
The Effect of Menopause Hypoestrogenism on Osteogenic Differentiation of Periodontal Ligament Cells (PDLC) and Stem Cells (PDLCs): A Systematic Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Critical Evaluation
3. Results
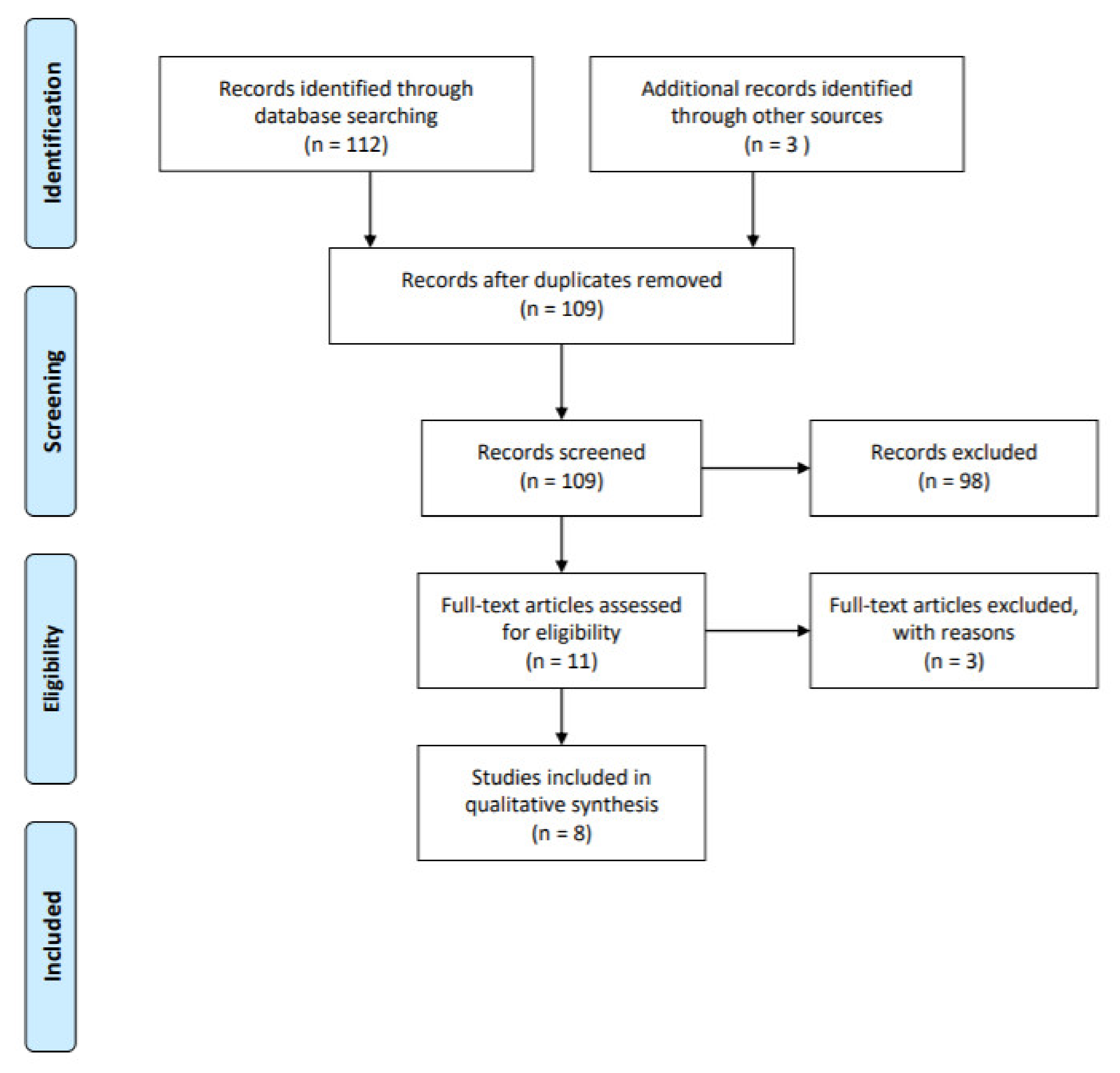
3.1. Summary of the Data Retrieval
3.2. Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bianchi, S.; Macchiarelli, G.; Micara, G.; Aragona, C.; Maione, M.; Nottola, S.A. Ultrastructural and morphometric evaluation of aged cumulus-oocyte- complexes. Ital. J. Anat. Embryol. 2013, 32, 1343–1358. [Google Scholar]
- Cao, M.; Shu, L.; Li, J.; Su, J.; Zhang, W.; Wang, Q.; Guo, T.; Ding, Y. The expression of estrogen receptors and the effects of estrogen on human periodontal ligament cells. Methods Find Exp. Clin. Pharm. 2007, 29, 329–335. [Google Scholar]
- Bianchi, S.; Macchiarelli, G.; Micara, G.; Linari, A.; Boninsegna, C.; Aragona, C.; Rossi, G.; Cecconi, S.; Nottola, S.A. Ultrastructural markers of quality are impaired in human metaphase II aged oocytes: A comparison between reproductive and in vitro aging. J. Assist. Reprod. Genet. 2015, 32, 1343–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, M.; Matsumoto, C.; Hirata, M.; Tominari, T.; Inada, M.; Miyaura, C. The correlation between postmenopausal osteoporosis and inflammatory periodontitis regarding bone loss in experimental models. Exp. Anim. 2012, 61, 183–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nastri, L.; Moretti, A.; Migliaccio, S.; Paoletta, M.; Annunziata, M.; Liguori, S.; Toro, G.; Bianco, M.; Cecoro, G.; Guida, L.; et al. Do Dietary Supplements and Nutraceuticals Have Effects on Dental Implant Osseointegration? A Scoping Review. Nutrients 2020, 12, 268. [Google Scholar] [CrossRef] [Green Version]
- Cecoro, G.; Paoletta, M.; Annunziata, M.; Laino, L.; Nastri, L.; Gimigliano, F.; Liguori, S.; Toro, G.; Moretti, A.; Guida, L.; et al. The role of bone anabolic drugs in the management of periodontitis: A scoping review. Eur. Cell Mater. 2021, 41, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, S.; Nottola, S.A.; Torge, D.; Palmerini, M.G.; Necozione, S.; Macchiarelli, G. Association between Female Reproductive Health and Mancozeb: Systematic Review of Experimental Models. Int. J. Environ. Res. Public Health 2020, 17, 2580. [Google Scholar]
- Weinreb, M.; Rodan, G.A.; Thompson, D.D. Osteopenia in the immobilized rat hind limb is associated with increased bone resorption and decreased bone formation. Bone 1989, 10, 187–194. [Google Scholar] [CrossRef]
- Di Venere, D.; Corsalini, M.; Nardi, G.M.; Laforgia, A.; Grassi, F.R.; Rapone, B.; Pettini, F. Obstructive site localization in patients with Obstructive Sleep Apnea Syndrome: A comparison between otolaryngologic data and cephalometric values. Oral Implantol. 2017, 10, 295–310. [Google Scholar] [CrossRef]
- Fullmer, H.M.; Sheetz, J.H.; Narkates, A.J. Oxytalan connective tissue fibers: A review. J Oral Pathol. 1974, 3, 291–316. [Google Scholar] [CrossRef]
- Johnson, R.B.; Pylypas, S.P. A re-evaluation of the distribution of the elastic meshwork within the periodontal ligament of the mouse. J. Periodontal. Res. 1992, 27, 239–249. [Google Scholar] [CrossRef]
- Parkar, M.H.; Newman, H.N.; Olsen, I. Polymerase chain reaction analysis of oestrogen and androgen receptor expression in human gingival and periodontal tissue. Arch Oral Biol. 1996, 41, 979–983. [Google Scholar] [CrossRef]
- Jonsson, D.; Andersson, G.; Ekblad, E.; Liang, M.; Bratthall, G.; Nilsson, B.O. Immunocytochemical demonstration of estrogen receptor beta in human periodontal ligament cells. Arch Oral Biol. 2004, 49, 85–88. [Google Scholar] [CrossRef]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Converti, I.; Grassi, F.R.; Santacroce, L.; Topi, S.; Gnoni, A.; Scacco, S.; Scarano, A.; et al. The Effect of Gaseous Ozone Therapy in Conjunction with Periodontal Treatment on Glycated Hemoglobin Level in Subjects with Type 2 Diabetes Mellitus: An Unmasked Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 5467. [Google Scholar] [CrossRef]
- Riggs, B.L. The mechanisms of estrogen regulation of bone resorption. J. Clin. Investig. 2000, 106, 1203–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nojima, N.; Kobayashi, M.; Shionome, M.; Takahashi, N.; Suda, T.; Hasegawa, K. Fibroblastic cells derived from bovine periodontal ligaments have the phenotypes of osteoblasts. J. Periodontal. Res. 1990, 25, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Chien, H.H.; Lin, W.L.; Cho, M.I. Expression of TGF-beta isoforms and their receptors during mineralized nodule formation by rat periodontal ligament cells in vitro. J. Periodontal. Res. 1999, 34, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Mariotti, A.J. Estrogen and extracellular matrix influence human gingival fibroblast proliferation and protein production. J. Periodontol. 2005, 76, 1391–1397. [Google Scholar] [CrossRef]
- Ejiri, S.; Toyooka, E.; Tanaka, M.; Anwar, R.B.; Kohno, S. Histological and histomorphometrical changes in rat alveolar bone following antagonistic tooth extraction and/or ovariectomy. Arch Oral Biol. 2006, 51, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Quaglia, E.; Moscufo, L.; Corsalini, M.; Coscia, D.; Sportelli, P.; Cantatore, F.; De Rinaldis, C.; Rapone, B.; Carossa, M.; Carossa, S. Polyamide vs silk sutures in the healing of postextraction sockets: A split mouth study. Oral Implantol. 2018, 11, 115–120. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar]
- Ou, Q.; Wang, X.; Wang, Y.; Wang, Y.; Lin, X. Oestrogen retains human periodontal ligament stem cells stemness in long-term culture. Cell Prolif. 2018, 51, e12396. [Google Scholar]
- Ling-Ling, E.; Xu, W.H.; Feng, L.; Liu, Y.; Cai, D.Q.; Wen, N.; Zheng, W.J. Estrogen enhances the bone regeneration potential of periodontal ligament stem cells derived from osteoporotic rats and seeded on nano-hydroxyapatite/collagen/poly(L-lactide). Int. J. Mol. Med. 2016, 37, 1475–1486. [Google Scholar]
- Cai, C.; Yuan, G.J.; Huang, Y.; Yang, N.; Chen, X.; Wen, L.; Wang, X.; Zhang, L.; Ding, Y. Estrogen-related receptor α is involved in the osteogenic differentiation of mesenchymal stem cells isolated from human periodontal ligaments. Int. J. Mol. Med. 2013, 31, 1195–1201. [Google Scholar]
- Wang, Y.; Zheng, Y.; Wang, Z.; Li, J.; Wang, Z.; Zhang, G.; Yu, J. 10(-7) m 17β-oestradiol enhances odonto/osteogenic potency of human dental pulp stem cells by activation of the NF-κB pathway. Cell Prolif. 2013, 46, 677–684. [Google Scholar]
- Zhang, B.; Li, Y.; Zhou, Q.; Ding, Y. Estrogen deficiency leads to impaired osteogenic differentiation of periodontal ligament stem cells in rats. Tohoku J. Exp. Med. 2011, 223, 177–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Zhang, R.; Wang, G.; Ding, Y. Oestrogen receptors are involved in the osteogenic differentiation of periodontal ligament stem cells. Biosci Rep. 2011, 31, 117–124. [Google Scholar]
- Liang, L.; Yu, J.F.; Wang, Y.; Wang, G.; Ding, Y. Effect of estrogen receptor beta on the osteoblastic differentiation function of human periodontal ligament cells. Arch Oral Biol. 2008, 53, 553–557. [Google Scholar] [CrossRef]
- Liang, L.; Yu, J.F.; Wang, Y.; Ding, Y. Estrogen Regulates Expression of Osteoprotegerin and RANKL in Human Periodontal Ligament Cells Through Estrogen Receptor Beta. J. Periodontol. 2008, 79, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Ferrara, E.; Corsalini, M.; Qorri, E.; Converti, I.; Lorusso, F.; Delvecchio, M.; Gnoni, A.; Scacco, S.; Scarano, A. Inflammatory Status and Glycemic Control Level of Patients with Type 2 Diabetes and Periodontitis: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 3018. [Google Scholar] [CrossRef]
- Li, Y.; Yan, M.; Wang, Z.; Zheng, Y.; Li, J.; Ma, S.; Liu, G.; Yu, J. 17beta-estradiol promotes the odonto/osteogenic differentiation of stem cells from apical papilla via mitogen-activated protein kinase pathway. Stem Cell Res. 2014, 5, 125. [Google Scholar] [CrossRef] [Green Version]
- Levy, G.G.; Mailland, M.L. Histologic study of the effects of occlusal hypofunction following antagonist tooth extraction in the rat. J. Periodontol. 1980, 51, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Ferrara, E.; Montemurro, N.; Converti, I.; Loverro, M.; Loverro, M.T.; Gnoni, A.; Scacco, S.; Siculella, L.; Corsalini, M.; et al. Oral microbiome and preterm birth: Correlation or coincidence? A narrative review. Open Access Maced. J. Med. Sci. 2020, 8, 123–132. [Google Scholar] [CrossRef]


{kind=link}
| Author and Year of Publication. | Main Characteristics of Models | Cell Lines Origin | Post-OVX Period (months) | Outcomes | Method for the Measurement of Bone Density and/or Oestrogen Deficiency |
|---|---|---|---|---|---|
| OU Q. et al., 2018 [22] | 12 caries-free premolars extracted for orthodontic reasons from donors aged between 18 and 20 | hPDLSCs | NR | Effects of E2 on hPDLSCs | Quantitative real-time reverse transcription polymerase chain reaction (RT-PCR); Western blotting; Immunofluorescence staining analysis |
| LING-LING E. et al., 2016 [23] | 48 healthy Sprague-Dawley female rats were randomly divided into three groups: OVX group; OVX + 17β oestradiol (E2) group, and Sham group | PDLSCs cells of animal origin | 3 | Effect of oestrogen on osteogenic differentiation in the PLDSCs; The role of oestrogen in regulating the mRNA expression levels of ALP, OCN, ERα and ERβ in the PLDSCs | Immunochemistry assay; Scanning electron microscopy (SEM) analysis; Real-Time reverse transcription polymerase Chain Reaction; Histological and morphometric study |
| CAI C. et al., 2013 [24] | Periodontal ligament (PDL) tissues were harvested from healthy premolars extracted for orthodontic reasons. Seven donors (12-16 years of age; four females and three males) | hPDLSCs | NR | ALP activity and OCN level of PDLSCs in the presence of oestrogens | Real-time reverse transcription polymerase chain reaction; Immunohistochemical analysis |
| WANG Y. et al., 2013 [25] | 12 caries-free human premolars extracted from six patients due to the orthodontic reasons | human DPSCs | NR | Effects of 17b-oestradiol on odonto/osteogenic differentiation of DPSCs | Real-time reverse transcription polymerase chain reaction |
| ZHANG B. et al., 2011 [26] | 20 Sprague Dawley (SD) rats were randomly divided into two groups: to the OVX group and Sham group. | PDLSCs cells of animal origin | 3 | The effect of oestrogen depletion on osteogenic differentiation of PDLSCs | Real-Time polymerase Chain Reaction |
| PAN F. et al., 2011 [27] | Partially impacted third molars (n = 6) were collected from three female individuals aged 18, 19 and 22 | human PDLSCs | NR | Effect of oestrogens on the osteogenic differentiation of PDLSCs in vitro | Real-Time polymerase Chain Reaction; Western Blot analysis Immunocytochemical analysis |
| LIANG L. et al., 2008 [28] | Premolars extracted from 4 premolars Donor’s age: 12 to 14 years old | PDL cells of human origin (hPDL) obtained from the middle of tooth root | NR | The effect of oestrogen depletion on osteogenic differentiation of hPDL cells The effect of oestrogen receptor beta (ERβ) inhibition on osteoblastic differentiation function of human periodontal ligament cells (hPDL) | Real-Time polymerase Chain Reaction; Western Blot analysis |
| LIANG L. et al., 2008 [29] | Premolars extracted from 4 premolars. Donor’s age: 10 to 12 years old | PDL cells of human origin (hPDL) obtained from the middle of tooth root | NR | The effect of oestrogen on the expression of OPG and RANKL in human PDL (hPDL) | Short interfering RNA technique |
| Study | Sample Size Calculation | Random Allocation to Treatment | Blinded Assessment of Outcomes | Compliance With Animal/Human Welfare Regulations | Conflicts of Interest Disclosed | Peer-Reviewed Publication | Quality Score |
|---|---|---|---|---|---|---|---|
| OU Q. et al., 2018 [22] | N | N | N | Y | N | Y | 2 |
| LING-LING E. et al., 2016 [23] | N | Y | N | Y | N | Y | 3 |
| CAI C. et al., 2013 [24] | N | Y | N | N | N | Y | 2 |
| WANG Y. et al., 2013 [25] | N | Y | N | Y | N | Y | 3 |
| ZHANG B. et al., 2011 [26] | N | Y | N | Y | Y | Y | 4 |
| PAN F. et al., 2011 [27] | N | Y | N | Y | Y | Y | 4 |
| LIANG L. et al., 2008 [28] | N | N | N | N | N | Y | 1 |
| LIANG L. et al., 2008 [29] | N | Y | N | Y | N | Y | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Naro, E.; Loverro, M.; Converti, I.; Loverro, M.T.; Ferrara, E.; Rapone, B. The Effect of Menopause Hypoestrogenism on Osteogenic Differentiation of Periodontal Ligament Cells (PDLC) and Stem Cells (PDLCs): A Systematic Review. Healthcare 2021, 9, 572. https://doi.org/10.3390/healthcare9050572
Di Naro E, Loverro M, Converti I, Loverro MT, Ferrara E, Rapone B. The Effect of Menopause Hypoestrogenism on Osteogenic Differentiation of Periodontal Ligament Cells (PDLC) and Stem Cells (PDLCs): A Systematic Review. Healthcare. 2021; 9(5):572. https://doi.org/10.3390/healthcare9050572
Chicago/Turabian StyleDi Naro, Edoardo, Matteo Loverro, Ilaria Converti, Maria Teresa Loverro, Elisabetta Ferrara, and Biagio Rapone. 2021. "The Effect of Menopause Hypoestrogenism on Osteogenic Differentiation of Periodontal Ligament Cells (PDLC) and Stem Cells (PDLCs): A Systematic Review" Healthcare 9, no. 5: 572. https://doi.org/10.3390/healthcare9050572