
Oral Health Impact Profile in Orthodontic Patients with Ectopic Canine: A Prospective Clinical Intervention of Four Treatment Modalities



Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ackerman, M.B. Enhancement Orthodontics: Theory and Practice; Wiley-Blackwell: Hoboken, NJ, USA, 2007. [Google Scholar]
- Talic, N.F. Adverse effects of orthodontic treatment: A clinical perspective. Saudi Dent. J. 2011, 23, 55–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, P.Y.-W.; Wong, R.W.-K. Risks and complications in orthodontic treatment. Hong Kong Dent. J. 2006, 3, 15–22. [Google Scholar]
- Fernandes, M.J.; Ruta, D.A.; Ogden, G.R.; Pitts, N.B.; Ogston, S.A. Assessing oral health-related quality of life in general dental practice in Scotland: Validation of the OHIP-14. Community Dent. Oral Epidemiol. 2006, 34, 53–62. [Google Scholar] [CrossRef]
- Javidi, H.; Vettore, M.; Benson, P.E. Does orthodontic treatment before the age of 18 years improve oral health-related quality of life? A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 644–655. [Google Scholar] [CrossRef]
- Liu, Z.; McGrath, C.; Hägg, U. The impact of malocclusion/orthodontic treatment need on the quality of life: A sys-tematic review. Angle Orthod. 2009, 79, 585–591. [Google Scholar] [CrossRef]
- Zubir, Z.M.; Masood, M.; Rahman, A.N.A.A. An Assessment of Oral Health Related Quality of Life in Orthodontics Patients with Micro-Implant: A Pilot Study. UI Proc. Health Med. 2017, 1, 131–135. [Google Scholar] [CrossRef] [Green Version]
- Nikiforuk, G. Ectopic Eruption: Discussion and clinical report. J. Ont. Dent. Assoc. 1948, 25, 243–246. [Google Scholar]
- Bothung, C.; Fischer, K.; Springer, I.; Wolfart, S. Upper canine inclination influences the aesthetics of a smile. J. Oral. Rehabil. 2015, 42, 144–152. [Google Scholar] [CrossRef]
- Jawad, M.M.; Husein, A.; Azlina, A.; Alam, M.K.; Hassan, R.; Shaari, R. Effect of 940nm low level laser therapy on osteo-genesis in vitro. J. Biomed. Optics. 2013, 18, 128001. [Google Scholar] [CrossRef]
- Jawad, M.M.; Husein, A.; Azlina, A.; Alam, M.K.; Hassan, R.; Shaari, R. Effects of low level laser therapy and low inten-sity pulsed ultrasound treatment and the combination of them on osteogenesis in vitro. Int. J. Orthod. 2018, 29, 60–67. [Google Scholar]
- Jawad, M.M.; Husein, A.; Alam, M.K.; Hassan, R.; Shaari, R.; Azlina, A.; Salzihan, M.S. Effect of low level laser and low in-tensity pulsed ultrasound therapy on bone remodeling during orthodontic tooth movement in rats. Prog. Orthod. 2018, 19, 10. [Google Scholar]
- Qamruddin, I.; Alam, M.K.; Fida, M.; Khan, A.G. Effect of a single dose of low-level laser therapy on spontaneous and chewing pain caused by elastomeric separators. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Qamruddin, I.; Alam, M.K.; Khamis, M.F.; Husein, A. Minimally Invasive Techniques to Accelerate the Orthodontic Tooth Movement: A Systematic Review of Animal Studies. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alam, M.K. Laser assisted orthodontic tooth movement in Saudi population: A randomized clinical trial. Bangladesh J. Med Sci. 2019, 18, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Qamruddin, I.; Alam, M.K.; Mahroof, V.; Fida, M.; Khamis, M.F.; Husein, A. Effects of low-level laser irradiation on the rate of orthodontic tooth movement and associated pain with self-ligating brackets. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 622–630. [Google Scholar] [CrossRef]
- Qamruddin, I.; Alam, M.K.; Abdullah, H.; Kamran, M.A.; Jawaid, N.; Mahroof, V. Effects of single-dose, low-level laser therapy on pain associated with the initial stage of fixed orthodontic treatment: A randomized clinical trial. Korean J. Orthod. 2018, 48, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.K. Laser-Assisted Orthodontic Tooth Movement in Saudi Population: A Prospective Clinical Interven-tion of Low-Level Laser Therapy in the 1st Week of Pain Perception in Four Treatment Modalities. Pain Res. Manage-Ment. 2019, 6271835, 11. [Google Scholar] [CrossRef] [PubMed]
- Mansor, N.; Saub, R.; Othman, S.A. Changes in the oral health-related quality of life 24 h following insertion of fixed orthodontic appliances. J. Orthod. Sci. 2012, 1, 98–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, T.-C.; Chiou, J.-Y.; Chen, T.; Chen, M.-H. Oral health-related quality of life in orthodontic patients during initial therapy with conventional brackets or self-ligating brackets. J. Dent. Sci. 2017, 12, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Andiappan, M.; Gao, W.; Bernabé, E.; Kandala, N.-B.; Donaldson, A.N. Malocclusion, orthodontic treatment, and the Oral Health Impact Profile (OHIP-14): Systematic review and meta-analysis. Angle Orthod. 2014, 85, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Heravi, F.; Farzanegan, F.; Tabatabaee, M.; Sadeghi, M. Do malocclusions affect the oral health-related quality of life? Oral. Health Prev. Dent. 2011, 9, 229–233. [Google Scholar] [PubMed]
- de Oliveira, C.M.; Sheiham, A. Orthodontic treatment and its impact on oral health-related quality of life in Brazil-ian adolescents. J. Orthod. 2004, 31, 20–27. [Google Scholar] [CrossRef]
- O’Brien, C.; Benson, P.E.; Marshman, Z. Evaluation of a quality of life measure for children with malocclusion. J. Orthod. 2007, 34, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Feu, D.; Miguel, J.A.M.; Celeste, R.K.; Oliveira, B.H. Effect of orthodontic treatment on oral health–related quality of life. Angle Orthod. 2013, 83, 892–898. [Google Scholar] [CrossRef]
- de Paula, J.D.; Santos, N.C.; da Silva, E.T.; Nunes, M.F.; Leles, C.R. Psychosocial impact of dental esthetics on quality of life in adolescents. Angle Orthod. 2009, 79, 1188–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.H.; Hagg, U.; Rabie, A.B. Concerns and motivations of skeletal Class III patients receiving orthodon-tic-surgical correction. Int. J. Adult Orthodon. Orthognath. Surg. 2001, 16, 7–17. [Google Scholar]
- Zhang, M.; McGrath, C.; Ha¨gg, U. The impact of malocclusion and its treatment on quality of life: A literature re-view. Int. J. Paediatr. Dent. 2006, 16, 381–387. [Google Scholar] [CrossRef]
- Liu, Z.; McGrath, C.; Ha¨gg, U. Associations between orthodontic treatment need and oral health-related quality of life among young adults: Does it depend on how you assess them? Community Dent. Oral. Epidemiol. 2011, 39, 137–144. [Google Scholar] [CrossRef]
- Fink, D.F.; Smith, R.J. The duration of orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 45–51. [Google Scholar] [CrossRef]
- Sayers, M.; Newton, J. Patients’ expectations of orthodontic treatment: Part 2—Findings from a questionnaire sur-vey. J. Orthod. 2007, 34, 25–35. [Google Scholar] [CrossRef]
- Jawad, M.M.; Husein, A.; Alam, M.K.; Hassan, R.; Shaari, R. Overview of non-invasive factors (low level laser and low intensity pulsed ultrasound) accelerating tooth movement during orthodontic treatment. Lasers Med. Sci. 2012, 29, 367–372. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Selection Guideline | Inclusive Healthy Orthodontic Patients of Saudi Ethnic Background: Angle Class I or II or III Malocclusion with Ectopic Maxillary Canine Requiring Space Creation or Extraction of First Premolar | Exclusive Patient on Long-Term Medication, Craniofacial Anomalies/Malformation, with Parafunctional Habits, Temporomandibular Joint Dysfunction, Multiple Missing Teeth, and Periodontally Compromised | |||
|---|---|---|---|---|---|
| Study design | Objective 1: Retrospective study, and objective 2: prospective evaluation | ||||
| Sample size calculation: Objective 1 | Utilizing effect-size r 0.63 [20], using G*Power software version 3.0.10 with power 80%; α 0.05 the total sample size intended for this research was 96 for three groups. Thus, 32 subjects were required for each group. | ||||
| Study groups (baseline) | Ectopic canine = 32 | Severe crowding = 32 | Class I normal occlusion = 32 | ||
| Study groups (ectopic canine) | Laser | Non-laser | |||
| Sample size calculation: Objective 2 | G*Power software version 3.0.10 with power 80%, α 0.05, and effect size (d) 0.22 was used. Hence, the total sample size intended for this research was 32 for four different treatment modalities [18], and thus each group required a minimum of eight subjects. | ||||
| Treatment modalities | Self-ligating | Conventional | Self-ligating | Conventional | |
| Number of subjects | 8 | 8 | 8 | 8 | |
| Armamentarium | The laser unit was a 940-nm aluminum–gallium–arsenide (Al–Ga–As) diode laser (iLase; Biolase, Irvine, CA, USA) set on continuous mode with power at 100 mW. The diameter of the optical fiber tip was 0.04 cm2, the energy density was calculated to be 7.5 J/cm2 for each point, and total energy density was 75 J per tooth. | ||||
| Orthodontic treatment | For all patients, treatment was commenced by bonding the upper arch with preadjusted edgewise 0.022-inch slot MBT prescription brackets, Agility self-ligating bracket system (G&H Orthodontics, Franklin, IN, USA), and Ortho Organizers conventional type bracket system (Carlsbad, CA, USA). Alignment and leveling started using 0.012-inch super-elastic nickel–titanium (NiTi) wire and was followed by 0.014, 0.016, and 0.018-in NiTi wires, changed at 4-week intervals between each wire. | ||||
| Laser application | Laser applied on gingival mucosa for 3 s each on five points labially/buccally and palatally per tooth, starting from central incisor to the first molar. These points were mesial and distal over the cervical-third of the root and middle of the root, and mesial and distal over the apical-third of the root. The fiber tip of the laser was in close but light contact with the surface of the gingival tissues and held perpendicular to the mucosa overlying the roots of teeth. | ||||
| OHIP-16 | The OHIP-16 measures focus on the impact of one’s oral health condition on QoL, contributing to seven domains: functional limitation, physical pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap. Responses of each item are made on a Likert scale and coded as 1 = never, 2 = hardly ever, 3 = occasionally, 4 = fairly often, and 5 = very often. The OHIP-16 scores range from 16 to 80, where 16 indicates no impact and 80 indicates the worst impact of one’s oral health on QoL. Individual domain scores can be calculated by summing responses to the items within a domain, with higher scores indicating greater impact. | ||||
| Data collection | Patients completed the first questionnaire, which was used as the baseline, before insertion of the fixed orthodontic appliance, and they completed the second and third questionnaire 24 h and 28 days after insertion, respectively. These questionnaires were given to the participants to be completed at home and returned at the following appointment. The participants were asked to record OHIP-16 score after 24 h and 28 days. In addition, telephone calls/message were made at day 28 to ensure accurate collection of data. | ||||
| Statistical analysis | IBM SPSS Statistics version 22.0 (IBM Co., Armonk, NY, USA) was used to analyze the data. Descriptive analysis was performed to obtain the mean values of OHIP-16 scores among four groups. One-way ANOVA and repeated measure ANOVA were used for comparison. | ||||
| Domain | Items | Groups | Mean | SD | 95% CI | p | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| Functional limitation | Difficulties in chewing | Ectopic canine | 1.81 | 0.41 | 1.66 | 1.96 | 0.34 |
| Malocclusion | 1.80 | 0.44 | 1.43 | 2.17 | |||
| Normal occlusion | 2.05 | 0.47 | 1.66 | 2.44 | |||
| Total | 1.85 | 0.42 | 1.73 | 1.97 | |||
| Bad breath | Ectopic canine | 1.53 | 0.30 | 1.42 | 1.64 | 0.48 | |
| Malocclusion | 1.53 | 0.32 | 1.26 | 1.79 | |||
| Normal occlusion | 1.68 | 0.34 | 1.39 | 1.96 | |||
| Total | 1.55 | 0.30 | 1.47 | 1.64 | |||
| Difficulties in pronunciation | Ectopic canine | 2.15 | 0.49 | 1.97 | 2.32 | 0.24 | |
| Malocclusion | 2.14 | 0.54 | 1.69 | 2.59 | |||
| Normal occlusion | 1.83 | 0.38 | 1.51 | 2.14 | |||
| Total | 2.09 | 0.49 | 1.95 | 2.23 | |||
| Discomfort in eating | Ectopic canine | 1.66 | 0.35 | 1.53 | 1.79 | 0.97 | |
| Malocclusion | 1.65 | 0.39 | 1.33 | 1.97 | |||
| Normal occlusion | 1.69 | 0.32 | 1.42 | 1.96 | |||
| Total | 1.66 | 0.35 | 1.56 | 1.76 | |||
| Physical pain | Ulcer | Ectopic canine | 1.81 | 0.41 | 1.66 | 1.96 | 0.93 |
| Malocclusion | 1.80 | 0.44 | 1.43 | 2.17 | |||
| Normal occlusion | 1.75 | 0.36 | 1.45 | 2.05 | |||
| Total | 1.80 | 0.40 | 1.68 | 1.91 | |||
| Pain | Ectopic canine | 1.59 | 0.32 | 1.48 | 1.71 | 0.22 | |
| Malocclusion | 1.59 | 0.35 | 1.30 | 1.88 | |||
| Normal occlusion | 1.83 | 0.38 | 1.51 | 2.14 | |||
| Total | 1.63 | 0.34 | 1.53 | 1.73 | |||
| Psychological discomfort | Food stuck in between teeth | Ectopic canine | 2.15 | 0.49 | 1.97 | 2.32 | 0.06 |
| Malocclusion | 2.14 | 0.54 | 1.69 | 2.59 | |||
| Normal occlusion | 1.69 | 0.32 | 1.42 | 1.96 | |||
| Total | 2.07 | 0.50 | 1.92 | 2.21 | |||
| Embarrassment | Ectopic canine | 3.50 | 0.99 | 3.14 | 3.85 | 0.00 | |
| Malocclusion | 3.54 | 1.00 | 2.71 | 4.37 | |||
| Normal occlusion | 1.69 | 0.32 | 1.42 | 1.96 | |||
| Total | 3.20 | 1.13 | 2.87 | 3.53 | |||
| Physical disability | Avoidances of eating certain foods | Ectopic canine | 2.06 | 0.47 | 1.89 | 2.23 | 0.23 |
| Malocclusion | 2.05 | 0.52 | 1.62 | 2.48 | |||
| Normal occlusion | 1.75 | 0.36 | 1.45 | 2.05 | |||
| Total | 2.01 | 0.46 | 1.87 | 2.14 | |||
| Avoid smiling | Ectopic canine | 3.58 | 1.03 | 3.21 | 3.95 | 0.00 | |
| Malocclusion | 3.63 | 1.03 | 2.77 | 4.48 | |||
| Normal occlusion | 1.75 | 0.36 | 1.45 | 2.05 | |||
| Total | 3.28 | 1.16 | 2.95 | 3.62 | |||
| Psychological disability | Disturbed sleep | Ectopic canine | 1.38 | 0.14 | 1.33 | 1.43 | 0.61 |
| Malocclusion | 1.38 | 0.15 | 1.25 | 1.50 | |||
| Normal occlusion | 1.44 | 0.17 | 1.30 | 1.58 | |||
| Total | 1.39 | 0.15 | 1.35 | 1.43 | |||
| Concentration affected | Ectopic canine | 1.63 | 0.34 | 1.51 | 1.76 | 0.47 | |
| Malocclusion | 1.65 | 0.39 | 1.33 | 1.97 | |||
| Normal occlusion | 1.48 | 0.20 | 1.31 | 1.64 | |||
| Total | 1.61 | 0.33 | 1.51 | 1.70 | |||
| Social disability | Avoided going out | Ectopic canine | 1.73 | 0.38 | 1.59 | 1.87 | 0.21 |
| Malocclusion | 1.73 | 0.41 | 1.38 | 2.07 | |||
| Normal occlusion | 1.48 | 0.20 | 1.31 | 1.64 | |||
| Total | 1.69 | 0.37 | 1.58 | 1.79 | |||
| Difficulty carrying out daily activities | Ectopic canine | 1.54 | 0.29 | 1.43 | 1.64 | 0.85 | |
| Malocclusion | 1.53 | 0.32 | 1.26 | 1.79 | |||
| Normal occlusion | 1.48 | 0.20 | 1.31 | 1.64 | |||
| Total | 1.53 | 0.28 | 1.45 | 1.61 | |||
| Handicap | Lack of self-confidence | Ectopic canine | 3.33 | 0.92 | 2.99 | 3.66 | 0.00 |
| Malocclusion | 3.36 | 0.93 | 2.58 | 4.14 | |||
| Normal occlusion | 1.56 | 0.27 | 1.34 | 1.79 | |||
| Total | 3.04 | 1.07 | 2.73 | 3.35 | |||
| Difficulties in cleaning | Ectopic canine | 1.81 | 0.41 | 1.66 | 1.96 | 0.16 | |
| Malocclusion | 1.80 | 0.44 | 1.43 | 2.17 | |||
| Normal occlusion | 1.51 | 0.24 | 1.32 | 1.71 | |||
| Total | 1.76 | 0.40 | 1.64 | 1.87 | |||
| Total | OHIP-16 | Ectopic canine | 33.06 | 7.12 | 30.49 | 35.62 | 0.06 |
| Malocclusion | 33.09 | 7.68 | 26.67 | 39.51 | |||
| Normal occlusion | 26.43 | 4.64 | 22.54 | 30.31 | |||
| Total | 31.96 | 7.19 | 29.87 | 34.04 | |||
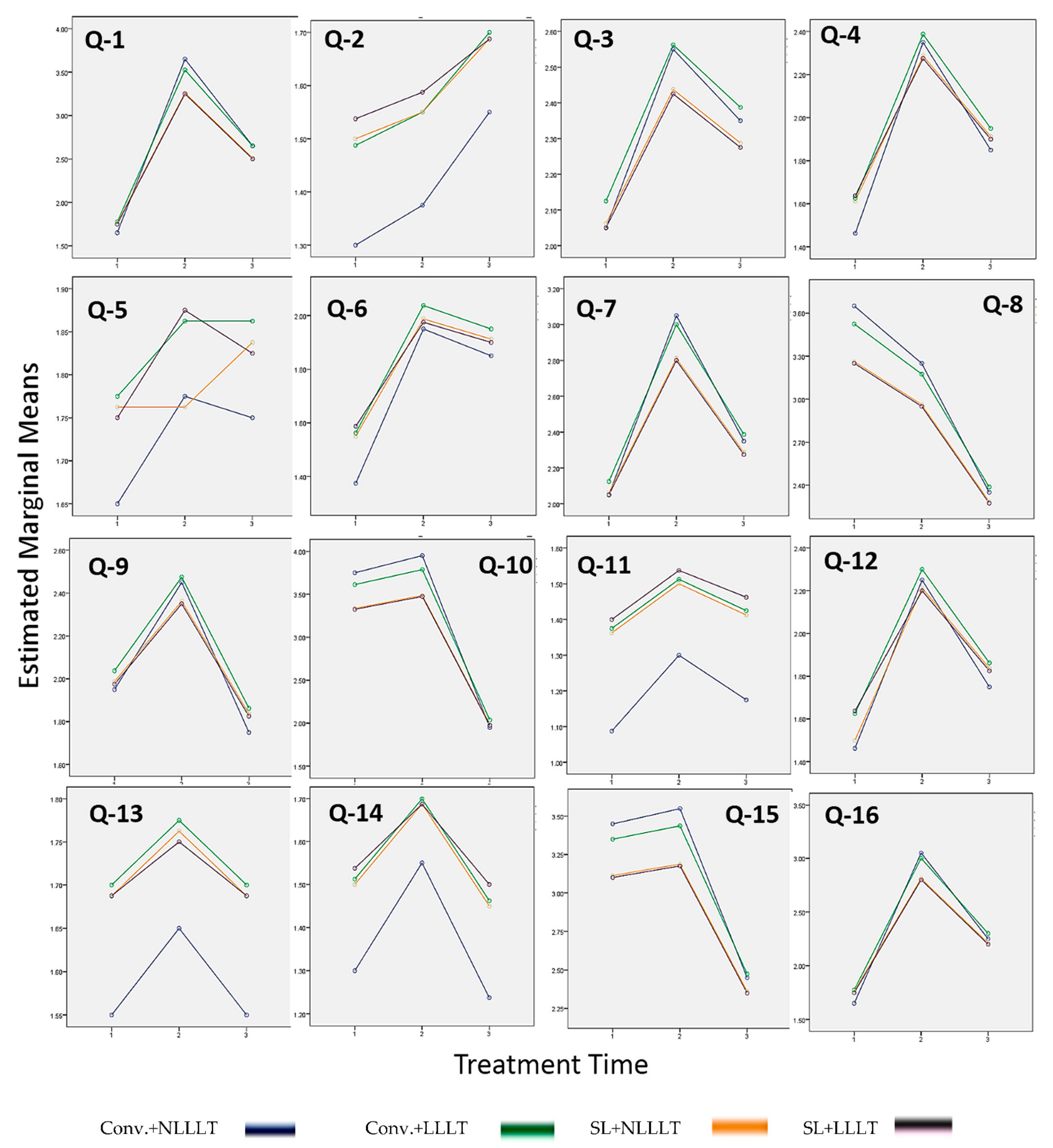
| Domain | Items | OTM | Baseline | 1 Day after | 28 Days after | |||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |||
| Functional limitation | Difficulties in chewing | Conv. + NLLLT | 1.65 | 0.37 | 3.65 | 0.37 | 2.65 | 0.37 |
| Conv. + LLLT | 1.78 | 0.43 | 3.53 | 0.95 | 2.65 | 0.64 | ||
| SL + NLLLT | 1.76 | 0.36 | 3.26 | 1.18 | 2.51 | 0.74 | ||
| SL + LLLT | 1.75 | 0.49 | 3.25 | 1.25 | 2.50 | 0.83 | ||
| Bad breath | Conv. + NLLLT | 1.30 | 0.31 | 1.38 | 0.34 | 1.55 | 0.37 | |
| Conv. + LLLT | 1.49 | 0.34 | 1.55 | 0.36 | 1.70 | 0.40 | ||
| SL + NLLLT | 1.50 | 0.24 | 1.55 | 0.28 | 1.69 | 0.34 | ||
| SL + LLLT | 1.54 | 0.33 | 1.59 | 0.37 | 1.69 | 0.46 | ||
| Difficulties in pronunciation | Conv. + NLLLT | 2.05 | 0.37 | 2.55 | 0.37 | 2.35 | 0.37 | |
| Conv. + LLLT | 2.13 | 0.49 | 2.56 | 0.62 | 2.39 | 0.56 | ||
| SL + NLLLT | 2.06 | 0.50 | 2.44 | 0.70 | 2.29 | 0.62 | ||
| SL + LLLT | 2.05 | 0.61 | 2.43 | 0.79 | 2.28 | 0.71 | ||
| Discomfort in eating | Conv. + NLLLT | 1.46 | 0.35 | 2.35 | 0.37 | 1.85 | 0.37 | |
| Conv. + LLLT | 1.63 | 0.38 | 2.39 | 0.56 | 1.95 | 0.46 | ||
| SL + NLLLT | 1.61 | 0.31 | 2.29 | 0.62 | 1.91 | 0.43 | ||
| SL + LLLT | 1.64 | 0.41 | 2.28 | 0.71 | 1.90 | 0.55 | ||
| Physical pain | Ulcer | Conv. + NLLLT | 1.65 | 0.37 | 1.78 | 0.32 | 1.75 | 0.37 |
| Conv. + LLLT | 1.78 | 0.43 | 1.86 | 0.46 | 1.86 | 0.44 | ||
| SL + NLLLT | 1.76 | 0.36 | 1.76 | 0.36 | 1.84 | 0.39 | ||
| SL + LLLT | 1.75 | 0.49 | 1.88 | 0.49 | 1.83 | 0.52 | ||
| Pain | Conv. + NLLLT | 1.38 | 0.34 | 1.95 | 0.37 | 1.85 | 0.37 | |
| Conv. + LLLT | 1.56 | 0.35 | 2.04 | 0.47 | 1.95 | 0.46 | ||
| SL + NLLLT | 1.55 | 0.28 | 1.99 | 0.46 | 1.91 | 0.43 | ||
| SL + LLLT | 1.59 | 0.37 | 1.98 | 0.58 | 1.90 | 0.55 | ||
| Psychological discomfort | Food stuck in between teeth | Conv. + NLLLT | 2.05 | 0.37 | 3.05 | 0.37 | 2.35 | 0.37 |
| Conv. + LLLT | 2.13 | 0.49 | 3.00 | 0.76 | 2.39 | 0.56 | ||
| SL + NLLLT | 2.06 | 0.50 | 2.81 | 0.92 | 2.29 | 0.62 | ||
| SL + LLLT | 2.05 | 0.61 | 2.80 | 0.99 | 2.28 | 0.71 | ||
| Embarrassment | Conv. + NLLLT | 3.65 | 0.37 | 3.25 | 0.37 | 2.35 | 0.37 | |
| Conv. + LLLT | 3.53 | 0.95 | 3.18 | 0.82 | 2.39 | 0.56 | ||
| SL + NLLLT | 3.26 | 1.18 | 2.96 | 1.01 | 2.29 | 0.62 | ||
| SL + LLLT | 3.25 | 1.25 | 2.95 | 1.08 | 2.28 | 0.71 | ||
| Physical disability | Avoidances of eating certain foods | Conv. + NLLLT | 1.95 | 0.37 | 2.45 | 0.37 | 1.75 | 0.37 |
| Conv. + LLLT | 2.04 | 0.47 | 2.48 | 0.59 | 1.86 | 0.44 | ||
| SL + NLLLT | 1.99 | 0.46 | 2.36 | 0.66 | 1.84 | 0.39 | ||
| SL + LLLT | 1.98 | 0.58 | 2.35 | 0.75 | 1.83 | 0.52 | ||
| Avoid smiling | Conv. + NLLLT | 3.75 | 0.37 | 3.95 | 0.37 | 1.95 | 0.37 | |
| Conv. + LLLT | 3.61 | 0.98 | 3.79 | 1.04 | 2.04 | 0.47 | ||
| SL + NLLLT | 3.34 | 1.23 | 3.49 | 1.32 | 1.99 | 0.46 | ||
| SL + LLLT | 3.33 | 1.29 | 3.48 | 1.38 | 1.98 | 0.58 | ||
| Psychological disability | Disturbed sleep | Conv. + NLLLT | 1.09 | 0.15 | 1.30 | 0.31 | 1.18 | 0.23 |
| Conv. + LLLT | 1.38 | 0.18 | 1.51 | 0.31 | 1.43 | 0.24 | ||
| SL + NLLLT | 1.36 | 0.12 | 1.50 | 0.24 | 1.41 | 0.18 | ||
| SL + LLLT | 1.40 | 0.16 | 1.54 | 0.33 | 1.46 | 0.24 | ||
| Concentration affected | Conv. + NLLLT | 1.46 | 0.35 | 2.25 | 0.37 | 1.75 | 0.37 | |
| Conv. + LLLT | 1.63 | 0.38 | 2.30 | 0.54 | 1.86 | 0.44 | ||
| SL + NLLLT | 1.50 | 0.22 | 2.21 | 0.58 | 1.84 | 0.39 | ||
| SL + LLLT | 1.64 | 0.41 | 2.20 | 0.68 | 1.83 | 0.52 | ||
| Social disability | Avoided going out | Conv. + NLLLT | 1.55 | 0.37 | 1.65 | 0.37 | 1.55 | 0.37 |
| Conv. + LLLT | 1.70 | 0.40 | 1.78 | 0.43 | 1.70 | 0.40 | ||
| SL + NLLLT | 1.69 | 0.34 | 1.76 | 0.36 | 1.69 | 0.34 | ||
| SL + LLLT | 1.69 | 0.46 | 1.75 | 0.49 | 1.69 | 0.46 | ||
| Difficulty carrying out daily activities | Conv. + NLLLT | 1.30 | 0.31 | 1.55 | 0.37 | 1.24 | 0.27 | |
| Conv. + LLLT | 1.51 | 0.31 | 1.70 | 0.40 | 1.46 | 0.28 | ||
| SL + NLLLT | 1.50 | 0.24 | 1.69 | 0.34 | 1.45 | 0.21 | ||
| SL + LLLT | 1.54 | 0.33 | 1.69 | 0.46 | 1.50 | 0.29 | ||
| Handicap | Lack of self-confidence | Conv. + NLLLT | 3.45 | 0.37 | 3.55 | 0.37 | 2.45 | 0.37 |
| Conv. + LLLT | 3.35 | 0.88 | 3.44 | 0.91 | 2.48 | 0.59 | ||
| SL + NLLLT | 3.11 | 1.09 | 3.19 | 1.14 | 2.36 | 0.66 | ||
| SL + LLLT | 3.10 | 1.16 | 3.18 | 1.20 | 2.35 | 0.75 | ||
| Difficulties in cleaning | Conv. + NLLLT | 1.65 | 0.37 | 3.05 | 0.37 | 2.25 | 0.37 | |
| Conv. + LLLT | 1.78 | 0.43 | 3.00 | 0.76 | 2.30 | 0.54 | ||
| SL + NLLLT | 1.76 | 0.36 | 2.81 | 0.92 | 2.21 | 0.58 | ||
| SL + LLLT | 1.75 | 0.49 | 2.80 | 0.99 | 2.20 | 0.68 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.K.; Alfawzan, A.A. Oral Health Impact Profile in Orthodontic Patients with Ectopic Canine: A Prospective Clinical Intervention of Four Treatment Modalities. Healthcare 2021, 9, 337. https://doi.org/10.3390/healthcare9030337
Alam MK, Alfawzan AA. Oral Health Impact Profile in Orthodontic Patients with Ectopic Canine: A Prospective Clinical Intervention of Four Treatment Modalities. Healthcare. 2021; 9(3):337. https://doi.org/10.3390/healthcare9030337
Chicago/Turabian StyleAlam, Mohammad Khursheed, and Ahmed Ali Alfawzan. 2021. "Oral Health Impact Profile in Orthodontic Patients with Ectopic Canine: A Prospective Clinical Intervention of Four Treatment Modalities" Healthcare 9, no. 3: 337. https://doi.org/10.3390/healthcare9030337