
A Short Mindfulness Retreat for Students to Reduce Stress and Promote Self-Compassion: Pilot Randomised Controlled Trial Exploring Both an Indoor and a Natural Outdoor Retreat Setting

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
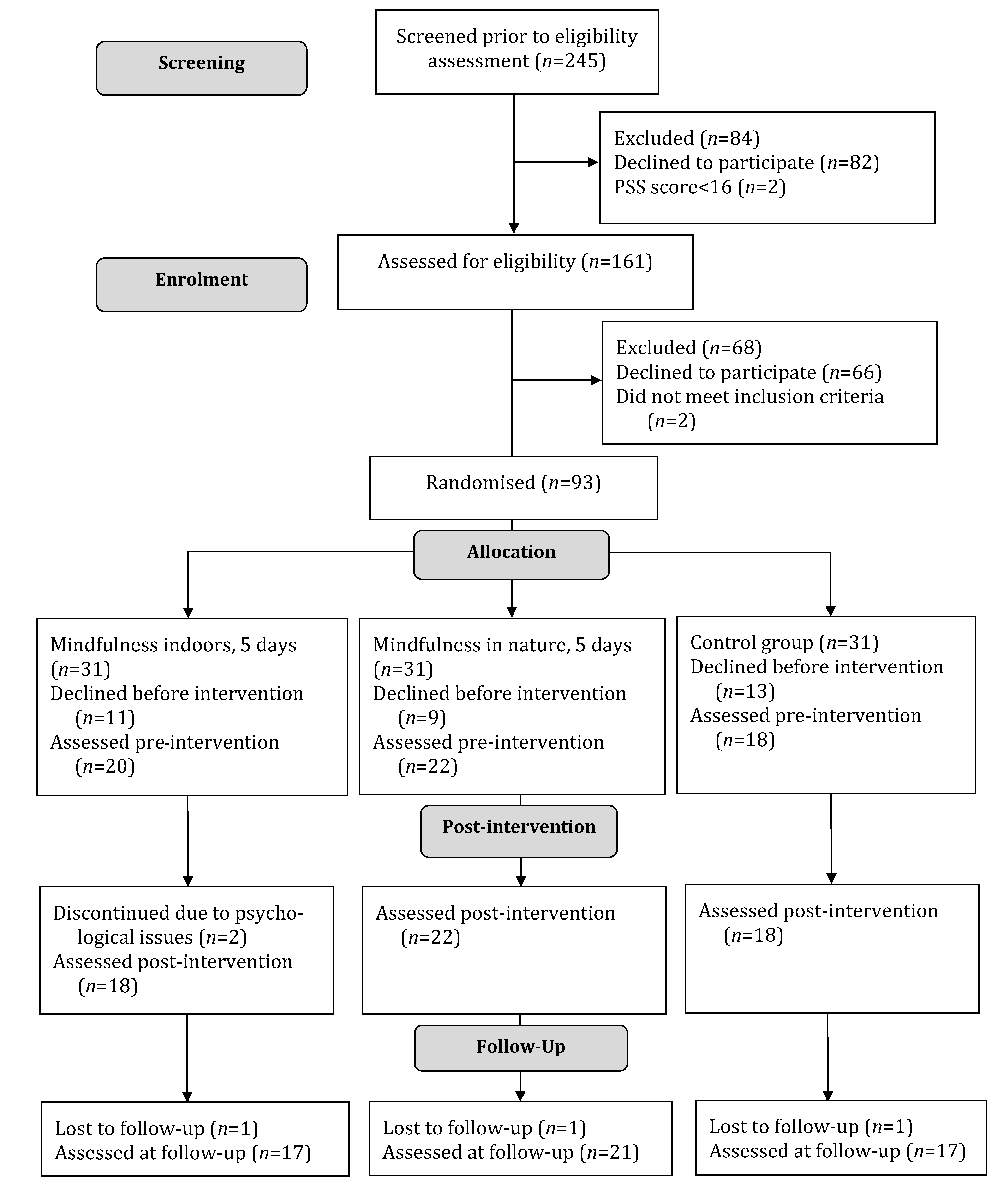
2.2. Participants and Procedure
- Participants were active bachelor’s or master’s degree students at Danish universities or university colleges;
- They had elevated self-reported perceived stress at the time of enrolment in the project, indicated by a PSS score of 16 or above [34];
- They had no known psychiatric diagnosis such as severe depression, severe anxiety, adjustment disorder, post-traumatic stress disorder, personality disorder, or psychosis, and no known autism or untreated attention deficit hyperactivity disorder;
- They had no self-reported risk of suicide or addiction to alcohol, tobacco, or drugs.
2.3. Randomisation
2.4. Interventions
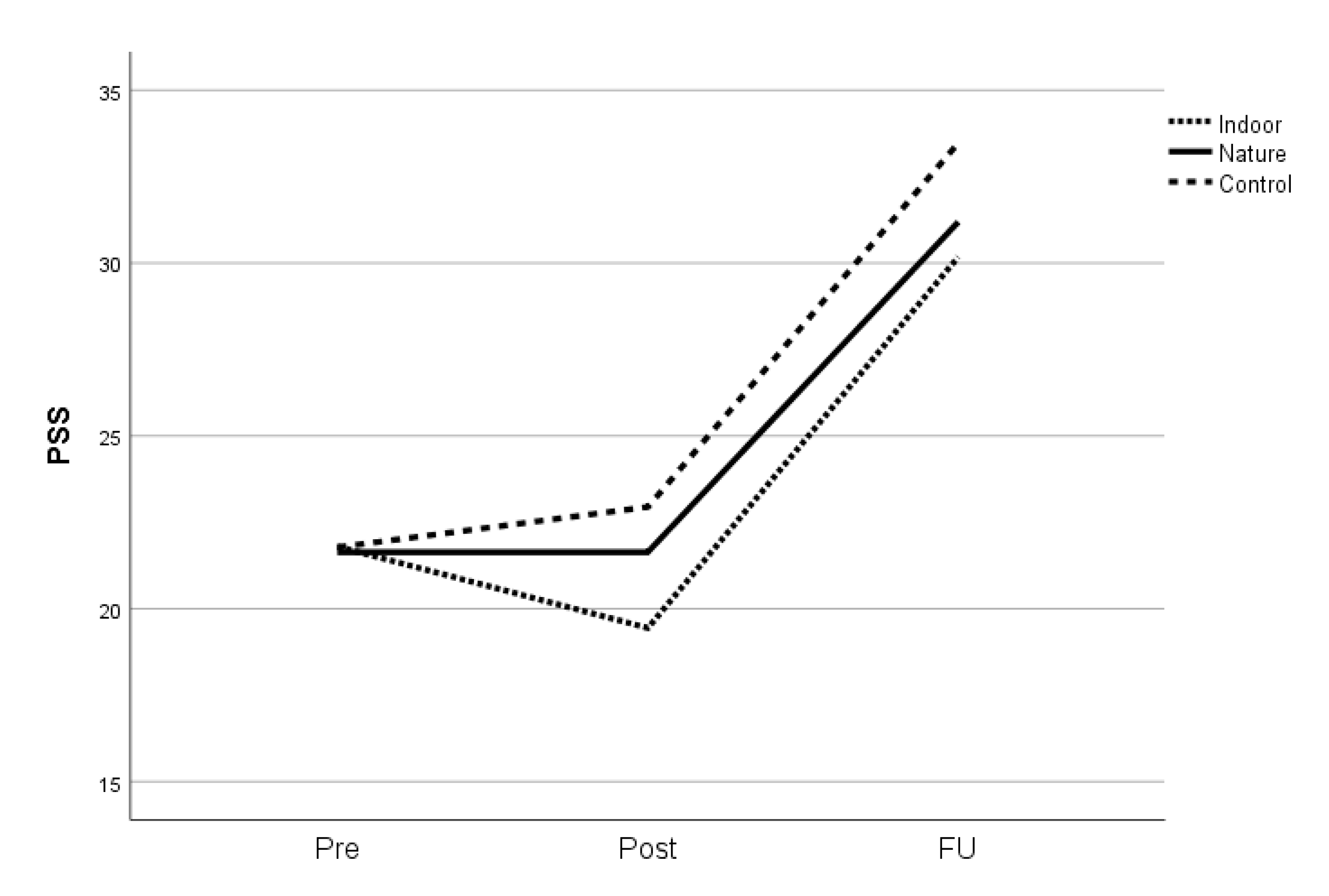
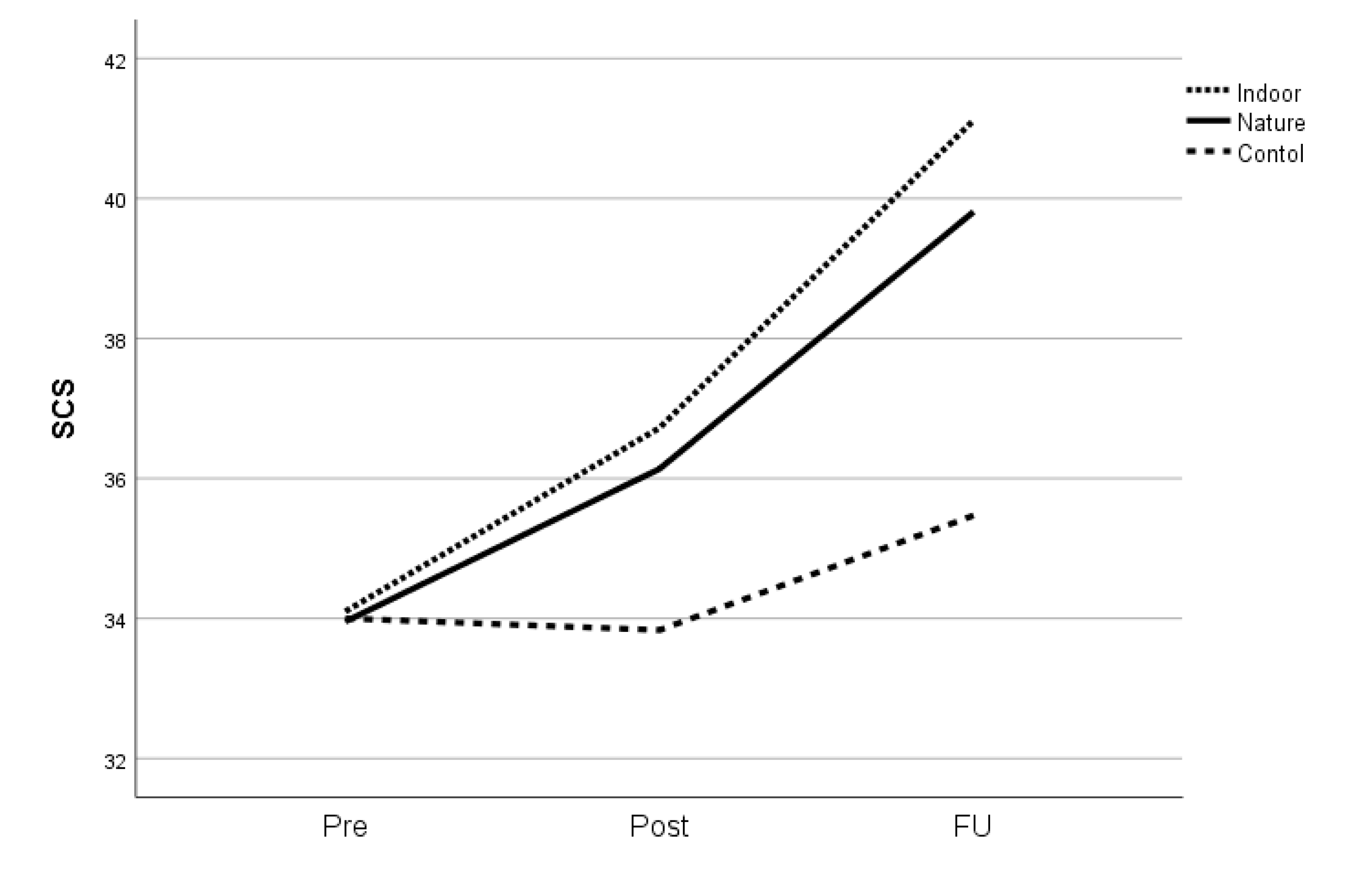
2.5. Primary Outcomes
2.6. Secondary Outcomes
2.7. Analytic Strategy
3. Results
3.1. Characteristics of Participants
3.2. Effects of the 5-Day Residential Mindfulness Interventions
3.3. Effects of Bringing the Programme into a Natural Setting
4. Discussion
4.1. Effects of the Residential Mindfulness Training Programme
4.2. Mindfulness in the Indoor Setting Compared with the Natural Outdoor Setting
4.3. Further Research
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychological Association. Stress in AmericaTM 2019. Available online: https://www.apa.org/news/press/releases/stress/2019/stress-america-2019.pdf (accessed on 25 April 2021).
- Hvidberg, M.F.; Johnsen, S.P.; Davidsen, M.; Ehlers, L. A nationwide study of prevalence rates and characteristics of 199 chronic conditions in Denmark. Pharm. Open 2019, 4, 361–380. [Google Scholar] [CrossRef] [Green Version]
- Weinberger, A.H.; Gbedemah, M.; Martinez, A.M.; Nash, D.; Galea, S.; Goodwin, R.D. Trends in depression prevalence in the USA from 2005 to 2015: Widening disparities in vulnerable groups. Psychol. Med. 2018, 48, 1308–1315. [Google Scholar] [CrossRef]
- Auerbach, R.P.; Mortier, P.; Bruffaerts, R.; Alonso, J.; Benjet, C.; Cuijpers, P.; Kessler, R.C. WHO world mental health surveys international college student project: Prevalence and distribution of mental disorders. J. Abnorm. Psychol. 2018, 127, 623–638. [Google Scholar] [CrossRef]
- Mahmoud, J.S.R.; Staten, R.T.; Hall, L.A.; Lennie, T.A. The relationship among young adult college students’ depression, anxiety, stress, demographics, life satisfaction, and coping styles. Issues Ment. Health Nurs. 2012, 33, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Bantam Books: New York, NY, USA, 2013. [Google Scholar]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H.; Lawler, J.J.; Wood, S.A. Nature contact and human health: A research agenda. Environ. Health Perspect. 2017, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClintock, A.S.; Brown, R.; Coe, C.L.; Zgierska, A.; Barrett, B. mindfulness practice and stress following mindfulness-based stress reduction: Examining within-person and between-person associations with latent curve modeling. Mindfulness 2019, 10, 1905–1914. [Google Scholar] [CrossRef]
- Gilbert, P. The origins and nature of compassion focused therapy. Br. J. Clin. Psychol. 2014, 53, 6–41. [Google Scholar] [CrossRef]
- Gilbert, P. The Compassionate Mind: A New Approach to the Challenge of Life; Constable Robinson: London, UK, 2010. [Google Scholar]
- Williams, J.M.G.; Kabat-Zinn, J. Mindfulness: Diverse perspectives on its meaning, origins, and multiple applications at the intersection of science and dharma. Contemp. Buddhism 2011, 12, 1–18. [Google Scholar] [CrossRef]
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef]
- Khoury, B.; Lecomte, T.; Fortin, G.; Masse, M.; Therien, P.; Bouchard, V.; Hofmann, S.G. Mindfulness-based therapy: A comprehensive meta-analysis. Clin. Psychol. Rev. 2013, 33, 763–771. [Google Scholar] [CrossRef]
- Nam, S.; Toneatto, T. The influence of attrition in evaluating the efficacy and effectiveness of mindfulness-based interventions. Int. J. Ment. Health Addict. 2016, 14, 969–981. [Google Scholar] [CrossRef]
- Mackenzie, C.S.; Poulin, P.A.; Seidman-Carlson, R. A brief mindfulness-based stress reduction intervention for nurses and nurse aides. Appl. Nurs. Res. 2006, 19, 105–109. [Google Scholar] [CrossRef]
- Spijkerman, M.P.J.; Pots, W.T.M.; Bohlmeijer, E.T. Effectiveness of online mindfulness-based interventions in improving mental health: A review and meta-analysis of randomised controlled trials. Clin. Psychol. Rev. 2016, 45, 102–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoury, B.; Knäuper, B.; Schlosser, M.; Carrière, K.; Chiesa, A. Effectiveness of traditional meditation retreats: A systematic review and meta-analysis. J. Psychosom. Res. 2017, 92, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The restorative benefits of nature: Towards an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Kaplan, S.; Kaplan, R. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Kaplan, S.; Bardwell, L.V.; Slakter, D.B. The museum as a restorative environment. Environ. Behav. 1993, 25, 725–742. [Google Scholar] [CrossRef]
- Stevenson, M.P.; Schilhab, T.; Bentsen, P. Attention restoration theory II: A systematic review to clarify attention processes affected by exposure to natural environments. J. Toxicol. Environ. Health Part B Crit. Rev. 2018, 21, 227–268. [Google Scholar] [CrossRef]
- Kaplan, S. Meditation, restoration, and the management of mental fatigue. Environ. Behav. 2001, 33, 480–506. [Google Scholar] [CrossRef] [Green Version]
- Tang, Y.Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef]
- Fox, K.C.R.; Dixon, M.L.; Nijeboer, S.; Girn, M.; Floman, J.L.; Lifshitz, M.; Ellamil, M.; Sedlmeier, P.; Christoff, K. Functional neuroanatomy of meditation: A review and meta-analysis of 78 functional neuroimaging investigations. Neurosci. Biobehav. Rev. 2016, 65, 208–228. [Google Scholar] [CrossRef] [Green Version]
- Djernis, D.; Lerstrup, I.; Poulsen, D.; Stigsdotter, U.; Dahlgaard, J.; O’Toole, M. A systematic review and meta-analysis of nature-based mindfulness: Effects of moving mindfulness training into an outdoor natural setting. Int. J. Environ. Res. Public Health 2019, 16, 3202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Nyed, P.K.; Larsen, H.B.; Fjorback, L.O. Efficacy of nature-based therapy for individuals with stress-related illnesses: Randomised controlled trial. Br. J. Psychiatry 2018, 213, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Willert, M.V.; Thulstrup, A.M.; Wieclaw, J. Rehabilitation of individuals on long-term sick leave due to sustained stress-related symptoms: A comparative follow-up study. Scand. J. Public Health 2014, 42, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Lymeus, F.; Lindberg, P.; Hartig, T. Building mindfulness bottom-up: Meditation in natural settings supports open monitoring and attention restoration. Conscious. Cogn. 2018, 59, 40–56. [Google Scholar] [CrossRef] [PubMed]
- Lymeus, F. Mindfulness Training Supported by a Restorative Natural Setting. Ph.D. Thesis, Uppsala University, Uppsala, Sweden, 18 October 2019. [Google Scholar]
- Choe, E.Y.; Jorgensen, A.; Sheffield, D. Does a natural environment enhance the effectiveness of mindfulness-based stress reduction (MBSR)? Examining the mental health and wellbeing, and nature connectedness benefits. Landsc. Urban Plan. 2020, 202, 103886. [Google Scholar] [CrossRef]
- Sedlmeier, P.; Eberth, J.; Schwarz, M.; Zimmermann, D.; Haarig, F.; Jaeger, S.; Kunze, S. The psychological effects of meditation: A meta-analysis. Psychol. Bull. 2012, 138, 1139–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Levinson, D.B.; Stoll, E.L.; Kindy, S.D.; Merry, H.L.; Davidson, R.J. A mind you can count on: Validating breath counting as a behavioral measure of mindfulness. Front. Psychol. 2014, 5, 1–10. [Google Scholar] [CrossRef]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Raes, F.; Pommier, E.; Neff, K.D.; Van Gucht, D. Construction and factorial validation of a short form of the self-compassion scale. Clin. Psychol. Psychother. 2011, 18, 250–255. [Google Scholar] [CrossRef]
- Eskildsen, A.; Dalgaard, V.L.; Nielsen, K.J.; Andersen, J.H.; Zachariae, R.; Olsen, L.R.; Jørgensen, A.; Christiansen, D.H. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item perceived stress scale. Scand. J. Work. Environ. Health 2015, 41, 486–490. [Google Scholar] [CrossRef]
- Bohlmeijer, E.; Klooster, P.M.; Fledderus, M.; Veehof, M.; Baer, R. Psychometric properties of the five facet mindfulness questionnaire in depressed adults and development of a short form. Assessment 2011, 18, 308–320. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.G.; Krogh, S.C.; Westphael, G.; Hjordt, L.V. Mindfulness is positively related to socioeconomic job status and income and independently predicts mental distress in a long-term perspective: Danish validation studies of the Five-Factor Mindfulness Questionnaire. Psychol. Assess. 2019, 31, e1–e20. [Google Scholar] [CrossRef]
- Mayer, F.S.; Frantz, C.M.P. The connectedness to nature scale: A measure of individuals’ feeling in community with nature. J. Environ. Psychol. 2004, 24, 503–515. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.F.; Massar, S.A.; Chee, M.W.; Lim, J. Towards an objective measure of mindfulness: Replicating and extending the features of the breath-counting task. Mindfulness 2018, 9, 1402–1410. [Google Scholar] [CrossRef] [Green Version]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef] [PubMed]
- Heck, R.H.; Thomas, S.L.; Tabata, L.N. Multilevel and Longitudinal Modeling with IBM SPSS, 2nd ed.; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life. Med. Care 2011, 41, 582–592. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Hillsdale, NJ, USA; New York, NY, USA, 1988. [Google Scholar]
- Kozasa, E.H.; Lacerda, S.S.; Menezes, C.; Wallace, B.A.; Radvany, J.; Mello, L.E.A.M.; Sato, J.R. Effects of a 9-day Shamatha Buddhist meditation retreat on attention, mindfulness and self-compassion in participants with a broad range of meditation experience. Mindfulness 2015, 6, 1235–1241. [Google Scholar] [CrossRef]
- Ostafin, B.D.; Chawla, N.; Bowen, S.; Dillworth, T.M.; Witkiewitz, K.; Marlatt, G.A. Intensive mindfulness training and the reduction of psychological distress: A preliminary study. Cogn. Behav. Pract. 2006, 13, 191–197. [Google Scholar] [CrossRef]
- De Vibe, M. Mindfulness based stress reduction (MBSR) for improving health, quality of life, and social functioning in adults. Campbell Syst. Rev. 2012, 8, 1–127. [Google Scholar] [CrossRef] [Green Version]
- Eberth, J.; Sedlmeier, P. The effects of mindfulness meditation: A meta-analysis. Mindfulness 2012, 3, 174–189. [Google Scholar] [CrossRef]
- Schmidt Hammer Lassen Architects. Available online: https://www.shl.dk/via-university-college-campus/ (accessed on 25 April 2021).
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Piatkus: London, UK, 1994. [Google Scholar]
- Sarter, M.; Givens, B.; Bruno, J.P. The cognitive neuroscience of sustained attention: Where top-down meets bottom-up. Brain Res. Rev. 2001, 35, 146–160. [Google Scholar] [CrossRef]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Lymeus, F.; Lundgren, T.; Hartig, T. Attentional effort of beginning mindfulness training is offset with practice directed toward images of natural scenery. Environ. Behav. 2017, 49, 536–559. [Google Scholar] [CrossRef]
- Tang, Y.Y.; Posner, M.I. Attention training and attention state training. Trends Cogn. Sci. 2009, 13, 222–227. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Time | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 |
|---|---|---|---|---|---|---|
| 7.00–8.00 | Sitting, yoga and body scan | Sitting, mindful movement/sitting | Sitting, yoga, sitting | Sitting, yoga, sitting | Sitting, walking, sitting (no guidance) | |
| 9.30–12.30 | Session 1, second part | Session 3 | Sessions 5–6 | ‘All day’ in silence ends | Session 8, second part (until 11:30 a.m.) | |
| 14.30–18.00 | Session 2 | Sessions 4–5 | ‘All day’ in silence begins | Session 7 | ||
| 19.30–20.30 | Presentation, silent walk, Session 1, first part | Silent walk, circle, economy of words | Silent walk, circle reflections | Sitting, silent walk, sitting | Sitting, silent walk |
| Session | Content |
|---|---|
| 1 | Introduction to the programme, theoretical underpinnings of mindfulness. Guided reflections and sitting meditation, mindful eating, body scan, and yoga. |
| 2 | Guided yoga, sitting meditation, and body scan. Theme: how we perceive the world. |
| 3 | Guided yoga, sitting, and walking meditation. Themes: formal versus informal meditation/presence, and awareness of pleasant events. |
| 4 | Guided yoga and sitting meditation. Theme: awareness of unpleasant events, focusing on stress reactivity. |
| 5 | Guided yoga, sitting meditation. Themes: stress, reacting versus responding to stressful events. |
| 6 | Guided yoga, sitting meditation. Theme: communication. Illustrative exercises including different communication styles and behaviour patterns. |
| All day | Guided yoga, sitting and walking meditation, body scan, eating meditation, mountain or lake meditation, loving–kindness meditation, and visual meditation. |
| 7 | Guided yoga and sitting meditation. Inclusion of aspects from previous sessions with emphasis on making the practice one’s own. |
| 8 | Guided body scan, yoga, and sitting meditation. Guided reflections on the course and future actions. |
| Group | N | Mean (SD) | Range | CI | ANOVA F (p) | |
|---|---|---|---|---|---|---|
| Age, years | 0.821 (0.445) | |||||
| Indoor | 20 | 31.65 (7.45) | 24–54 | 28.16–35.14 | ||
| Nature | 22 | 31.27 (9.59) | 21–60 | 27.02–35.53 | ||
| Control | 18 | 28.61 (5.91) | 22–44 | 25.67–31.55 | ||
| Total | 60 | 30.60 (7.91) | 21–60 | 28.56–32.64 | ||
| Prior mindfulness training | 0.2 (0.790) | |||||
| Indoor | 20 | 0.32 (0.48) | 0–1 | 0.09–0.55 | ||
| Nature | 22 | 0.24 (0.44) | 0–1 | 0.04–0.44 | ||
| Control | 18 | 0.22 (0.43) | 0–1 | 0.01–0.43 | ||
| Total | 60 | 0.26 (0.44) | 0–1 | 0.14–0.37 | ||
| Prior exposure to nature | 0.055 (0.947) | |||||
| Indoor | 20 | 6.05 (1.79) | 3–10 | 5.21–6.89 | ||
| Nature | 22 | 6.27 (2.35) | 2–11 | 5.23–7.32 | ||
| Control | 18 | 6.17 (2.33) | 2–10 | 5.01–7.33 | ||
| Total | 60 | 6.17 (2.14) | 2–11 | 5.61–6.72 | ||
| Outcome variables | ||||||
| PSS | 0.005 (0.995) | |||||
| Indoor | 20 | 21.80 (6.49) | 5–32 | 18.76–24.84 | ||
| Nature | 22 | 21.64 (4.77) | 14–30 | 19.52–23.75 | ||
| Control | 18 | 21.78 (5.29) | 12–32 | 19.15–24.41 | ||
| Total | 60 | 21.73 (5.45) | 5–32 | 20.33–23.14 | ||
| SCS | 0.002 (0.998) | |||||
| Indoor | 20 | 34.10 (6.49) | 24–48 | 31.06–37.14 | ||
| Nature | 22 | 33.95 (7.39) | 19–52 | 30.68–37.23 | ||
| Control | 18 | 34.00 (9.29) | 17–50 | 29.38–38.62 | ||
| Total | 60 | 34.02 (7.61) | 17–52 | 32.05–35.98 | ||
| FFMQ | 0.406 (0.668) | |||||
| Indoor | 20 | 118.45 (17.85) | 87–151 | 110.09–126.81 | ||
| Nature | 22 | 120.91 (19.24) | 82–161 | 112.38–129.44 | ||
| Control | 18 | 124.11 (21.06) | 84–159 | 113.64–134.59 | ||
| Total | 60 | 121.05 (19.17) | 82–161 | 116.10–126.00 | ||
| BCT | 1.1201 (0.309) | |||||
| Indoor | 20 | 83.11 (13.36) | 50–100 | 76.86–89.36 | ||
| Nature | 22 | 80.29 (20.56) | 22.73–100 | 71.17–89.40 | ||
| Control | 18 | 88.29 (13.24) | 53.85–100 | 81.70–94.88 | ||
| Total | 60 | 83.63 (16.41) | 22.73–100 | 79.39.87.87 | ||
| CNS | 0.869 (0.425) | |||||
| Indoor | 20 | 52.10 (6.38) | 43–64 | 49.11–55.09 | ||
| Nature | 22 | 48.68 (10.12) | 25–63 | 44.19–53.17 | ||
| Control | 18 | 50.94 (8.60) | 40–66 | 46.67–55.22 | ||
| Total | 60 | 50.50 (8.55) | 25–66 | 48.29–52.71 |
| Time x Group Interaction Post-Treatment | Time x Group Interaction at Follow-Up | |||||
|---|---|---|---|---|---|---|
| F | p | g | F | p | g | |
| Primary outcome PSS | ||||||
| All groups | 2.0 | 0.146 | 0.36 | 1.0 | 0.373 | 0.18 |
| Control vs. indoor | 3.0 | 0.091 | 0.56 | 1.6 | 0.212 | 0.29 |
| Control vs. nature | 1.2 | 0.283 | 0.34 | 1.2 | 0.276 | 0.24 |
| Indoor vs. nature | 1.4 | 0.241 | 0.36 | 0.3 | 0.578 | 0.12 |
| Primary outcome SCS | ||||||
| All groups | 0.6 | 0.532 | 0.20 | 2.9 | 0.058 | 0.31 |
| Control vs. indoor | 1.0 | 0.323 | 0.33 | 5.4 | 0.023 | 0.54 |
| Control vs. nature | 1.4 | 0.242 | 0.37 | 4.9 | 0.030 | 0.49 |
| Indoor vs. nature | <0.1 | 0.931 | 0.03 | 0.1 | 0.752 | 0.07 |
| Secondary outcome FFMQ | ||||||
| All groups | 1.1 | 0.350 | 0.27 | 4.0 | 0.021 | 0.37 |
| Control vs. indoor | 2.3 | 0.136 | 0.50 | 9.8 | 0.003 | 0.74 |
| Control vs. nature | 1.8 | 0.187 | 0.42 | 4.8 | 0.032 | 0.48 |
| Indoor vs. nature | <0.1 | 0.982 | 0.01 | 0.5 | 0.479 | 0.15 |
| Secondary outcome BCT | ||||||
| All groups | 3.6 | 0.032 | 0.49 | 1.7 | 0.195 | 0.24 |
| Control vs. indoor | 7.6 | 0.009 | 0.90 | 3.6 | 0.060 | 0.45 |
| Control vs. nature | 3.2 | 0.080 | 0.55 | 0.9 | 0.344 | 0.21 |
| Indoor vs. nature | 0.6 | 0.448 | 0.23 | 0.8 | 0.375 | 0.20 |
| Secondary outcome CNS | ||||||
| All groups | 2.1 | 0.135 | 0.37 | 2.4 | 0.096 | 0.29 |
| Control vs. indoor | 0.2 | 0.676 | 0.15 | 1.6 | 0.210 | 0.30 |
| Control vs. nature | 2.2 | 0.150 | 0.46 | 5.4 | 0.023 | 0.52 |
| Indoor vs. nature | 2.9 | 0.096 | 0.53 | 0.7 | 0.399 | 0.18 |
| n | PSS | SCS | FFMQ | BCT | CNS | ||
|---|---|---|---|---|---|---|---|
| Pre | Nature | 22 | 21.6 (4.8) | 34.0 (7.4) | 120.9 (12.2) | 80.3 (13.4) | 48.7 (10.1) |
| Indoor | 20 | 21.8 (6.5) | 34.1 (6.4) | 118.5 (17.8) | 83.1 (13.3) | 52.1 (6.4) | |
| Control | 18 | 21.8 (5.3) | 34.0 (9.3) | 124.1 (21.1) | 88.3 (13.22) | 50.5 (8.5) | |
| Post | Nature | 22 | 21.6 (4.9) | 36.1 (9.1) | 128.7 (21.1) | 87.6 (8.8) | 51.5 (9.5) |
| Indoor | 18 | 19.4 (7.7) | 36.7 (10.5) | 125.7 (20.7) | 94.1 (9.4) | 51.5 (9.5) | |
| Control | 18 | 22.9 (6.7) | 33.8 (10.7) | 124.4 (25.4) | 84.8 (18.8) | 51.7 (8.2) | |
| FU | Nature | 21 | 31.2 (3.6) | 39.8 (7.8) | 132.5 (21.2) | 84.3 (13.1) | 52.5 (10.2) |
| Indoor | 17 | 30.1 (3.8) | 41.1 (6.9) | 133.8 (20.3) | 90.7 (9.5) | 54.1 (8.4) | |
| Control | 17 | 33.5 (3.5) | 35.5 (8.9) | 125.9 (24.5) | 86.5 (15.7) | 52.3 (8.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Djernis, D.; O’Toole, M.S.; Fjorback, L.O.; Svenningsen, H.; Mehlsen, M.Y.; Stigsdotter, U.K.; Dahlgaard, J. A Short Mindfulness Retreat for Students to Reduce Stress and Promote Self-Compassion: Pilot Randomised Controlled Trial Exploring Both an Indoor and a Natural Outdoor Retreat Setting. Healthcare 2021, 9, 910. https://doi.org/10.3390/healthcare9070910
Djernis D, O’Toole MS, Fjorback LO, Svenningsen H, Mehlsen MY, Stigsdotter UK, Dahlgaard J. A Short Mindfulness Retreat for Students to Reduce Stress and Promote Self-Compassion: Pilot Randomised Controlled Trial Exploring Both an Indoor and a Natural Outdoor Retreat Setting. Healthcare. 2021; 9(7):910. https://doi.org/10.3390/healthcare9070910
Chicago/Turabian StyleDjernis, Dorthe, Mia S. O’Toole, Lone O. Fjorback, Helle Svenningsen, Mimi Y. Mehlsen, Ulrika K. Stigsdotter, and Jesper Dahlgaard. 2021. "A Short Mindfulness Retreat for Students to Reduce Stress and Promote Self-Compassion: Pilot Randomised Controlled Trial Exploring Both an Indoor and a Natural Outdoor Retreat Setting" Healthcare 9, no. 7: 910. https://doi.org/10.3390/healthcare9070910