
Does Customized Handle Toothbrush Influence Dental Plaque Removal in Children with Down Syndrome? A Randomized Controlled Trial

 , ,
, ,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
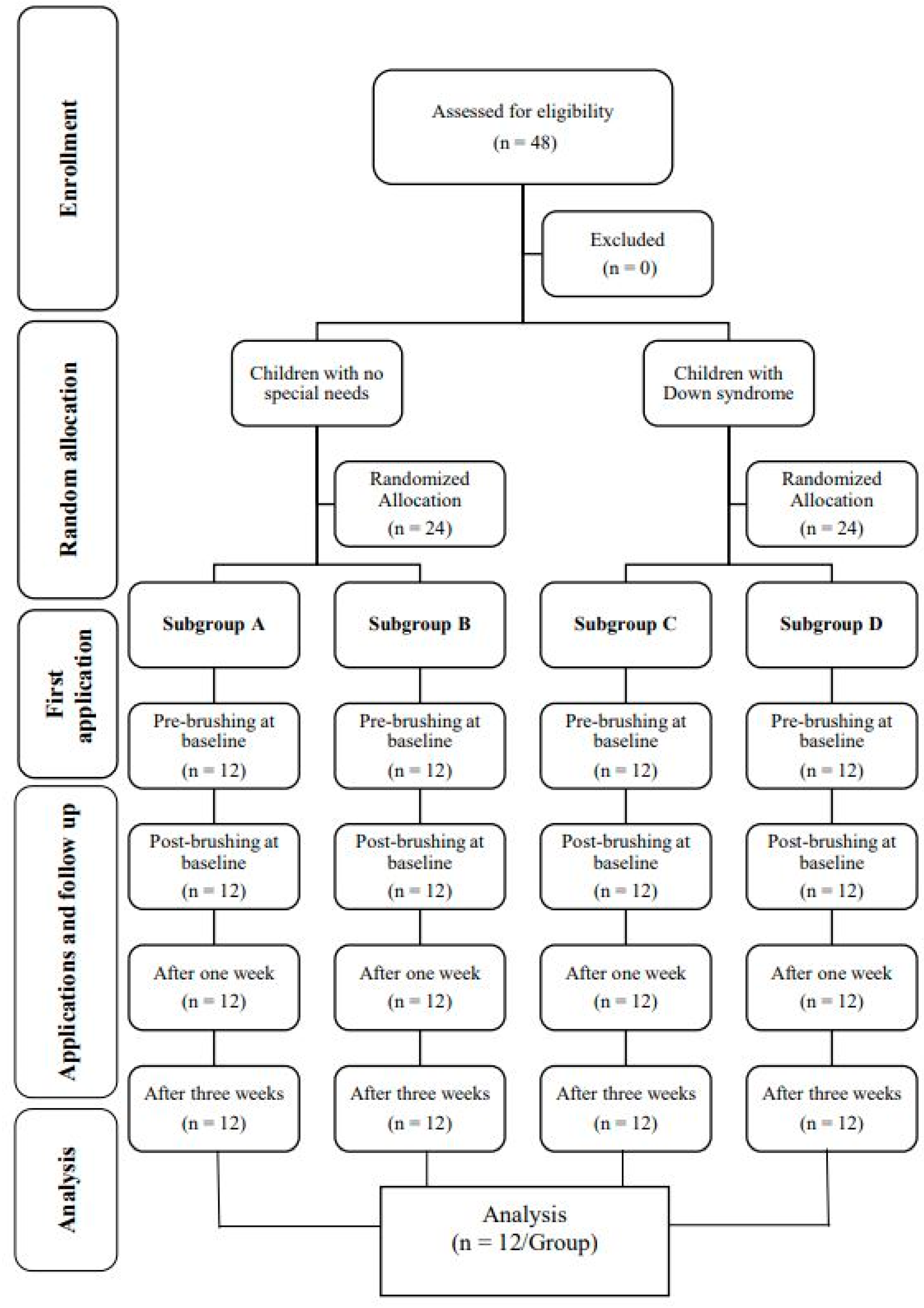
2.1. Study Design
2.2. Sample Size Calculation
2.3. Randomization and Blinding
2.4. Participants
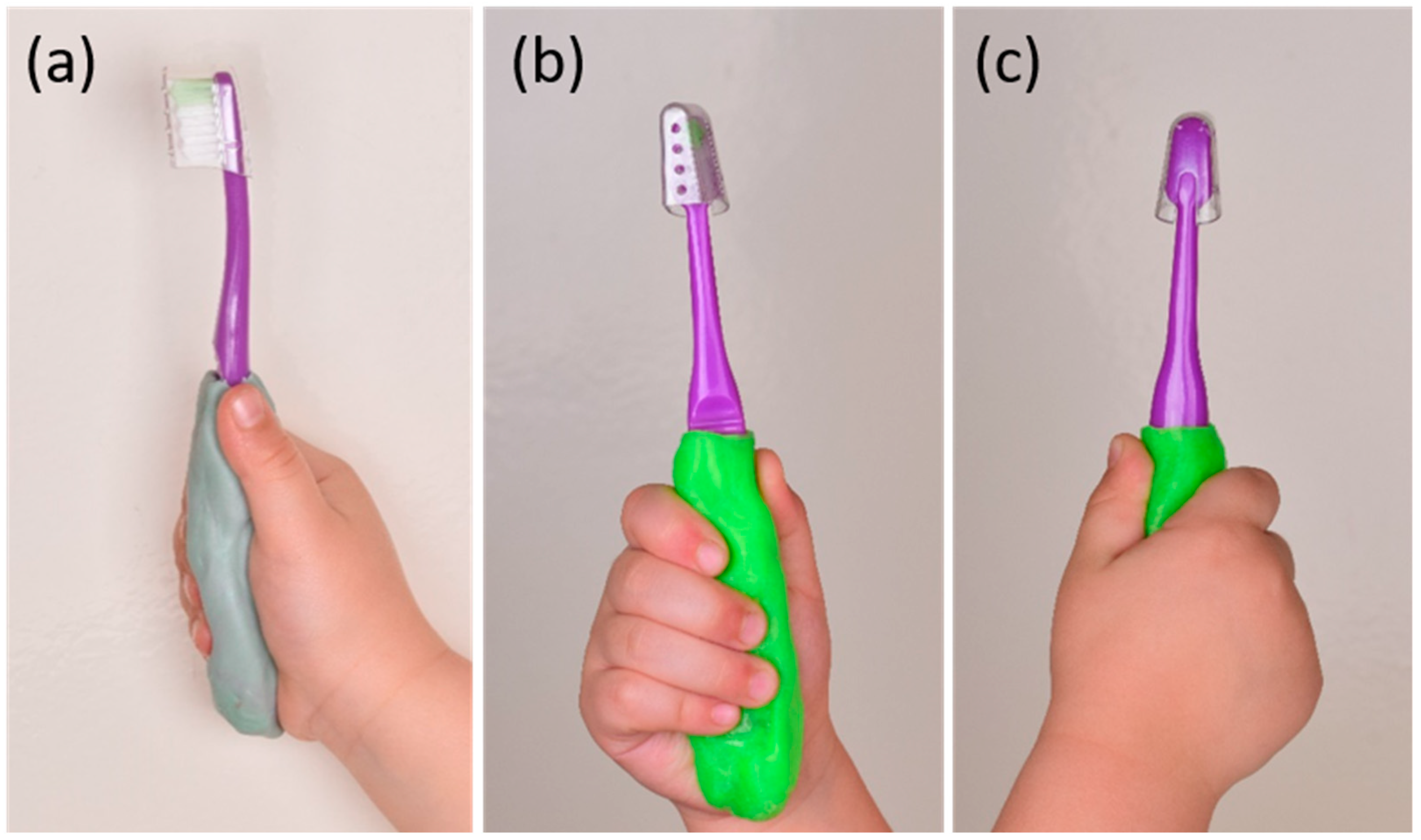
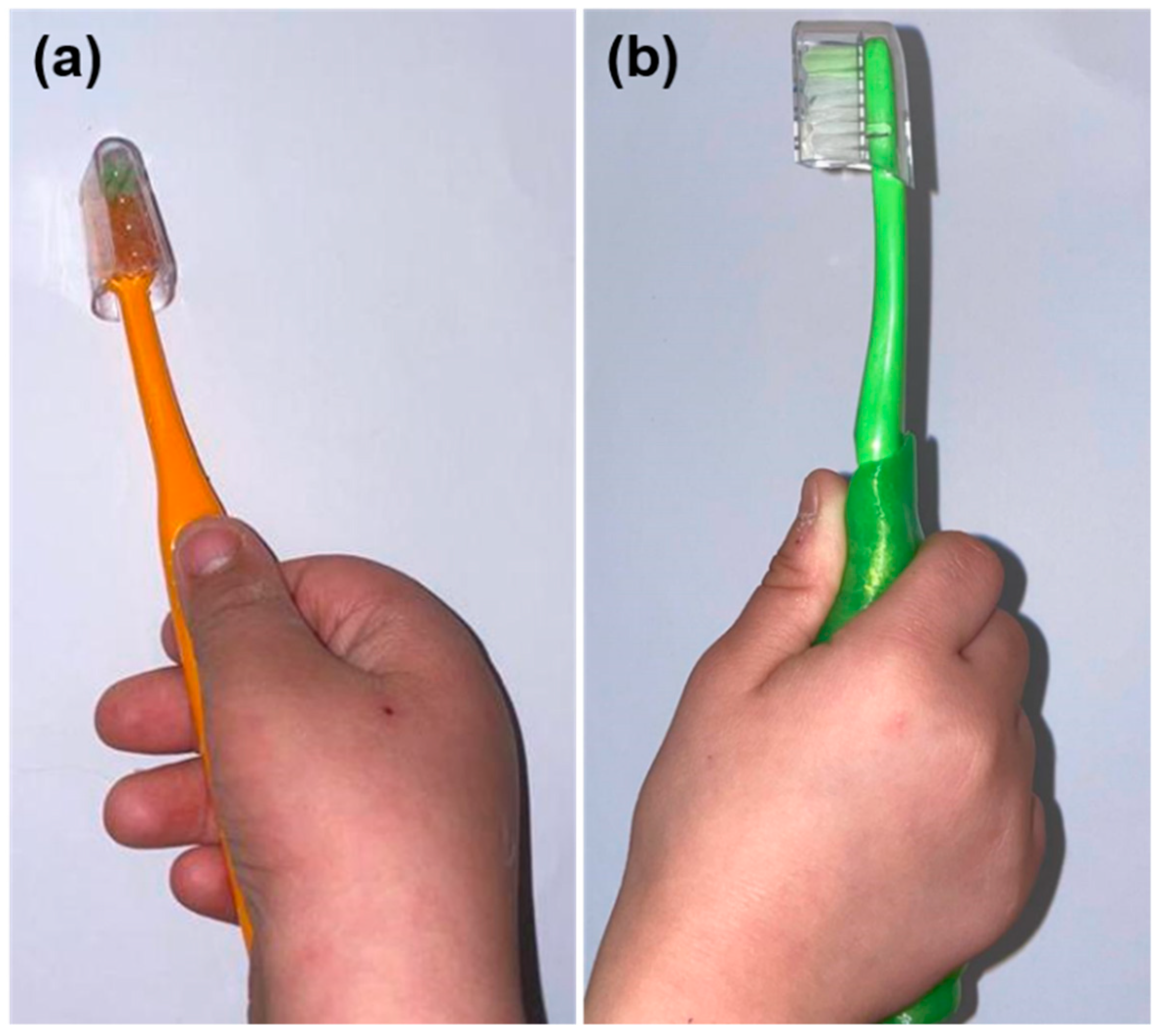
2.5. Intervention and Customized Handle Toothbrush Fabrication
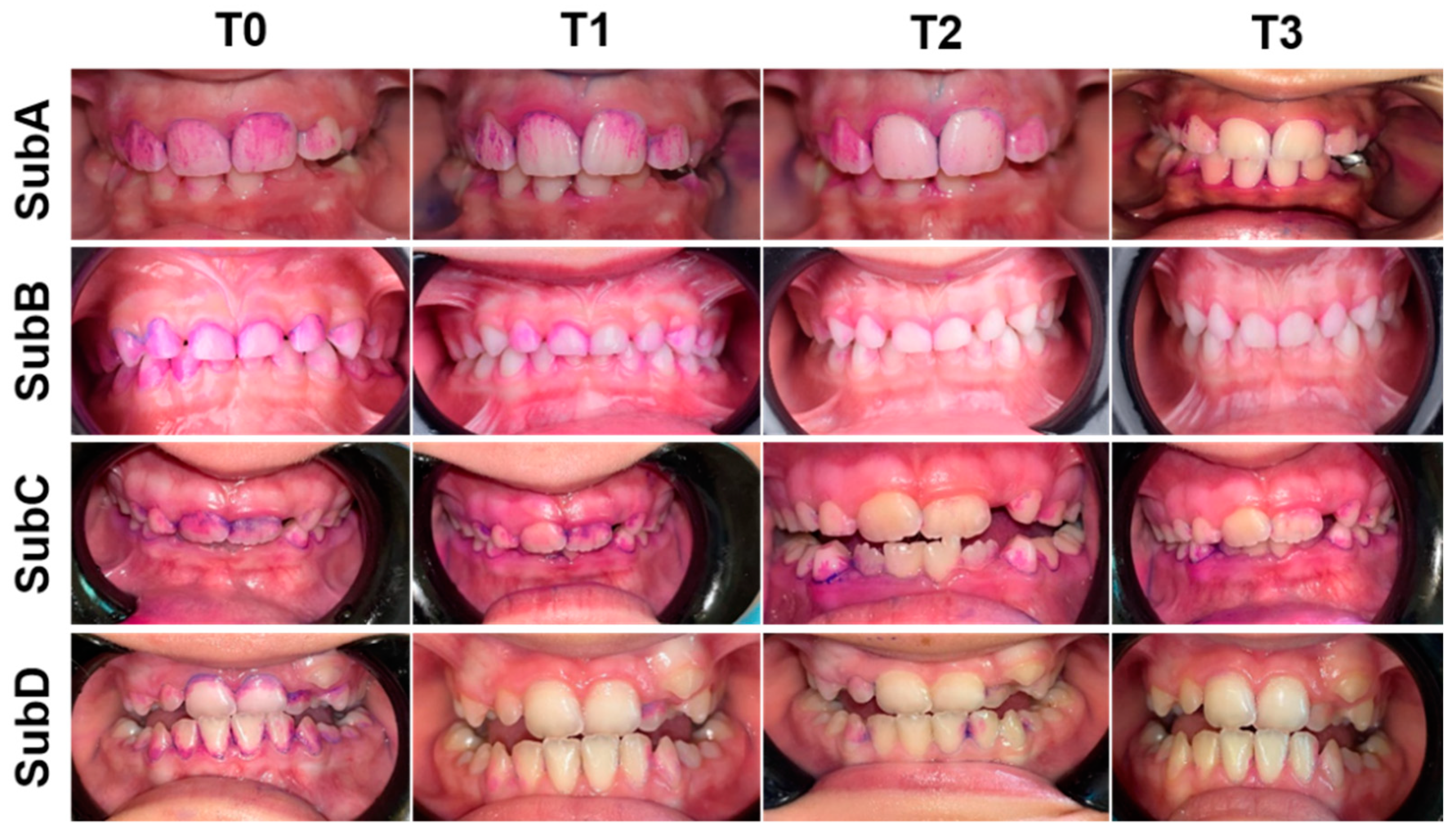
2.6. Evaluation and Follow Up
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, P.E.; Baez, R.J.; Ogawa, H. Global application of oral disease prevention and health promotion as measured 10 years after the 2007 World Health Assembly statement on oral health. Community Dent. Oral Epidemiol. 2020, 48, 338–348. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, S.; Ohsumi, T.; Noiri, Y. Evidence-based strategy for dental biofilms: Current evidence of mouthwashes on dental biofilm and gingivitis. Jpn. Dent. Sci. Rev. 2019, 55, 33–40. [Google Scholar] [CrossRef]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2014, 64, 57–80. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, N.; Singh, S. Periodontitis. In StatPearls, StatPearls Publishing Copyright©; StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Sälzer, S.; Graetz, C.; Dörfer, C.E.; Slot, D.E.; Van Der Weijden, F.A. Contemporary practices for mechanical oral hygiene to prevent periodontal disease. Periodontology 2000 2020, 84, 35–44. [Google Scholar] [CrossRef]
- Hayasaki, H.; Saitoh, I.; Nakakura-Ohshima, K.; Hanasaki, M.; Nogami, Y.; Nakajima, T.; Inada, E.; Iwasaki, T.; Iwase, Y.; Sawami, T.; et al. Tooth brushing for oral prophylaxis. Jpn. Dent. Sci. Rev. 2014, 50, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Ng, E.; Lim, L.P. An Overview of Different Interdental Cleaning Aids and Their Effectiveness. Dent. J. 2019, 7, 56. [Google Scholar] [CrossRef] [Green Version]
- Vyas, T.; Bhatt, G.; Gaur, A.; Sharma, C.; Sharma, A.; Nagi, R. Chemical plaque control—A brief review. J. Fam. Med. Prim. Care 2021, 10, 1562–1568. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.P.; Patil, P.B.; Kashetty, M.V. Effectiveness of different tooth brushing techniques on the removal of dental plaque in 6-8 year old children of Gulbarga. J. Int. Soc. Prev. Community Dent. 2014, 4, 113–116. [Google Scholar] [CrossRef] [Green Version]
- Pujar, P.; Subbareddy, V.V. Evaluation of the tooth brushing skills in children aged 6–12 years. Eur. Arch. Paediatr. Dent. 2013, 14, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Sandström, A.; Cressey, J.; Stecksén-Blicks, C. Tooth-brushing behaviour in 6–12 year olds. Int. J. Paediatr. Dent. 2010, 21, 43–49. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Fast Facts. 2013. Available online: www.aapd.Org/assets/1/7/fastfacts.pdf (accessed on 11 August 2014).
- Wilkins, E.M. Clinical Practice of the Dental Hygienist, 11th ed.; Lippincott and Williams: Philadelphia, PA, USA, 2013. [Google Scholar]
- Baruah, K.; Thumpala, V.; Khetani, P.; Baruah, Q.; Tiwari, R.; Dixit, H. A Review on Toothbrushes and Tooth Brushing Methods. Int. J. Pharm. Sci. Invent. 2017, 6, 29–38. [Google Scholar]
- Asim, A.; Kumar, A.; Muthuswamy, S.; Jain, S.; Agarwal, S. Down syndrome: An insight of the disease. J. Biomed. Sci. 2015, 22, 41. [Google Scholar] [CrossRef] [Green Version]
- Forés-Martos, J.; Cervera-Vidal, R.; Chirivella, E.; Ramos-Jarero, A.; Climent, J.; Martos, J.F. A genomic approach to study down syndrome and cancer inverse comorbidity: Untangling the chromosome 21. Front. Physiol. 2015, 6, 10. [Google Scholar] [CrossRef] [Green Version]
- Hennequin, M.; Allison, P.J.; Veyrune, J.L. Prevalence of oral health problems in a group of individuals with Down syndrome in France. Dev. Med. Child. Neurol. 2000, 42, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Allareddy, V.; Ching, N.; Macklin, E.A.; Voelz, L.; Weintraub, G.; Davidson, E.; Prock, L.A.; Rosen, D.; Brunn, R.; Skotko, B.G. Craniofacial features as assessed by lateral cephalometric measurements in children with Down syndrome. Prog. Orthod. 2016, 17, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deps, T.D.; Angelo, G.L.; Martins, C.; Paiva, S.M.; Pordeus, I.; Borges-Oliveira, A.C. Association between Dental Caries and Down Syndrome: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0127484. [Google Scholar] [CrossRef]
- Oredugba, F. Oral health condition and treatment needs of a group of Nigerian individuals with Down syndrome. Down Syndr. Res. Pract. 2007, 12, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Foley, C.; Killeen, O.G. Musculoskeletal anomalies in children with Down syndrome: An observational study. Arch. Dis. Child. 2018, 104, 482–487. [Google Scholar] [CrossRef] [Green Version]
- Elserty, N.; Wagdy, E. Influence of shoulder stabilization exercises on hand grip strength in children with Down syndrome: Randomized clinical trial. Bull. Fac. Phys. Ther. 2020, 25, 1–9. [Google Scholar] [CrossRef]
- Dougall, A.M.; Fiske, J. Access to special care dentistry, part 4. Education. Br. Dent. J. 2008, 205, 119–130. [Google Scholar] [CrossRef]
- Weddell, J.A.; Sanders, B.J.; Jones, J.E. Dental Problems of Children with Special Health Care Needs. In McDonald and Avery Dentistry for the Child and Adolescent, 10th ed.; Elsevier: Amsterdam, The Netherlands, 2011; pp. 460–486. [Google Scholar]
- Reeson, M.G.; Jepson, N.J. Customizing the size of toothbrush handles for patients with restricted hand and finger movement. J. Prosthet. Dent. 2002, 87, 700. [Google Scholar] [CrossRef]
- Kammers, A.C.; Zanetti, A.L.; Lacerda, T.E.; Aroca, J.P.; Camilotti, V.; Mendonça, M.J. Toothbrush Handles Individually Adapted for Use by Elderly Patients to Reduce Biofilm on Complete Dentures: A Pilot Study. J. Clin. Diagn. Res. JCDR 2015, 9, ZC94–ZC97. [Google Scholar] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef]
- Shamseer, L.; Hopewell, S.; Altman, U.G.; Moher, D.; Schulz, K.F. Update on the endorsement of CONSORT by high impact factor journals: A survey of journal “Instructions to Authors” in 2014. Trials 2016, 17, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stillman, P.R. A philosophy of treatment of periodontal disease. Dental. Digest. 1932, 38, 315–322. [Google Scholar]
- Droubi, L.; Laflouf, M.; Singh, P. Customized Handle for Toothbrush by Using 3D Printer. Int. J. Dent. Sci. Innov. Res. (IJDSIR) 2021, 4, 473–477. [Google Scholar]
- Quigley, G.A.; Hein, J.W. Comparative cleansing efficiency of manual and power brushing. J. Am. Dent. Assoc. 1962, 65, 26–29. [Google Scholar] [CrossRef]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced plaque formation by the chloromethyl analogue of victamine C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef] [Green Version]
- Lobene, R.R.; Weatherford, T.; Ross, N.M.; Lamm, R.A.; Menaker, L. A modified gingival index for use in clinical trials. Clin. Prev. Dent. 1986, 8, 3–6. [Google Scholar]
- Mehta, S.; Vyaasini, C.S.; Jindal, L.; Sharma, V.; Jasuja, T. Toothbrush, its design and modifications: An Overview. J. Curr. Med Res. Opin. 2020, 3, 570. [Google Scholar] [CrossRef]
- Hovliaras, C.; Gatzemeyer, J.; Jimenez, E.; Panagakos, F.S. Ergonomics and toothbrushes. J. Clin. Dent. 2015, 26, 28–32. [Google Scholar] [PubMed]
- Davidovich, E.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Cunningham, P.; Zini, A. Randomised clinical study of plaque removal efficacy of a power toothbrush in a paediatric population. Int. J. Paediatr. Dent. 2017, 27, 558–567. [Google Scholar] [CrossRef] [Green Version]
- Kayalvizhi, G.; Ramesh, V.; Arumugam, S.B.; Radha, S.; Mohandoss, S. Comparative Evaluation of Plaque Removal Effectiveness of Manual and Chewable Toothbrushes in Children: A Randomized Clinical Trial. Int. J. Clin. Pediatr. Dent. 2019, 12, 107–110. [Google Scholar] [CrossRef]
- Morinushi, T.; Lopatin, D.E.; Nakao, R.; Kinjyo, S. A Comparison of the Gingival Health of Children with Down Syndrome to Healthy Children Residing in an Institution. Spéc. Care Dent. 2006, 26, 13–19. [Google Scholar] [CrossRef]
- Pasiga, B. The Ability of Elderly to Clean Plaque on Full Denture Prosthesis Using Toothbrush with Special Grip Design. Int. J. Dent. Med. Sci. Res. 2018, 2, 22–27. [Google Scholar]
- Frank, K.; Esbensen, A.J. Fine motor and self-care milestones for individuals with Down syndrome using a Retrospective Chart Review. J. Intellect. Disabil. Res. 2015, 59, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Corsi, C.; Cimolin, V.; Capodaglio, P.; Condoluci, C.; Galli, M. A biomechanical study of gait initiation in Down syndrome. BMC Neurol. 2019, 19, 66. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, C.; Millwood, J. Toothbrush handle adaptation using silicone impression putty. Dent. Updat. 1999, 26, 288–289. [Google Scholar] [CrossRef] [PubMed]
- Singhvi, M.S.; Zinjarde, S.S.; Gokhale, D.V. Polylactic acid: Synthesis and biomedical applications. J. Appl. Microbiol. 2019, 127, 1612–1626. [Google Scholar] [CrossRef] [Green Version]
- Pasiga, B.D.; Dewi, C. The Effectiveness of the Use of “Special Grip Toothbrushes” on Dental Hygiene for Indonesian Patients with Ischemic Stroke. Pesqui. Bras. Odontopediatria Clín. Integr. 2019, 19, 1–10. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Criteria |
|---|---|
| 0 | No plaque present |
| 1 | Separate flecks of plaque at the cervical margin |
| 2 | A thin continuous back of plaque (up to 1 mm) at the cervical margin |
| 3 | A band of plaque wider than 1 mm but covering less than one-third of the side of the crown of the tooth |
| 4 | Plaque covering at least one-third but less than two-thirds of the side of crown of the tooth |
| 5 | Plaque covering two-thirds or more of the side of the crown of the tooth |
| Score | Criteria |
|---|---|
| 0 | Absence of inflammation |
| 1 | Mild inflammation or with slight changes in color and texture but not in all portions of gingival marginal or papillary |
| 2 | Mild inflammation, such as the preceding criteria, in all portions of gingival marginal or papillary |
| 3 | Moderate, bright surface inflammation, erythema, edema and/or hypertrophy of gingival marginal or papillary |
| 4 | Severe inflammation: erythema, edema and/or marginal gingival hypertrophy of the unit or spontaneous bleeding, papillary, congestion or ulceration |
| Time\Subgroups | SubA | SubB | SubC | SubD | p < 0.05 |
|---|---|---|---|---|---|
| T0 | 3.19 ± 0.5 a | 3.05 ± 0.18 c | 3.63 ± 0.29 b | 4.41 ± 0.25 d | a < b & c < d |
| T1 | 1.7 ± 0.68 a,e | 0.96 ± 0.29 b | 2.69 ± 0.45 c,f | 0.97 ± 0.35 d | a > b & c > d e < f |
| T2 | 1.41 ± 0.39 a,e | 0.38 ± 0.43 b,g | 2.23 ± 0.54 c,f | 0.52 ± 0.21 d,h | a > b & c > d e < f & g < h |
| T3 | 1.21 ± 0.47 a,e | 0.14 ± 0.27 b,g | 1.9 ± 0.58 c,f | 0.26 ± 0.1 d,h | a > b & c > d e < f & g < h |
| p < 0.05 | T0 > T1 T1 > T2 | T0 > T1 T1 > T2 T2 > T3 | T0 > T1 T1 > T2 T2 > T3 | T0 > T1 T1 > T2 T2 > T3 |
| Time\Subgroups | SubA | SubB | SubC | SubD | p < 0.05 |
|---|---|---|---|---|---|
| T0 | 1.4 ± 0.76 a | 1.12 ± 0.64 c | 2.95 ± 0.72 b | 2.91 ± 0.73 d | a < b & c < d |
| T2 | 0.8 ± 0.43 a,e | 0.41 ± 0.46 b,g | 1.95 ± 0.62 c,f | 1.41 ± 0.55 d,h | e < f & g < h |
| T3 | 0.54 ± 0.49 a,e | 0.83 ± 0.19 b,g | 1.54 ± 0.62 c,f | 0.75 ± 0.45 d,h | a > b & c > d e < f & g < h |
| p < 0.05 | T0 > T2 T2 > T3 | T0 > T2 T2 > T3 | T0 > T2 T2 > T3 | T0 > T2 T2 > T3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Droubi, L.; Laflouf, M.; Alkurdi, S.; Sauro, S.; Mancino, D.; Haikel, Y.; Kharouf, N. Does Customized Handle Toothbrush Influence Dental Plaque Removal in Children with Down Syndrome? A Randomized Controlled Trial. Healthcare 2021, 9, 1130. https://doi.org/10.3390/healthcare9091130
Droubi L, Laflouf M, Alkurdi S, Sauro S, Mancino D, Haikel Y, Kharouf N. Does Customized Handle Toothbrush Influence Dental Plaque Removal in Children with Down Syndrome? A Randomized Controlled Trial. Healthcare. 2021; 9(9):1130. https://doi.org/10.3390/healthcare9091130
Chicago/Turabian StyleDroubi, Line, Mohannad Laflouf, Saleh Alkurdi, Salvatore Sauro, Davide Mancino, Youssef Haikel, and Naji Kharouf. 2021. "Does Customized Handle Toothbrush Influence Dental Plaque Removal in Children with Down Syndrome? A Randomized Controlled Trial" Healthcare 9, no. 9: 1130. https://doi.org/10.3390/healthcare9091130