
Patterns of Cone-Beam Computed Tomography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection
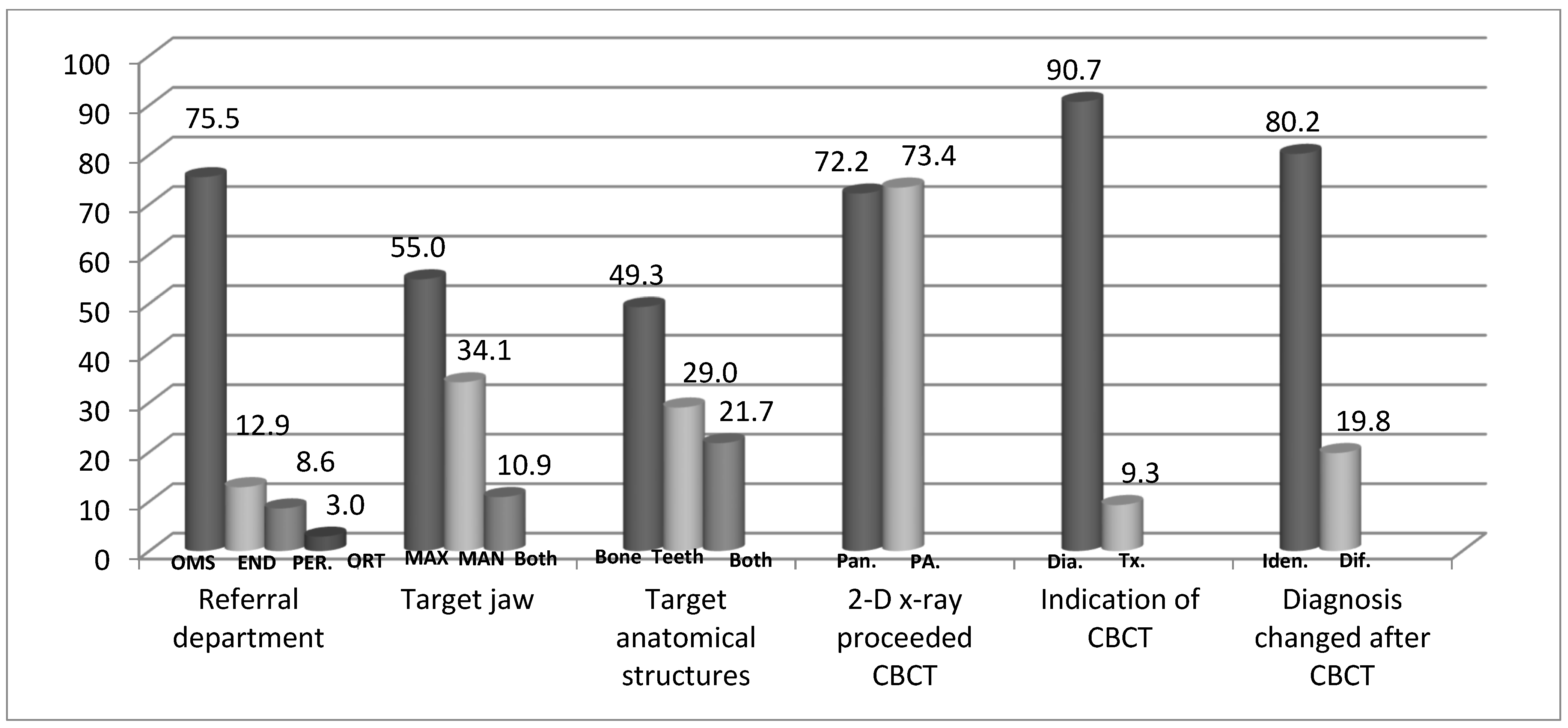
- Demographics: age (years), sex (men/women).
- Referring department: Oral and Maxillofacial Surgery/Orthodontics/Endodontics/Periodontology.
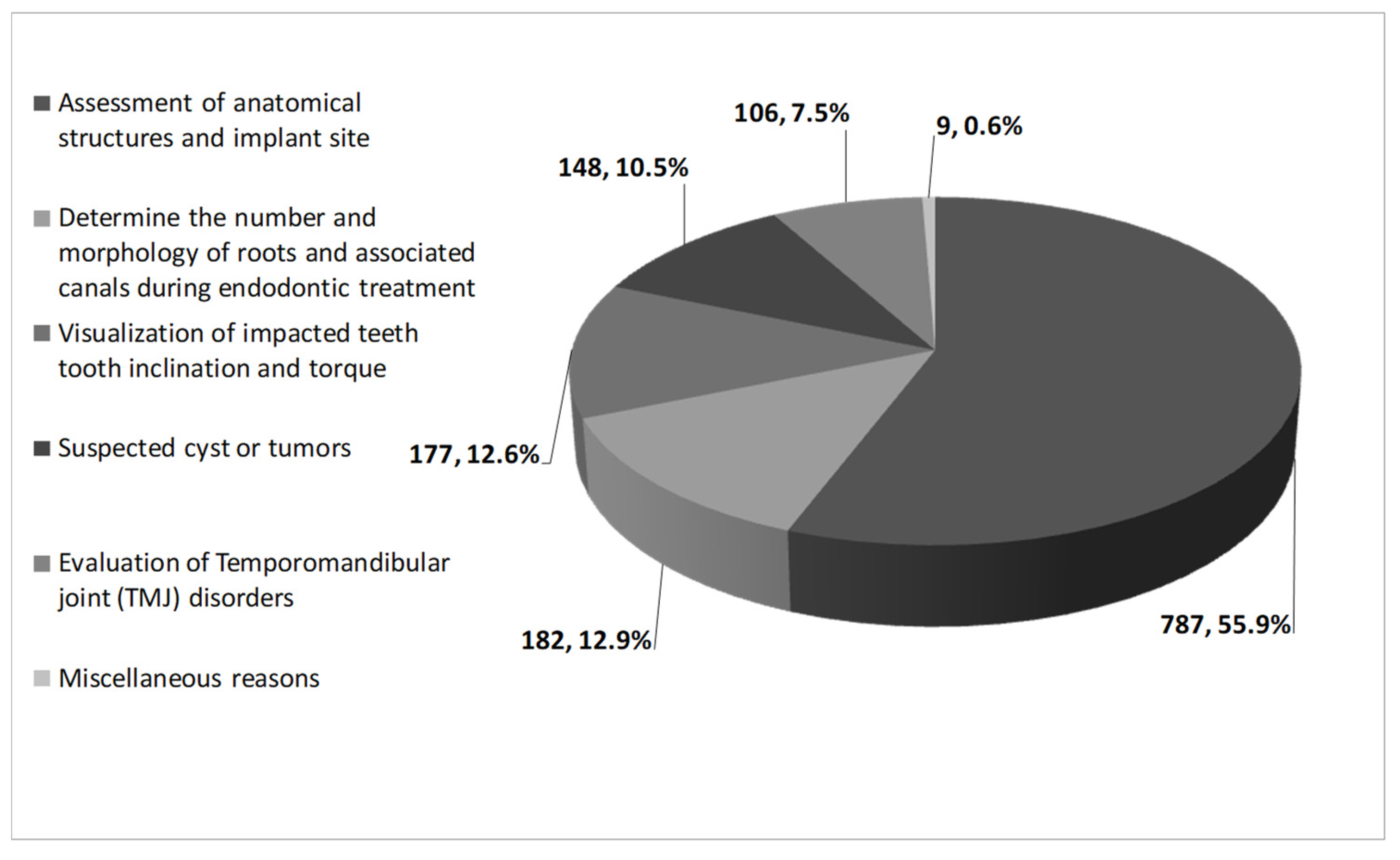
- The indication for referring the patient for CBCT as recorded in the medical file.
- Target jaw evaluated: Maxilla/Mandible/both jaws.
- Anatomical structures evaluated: teeth/bone/teeth and bone.
- Did panoramic X-ray precede the CBCT? yes/no.
- Did periapical X-ray precede the CBCT? yes/no.
- The indications for patient referral for the CBCT: for diagnosis/for treatment planning.
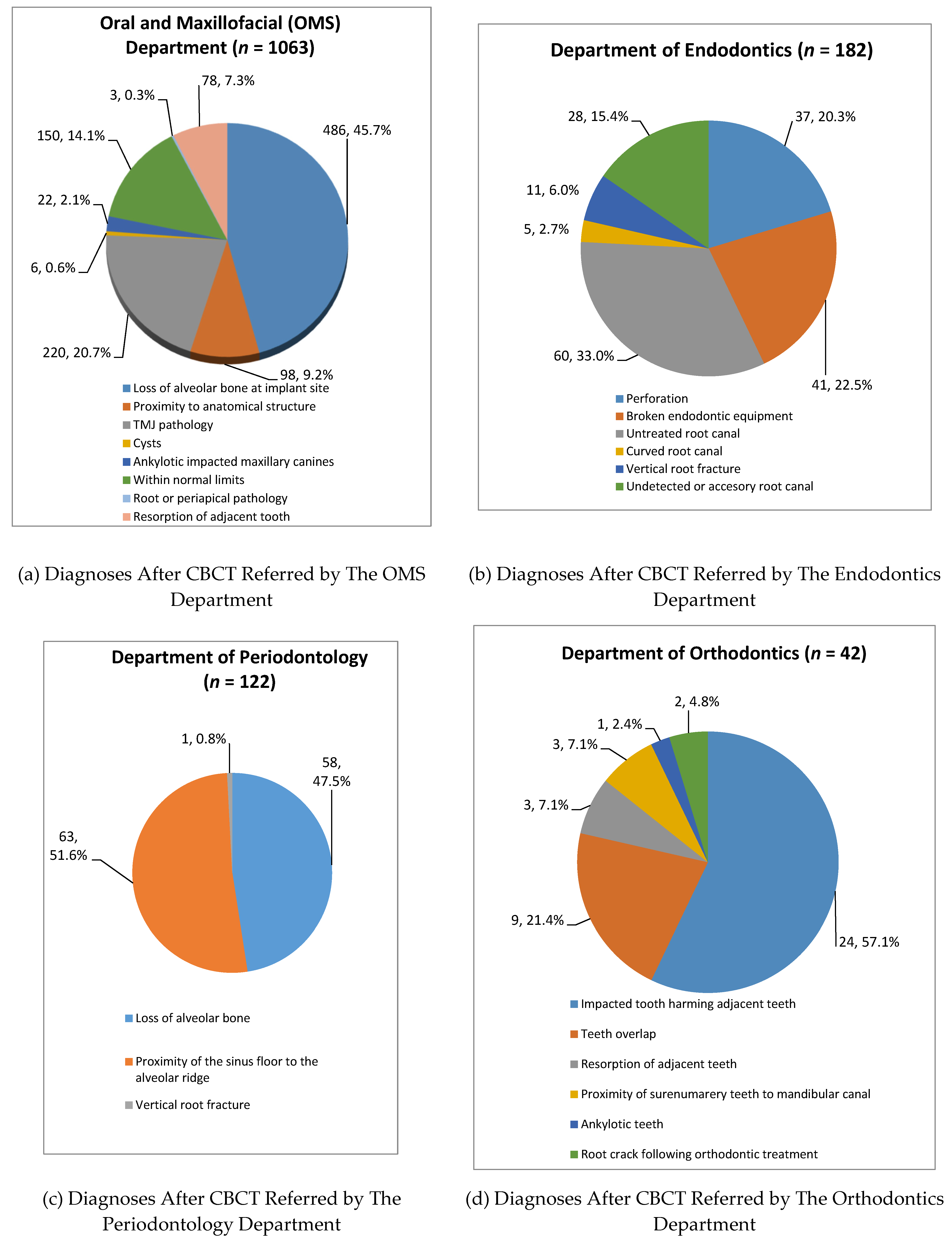
- Final diagnosis: as recorded in the medical file.
- Did the interpretation of the CBCT change the diagnosis and/or treatment plan which was given prior to referral? yes/no.
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. The Impact of CBCT on The Diagnostic Process
4.2. Targeted Jaw and Anatomical Structure in CBCT
4.3. Final Diagnoses: Oral and Maxillofacial Surgery Department
4.4. Department of Endodontics
4.5. Department of Periodontology
4.6. Department of Orthodontics
4.7. Strength and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Rushton, V.E.; Horner, K. The use of panoramic radiology in dental practice. J. Dent. 1996, 24, 185–201. [Google Scholar] [CrossRef]
- Sedaghatfar, M.; August, M.A.; Dodson, T.B. Panoramic radiographic findings as predictors of inferior alveolar nerve exposure following third molar extraction. J. Oral Maxillofac. Surg. 2005, 63, 3–7. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, R.; Quirynen, M. Dental cone beam computed tomography: Justification for use in planning oral implant placement. Periodontol. 2000 2014, 66, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 112–123. [Google Scholar] [CrossRef]
- Dula, K.; Benic, G.I.; Bornstein, M.; Dagassan-Berndt, D.; Filippi, A.; Hicklin, S.; Kissling-Jeger, F.; Luebbers, H.T.; Sculean, A.; Sequeira-Byron, P.; et al. SADMFR Guidelines for the Use of Cone-Beam Computed Tomography/Digital Volume Tomography. Swiss Dent. J. 2015, 125, 945–953. [Google Scholar] [PubMed]
- Brown, J.; Jacobs, R.; Levring Jaghagen, E.; Lindh, C.; Baksi, G.; Schulze, D.; Schulze, R. Basic training requirements for the use of dental CBCT by dentists: A position paper prepared by the European Academy of DentoMaxilloFacial Radiology. Dentomaxillofac. Radiol. 2014, 43, 20130291. [Google Scholar] [CrossRef] [Green Version]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.A. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef]
- Arai, Y.; Tammisalo, E.; Iwai, K.; Hashimoto, K.; Shinoda, K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac. Radiol. 1999, 28, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Terakado, M.; Hashimoto, K.; Arai, Y.; Honda, M.; Sekiwa, T.; Sato, H. Diagnostic imaging with newly developed ortho cubic super-high resolution computed tomography (Ortho-CT). Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 509–518. [Google Scholar] [CrossRef]
- Ganz, S.D. Three-dimensional imaging and guided surgery for dental implants. Dent. Clin. N. Am. 2015, 59, 265–290. [Google Scholar] [CrossRef] [PubMed]
- Flugge, T.V.; Nelson, K.; Schmelzeisen, R.; Metzger, M.C. Three-dimensional plotting and printing of an implant drilling guide: Simplifying guided implant surgery. J. Oral Maxillofac. Surg. 2013, 71, 1340–1346. [Google Scholar] [CrossRef]
- Cassetta, M.; Stefanelli, L.V.; Di Carlo, S.; Pompa, G.; Barbato, E. The accuracy of CBCT in measuring jaws bone density. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1425–1429. [Google Scholar]
- Cassetta, M.; Stefanelli, L.V.; Pacifici, A.; Pacifici, L.; Barbato, E. How accurate is CBCT in measuring bone density? A comparative CBCT-CT in vitro study. Clin. Implant. Dent. Relat. Res. 2014, 16, 471–478. [Google Scholar] [CrossRef]
- Jacobs, R. Dental cone beam CT and its justified use in oral health care. JBR-BTR 2011, 94, 254–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuigan, M.B.; Duncan, H.F.; Horner, K. An analysis of effective dose optimization and its impact on image quality and diagnostic efficacy relating to dental cone beam computed tomography (CBCT). Swiss Dent. J. 2018, 128, 297–316. [Google Scholar] [PubMed]
- Radic, J.; Patcas, R.; Stadlinger, B.; Wiedemeier, D.; Rucker, M.; Giacomelli-Hiestand, B. Do we need CBCTs for sufficient diagnostics?-dentist-related factors. Int. J. Implant. Dent. 2018, 4, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, R., 2nd; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaeta-Araujo, H.; Leite, A.F.; Vasconcelos, K.F.; Jacobs, R. Two decades of research on CBCT imaging in DMFR—An appraisal of scientific evidence. Dentomaxillofac. Radiol. 2021, 50, 20200367. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Vranckx, M.; Vanderstuyft, T.; Quirynen, M.; Salmon, B. CBCT vs. other imaging modalities to assess peri-implant bone and diagnose complications: A systematic review. Eur. J. Oral Implantol. 2018, 11 (Suppl. 1), 77–92. [Google Scholar]
- Scarfe, W.C.; Toghyani, S.; Azevedo, B. Imaging of Benign Odontogenic Lesions. Radiol. Clin. N. Am. 2018, 56, 45–62. [Google Scholar] [CrossRef]
- Theodorakou, C.; Walker, A.; Horner, K.; Pauwels, R.; Bogaerts, R.; Jacobs, R. Estimation of paediatric organ and effective doses from dental cone beam CT using anthropomorphic phantoms. Br. J. Radiol. 2012, 85, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Dave, M.; Coulthard, P.; Patel, N.; Seoudi, N.; Horner, K. Letter to the Editor: Use of Dental Radiography in the COVID-19 Pandemic. J. Dent. Res. 2020, 99, 1112. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.; Polizzi, E.; Tete, G.; Cappare, P. Dentistry and Covid-19 pandemic: Operative indications post-lockdown. New Microbiol. 2021, 44, 1–11. [Google Scholar] [PubMed]
- Barba, L.; Berrocal, A.L.; Hidalgo, A. Uses of cone-beam computed tomography in San Jose, Costa Rica. Imaging Sci. Dent. 2018, 48, 103–109. [Google Scholar] [CrossRef]
- Mandelaris, G.A.; Scheyer, E.T.; Evans, M.; Kim, D.; McAllister, B.; Nevins, M.L.; Rios, H.F.; Sarment, D. American Academy of Periodontology Best Evidence Consensus Statement on Selected Oral Applications for Cone-Beam Computed Tomography. J. Periodontol. 2017, 88, 939–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woelber, J.P.; Fleiner, J.; Rau, J.; Ratka-Kruger, P.; Hannig, C. Accuracy and Usefulness of CBCT in Periodontology: A Systematic Review of the Literature. Int. J. Periodontics Restor. Dent. 2018, 38, 289–297. [Google Scholar] [CrossRef] [Green Version]
- Walter, C.; Schmidt, J.C.; Dula, K.; Sculean, A. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: A systematic review. Quintessence Int. 2016, 47, 25–37. [Google Scholar] [CrossRef]
- Walter, C.; Schmidt, J.C.; Rinne, C.A.; Mendes, S.; Dula, K.; Sculean, A. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: Systematic review update. Clin. Oral Investig. 2020, 24, 2943–2958. [Google Scholar] [CrossRef]
- Liu, D.G.; Zhang, W.L.; Zhang, Z.Y.; Wu, Y.T.; Ma, X.C. Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 105, 91–98. [Google Scholar] [CrossRef]
- Harris, D.; Horner, K.; Grondahl, K.; Jacobs, R.; Helmrot, E.; Benic, G.I.; Bornstein, M.M.; Dawood, A.; Quirynen, M.E.A.O. guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. Clin. Oral Implant. Res. 2012, 23, 1243–1253. [Google Scholar] [CrossRef]
- Tyndall, D.A.; Price, J.B.; Tetradis, S.; Ganz, S.D.; Hildebolt, C.; Scarfe, W.C. Position statement of the American Academy of Oral and Maxillofacial Radiology on selection criteria for the use of radiology in dental implantology with emphasis on cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 817–826. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Scarfe, W.C.; Vaughn, V.M.; Jacobs, R. Cone beam computed tomography in implant dentistry: A systematic review focusing on guidelines, indications, and radiation dose risks. Int. J. Oral Maxillofac. Implant. 2014, 29, 55–77. [Google Scholar] [CrossRef]
- Dagassan-Berndt, D.C.; Clemens, W.; Zitzmann, N.U.; Schulze, R.K. Influence of Three-dimensional Imaging on Implant Treatment Planning: Implant Diameter and Length. J. Contemp. Dent. Pract. 2018, 19, 704–711. [Google Scholar] [CrossRef]
- Lo Giudice, R.; Nicita, F.; Puleio, F.; Alibrandi, A.; Cervino, G.; Lizio, A.S.; Pantaleo, G. Accuracy of Periapical Radiography and CBCT in Endodontic Evaluation. Int. J. Dent. 2018, 2018, 2514243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fayad, M.I.; Nair, M.; Levin, M.D.; Benavides, E.; Rubinstein, R.A.; Barghan, S.; Hirschberg, C.S.; Ruprecht, A. AAE and AAOMR Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 508–512. [Google Scholar] [CrossRef]
- Patel, S.; Brown, J.; Semper, M.; Abella, F.; Mannocci, F. European Society of Endodontology position statement: Use of cone beam computed tomography in Endodontics: European Society of Endodontology (ESE) developed by. Int. Endod. J. 2019, 52, 1675–1678. [Google Scholar] [CrossRef] [Green Version]
- Ee, J.; Fayad, M.I.; Johnson, B.R. Comparison of endodontic diagnosis and treatment planning decisions using cone-beam volumetric tomography versus periapical radiography. J. Endod. 2014, 40, 910–916. [Google Scholar] [CrossRef] [PubMed]
- Mota de Almeida, F.J.; Knutsson, K.; Flygare, L. The impact of cone beam computed tomography on the choice of endodontic diagnosis. Int. Endod. J. 2015, 48, 564–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez, G.; Patel, S.; Duran-Sindreu, F.; Roig, M.; Abella, F. Influence of Cone-beam Computed Tomography on Endodontic Retreatment Strategies among General Dental Practitioners and Endodontists. J. Endod. 2017, 43, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Patel, S.; Foschi, F.; Andiappan, M.; Mitchell, P.J.; Mannocci, F. The detection of periapical pathoses using digital periapical radiography and cone beam computed tomography in endodontically retreated teeth—Part 2: A 1 year post-treatment follow-up. Int. Endod. J. 2016, 49, 623–635. [Google Scholar] [CrossRef]
- Venskutonis, T.; Plotino, G.; Juodzbalys, G.; Mickeviciene, L. The importance of cone-beam computed tomography in the management of endodontic problems: A review of the literature. J. Endod. 2014, 40, 1895–1901. [Google Scholar] [CrossRef]
- American Association of Endodontics (American Association of Endodontists/American Academy of Oral and Maxillofacial Radiology)) and American Academy of Oral and Maxillofacial Radiology (AAOMR) Joint Position Statement: Use of Cone Beam Computed Tomography in Endodontics 2015 Update. J. Endod. 2015, 41, 1393–1396.
- Du Bois, A.H.; Kardachi, B.; Bartold, P.M. Is there a role for the use of volumetric cone beam computed tomography in periodontics? Aust. Dent. J. 2012, 57 (Suppl. 1), 103–108. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Singh, A.; Gundappa, M. Three-dimensional imaging in periodontal diagnosis—Utilization of cone beam computed tomography. J. Indian Soc. Periodontol. 2011, 15, 11–17. [Google Scholar] [PubMed]
- De Faria Vasconcelos, K.; Evangelista, K.M.; Rodrigues, C.D.; Estrela, C.; de Sousa, T.O.; Silva, M.A. Detection of periodontal bone loss using cone beam CT and intraoral radiography. Dentomaxillofac. Radiol. 2012, 41, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Haney, E.; Gansky, S.A.; Lee, J.S.; Johnson, E.; Maki, K.; Miller, A.J.; Huang, J.C. Comparative analysis of traditional radiographs and cone-beam computed tomography volumetric images in the diagnosis and treatment planning of maxillary impacted canines. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, S.; Verna, C.; Cattaneo, P.M.; Heidmann, J.; Melsen, B. Two- versus three-dimensional imaging in subjects with unerupted maxillary canines. Eur. J. Orthod. 2011, 33, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Katheria, B.C.; Kau, C.H.; Tate, R.; Chen, J.W.; English, J.; Bouquot, J. Effectiveness of impacted and supernumerary tooth diagnosis from traditional radiography versus cone beam computed tomography. Pediatr. Dent. 2010, 32, 304–309. [Google Scholar]
- Kapila, S.D.; Nervina, J.M. CBCT in orthodontics: Assessment of treatment outcomes and indications for its use. Dentomaxillofac. Radiol. 2015, 44, 20140282. [Google Scholar] [CrossRef] [Green Version]
- Scarfe, W.C.; Azevedo, B.; Toghyani, S.; Farman, A.G. Cone Beam Computed Tomographic imaging in orthodontics. Aust. Dent. J. 2017, 62 (Suppl. 1), 33–50. [Google Scholar] [CrossRef] [Green Version]
- Schulze, R.K.W.; Drage, N.A. Cone-beam computed tomography and its applications in dental and maxillofacial radiology. Clin. Radiol. 2020, 75, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Dao-Ngoc, L.; Du, Y.C. Generative Noise Reduction in Dental Cone-Beam CT by a Selective Anatomy Analytic Iteration Reconstruction Algorithm. Electronics 2019, 8, 1381. [Google Scholar] [CrossRef] [Green Version]
- Niebler, S.; Schomer, E.; Tjaden, H.; Schwanecke, U.; Schulze, R. Projection-based improvement of 3D reconstructions from motion-impaired dental cone beam CT data. Med. Phys. 2019, 46, 4470–4480. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Referring department | p Value | ||||
|---|---|---|---|---|---|---|
| Oral and Maxillofacial Surgery (n = 1063) | Endodontics (n = 182) | Periodontology (n = 122) | Orthodontics (n = 42) | |||
| Target jaw | Maxilla | 577 (54.3) | 101 (55.5) | 73 (59.8) | 23(54.8) | <0.001 ^ |
| Mandible | 371 (34.9) | 73 (40.1) | 18 (14.8) | 19 (45.2) | ||
| Maxilla and mandible | 115 (10.8) | 8 (4.4) | 31 (25.4) | 0 (0) | ||
| Target anatomical structures | Teeth | 83 (7.8) | 182 (100) | 0 (0) | 42 (100) | <0.001 ^ |
| Bone | 572 (53.8) | 0 (0) | 122 (100) | 0 (0) | ||
| Bone and teeth | 408 (38.4) | 0 (0) | 0 (0) | 0 (0) | ||
| Panoramic X ray proceeded the CBCT | Yes | 891 (83.8) | 39 (21.4) | 48 (39.3) | 40 (95.2) | <0.001 ^ |
| No | 172 (16.2) | 143 (78.6) | 74 (60.7) | 2 (4.8) | ||
| Periapical X ray preceded the CBCT | Yes | 689 (66.6) | 182 (100) | 122 (100) | 41 (97.6) | <0.001 ^ |
| No | 374 (35.2) | 0 (0) | 0 (0) | 1 (2.4) | ||
| Indication of CBCT | Diagnostic need | 935 (88.0) | 182 (100) | 122 (100) | 39 (92.9) | <0.001 ^ |
| Treatment need | 128 (12.0) | 0 (0) | 0 (0) | 3 (7.1) | ||
| Diagnosis has been changed after CBCT | No | 872 (82.0) | 147 (80.8) | 97 (79.5) | 14 (33.3) | <0.001 ^ |
| Yes | 191 (18.0) | 35 (19.2) | 25 (20.5) | 28 (66.7) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedlander-Barenboim, S.; Hamed, W.; Zini, A.; Yarom, N.; Abramovitz, I.; Chweidan, H.; Finkelstein, T.; Almoznino, G. Patterns of Cone-Beam Computed Tomography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center. Healthcare 2021, 9, 1042. https://doi.org/10.3390/healthcare9081042
Friedlander-Barenboim S, Hamed W, Zini A, Yarom N, Abramovitz I, Chweidan H, Finkelstein T, Almoznino G. Patterns of Cone-Beam Computed Tomography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center. Healthcare. 2021; 9(8):1042. https://doi.org/10.3390/healthcare9081042
Chicago/Turabian StyleFriedlander-Barenboim, Silvina, Wafi Hamed, Avraham Zini, Noam Yarom, Itzhak Abramovitz, Harry Chweidan, Tamar Finkelstein, and Galit Almoznino. 2021. "Patterns of Cone-Beam Computed Tomography (CBCT) Utilization by Various Dental Specialties: A 4-Year Retrospective Analysis from a Dental and Maxillofacial Specialty Center" Healthcare 9, no. 8: 1042. https://doi.org/10.3390/healthcare9081042