
Does the Coronectomy a Feasible and Safe Procedure to Avoid the Inferior Alveolar Nerve Injury during Third Molars Extractions? A Systematic Review


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focused Question Based on PICOS Strategy
2.3. Outcome Measures
2.4. Search Strategy
2.5. Eligibility Criteria and Study Selection Process
2.6. Data Synthesis
2.7. Assessment of the Risk of Bias
2.8. Statistical Analysis
3. Results
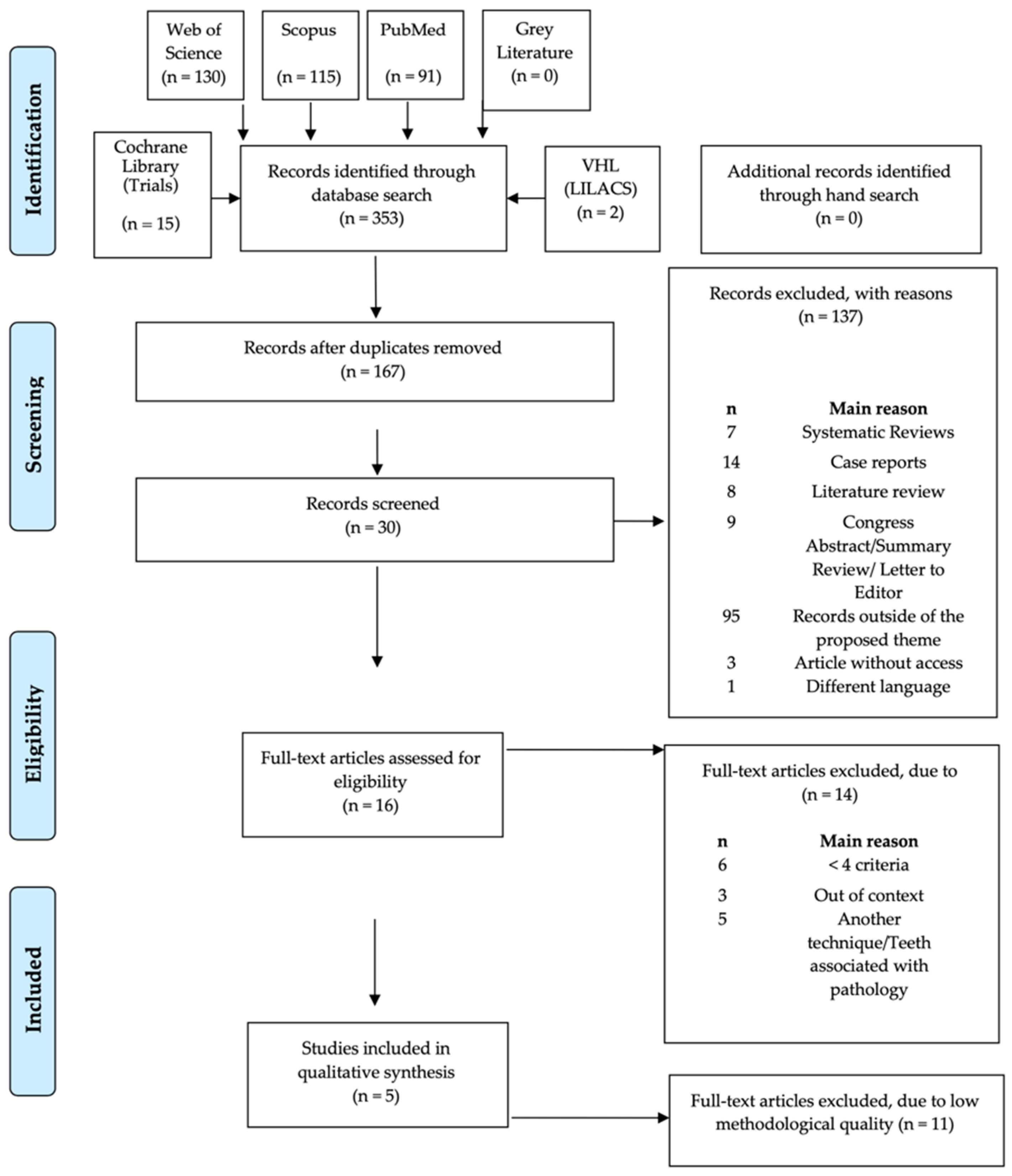
3.1. Literature Search
3.2. Study Characteristics
3.2.1. IAN Injury
3.2.2. LN Injury
3.2.3. Root Migration
3.2.4. Pain
3.2.5. Infection
3.2.6. Dry Socket
3.2.7. Extraction of the Remaining Root
3.2.8. Necessity for Reintervention
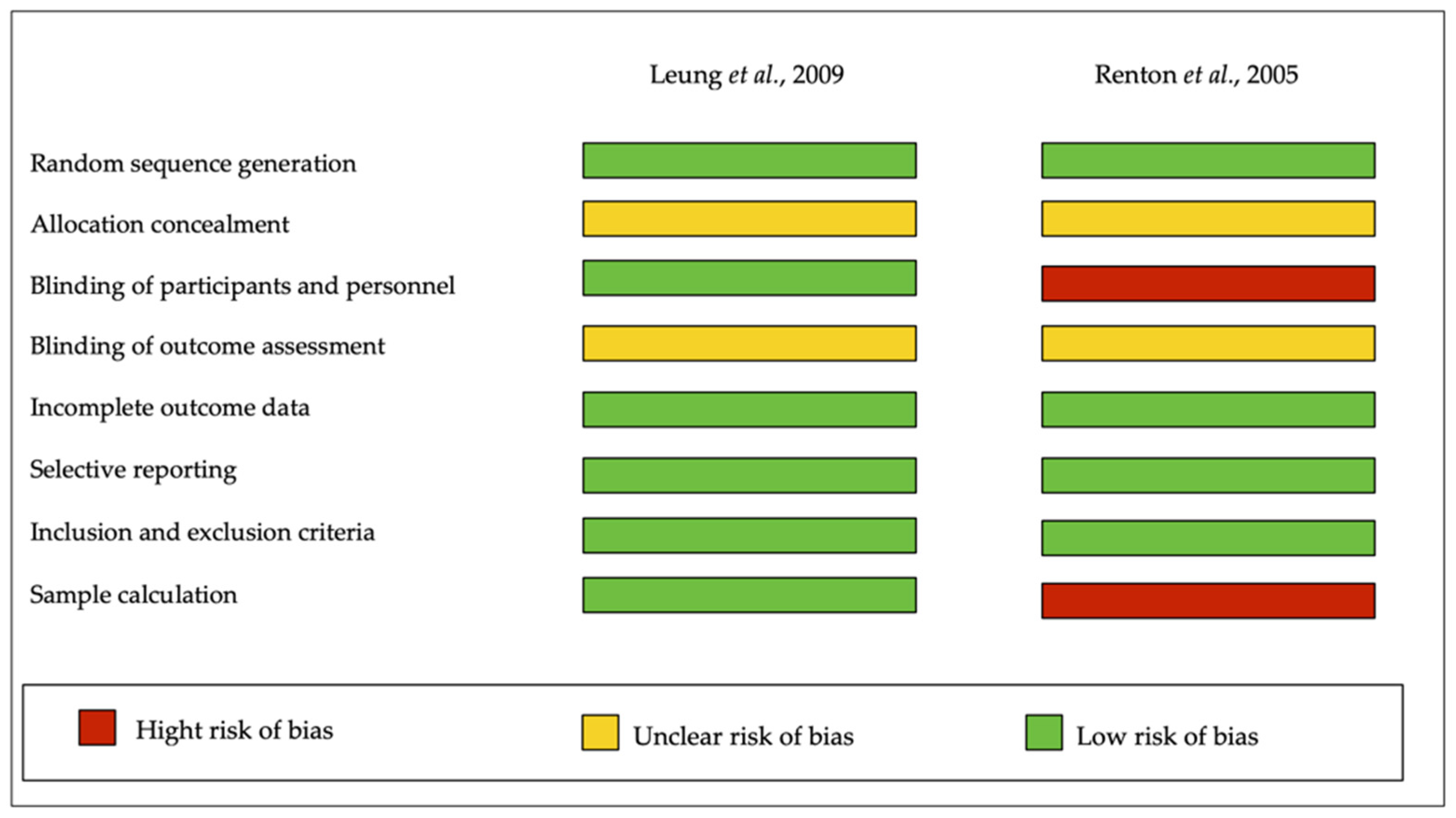
3.3. Assessments of the Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ali, A.; Benton, J.; Yates, J. Risk of inferior alveolar nerve injury with coronectomy vs surgical extraction of mandibular third molars—A comparison of two techniques and review of the literature. J. Oral Rehabil. 2018, 45, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Frenkel, B.; Givol, N.; Shoshani, Y. Coronectomy of the mandibular third molar: A retrospective study of 185 procedures and the decision to repeat the coronectomy in cases of failure. J. Oral Maxillofac. Surg. 2015, 73, 587–594. [Google Scholar] [CrossRef]
- Kouwenberg, A.; Stroy, L.; Rijt, E.V.-V.D.; Mensink, G.; Gooris, P. Coronectomy of the mandibular third molar: Respect for the inferior alveolar nerve. J. Cranio-Maxillofac. Surg. 2016, 44, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Lieblich, S.E.; Dym, H.; Fenton, D. Dentoalveolar Surgery. J. Oral Maxillofac. Surg. 2017, 75, e50–e73. [Google Scholar] [CrossRef] [PubMed]
- Cervera-Espert, J.; Pérez-Martínez, S.; Cervera-Ballester, J.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Coronectomy of impacted mandibular third molars: A meta-analysis and systematic review of the literature. Med. Oral Patol. Oral y Cir. Bucal 2016, 21, e505. [Google Scholar] [CrossRef] [PubMed]
- Cilasun, U.; Yildirim, T.; Guzeldemir, E.; Pektas, Z.O. Coronectomy in patients with high risk of inferior alveolar nerve injury diagnosed by computed tomography. J. Oral Maxillofac. Surg. 2011, 69, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Yun, P.-Y.; Kim, Y.-K. Intentional partial odontectomy—A long-term follow-up study. Maxillofac. Plast. Reconstr. Surg. 2017, 39, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, Y.Y.; Cheung, L.K. Safety of coronectomy versus excision of wisdom teeth: A randomized controlled trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 108, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Dalle Carbonare, M.; Zavattini, A.; Duncan, M.; Williams, M.; Moody, A. Injury to the inferior alveolar and lingual nerves in successful and failed coronectomies: Systematic review. Br. J. Oral Maxillofac. Surg. 2017, 55, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Rood, J.; Shehab, B.N. The radiological prediction of inferior alveolar nerve injury during third molar surgery. Br. J. Oral Maxillofac. Surg. 1990, 28, 20–25. [Google Scholar] [CrossRef]
- Knutsson, K.; Lysell, L.; Rohlin, M. Postoperative status after partial removal of the mandibular third molar. Swed. Dent. J. 1989, 13, 15–22. [Google Scholar]
- Pogrel, M.A. An update on coronectomy. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2009, 67, 1782–1783. [Google Scholar] [CrossRef]
- Pogrel, M.A.; Lee, J.; Muff, D. Coronectomy: A technique to protect the inferior alveolar nerve. J. Oral Maxillofac. Surg. 2004, 62, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Ítems de referencia para publicar Protocolos de Revisiones Sistemáticas y Metaanálisis: Declaración PRISMA-P 2015. Rev. Española de Nutr. Hum. y Dietética 2016, 20, 148–160. [Google Scholar]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 17 June 2021).
- Higgins, J.P.; Green, S. The Cochrane Collaboration. Cochrane Handb. Syst. Rev. Interv. 2011, 4. [Google Scholar]
- Agbaje, J.O.; Heijsters, G.; Salem, A.S.; Van Slycke, S.; Schepers, S.; Politis, C.; Vrielinck, L. Coronectomy of deeply impacted lower third molar: Incidence of outcomes and complications after one year follow-up. J. Oral Maxillofac. Res. 2015, 6, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, F.; Xue, Z.; Zhou, X.; Zhang, X.; Hou, G.; Feng, Y. Coronectomy: A useful approach in minimizing nerve injury compared with traditional extraction of deeply impacted mandibular third molars. J. Oral Maxillofac. Surg. 2019, 77, 2221.e1–2221.e14. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Cheung, L.K. Long-term morbidities of coronectomy on lower third molar. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, 5–11. [Google Scholar] [CrossRef]
- Leung, Y.Y.; Cheung, L.K. Coronectomy of the lower third molar is safe within the first 3 years. J. Oral Maxillofac. Surg. 2012, 70, 1515–1522. [Google Scholar] [CrossRef]
- Mendes, P.A.; Neiva, I.M.; de Arruda, J.A.A.; Brasileiro, C.B.; Souza, A.C.R.A.; Mesquita, R.A.; Souza, L.N. Coronectomy of partially erupted lower third molars performed by an undergraduate dentistry student: A case series. Oral Maxillofac. Surg. 2020, 24, 417–422. [Google Scholar] [CrossRef]
- Monaco, G.; D'Ambrosio, M.; De Santis, G.; Vignudelli, E.; Gatto, M.R.A.; Corinaldesi, G. Coronectomy: A surgical option for impacted third molars in close proximity to the inferior alveolar nerve—A 5-year follow-up study. J. Oral Maxillofac. Surg. 2019, 77, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, M.; Bak, J.; Matzen, L.; Hartlev, J.; Bindslev, J.; Schou, S.; Nørholt, S. Coronectomy of mandibular third molars: A clinical and radiological study of 231 cases with a mean follow-up period of 5.7 years. Int. J. Oral Maxillofac. Surg. 2018, 47, 1596–1603. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, S.; Vikraman, B.; Duraiswamy Sankar, M.S.V. Evaluation of outcome following coronectomy for the management of mandibular third molars in close proximity to inferior alveolar nerve. J. Clin. Diagn. Res. JCDR 2016, 10, ZC57. [Google Scholar] [CrossRef] [PubMed]
- Kohara, K.; Kurita, K.; Kuroiwa, Y.; Goto, S.; Umemura, E. Usefulness of mandibular third molar coronectomy assessed through clinical evaluation over three years of follow-up. Int. J. Oral Maxillofac. Surg. 2015, 44, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Hatano, Y.; Kurita, K.; Kuroiwa, Y.; Yuasa, H.; Ariji, E. Clinical evaluations of coronectomy (intentional partial odontectomy) for mandibular third molars using dental computed tomography: A case-control study. J. Oral Maxillofac. Surg. 2009, 67, 1806–1814. [Google Scholar] [CrossRef]
- Renton, T.; Hankins, M.; Sproate, C.; McGurk, M. A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br. J. Oral Maxillofac. Surg. 2005, 43, 7–12. [Google Scholar] [CrossRef]
- Leung, Y.; Cheung, K. Root migration pattern after third molar coronectomy: A long-term analysis. Int. J. Oral Maxillofac. Surg. 2018, 47, 802–808. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search Strategy |
|---|---|
| PubMed | #1 ((((((((third molar * [MeSH Terms]) OR third molar * [Title/Abstract]) OR wisdom tooth [MeSH Terms]) OR wisdom tooth [Title/Abstract]) OR wisdom teeth [MeSH Terms]) OR wisdom teeth [Title/Abstract]) OR tooth extraction * [MeSH Terms]) OR tooth extraction * [Title/Abstract]) OR surgical removal [Title/Abstract] #2 (partial odontectom * [Title/Abstract]) OR coronectom * #3 (((((((((((((nerve injury [Title/Abstract]) OR alveolar nerve injury [Title/Abstract]) OR mandibular nerve * [MeSH Terms]) OR mandibular nerve * [Title/Abstract]) OR Inferior Alveolar Nerve * [MeSH Terms]) OR Inferior Alveolar Nerve * [Title/Abstract]) OR paresthesia * [MeSH Terms]) OR paresthesia * [Title/Abstract]) OR dysesthesia * [MeSH Terms]) OR dysesthesia * [Title/Abstract]) OR lingual nerve * [MeSH Terms]) OR lingual nerve * [Title/Abstract]) OR lingual nerve injur * [MeSH Terms]) OR lingual nerve injur * [Title/Abstract] #1 and #2 and #3 |
| Web of Science | #1 TOPIC: (third molar *) OR TOPIC: (wisdom tooth) OR TOPIC: (wisdom teeth) OR TOPIC: (tooth extraction *) OR TOPIC: (surgical removal) #2 TOPIC: (partial odontectom *) OR TOPIC: (coronectom *) #3 TOPIC: (nerve injury) OR TOPIC: (alveolar nerve injury) OR TOPIC: (mandibular nerve *) OR TOPIC: (inferior alveolar nerve *) OR TOPIC: (paresthesia *) OR TOPIC: (dysesthesia *) OR TOPIC: (lingual nerve *) OR TOPIC: (lingual nerve injur *) #1 and #2 and #3 |
| Scopus | #1 Topic: (TITLE-ABS-KEY (third AND molar *) OR TITLE-ABS-KEY (wisdom AND tooth) OR TITLE-ABS-KEY (wisdom AND teeth) OR TITLE-ABS-KEY (tooth AND extraction *) OR TITLE-ABS-KEY (surgical AND removal)) #2 Topic: (TITLE-ABS-KEY (partial AND odontectom *) OR TITLE-ABS-KEY (coronectom *)) #3 Topic: (TITLE-ABS-KEY (nerve AND injury) OR TITLE-ABS-KEY (alveolar AND nerve AND injury) OR TITLE-ABS-KEY (mandibular AND nerve *) OR TITLE-ABS-KEY (inferior AND alveolar AND nerve *) OR TITLE-ABS-KEY (paresthesia *) OR TITLE-ABS-KEY (dysesthesia *) OR TITLE-ABS-KEY (lingual AND nerve *) OR TITLE-ABS-KEY (lingual AND nerve AND injur *)) #1 and #2 and #3 |
| Cochrane Library | third molar * OR wisdom tooth OR wisdom teeth OR tooth extraction * OR surgical removal in Title, Abstract, Keywords, and partial odontectom * OR coronectom * in Title, Abstract, Keywords and nerve injury OR alveolar nerve injury OR mandibular nerve * OR inferior alveolar nerve * OR paresthesia * OR dysesthesia * OR lingual nerve * OR lingual nerve injur * in Title, Abstract, Keywords in Trials |
| VHL(LILACS) | (tw:(third molar OR tooth extraction)) AND (tw:(partial odontectom * OR coronectom *)) AND (tw:(mandibular nerve OR paresthesia OR lingual nerve *)) AND (instance:”regional”) AND (db:(“LILACS”)) |
| Author | Included Coronectomies (n) | IAN Damage (%) | LN Damage (%) | Pain (%) | Infection (%) | Dry Socket (%) | Extraction of the Root (%) | Surgical Reintervention (%) |
|---|---|---|---|---|---|---|---|---|
| Agbaje et al., 2015 | 96 | 0% | 0% | 4.16% | 4.16% | 4.16% | 9.37% | * |
| Cilasun et al., 2011 | 88 | 0% | 0% | 1,13% | 1.13% | 0% | 1.13% | 0% |
| Frenkel et al., 2015 | 185 | 0.54% | * | 8.65% | 1.62% | * | 3.24% | 2.16% |
| Hatano et al., 2009 | 102 | 0.98% | 0% | 18.63% | 0.98% | 1.96% | 4.9% | 0.00% |
| Kang, 2019 | 55 | 0% | * | * | 0% | 2% | 9.09% | * |
| Kohara et al., 2015 | 111 | 0.9% | * | * | * | 0.9% | 9.01% | * |
| Kouwenberg et al., 2016 | 151 | 0% | 0% | * | * | * | 11.26% | * |
| Leung et al., 2009 | 171 | 1.17% | 0% | 38.01% | 5.26% | 0% | 9.36% | * |
| Leung et al., 2012 | 135 | 0.74% | 0% | 42.96% | 4.44% | 0% | 2.96% | * |
| Leung et al., 2016 | 612 | 0.16% | 0% | 31.21% | 2.94% | 0.16% | 2.94% | 0.33% |
| Mendes, 2020 | 35 | 2.85% | * | 48.57% | 2.85% | * | 8.57% | 5.71% |
| Monaco, 2019 | 76 | 0% | 0% | * | 0% | * | 6.57% | 5.26% |
| Mukherjee et al., 2016 | 20 | 0% | 5% | 15% | * | * | 10% | * |
| Pederson et al., 2018 | 231 | 2.16% | 0.86% | 0% | 11.69% | * | 3.46% | * |
| Pogrel et al., 2004 | 50 | 0% | 2% | * | * | * | 6% | * |
| Renton T et al., 2005 | 58 | 0% | 0% | 13.79% | 5.17% | 12.06% | 8% | 0% |
| Total | 2176 |
| Author, Year | Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Exposed Cohort | SELECTION of External Control | Ascertainment of Exposure | Outcome of Interest Not Present at the Start | Comparability of Cohorts on the Basis of the Design of Analysis | Assessment of the Outcome | Was Follow-up Long Enough for Outcomes Occur | Adequacy of Follow up of Cohorts | Total 9/9 | |
| Agbaje et al., 2015 | 0 | 0 | * | 0 | 0 | * | * | * | 4/9 |
| Cilasun et al., 2011 | 0 | * | * | 0 | ** | * | * | 0 | 6/9 |
| Frenkel et al., 2015 | 0 | 0 | * | 0 | 0 | * | * | 0 | 3/9 |
| Kohara et al., 2015 | 0 | 0 | * | 0 | 0 | * | * | * | 4/9 |
| Kouwenberg et al., 2016 | 0 | 0 | * | 0 | 0 | * | 0 | * | 3/9 |
| Leung et al., 2012 | 0 | 0 | * | 0 | 0 | * | * | * | 4/9 |
| Leung et al., 2016 | 0 | 0 | * | 0 | 0 | * | * | 0 | 3/9 |
| Mukherjee et al., 2016 | 0 | 0 | * | 0 | 0 | * | * | 0 | 3/9 |
| Pogrel et al., 2004 | 0 | 0 | * | 0 | 0 | * | 0 | * | 3/9 |
| Pedersen et al., 2018 | 0 | 0 | * | 0 | 0 | * | * | * | 4/9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Póvoa, R.C.d.S.; Mourão, C.F.d.A.B.; Geremias, T.C.; Sacco, R.; Guimarães, L.S.; Montemezzi, P.; Cardarelli, A.; Moraschini, V.; Calasans-Maia, M.D.; Louro, R.S. Does the Coronectomy a Feasible and Safe Procedure to Avoid the Inferior Alveolar Nerve Injury during Third Molars Extractions? A Systematic Review. Healthcare 2021, 9, 750. https://doi.org/10.3390/healthcare9060750
Póvoa RCdS, Mourão CFdAB, Geremias TC, Sacco R, Guimarães LS, Montemezzi P, Cardarelli A, Moraschini V, Calasans-Maia MD, Louro RS. Does the Coronectomy a Feasible and Safe Procedure to Avoid the Inferior Alveolar Nerve Injury during Third Molars Extractions? A Systematic Review. Healthcare. 2021; 9(6):750. https://doi.org/10.3390/healthcare9060750
Chicago/Turabian StylePóvoa, Raphaela Capella de Souza, Carlos Fernando de Almeida Barros Mourão, Thaise Cristina Geremias, Roberto Sacco, Ludmilla Silva Guimarães, Pietro Montemezzi, Angelo Cardarelli, Vittorio Moraschini, Mônica Diuana Calasans-Maia, and Rafael Seabra Louro. 2021. "Does the Coronectomy a Feasible and Safe Procedure to Avoid the Inferior Alveolar Nerve Injury during Third Molars Extractions? A Systematic Review" Healthcare 9, no. 6: 750. https://doi.org/10.3390/healthcare9060750