
Dental Trauma Management in a Young Teenager through Endodontics and Implantology: A Case Report

 , , ,
, , ,
Abstract
:1. Introduction
2. Case Report
2.1. Traumatology and Treatment
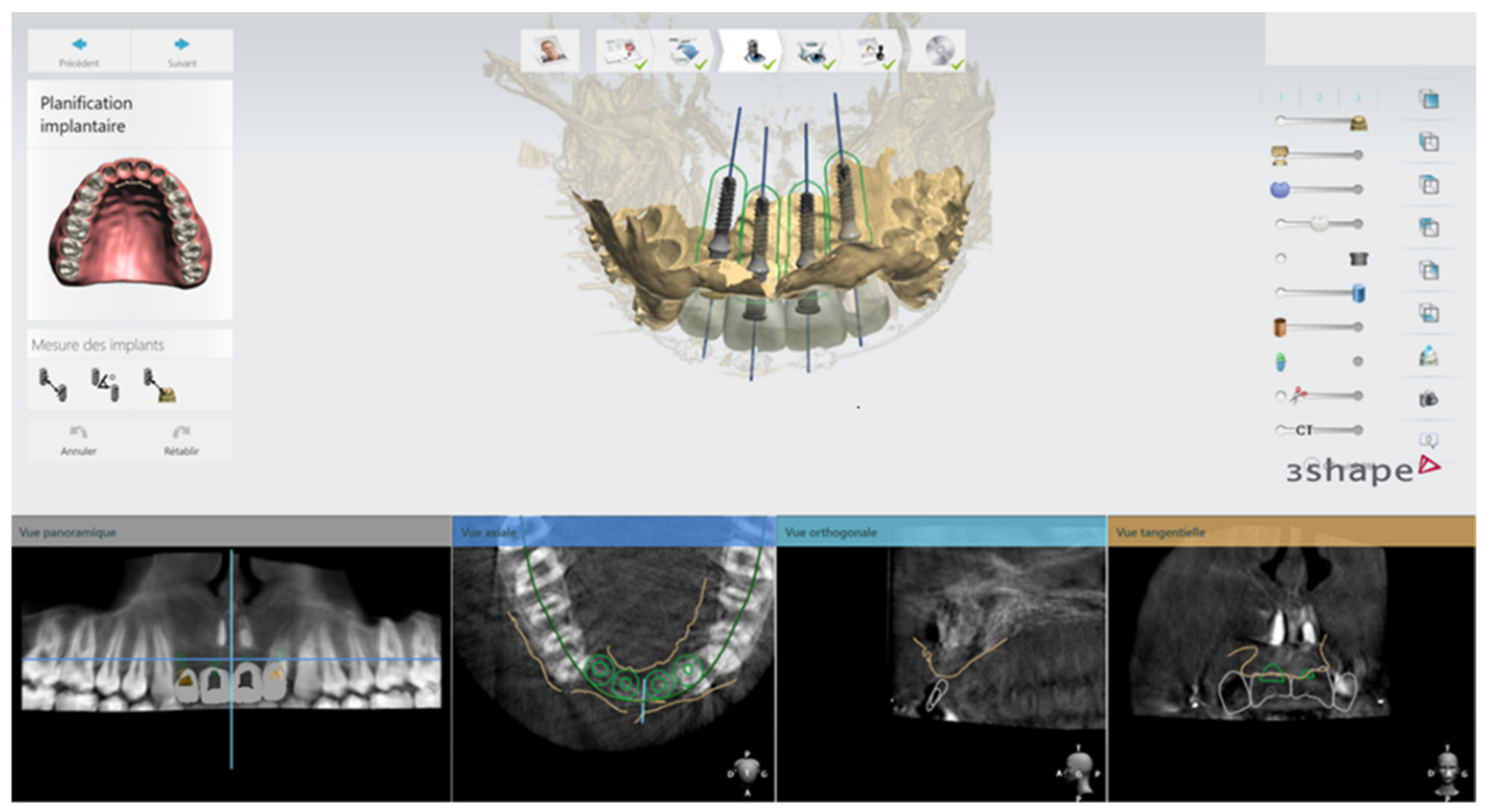
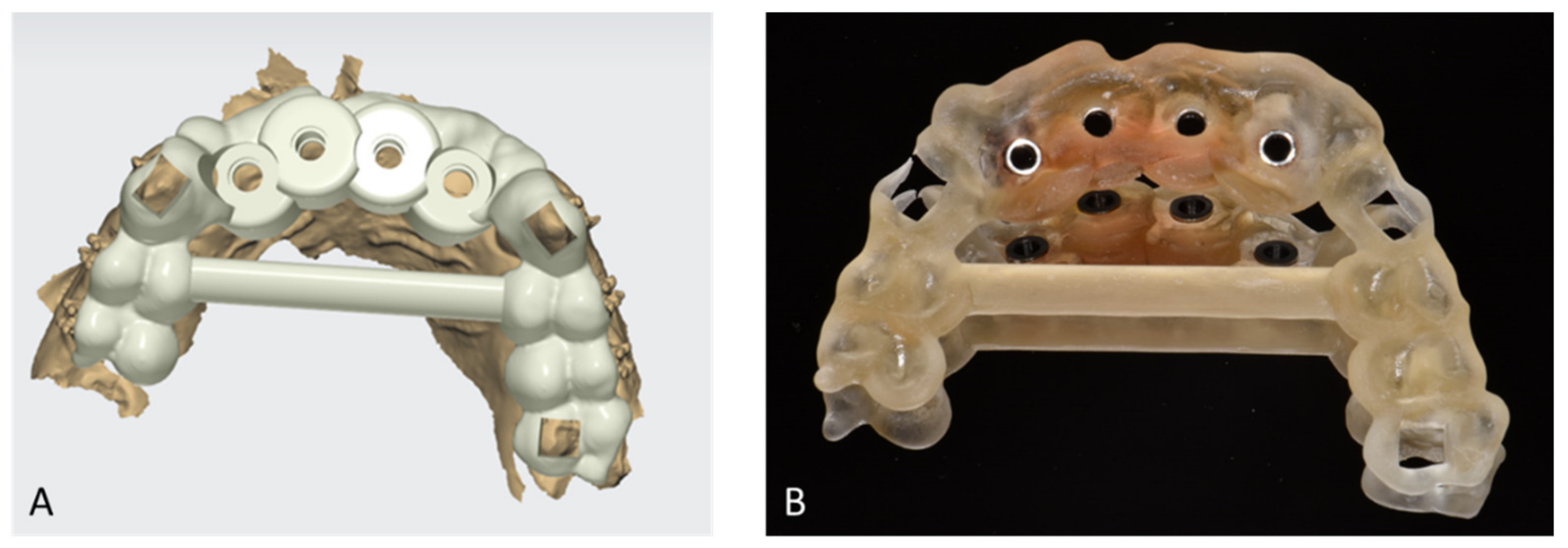
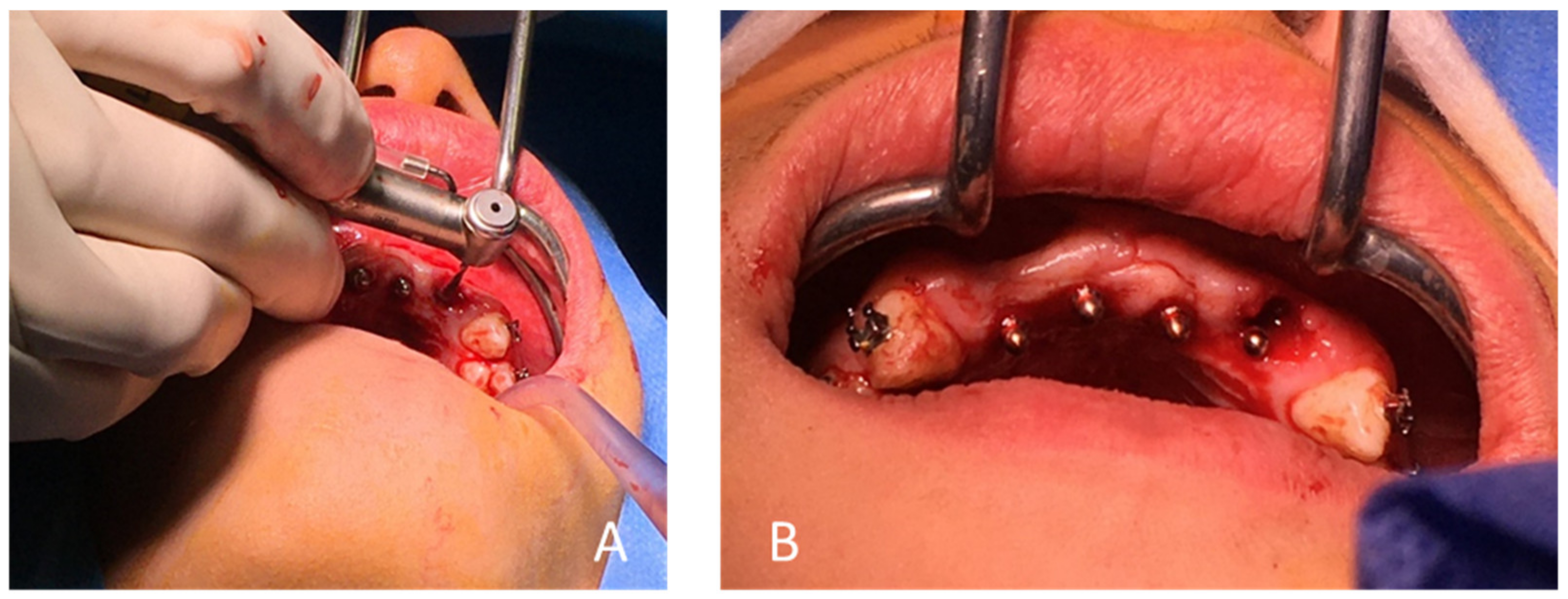
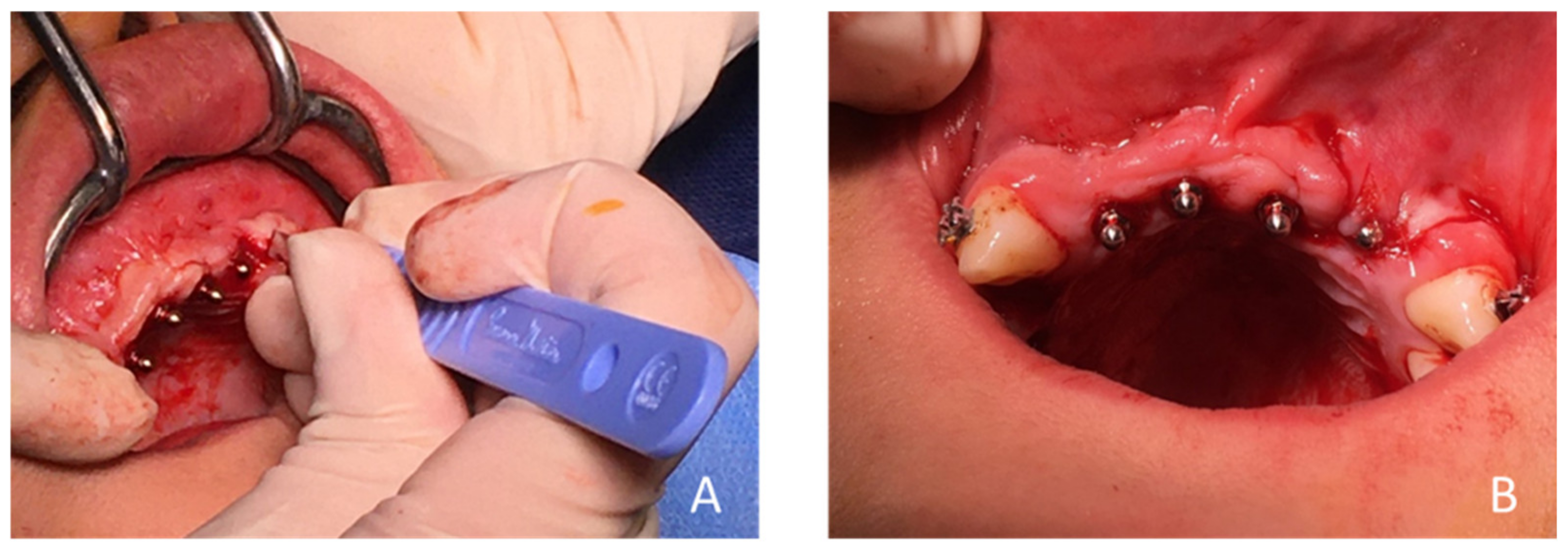
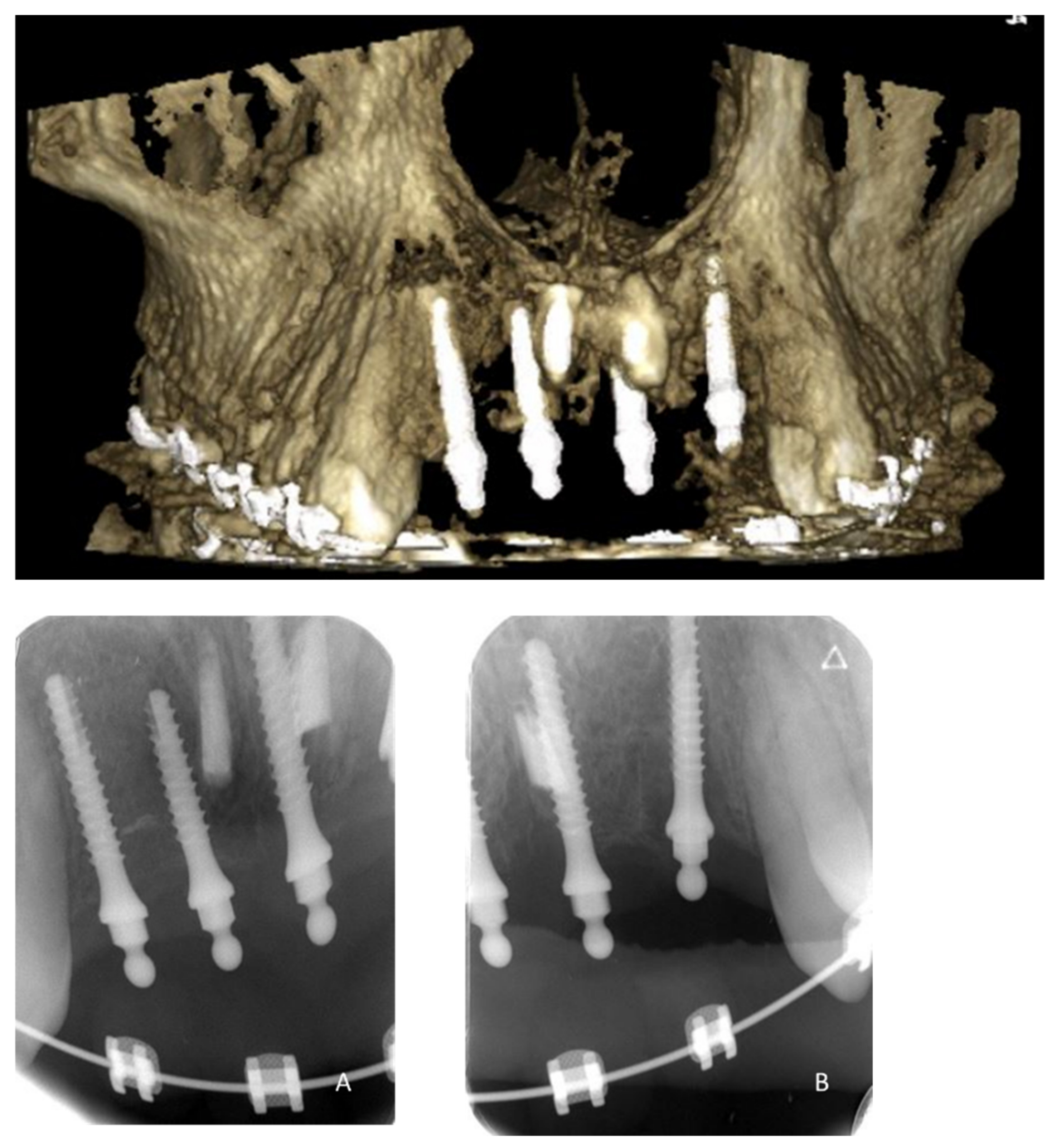
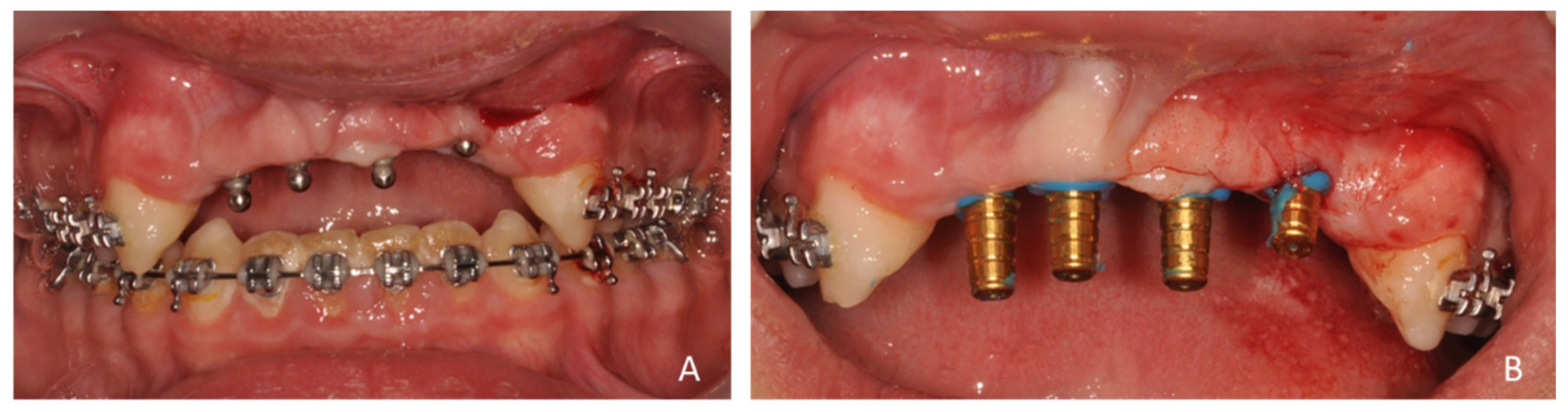
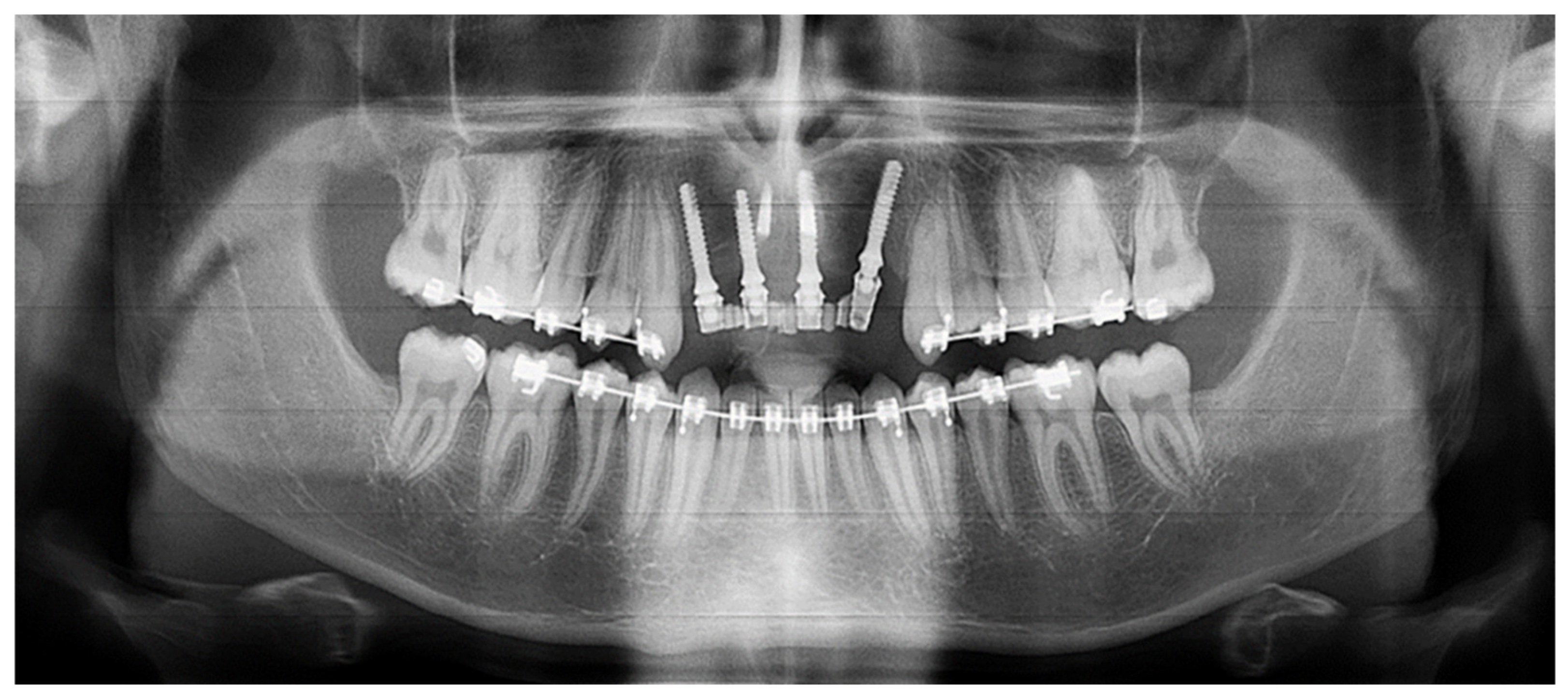
2.2. Second Step: Surgical Phase
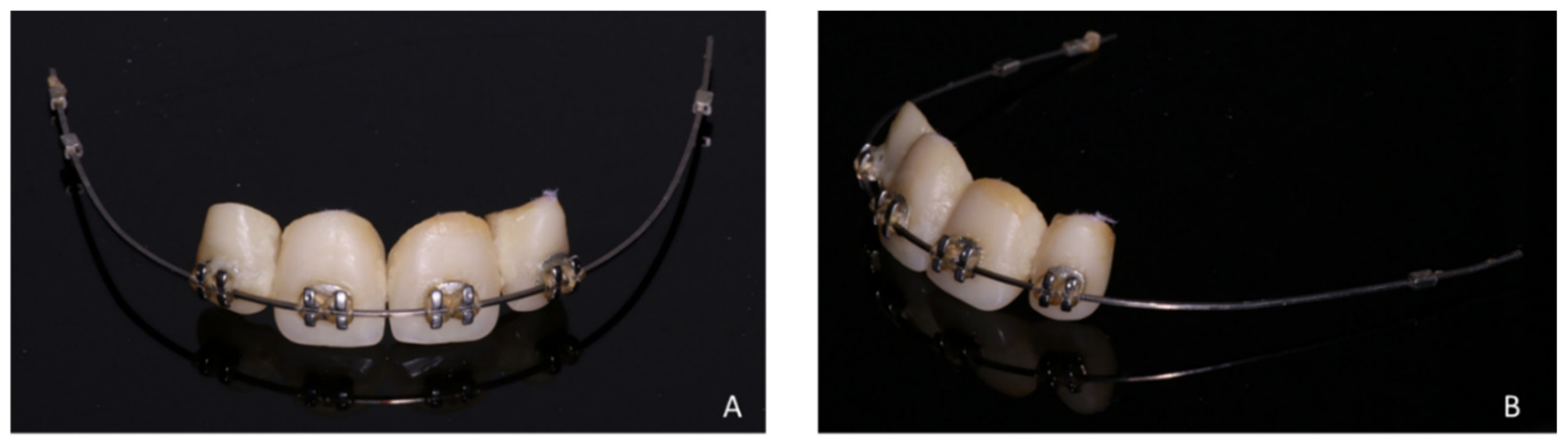
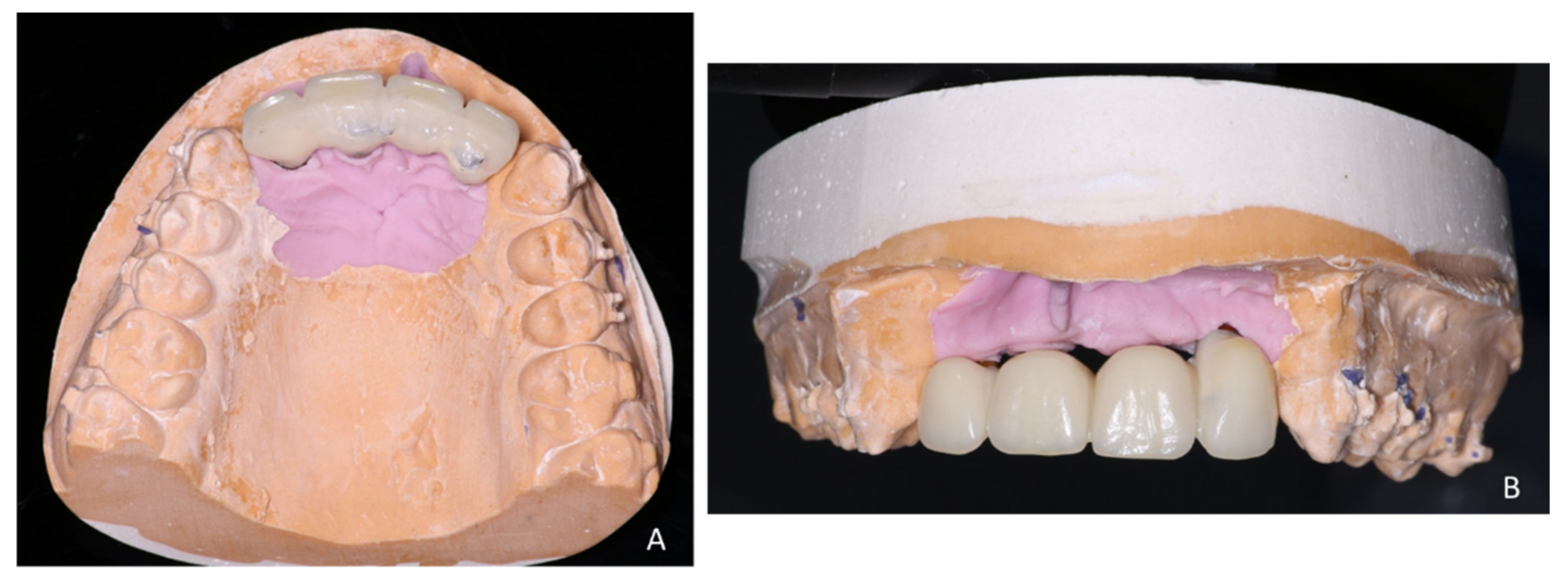
2.3. Third Step: Prosthetic Phase
3. Discussion
4. Conclusions
Authors Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacLeod, S.P.R.; Rudd, T.C. Update on the Management of Dentoalveolar Trauma. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Levin, L.; Ashkenazi, M. Treatment Options of Untreatable Traumatized Anterior Maxillary Teeth for Future Use of Dental Implantation. Implant Dent. 2004, 13, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Petersson, E.E.; Andersson, L.; Sörensen, S. Traumatic Oral vs Non-Oral Injuries. Swed. Dent. J. 1997, 21, 55–68. [Google Scholar] [PubMed]
- Bastone, E.B.; Freer, T.J.; McNamara, J.R. Epidemiology of Dental Trauma: A Review of the Literature. Aust. Dent. J. 2000, 45, 2–9. [Google Scholar] [CrossRef]
- Coste, S.C.; Silva, E.F.E.; Santos, L.C.M.; Barbato Ferreira, D.A.; de Souza Côrtes, M.I.; Colosimo, E.A.; Bastos, J.V. Survival of Replanted Permanent Teeth after Traumatic Avulsion. J. Endod. 2020, 46, 370–375. [Google Scholar] [CrossRef]
- Robertson, A.; Andreasen, F.M.; Andreasen, J.O.; Norén, J.G. Long-Term Prognosis of Crown-Fractured Permanent Incisors. The Effect of Stage of Root Development and Associated Luxation Injury. Int. J. Paediatr. Dent. 2000, 10, 191–199. [Google Scholar] [CrossRef]
- Wang, G.; Wang, C.; Qin, M. A Retrospective Study of Survival of 196 Replanted Permanent Teeth in Children. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2019, 35, 251–258. [Google Scholar] [CrossRef]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: 1. Fractures and Luxations. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef]
- Fouad, A.F.; Abbott, P.V.; Tsilingaridis, G.; Cohenca, N.; Lauridsen, E.; Bourguignon, C.; O’Connell, A.; Flores, M.T.; Day, P.F.; Hicks, L.; et al. International Association of Dental Traumatology Guidelines for the Management of Traumatic Dental Injuries: 2. Avulsion of Permanent Teeth. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2020, 36, 331–342. [Google Scholar] [CrossRef]
- Darcey, J.; Eldridge, D. Fifty Years of Dental Implant Development: A Continuous Evolution. Dent. Hist. Lindsay Club Newsl. 2016, 61, 75–92. [Google Scholar]
- Block, M.S. Dental Implants: The Last 100 Years. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2018, 76, 11–26. [Google Scholar] [CrossRef]
- Kamatham, R.; Avisa, P.; Vinnakota, D.N.; Nuvvula, S. Adverse Effects of Implants in Children and Adolescents: A Systematic Review. J. Clin. Pediatr. Dent. 2019, 43, 69–77. [Google Scholar] [CrossRef]
- Bohner, L.; Hanisch, M.; Kleinheinz, J.; Jung, S. Dental Implants in Growing Patients: A Systematic Review. Br. J. Oral Maxillofac. Surg. 2019, 57, 397–406. [Google Scholar] [CrossRef]
- Chesterman, J.; Chauhan, R.; Patel, M.; Chan, M.F.W.-Y. The Management of Traumatic Tooth Loss with Dental Implants: Part 1. Br. Dent. J. 2014, 217, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Heithersay, G.S. Invasive Cervical Resorption: An Analysis of Potential Predisposing Factors. Quintessence Int. Berl. Ger. 1985 1999, 30, 83–95. [Google Scholar]
- Heithersay, G.S. Invasive Cervical Resorption Following Trauma. Aust. Endod. J. 1999, 25, 79–85. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; McNamara, J.A. An Improved Version of the Cervical Vertebral Maturation (CVM) Method for the Assessment of Mandibular Growth. Angle Orthod. 2002, 72, 316–323. [Google Scholar] [CrossRef]
- Siboni, F.; Taddei, P.; Zamparini, F.; Prati, C.; Gandolfi, M.G. Properties of BioRoot RCS, a Tricalcium Silicate Endodontic Sealer Modified with Povidone and Polycarboxylate. Int. Endod. J. 2017, 50 (Suppl. 2), e120–e136. [Google Scholar] [CrossRef] [Green Version]
- Murphy, W.M. An in Vitro Model for Testing Biocompatibility of Endodontic Materials to Bone. Biomaterials 1985, 6, 427–430. [Google Scholar] [CrossRef]
- Bodrumlu, E. Biocompatibility of Retrograde Root Filling Materials: A Review. Aust. Endod. J. 2008, 34, 30–35. [Google Scholar] [CrossRef]
- Sales, P.H.H.; Oliveira-Neto, O.B.; Torres, T.S.; de Lima, F.J.C. Effectiveness of Dental Implants Placed in Bone Graft Area of Cleft Patients. Int. J. Oral Maxillofac. Surg. 2019, 48, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Shatkin, T.E.; Petrotto, C.A. Mini Dental Implants: A Retrospective Analysis of 5640 Implants Placed over a 12-Year Period. Compend. Contin. Educ. Dent. Jamesburg NJ 1995 2012, 33, 2–9. [Google Scholar]
- Shatkin, T.E.; Shatkin, S.; Oppenheimer, B.D.; Oppenheimer, A.J. Mini Dental Implants for Long-Term Fixed and Removable Prosthetics: A Retrospective Analysis of 2514 Implants Placed over a Five-Year Period. Compend. Contin. Educ. Dent. Jamesburg NJ 1995 2007, 28, 92–99. [Google Scholar]
- Jackson, B.J. Small-Diameter Implants: A 7-Year Retrospective Study. J. Oral Implantol. 2017, 43, 125–129. [Google Scholar] [CrossRef] [PubMed]























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment | ||||
|---|---|---|---|---|
| Date/Events | Teeth | |||
| 12 (Lateral Upper Right Incisor) | 11 (Central Upper Right Incisor) | 21 (Central Upper Left Incisor) | 22 (Lateral Upper Left Incisor) | |
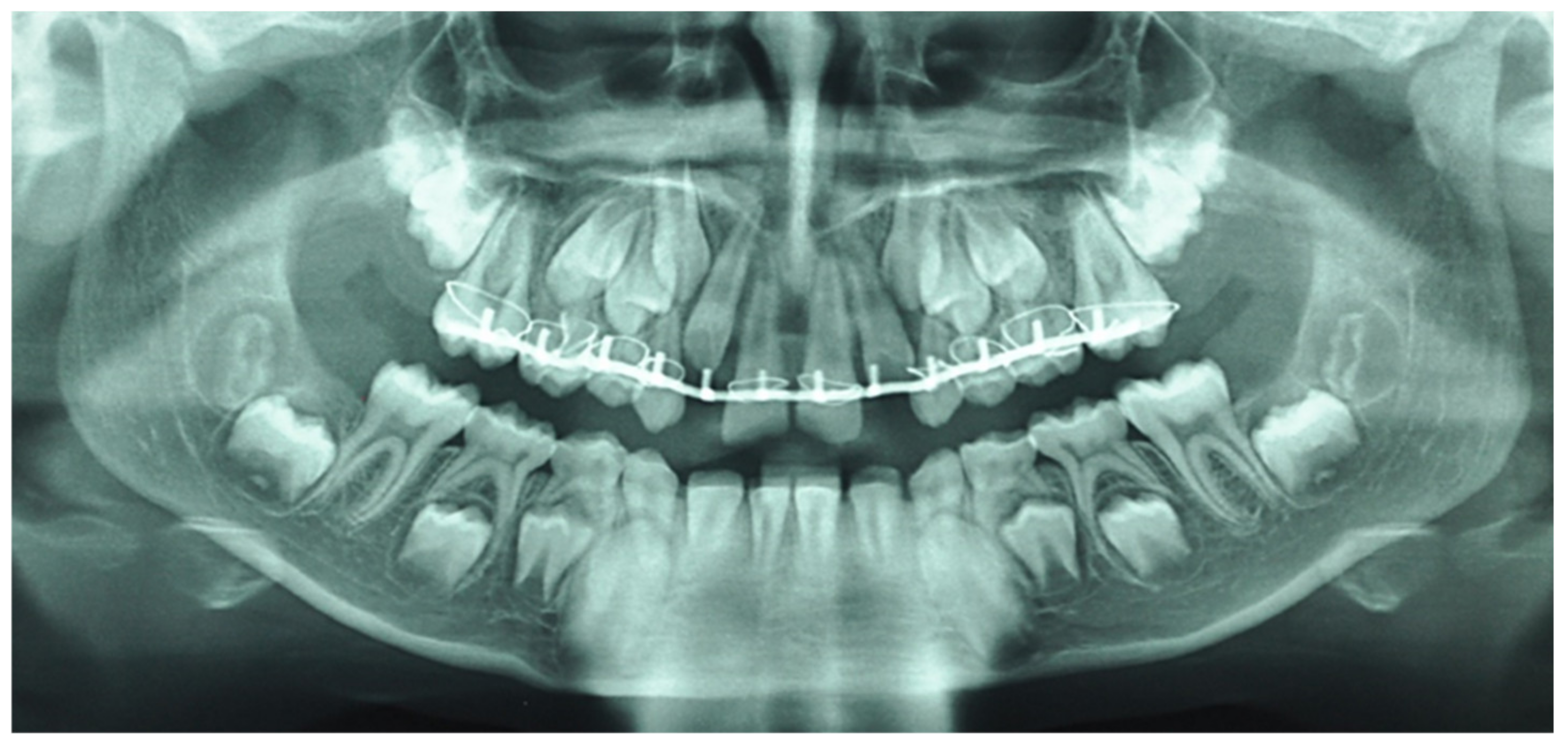
| August 2015: Maxilla-facial trauma, Dental traumatology, Alveolar fracture | Intrusive luxation | Complete extrusive luxation | Intrusive luxation | |
| August 2015: General Anesthesia | Reducing of extrusive luxations | |||
| Dautrey arch placed with inter-dental fixation using 2.0 steel wire between both first upper molar teeth to allow reduction in the associated alveolar fracture | ||||
| October 2015: Orthodontics consultation | Severe mobility and root resorption | |||
| Removal of the Dautrey arch and replacement with a fixed multi-fastener maxillary appliance | ||||
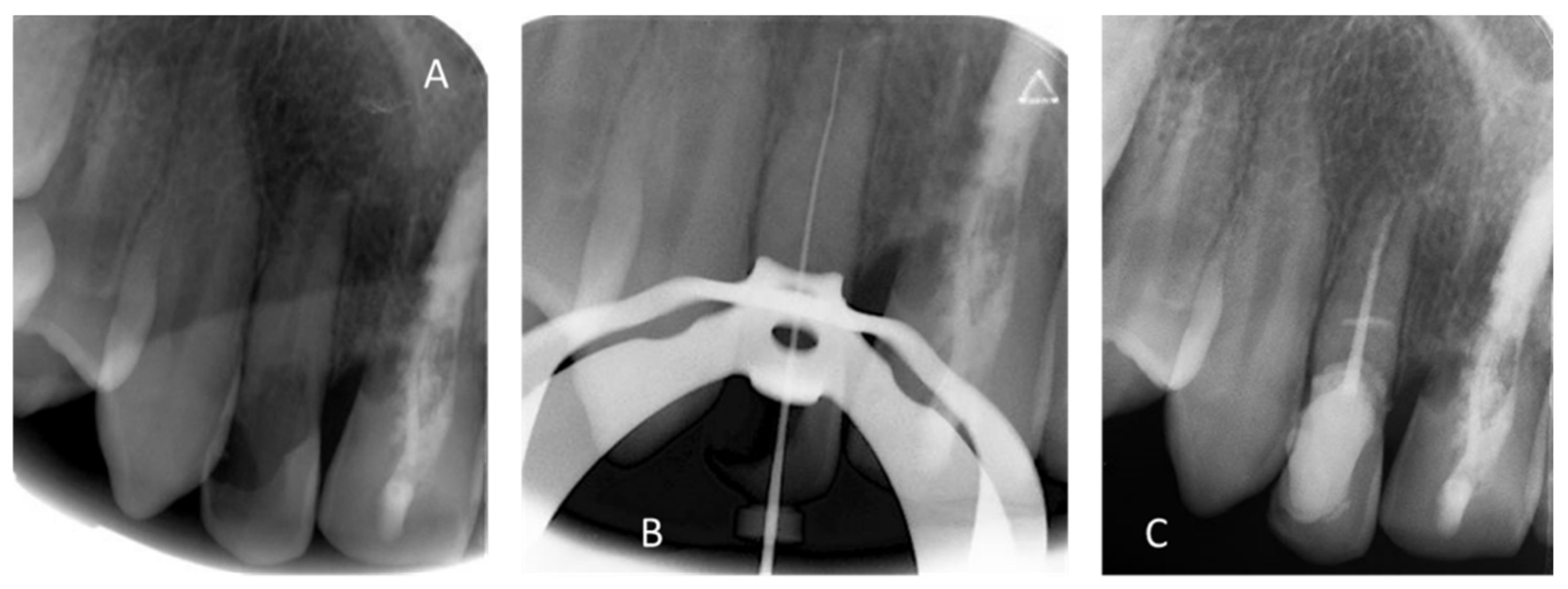
| December 2015 (Dentist treatment) | Endodontic treatment with calcium hydroxide and Gutta Percha | |||
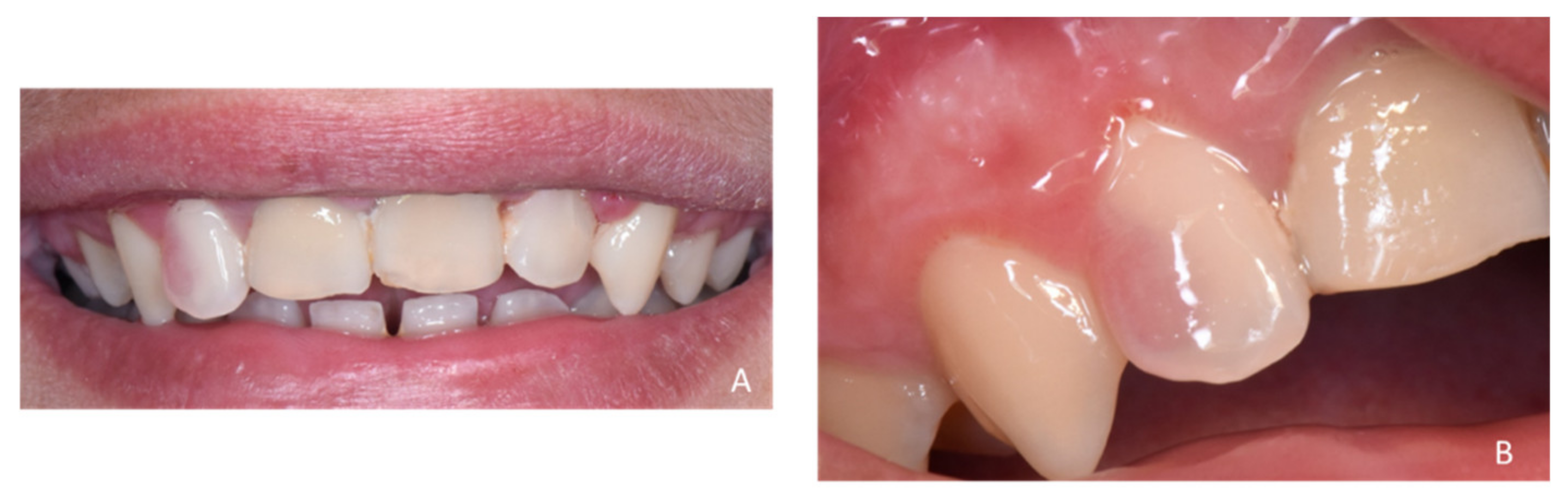
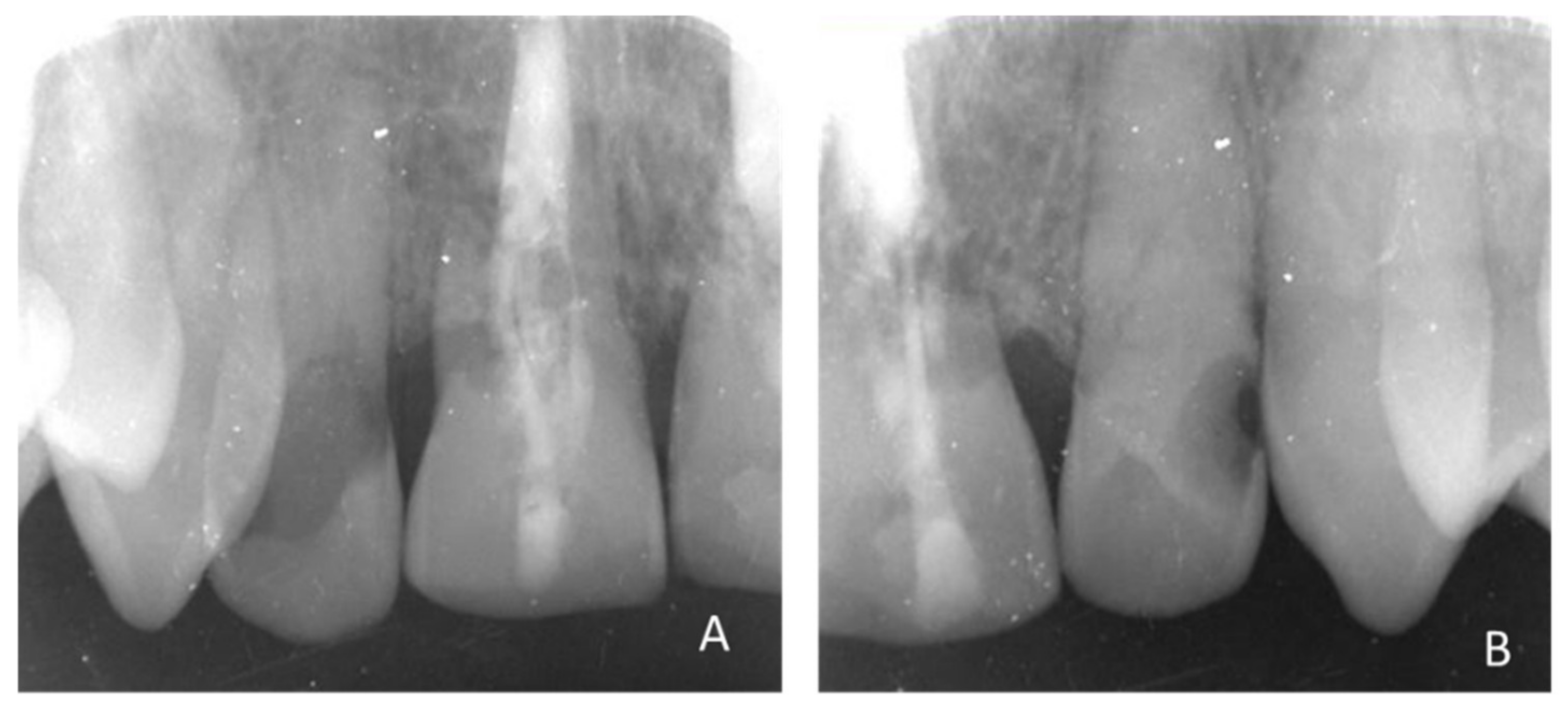
| April 2018 | “pink spot” lesions/invasive cervical resorption of class III according to Heithersay classification [15,16]/negative response to vitality test | Slight mobility/complete root inflammatory resorption around the gutta percha filling | “pink spot” lesions/invasive cervical resorption of class II according to Heithersay classification [15,16]/negative response to vitality test | |
| Figure 3, Figure 4 and Figure 5 | ||||
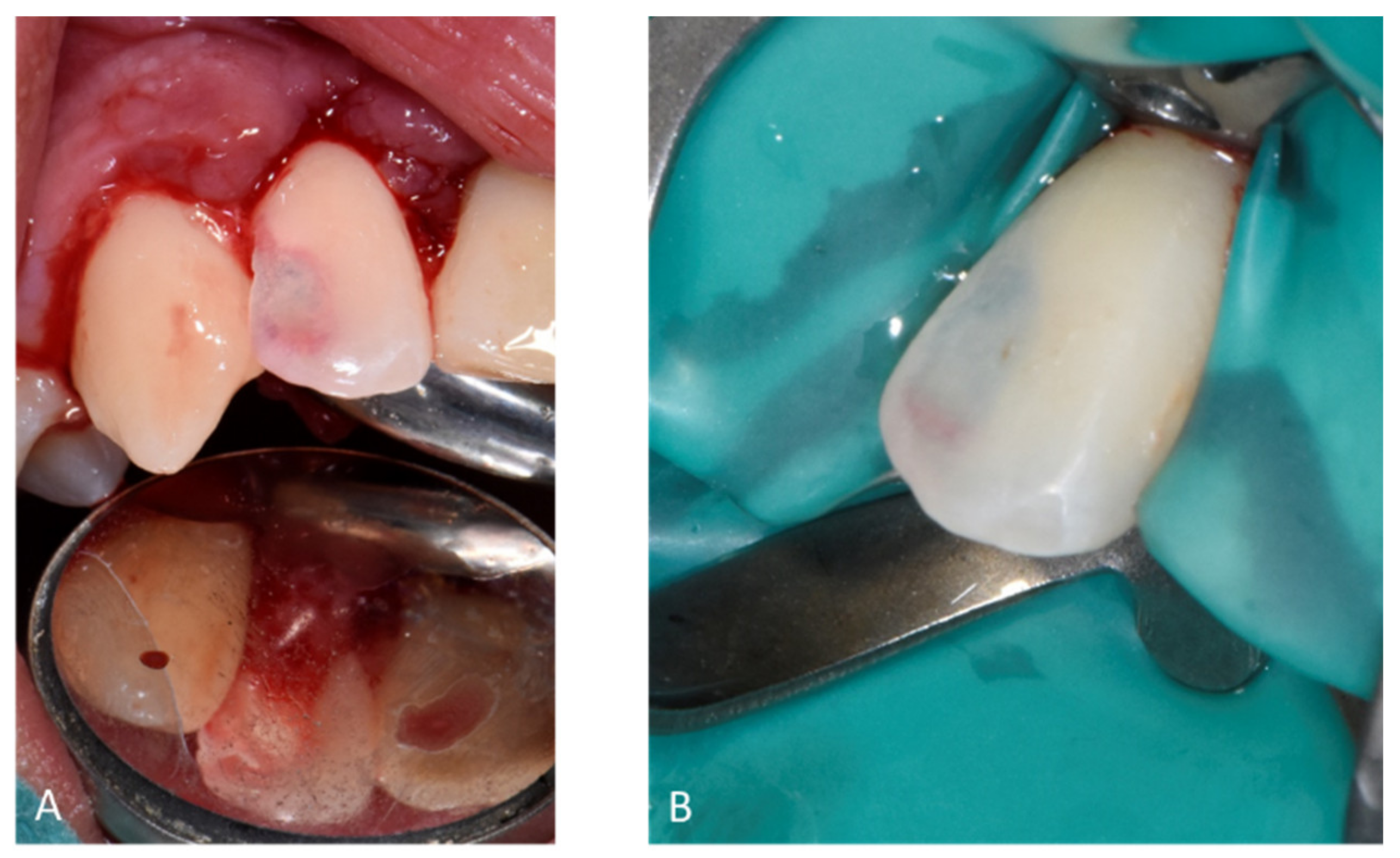
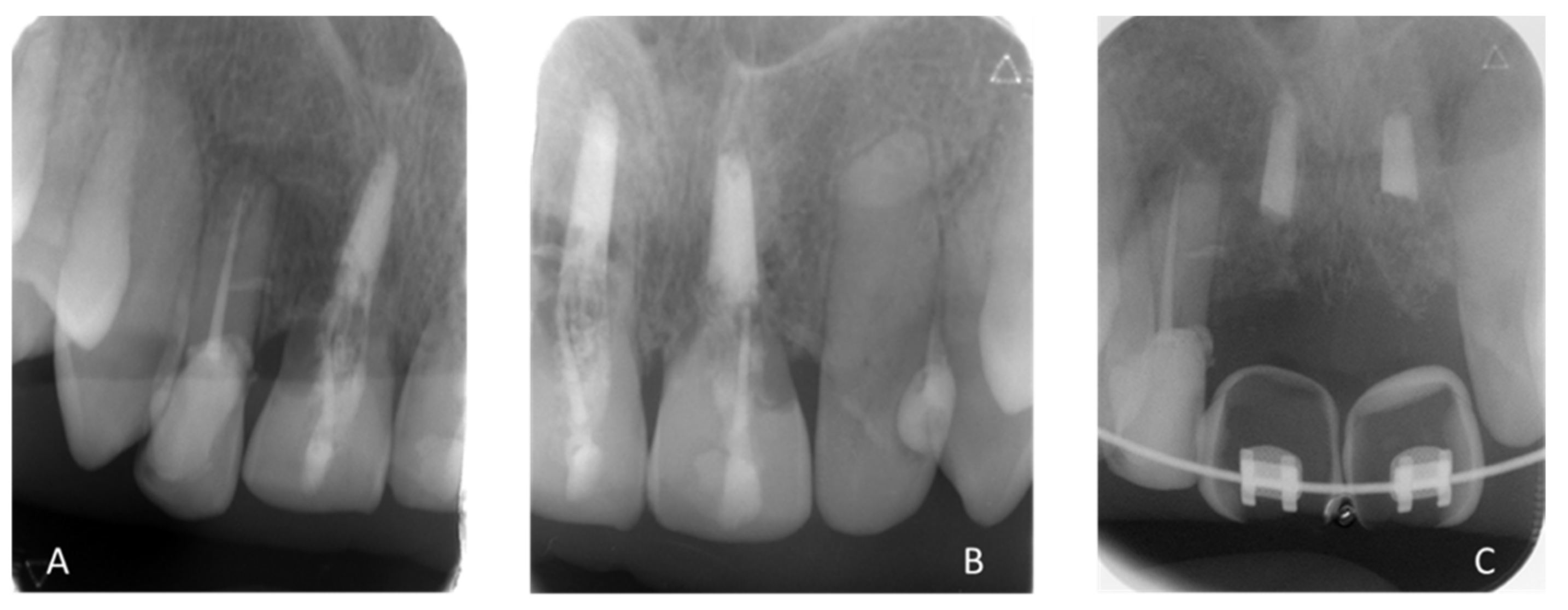
| May 2018 | Buccal and palatal flap of upper right anterior teeth without discharge/curettage of the granulation tissue/endodontic (lesion was of interest to the pulp)/restoration with a composite resin under dam/endodontics treatment with sodium hypochlorite irrigation and obturation at BioRoot™ and calibrated cone | Buccal flap without discharge from upper left anterior teeth/curettage of the granulation tissue/restoration with a composite resin under dam | ||
| Preservation of the bone capital until the implant solution | ||||
| Figure 6 and Figure 7 | ||||
| May 2019: Orthodontic treatment for skeletal class II | Avulsion | |||
| Maintaining space for future implant replacement with resin crown temporization on the orthodontic arch | ||||
| Figure 8 | ||||
| Summer 2019 | Two infectious episodes despite an endodontic re-treatment | |||
| January 2020 | Avulsion | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munoz-Sanchez, M.-L.; Decerle, N.; Devoize, L.; Nicolas, E.; Cousson, P.-Y.; Veyrune, J.-L. Dental Trauma Management in a Young Teenager through Endodontics and Implantology: A Case Report. Healthcare 2021, 9, 542. https://doi.org/10.3390/healthcare9050542
Munoz-Sanchez M-L, Decerle N, Devoize L, Nicolas E, Cousson P-Y, Veyrune J-L. Dental Trauma Management in a Young Teenager through Endodontics and Implantology: A Case Report. Healthcare. 2021; 9(5):542. https://doi.org/10.3390/healthcare9050542
Chicago/Turabian StyleMunoz-Sanchez, Marie-Laure, Nicolas Decerle, Laurent Devoize, Emmanuel Nicolas, Pierre-Yves Cousson, and Jean-Luc Veyrune. 2021. "Dental Trauma Management in a Young Teenager through Endodontics and Implantology: A Case Report" Healthcare 9, no. 5: 542. https://doi.org/10.3390/healthcare9050542