem Cells Int. 2017, 2017, 3674045. [Google Scholar] [CrossRef] [Green Version]
- Meesters, D.M.; Hannemann, P.F.; van Eijk, H.M.; Schriebl, V.T.; Brink, P.R.; Poeze, M.; Wijnands, K.A. Enhancement of fracture healing after citrulline supplementation in mice. Eur. Cell Mater. 2020, 39, 183–192. [Google Scholar] [CrossRef]
- Kdolsky, R.K.; Mohr, W.; Savidis-Dacho, H.; Beer, R.; Puig, S.; Reihsner, R.; Tangl, S.; Donath, K. The influence of oral L-arginine on fracture healing: An animal study. Wien. Klin. Wochenschr. 2005, 117, 693–701. [Google Scholar] [CrossRef]
- Baldik, Y.; Diwan, A.D.; Appleyard, R.C.; Fang, Z.M.; Wang, Y.; Murrell, G.A. Deletion of iNOS gene impairs mouse fracture healing. Bone 2005, 37, 32–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claes, L.; Recknagel, S.; Ignatius, A. Fracture healing under healthy and inflammatory conditions. Nat. Rev. Rheumatol. 2012, 8, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Schindeler, A.; McDonald, M.M.; Bokko, P.; Little, D.G. Bone remodeling during fracture repair: The cellular picture. Semin. Cell Dev. Biol. 2008, 19, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Wijnands, K.A.; Hoeksema, M.A.; Meesters, D.M.; van den Akker, N.M.; Molin, D.G.; Briede, J.J.; Ghosh, M.; Kohler, S.E.; van Zandvoort, M.A.; de Winther, M.P.; et al. Arginase-1 deficiency regulates arginine concentrations and NOS2-mediated NO production during endotoxemia. PLoS ONE 2014, 9, e86135. [Google Scholar] [CrossRef] [Green Version]
- van Basten Batenburg, M.; Houben, I.B.; Blokhuis, T.J. The Non-Union Scoring System: An interobserver reliability study. Eur. J. Trauma Emerg. Surg. 2019, 45, 13–19. [Google Scholar] [CrossRef]
- Calori, G.M.; Colombo, M.; Mazza, E.L.; Mazzola, S.; Malagoli, E.; Marelli, N.; Corradi, A. Validation of the Non-Union Scoring System in 300 long bone non-unions. Injury 2014, 45 (Suppl. S6), S93–S97. [Google Scholar] [CrossRef]
- Flynn, N.E.; Meininger, C.J.; Haynes, T.E.; Wu, G. The metabolic basis of arginine nutrition and pharmacotherapy. Biomed. Pharmacother. 2002, 56, 427–438. [Google Scholar] [CrossRef]
- Windmueller, H.G.; Spaeth, A.E. Source and fate of circulating citrulline. Am. J. Physiol. 1981, 241, E473–E480. [Google Scholar] [CrossRef]
- Wu, G.; Morris, S.M., Jr. Arginine metabolism: Nitric oxide and beyond. Biochem. J. 1998, 336 Pt 1, 1–17. [Google Scholar] [CrossRef]
- Moinard, C.; Cynober, L. Citrulline: A new player in the control of nitrogen homeostasis. J. Nutr. 2007, 137, 1621S–1625S. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Normal Bone Healing (Control Group) N = 8 | Nonunion with Primary Success N = 9 | Refractory Nonunion N = 8 | Significance | |
|---|---|---|---|---|
| Age (years) | 58 (30–66) | 64 (51–86) | 44 (18–71) | p = 0.03 * |
| Male/Female | 4/4 | 3/6 | 5/3 | N.S. |
| Length (cm) | 174 (166–191) | 172 (160–187) | 176 (165–192) | N.S. |
| Weight (kg) | 80 (65–94) | 83 (60–108) | 81 (62–108) | N.S. |
| BMI (kg/cm2) | 20.0 (19.1–30.4) | 28.0 (22.9–31.2) | 26.5 (19.0–39.7) | p < 0.05 ^ |
| Alcohol use (yes/no) | 3/5 | 5/4 | 1/7 | N.S. |
| Smoking (yes/no) | 6/2 | 5/4 | 6/2 | N.S. |
| NSAID use (yes/no) | 2/6 | 1/8 | 2/6 | N.S. |
| DM (yes/no) | 2/6 | 2/7 | 3/5 | N.S. |
| Localization (n) Femur Tibia Humerus Radius | 4 4 0 0 | 2 3 3 1 | 5 1 2 0 | n.a. |
| Defect size (mm) | n.a. | 30.4 (6–84) | 50.4 (8–155) | N.S. |
| Gustilo (n) 0 1 2 3 | 8 0 0 0 | 5 2 0 2 | 2 1 1 4 | |
| NUSS score (0–100) | n.a. | 64 (51–86) | 44 (18–71) | p = 0.03 * |
| Time between fracture and sampling (days) | 2 (1–4) | 499 (65–1143) | 655 (191–2331) |
| Gene | Name | Sequence (5′ → 3′) |
|---|---|---|
| Ppia | Cyclophylin-A (Fw) Cyclophylin-A (Rev) | CTCGAATAAGTTTGACTTGTGTTT CTAGGCATGGGAGGGAACA |
| ActB | Beta-actin (Fw) Beta-actin (Rev) | GCTGTGCTACGTCGCCCTG GGAGGAGCTGGAAGCAGCC |
| Nos2 | iNOS (Fw) iNOS (Rev) | TTGCAAGCTGATGGTCAAGATC CAACCCGAGCTCCTGGAA |
| Nos3 | eNOS (Fw) eNOS (Rev) | TTAATGTGGCCGTGTTGCA CTCTTGATGGAAGACAGGAGTTAGG |
| Arg1 | Arginase-1 (Fw) Arginase-1 (Rev) | CGCCAAGTCCAGAACCATAGG TCTCAATACTGTAGGGCCTTCTT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meesters, D.M.; Wijnands, K.A.P.; van Eijk, H.M.H.; Hofman, M.; Hildebrand, F.; Verbruggen, J.P.A.M.; Brink, P.R.G.; Poeze, M. Arginine Availability in Reamed Intramedullary Aspirate as Predictor of Outcome in Nonunion Healing. Biomedicines 2022, 10, 2474. https://doi.org/10.3390/biomedicines10102474
Meesters DM, Wijnands KAP, van Eijk HMH, Hofman M, Hildebrand F, Verbruggen JPAM, Brink PRG, Poeze M. Arginine Availability in Reamed Intramedullary Aspirate as Predictor of Outcome in Nonunion Healing. Biomedicines. 2022; 10(10):2474. https://doi.org/10.3390/biomedicines10102474
Chicago/Turabian StyleMeesters, Dennis M., Karolina A. P. Wijnands, Hans M. H. van Eijk, Martijn Hofman, Frank Hildebrand, Jan P. A. M. Verbruggen, Peter R. G. Brink, and Martijn Poeze. 2022. "Arginine Availability in Reamed Intramedullary Aspirate as Predictor of Outcome in Nonunion Healing" Biomedicines 10, no. 10: 2474. https://doi.org/10.3390/biomedicines10102474