
Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME


Abstract
:1. Introduction
- A detailed analysis of the results obtained and comparison with the performance of the same models being applied to independent datasets of either CT scans or X-ray images;
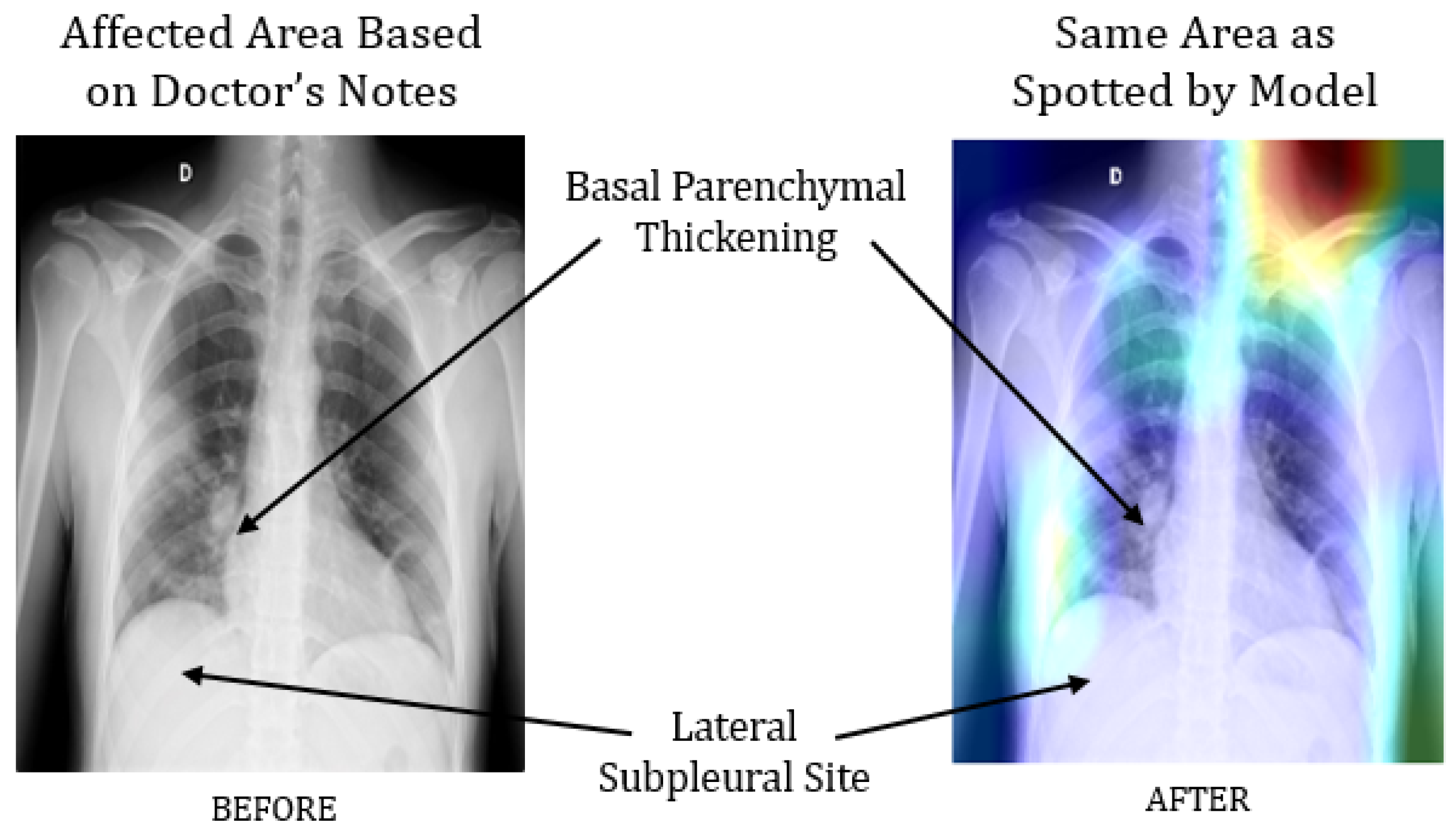
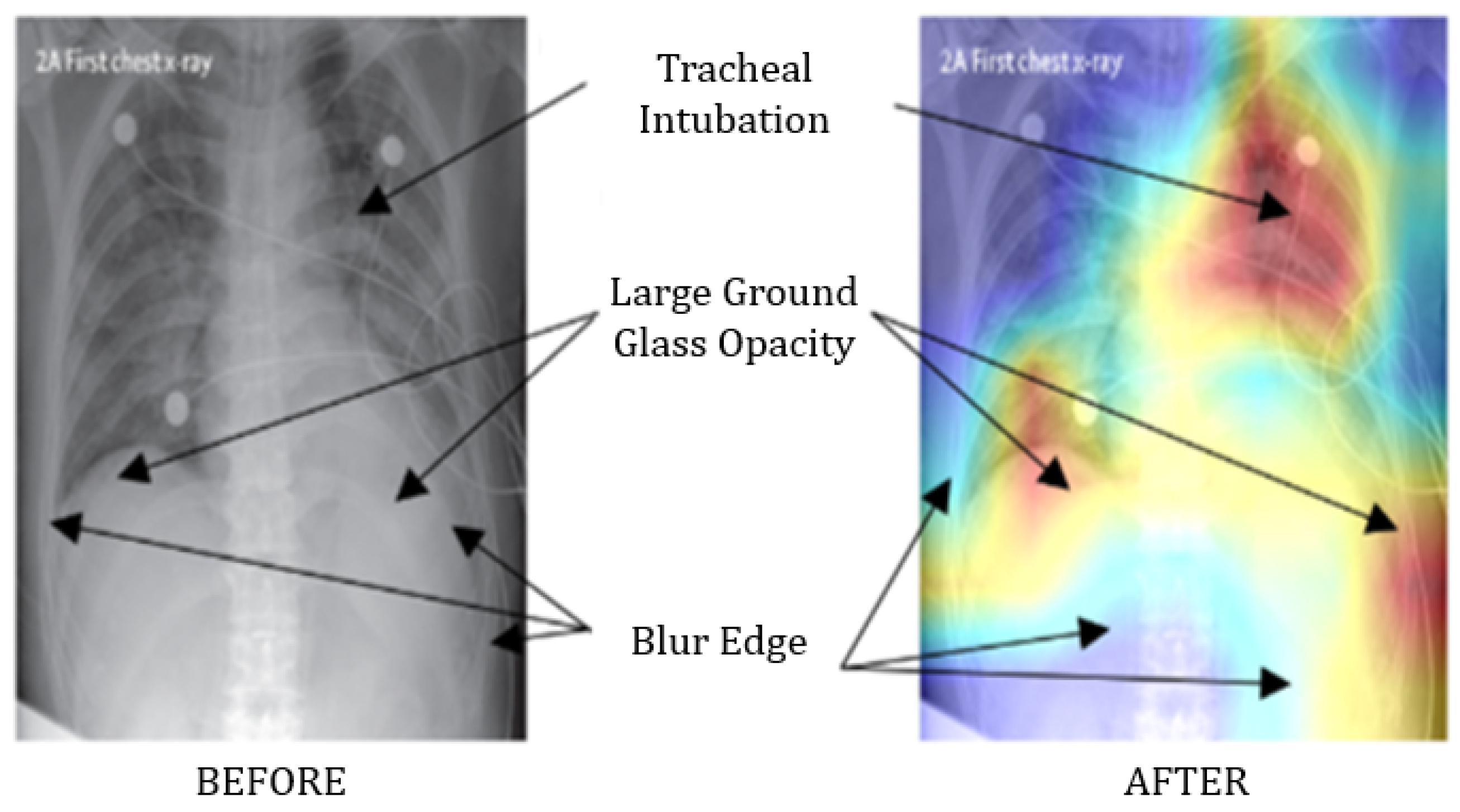
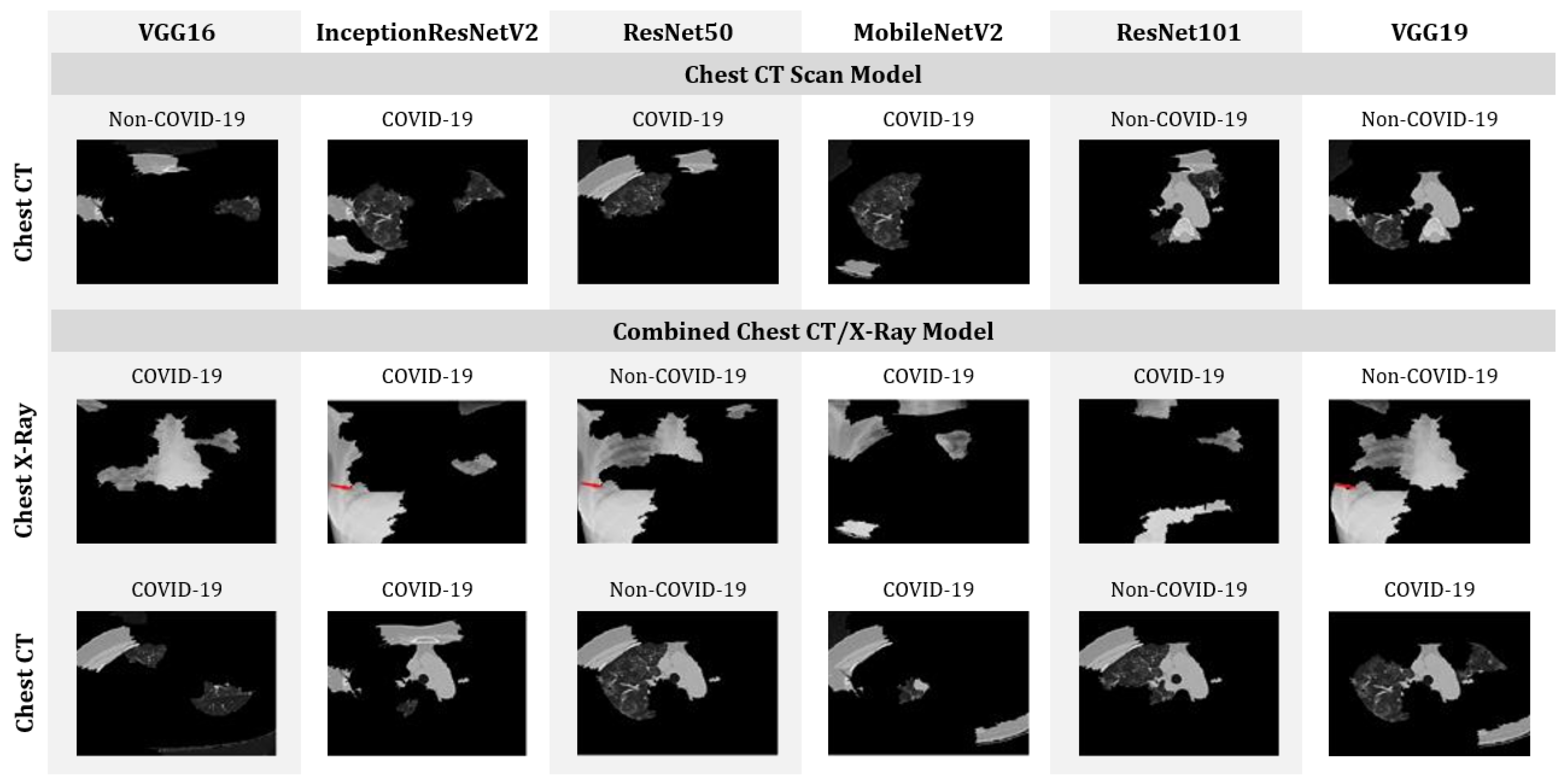
- Finally, we explain the models’ predictability considering top features with Local Interpretable Model-Agnostic Explanations (LIME).
2. Research Methodology
2.1. Using Pre-Trained Convolutional Networks
- Models are initiated with the pre-trained network without a fully connected (FC) layer;
- A new layer is added, containing “Maxpool” and “softmax” as activation functions and appended with the network’s primary architecture;
- The convolutional weights are kept frozen and only the new FC layers are trained with the new CNN architecture.
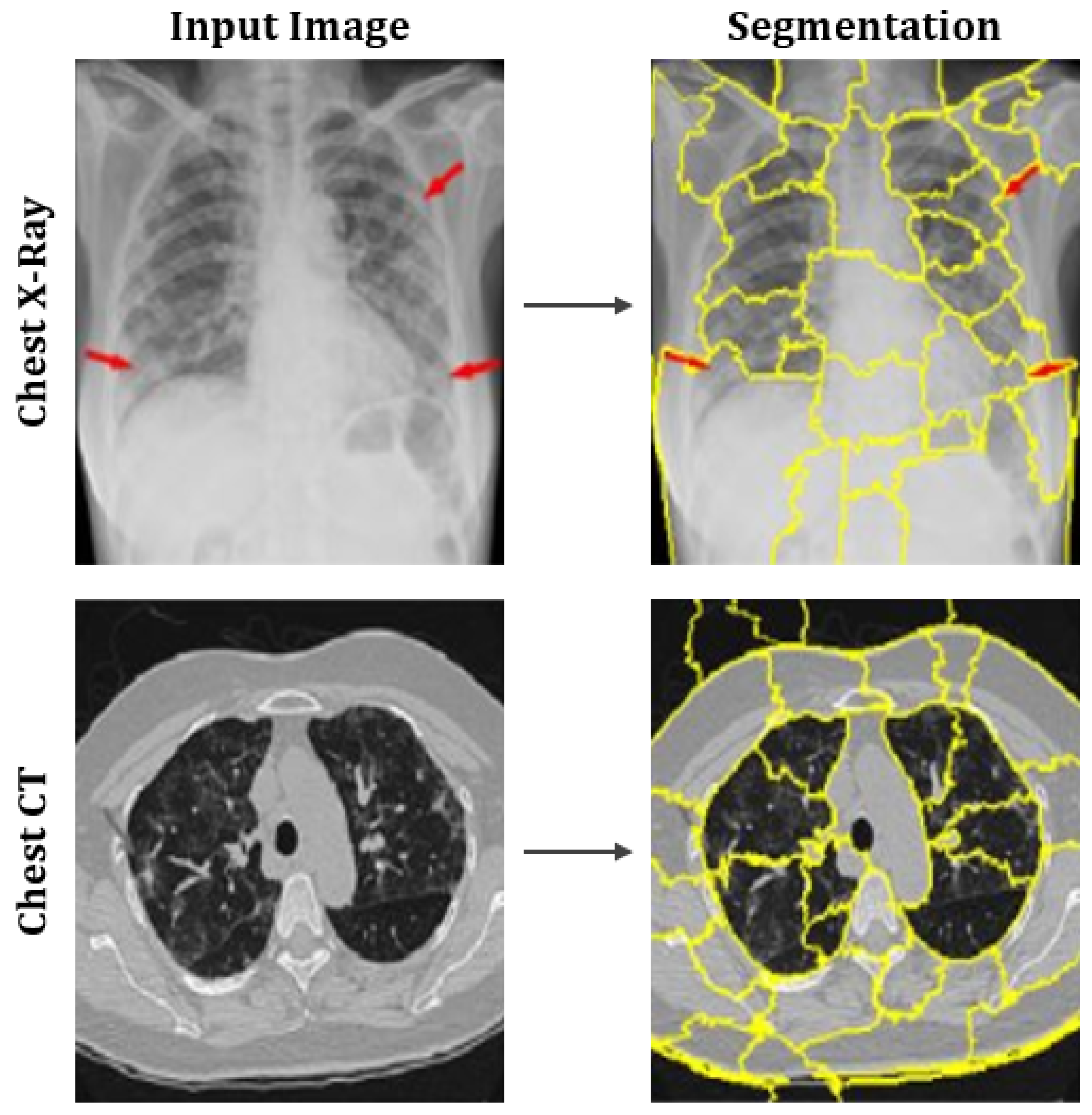
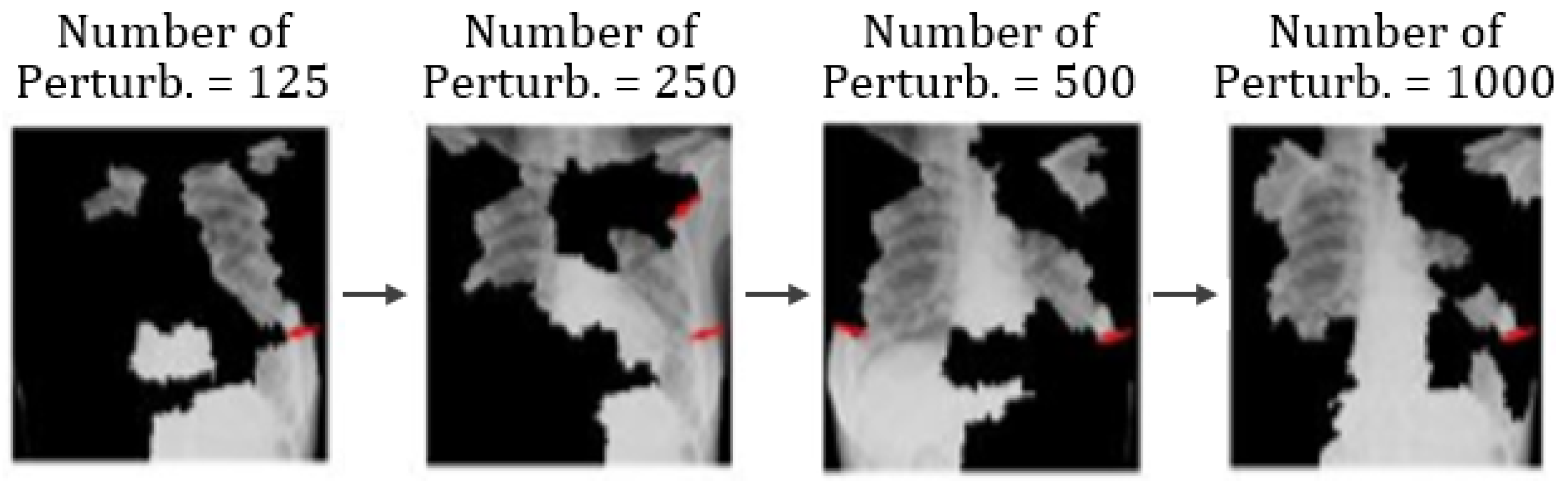
2.2. LIME as Explainable AI
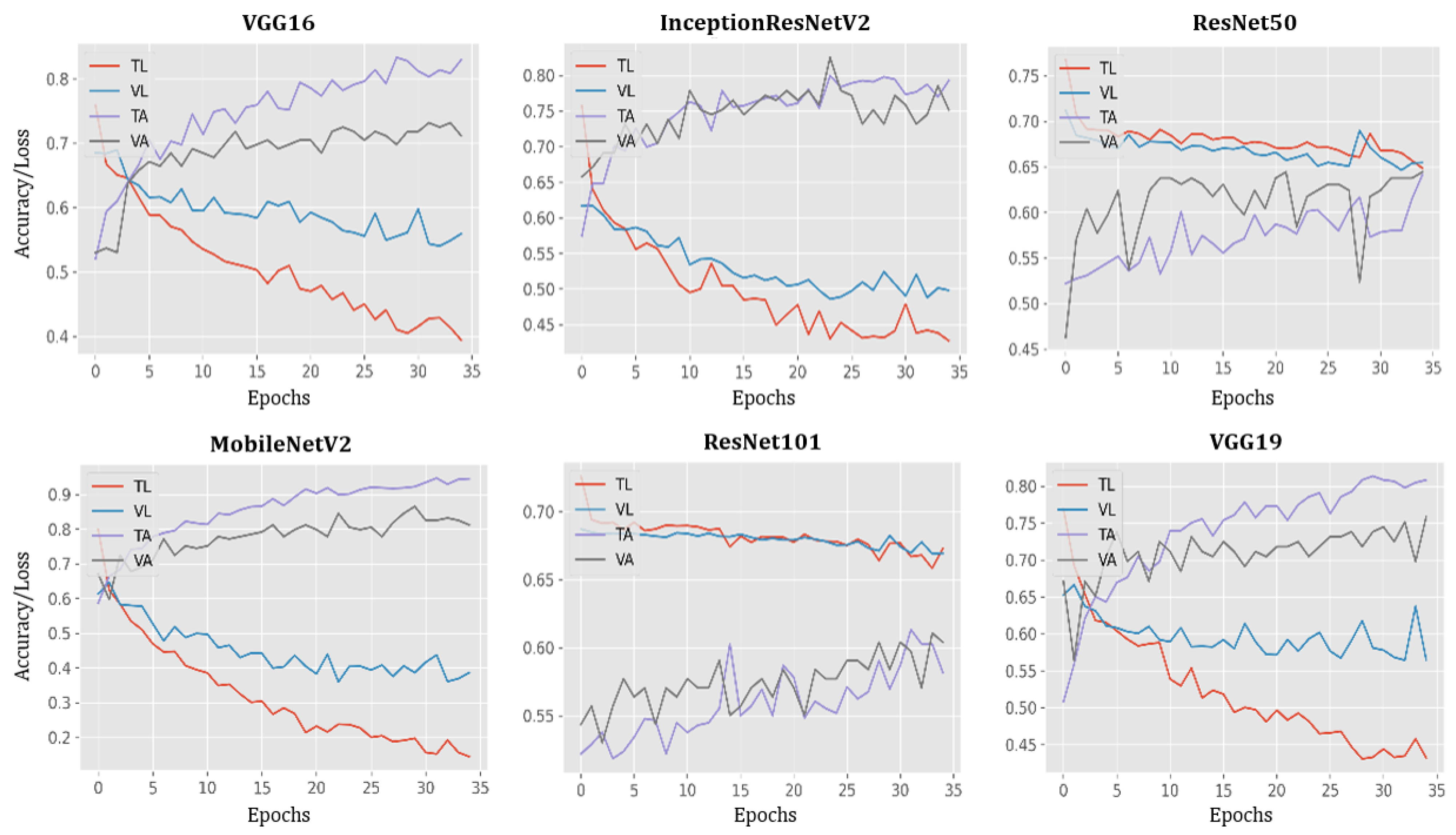
3. Results
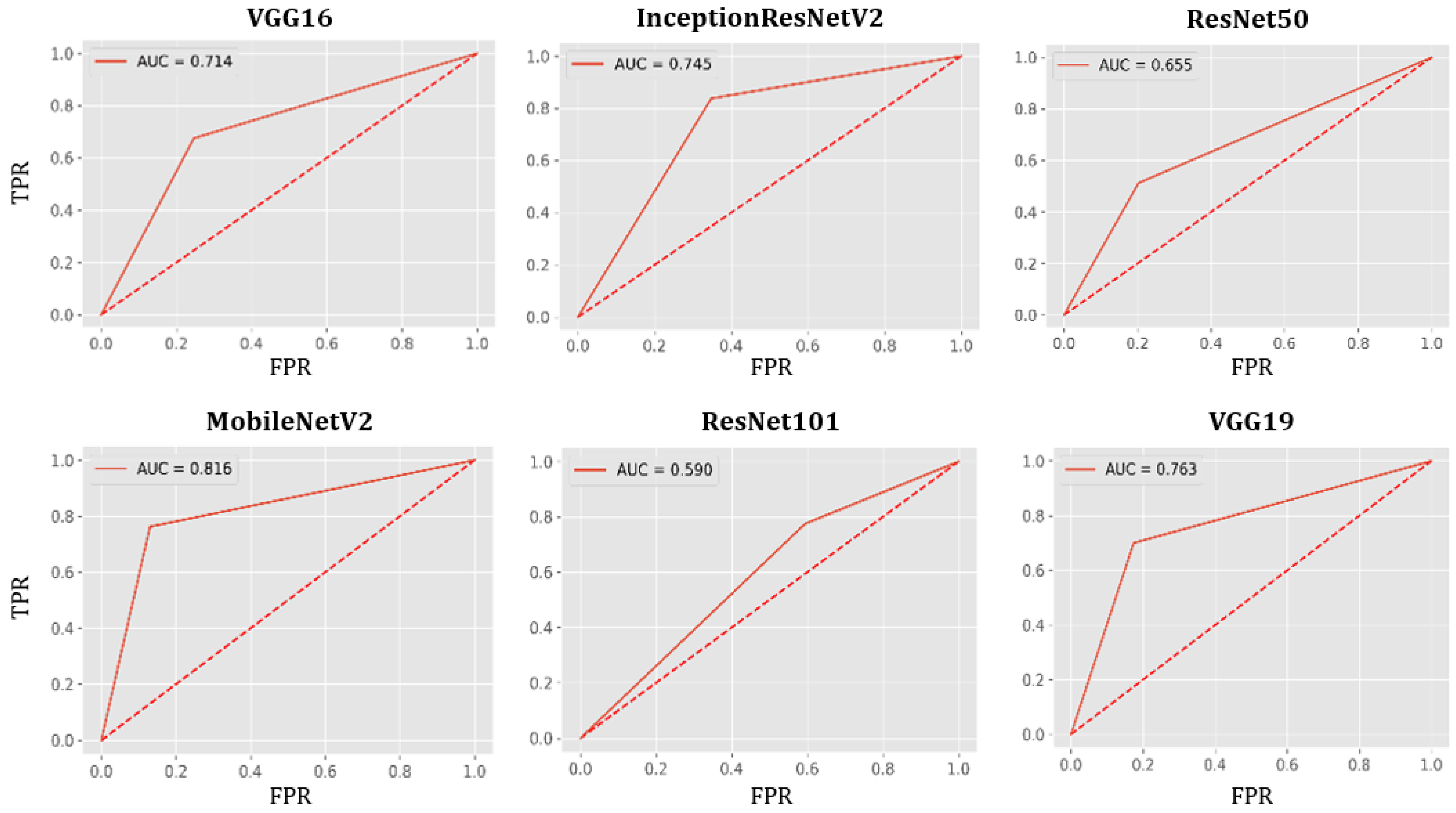
AUC-ROC Curve
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guardian, T. New US Mask Guidance Prompted by Evidence Vaccinated Can Spread Delta. August 2021. Available online: https://www.theguardian.com/world/2021/jul/28/cdc-director-new-mask-guidance-vaccinated-spreading-delta-variant (accessed on 3 August 2021).
- Dashbord. Covid-19 WorldMeter. June 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 August 2021).
- Haghanifar, A.; Majdabadi, M.M.; Ko, S. COVID-CXNet: Detecting COVID-19 in Frontal Chest X-ray Images using Deep Learning. arXiv 2020, arXiv:2006.13807. [Google Scholar]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, T. Handbook of COVID-19 Prevention and Treatment. First Affil. Hosp. Zhejiang Univ. Sch. Med. Compil. Accord. Clin. Exp. 2020, 68. Available online: https://www.alnap.org/help-library/handbook-of-covid-19-prevention-and-treatment (accessed on 15 February 2021).
- Chen, J.; Wu, L.; Zhang, J.; Zhang, L.; Gong, D.; Zhao, Y.; Hu, S.; Wang, Y.; Hu, X.; Zheng, B.; et al. Deep Learning-Based Model for Detecting 2019 Novel Coronavirus Pneumonia on High-Resolution Computed Tomography: A Prospective Study. Sci. Rep. 2020, 10, 1–11. [Google Scholar]
- Ardakani, A.A.; Kanafi, A.R.; Acharya, U.R.; Khadem, N.; Mohammadi, A. Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: Results of 10 convolutional neural networks. Comput. Biol. Med. 2020, 121, 103795. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Wang, X. Deep learning-based detection for COVID-19 from chest CT using weak label. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Wong, A. Covid-net: A Tailored Deep Convolutional Neural Network Design for Detection of Covid-19 Cases from Chest X-ray Images. arXiv 2020, arXiv:2003.09871. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological Findings of COVID-19 Associated with Acute Respiratory Distress Syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Hemdan, E.E.D.; Shouman, M.A.; Karar, M.E. Covidx-Net: A Framework of Deep Learning Classifiers to Diagnose Covid-19 in X-ray Images. arXiv 2020, arXiv:2003.11055. [Google Scholar]
- Sethy, P.K.; Behera, S.K. Detection of Coronavirus Disease (Covid-19) Based on Deep Features. Preprints 2020. [Google Scholar] [CrossRef]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic Detection of Coronavirus Disease (covid-19) Using X-ray Images and Deep Convolutional Neural Networks. arXiv 2020, arXiv:2003.10849. [Google Scholar]
- Ahsan, M.M.; Ahad, M.T.; Soma, F.A.; Paul, S.; Chowdhury, A.; Luna, S.A.; Yazdan, M.M.S.; Rahman, A.; Siddique, Z.; Huebner, P. Detecting SARS-CoV-2 from Chest X-ray using Artificial Intelligence. IEEE Access 2021, 9, 35501–35513. [Google Scholar] [CrossRef]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable Deep Learning for Pulmonary Disease and Coronavirus COVID-19 Detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef]
- Ghoshal, B.; Tucker, A. Estimating Uncertainty and Interpretability in Deep Learning for Coronavirus (COVID-19) Detection. arXiv 2020, arXiv:2003.10769. [Google Scholar]
- Apostolopoulos, I.D.; Mpesiana, T.A. Covid-19: Automatic Detection from X-ray Images Utilizing Transfer Learning with Convolutional Neural Networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef] [Green Version]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017; Volume 31. [Google Scholar]
- Akiba, T.; Suzuki, S.; Fukuda, K. Extremely large minibatch sgd: Training resnet-50 on imagenet in 15 minutes. arXiv 2017, arXiv:1711.04325. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L. MobileNetV2. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–22 June 2018; pp. 4510–4520. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Chest X-ray Images (Pneumonia). Available online: https://www.kaggle.com/paultimothymooney/chest-xray-pneumonia (accessed on 16 December 2020).
- Chollet, F. Deep Learning with Python; Simon and Schuster: New York, NY, USA, 2017. [Google Scholar]
- Smith, L.N. A disciplined approach to neural network hyper-parameters: Part 1–learning rate, batch size, momentum, and weight decay. arXiv 2018, arXiv:1803.09820. [Google Scholar]
- Smith, S.L.; Kindermans, P.J.; Ying, C.; Le, Q.V. Don’t decay the learning rate, increase the batch size. arXiv 2017, arXiv:1711.00489. [Google Scholar]
- Bergstra, J.; Bengio, Y. Random search for hyper-parameter optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Perez, L.; Wang, J. The effectiveness of data augmentation in image classification using deep learning. arXiv 2017, arXiv:1712.04621. [Google Scholar]
- Filipczuk, P.; Fevens, T.; Krzyżak, A.; Monczak, R. Computer-aided breast cancer diagnosis based on the analysis of cytological images of fine needle biopsies. IEEE Trans. Med. Imaging 2013, 32, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, M.M. Real Time Face Recognition in Unconstrained Environment; Lamar University: Beaumont, TX, USA, 2018. [Google Scholar]
- Molnar, C. Interpretable Machine Learning; Leanpub: Victoria, BC, Canada, 2020. [Google Scholar]
- Moore, A.P.; Prince, S.J.; Warrell, J.; Mohammed, U.; Jones, G. Superpixel lattices. In Proceedings of the 2008 IEEE Conference on Computer Vision and Pattern Recognition, Anchorage, AK, USA, 23–28 June 2008; pp. 1–8. [Google Scholar]
- Khan, A.I.; Shah, J.L.; Bhat, M.M. Coronet: A Deep Neural Network for Detection and Diagnosis of COVID-19 from Chest X-ray Images. Comput. Methods Programs Biomed. 2020, 196, 105581. [Google Scholar] [CrossRef]
- Li, L.; Qin, L.; Xu, Z.; Yin, Y.; Wang, X.; Kong, B.; Bai, J.; Lu, Y.; Fang, Z.; Song, Q.; et al. Artificial intelligence distinguishes COVID-19 from community acquired pneumonia on chest CT. Radiology 2020. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Kang, B.; Ma, J.; Zeng, X.; Xiao, M.; Guo, J.; Cai, M.; Yang, J.; Li, Y.; Meng, X.; et al. A deep learning algorithm using CT images to screen for Corona Virus Disease (COVID-19). Eur. Radiol. 2021, 31, 6096–6104. [Google Scholar] [CrossRef]
- Jin, C.; Chen, W.; Cao, Y.; Xu, Z.; Zhang, X.; Deng, L.; Zheng, C.; Zhou, J.; Shi, H.; Feng, J. Development and Evaluation of an AI System for COVID-19 Diagnosis. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Xie, Y.; Li, Y.; Shen, C.; Xia, Y. Covid-19 Screening on Chest X-ray Images Using Deep Learning Based Anomaly Detection. arXiv 2020, arXiv:2003.12338. [Google Scholar]
- Song, Y.; Zheng, S.; Li, L.; Zhang, X.; Zhang, X.; Huang, Z.; Chen, J.; Zhao, H.; Jie, Y.; Wang, R.; et al. Deep Learning Enables Accurate Diagnosis of Novel Coronavirus (COVID-19) with CT Images. MedRxiv 2020. [Google Scholar] [CrossRef]
- Orujov, F.; Maskeliūnas, R.; Damaševičius, R.; Wei, W. Fuzzy based image edge detection algorithm for blood vessel detection in retinal images. Appl. Soft Comput. 2020, 94, 106452. [Google Scholar] [CrossRef]
- Versaci, M.; Morabito, F.C. Image edge detection: A new approach based on fuzzy entropy and fuzzy divergence. Int. J. Fuzzy Syst. 2021, 23, 918–936. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Label | Train | Test | ||||
|---|---|---|---|---|---|---|---|
| Chest X-ray | CT scan | Total | Chest X-ray | CT scan | Total | ||
| Mixed Data | COVID-19 | 486 | 160 | 646 | 122 | 40 | 162 |
| Non-COVID-19 | 1266 | 160 | 1426 | 317 | 40 | 357 | |
| Total | 1752 | 320 | 2072 | 439 | 80 | 519 | |
| Function | Value |
|---|---|
| Kernel size | 200 |
| Maximum distance | 200 |
| Ratio | 0.2 |
| Algorithm | Accuracy (%) | Precision (%) | Recall (%) | F-1 Score (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T | T | CI | T | T | CI | T | T | CI | T | T | CI | |
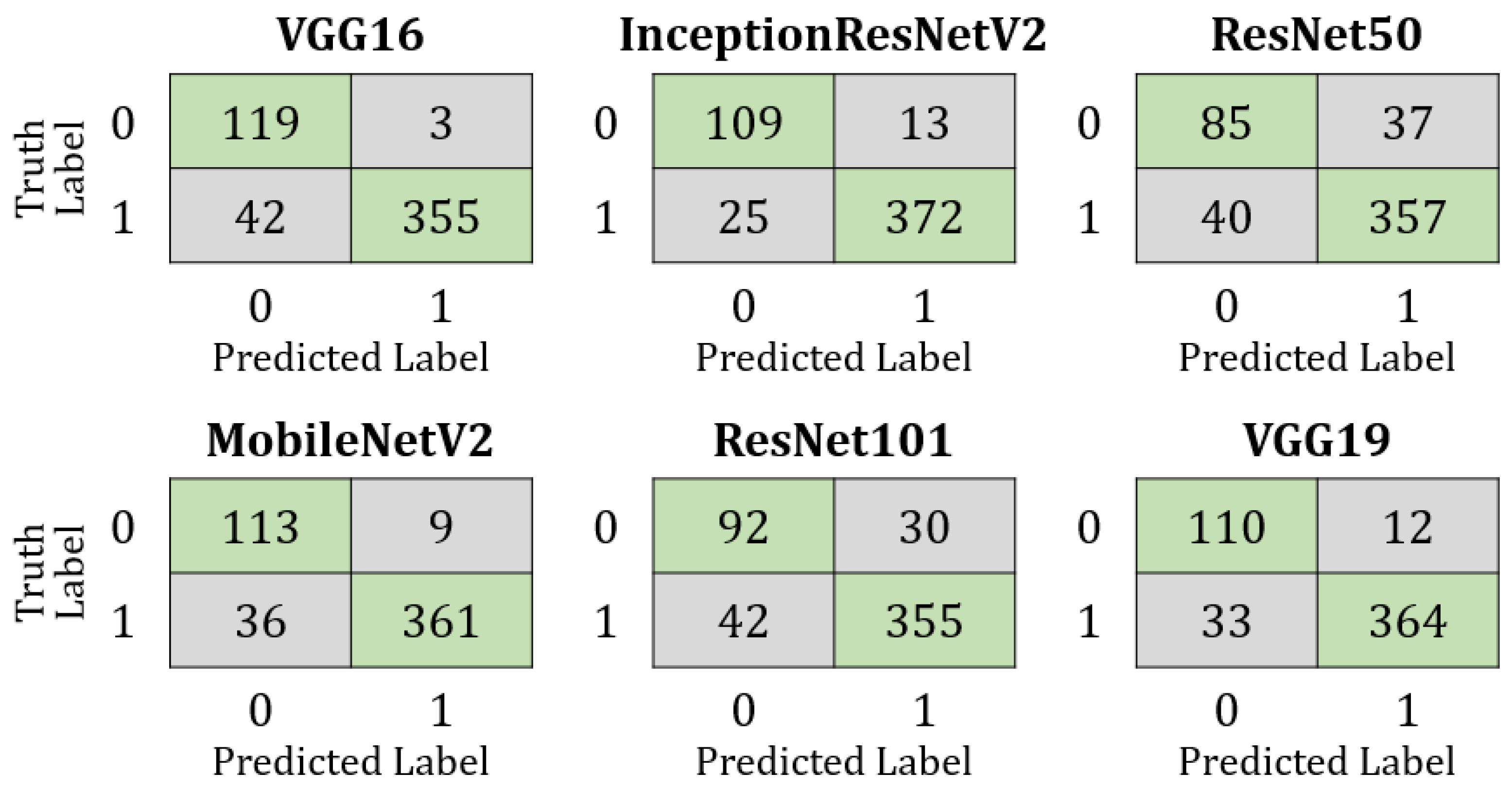
| VGG16 | 95 | 91 | 93 ± 1.4 | 95 | 93 | 94 ± 1.3 | 95 | 91 | 93 ± 1.4 | 95 | 92 | 93.5 ± 1.34 |
| InceptionResNetV2 | 94 | 93 | 93.5 ± 1.34 | 95 | 93 | 94 ± 1.3 | 94 | 93 | 93.5 ± 1.34 | 94 | 93 | 93.5 ± 1.35 |
| ResNet50 | 88 | 85 | 86.5 ± 1.86 | 87 | 85 | 86 ± 1.89 | 88 | 85 | 86.5 ± 1.86 | 87 | 85 | 86 ± 1.89 |
| MobileNetV2 | 99 | 91 | 95 ± 1.2 | 99 | 92 | 95.5 ± 1.13 | 99 | 91 | 95 ± 1.2 | 99 | 91 | 95 ± 1.2 |
| ResNet101 | 88 | 86 | 87 ± 1.83 | 88 | 87 | 87.5 ± 1.80 | 88 | 86 | 87 ± 1.83 | 88 | 86 | 87 ± 1.83 |
| VGG19 | 94 | 91 | 92.5 ± 1.43 | 94 | 92 | 93 ± 1.4 | 94 | 91 | 92.5 ± 1.43 | 94 | 92 | 93 ± 1.4 |
| Dataset | Datasize | Model | Accuracy (%) |
|---|---|---|---|
| X-ray | 400 | VGG16 | 98.5 ± 1.191 |
| MobileNetV2 | 98.5 ± 1.191 | ||
| CT-Scan | 400 | MobileNetV2 | 94 ± 2.327 |
| Mixed-data | 2591 | MobileNetV2 | 95 ± 1.12 |
| Reference | Model | Dataset Size | Accuracy |
|---|---|---|---|
| Li et al. (2020) [34] | ResNet50 | 4356 | 90% |
| Wang et al. (2021) [35] | Inception-M | 1065 | 74% |
| Zhang et al. (2020) [37] | ResNet50 | 1531 | 90% |
| Song et al. (2020) [38] | ResNet50 | 274 | 86% |
| Chen et al. (2020) [6] | UNet | 133 | 98.5% |
| Jin et al. (2020) [36] | CNN | 1882 | 94.1% |
| This study | MobileNetV2 | 400 | 98.5% ± 1.19% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahsan, M.M.; Nazim, R.; Siddique, Z.; Huebner, P. Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME. Healthcare 2021, 9, 1099. https://doi.org/10.3390/healthcare9091099
Ahsan MM, Nazim R, Siddique Z, Huebner P. Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME. Healthcare. 2021; 9(9):1099. https://doi.org/10.3390/healthcare9091099
Chicago/Turabian StyleAhsan, Md Manjurul, Redwan Nazim, Zahed Siddique, and Pedro Huebner. 2021. "Detection of COVID-19 Patients from CT Scan and Chest X-ray Data Using Modified MobileNetV2 and LIME" Healthcare 9, no. 9: 1099. https://doi.org/10.3390/healthcare9091099