
The Usefulness of the QR Code in Orthotic Applications after Orthopedic Surgery

 , , ,
, , ,
Abstract
:1. Introduction
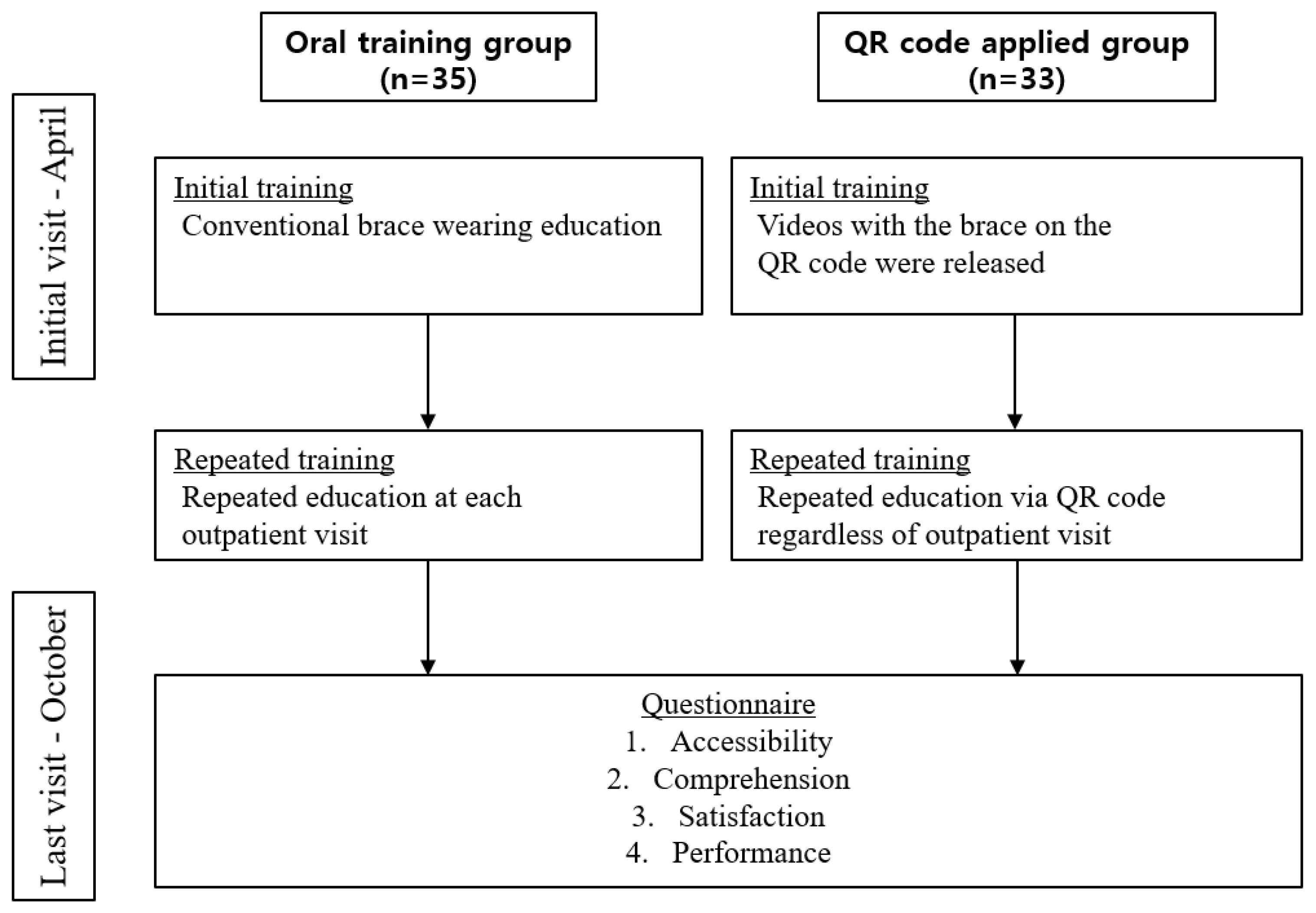
2. Materials and Methods
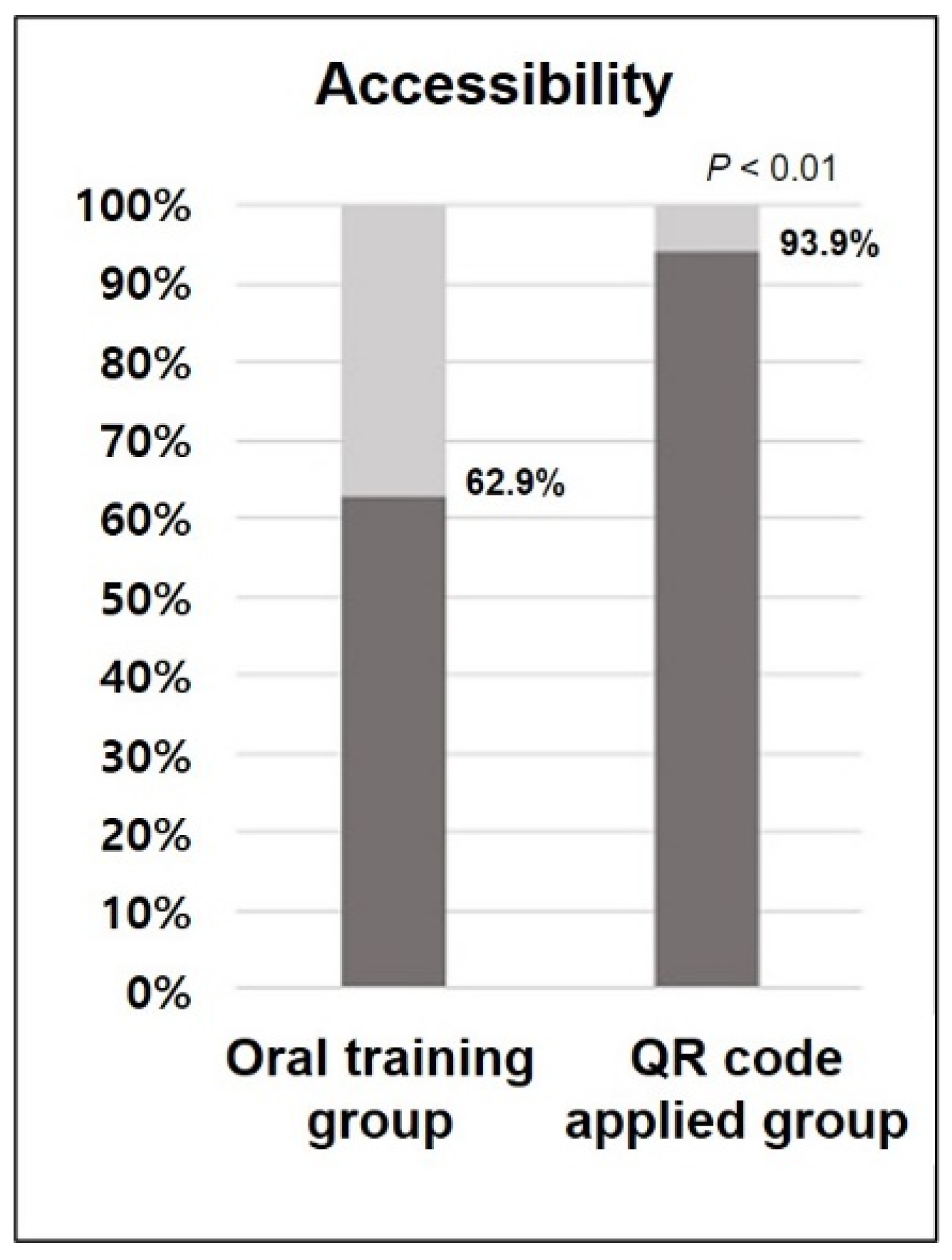
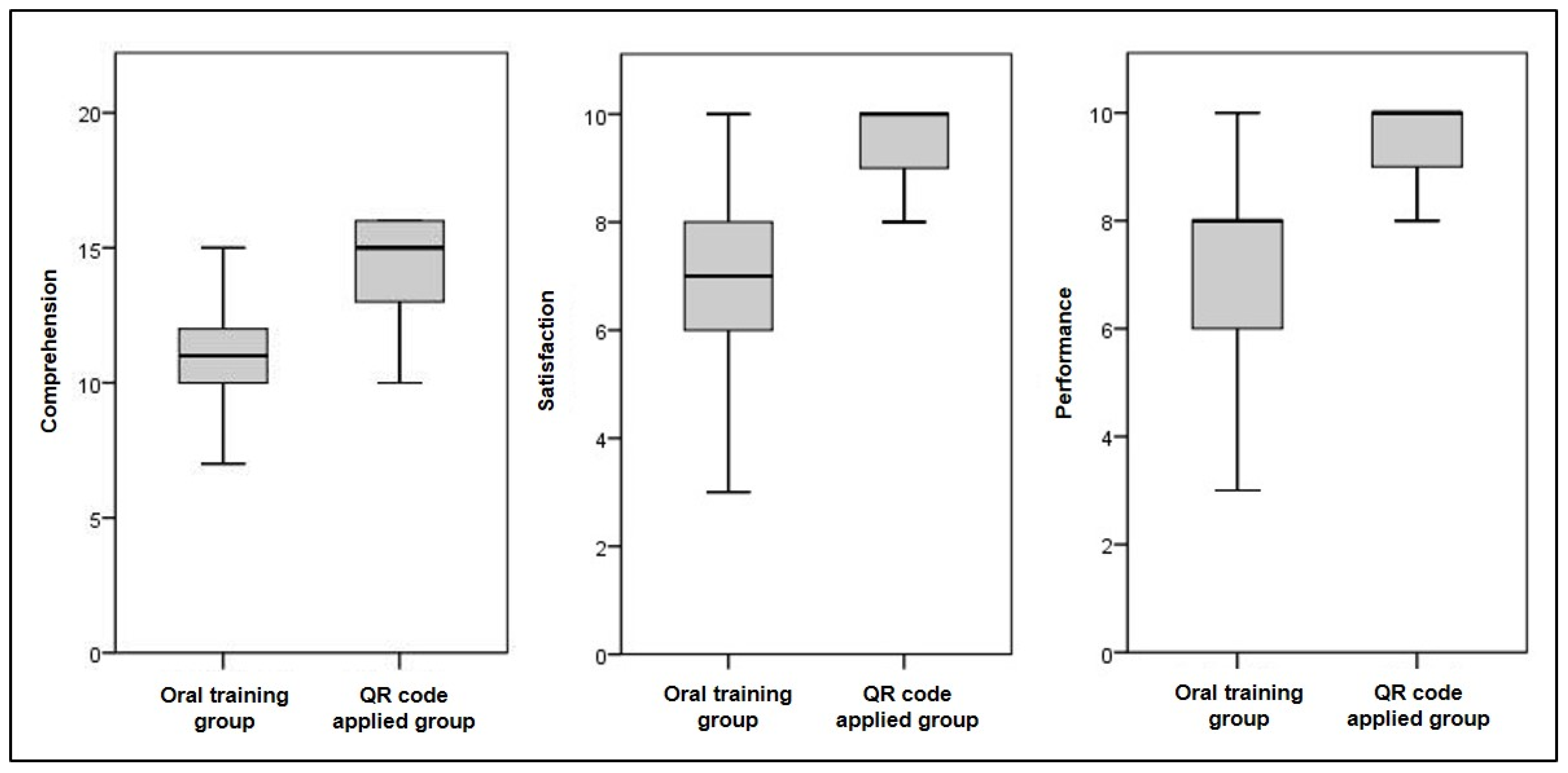
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Daack-Hirsch, S.; Campbell, C.A. The role of patient engagement in personalized healthcare. Pers. Med. 2014, 11, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Lundby, C.; Graabaek, T.; Ryg, J.; Søndergaard, J.; Pottegård, A.; Nielsen, D.S. Health care professionals’ attitudes towards deprescribing in older patients with limited life expectancy: A systematic review. Br. J. Clin. Pharmacol. 2019, 85, 868–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, D.J.; Franzone, J.M.; Matsumoto, H.; Gomez, J.A.; Avendaño, J.; Hyman, J.E.; Roye, D.P., Jr.; Vitale, M.G. Electronic monitoring improves brace-wearing compliance in patients with adolescent idiopathic scoliosis: A randomized clinical trial. Spine 2012, 37, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Judd, T.; Elliott, K. Selection and Use of Online Learning Resources by First-Year Medical Students: Cross-Sectional Study. JMIR Med. Educ. 2017, 3, e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srikesavan, C.; Williamson, E.; Cranston, T.; Hunter, J.; Adams, J.; Lamb, S.E. An Online Hand Exercise Intervention for Adults With Rheumatoid Arthritis (mySARAH): Design, Development, and Usability Testing. J. Med. Internet Res. 2018, 20, e10457. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.P. Patients’ memory for medical information. J. R. Soc. Med. 2003, 96, 219–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houts, P.S.; Bachrach, R.; Witmer, J.T.; Tringali, C.A.; Bucher, J.A.; Localio, R.A. Using pictographs to enhance recall of spoken medical instructions. Patient Educ. Couns. 1998, 35, 83–88. [Google Scholar] [CrossRef]
- Houts, P.S.; Witmer, J.T.; Egeth, H.E.; Loscalzo, M.J.; Zabora, J.R. Using pictographs to enhance recall of spoken medical instructions II. Patient Educ. Couns. 2001, 43, 231–242. [Google Scholar] [CrossRef]
- Sandberg, E.H.; Sharma, R.; Sandberg, W.S. Deficits in retention for verbally presented medical information. Anesthesiology 2012, 117, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Chien, T.W.; Lin, W.S. Improving Inpatient Surveys: Web-Based Computer Adaptive Testing Accessed via Mobile Phone QR Codes. JMIR Med. Inform. 2016, 4, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capranzano, P.; Francaviglia, B.; Sardone, A.; Agnello, F.; Valenti, N.; Frazzetto, M.; Legnazzi, M.; Occhipinti, G.; Scalia, L.; Calvi, V.; et al. Suitability for elderly with heart disease of a QR code-based feedback of drug intake: Overcoming limitations of current medication adherence telemonitoring systems. Int. J. Cardiol. 2021, 327, 209–216. [Google Scholar] [CrossRef]
- Nakipoğlu Yüzer, G.F.; Koyuncu, E.; Çam, P.; Özgirgin, N. The regularity of orthosis use and the reasons for disuse in stroke patients. Int. J. Rehabil. Res. 2018, 41, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.H.; Wu, H.C. A cloud medication safety support system using QR code and Web services for elderly outpatients. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2014, 22, 99–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, A.T.; Fieraru, G.; Gaffney, P.; Butler, M.; Kincaid, R.J.; Middleton, R.G. A novel use of QR code stickers after orthopaedic cast application. Ann. R. Coll. Surg. Engl. 2017, 99, 476–478. [Google Scholar] [CrossRef]
- Spaulding, S.E.; Yamane, A.; McDonald, C.L.; Spaulding, S.A. A conceptual framework for orthotic and prosthetic education. Prosthet. Orthot. Int. 2019, 43, 369–381. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Total (%) | p Value | |||
|---|---|---|---|---|---|
| Oral Training Group | QR Code Applied Group | ||||
| Age | Mean ± SD | 58.60 ± 16.20 | 63.55 ± 15.93 | 61.0 ± 16.14 | 0.209 * |
| Range (Min–Max) | 10–88 | 15–85 | 10–88 | ||
| Sex | Male | 20 | 19 | 39 (57.4) | 0.971 † |
| Female | 15 | 14 | 29 (42.6) | ||
| Orthosis | Shoulder abduction brace | 15 | 7 | 22 (32.4) | 0.354 † |
| TLSO | 11 | 12 | 23 (33.8) | ||
| Hip abduction brace | 4 | 5 | 9 (13.2) | ||
| Corset | 4 | 6 | 10 (14.7) | ||
| P-brace | 1 | 3 | 4 (5.9) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; Seo, G.-W.; Lee, J.S.; Cho, H.K.; Kang, E.M.; Kim, J.; Chun, D.-I.; Yi, Y.; Won, S.H. The Usefulness of the QR Code in Orthotic Applications after Orthopedic Surgery. Healthcare 2021, 9, 298. https://doi.org/10.3390/healthcare9030298
Cho J, Seo G-W, Lee JS, Cho HK, Kang EM, Kim J, Chun D-I, Yi Y, Won SH. The Usefulness of the QR Code in Orthotic Applications after Orthopedic Surgery. Healthcare. 2021; 9(3):298. https://doi.org/10.3390/healthcare9030298
Chicago/Turabian StyleCho, Jaeho, Gi-Won Seo, Jeong Seok Lee, Hyung Ki Cho, Eun Myeong Kang, Jahyung Kim, Dong-Il Chun, Young Yi, and Sung Hun Won. 2021. "The Usefulness of the QR Code in Orthotic Applications after Orthopedic Surgery" Healthcare 9, no. 3: 298. https://doi.org/10.3390/healthcare9030298