
Immersive 3D Educational Contents: A Technical Note for Dental Educators


 , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methodology
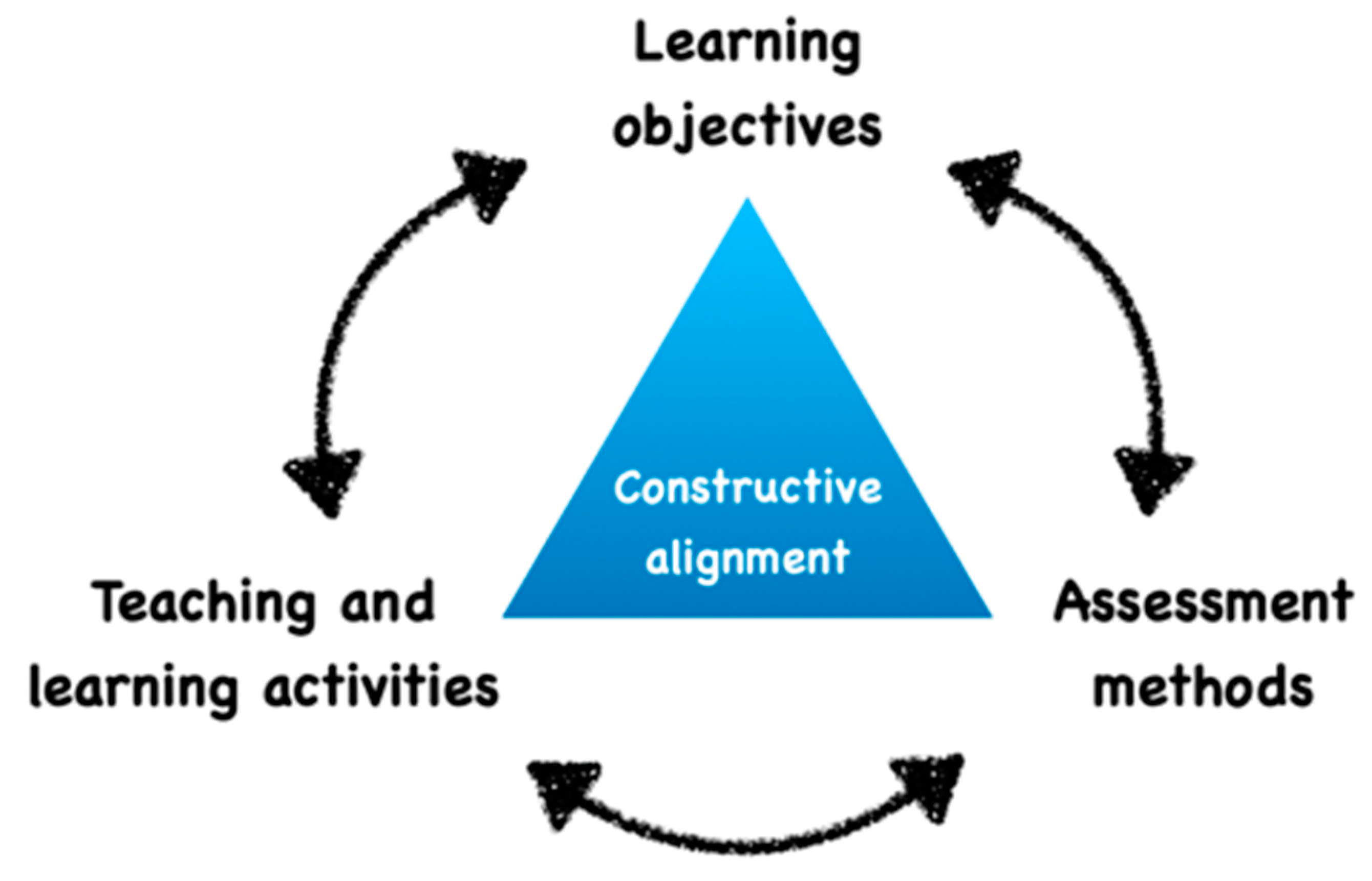
2.1. Alignment of Educational Objective to Educational Content
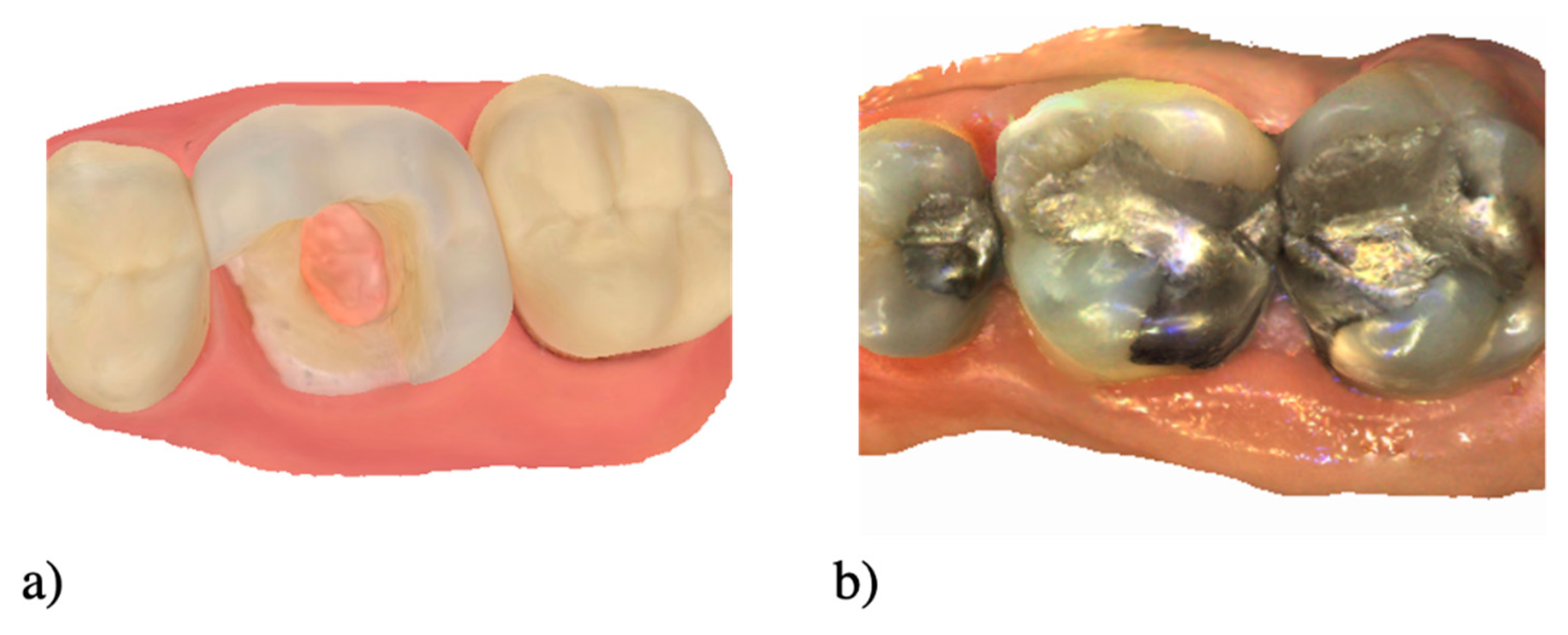
2.2. Create or Collect the Situation
2.3. Scan with an IOS
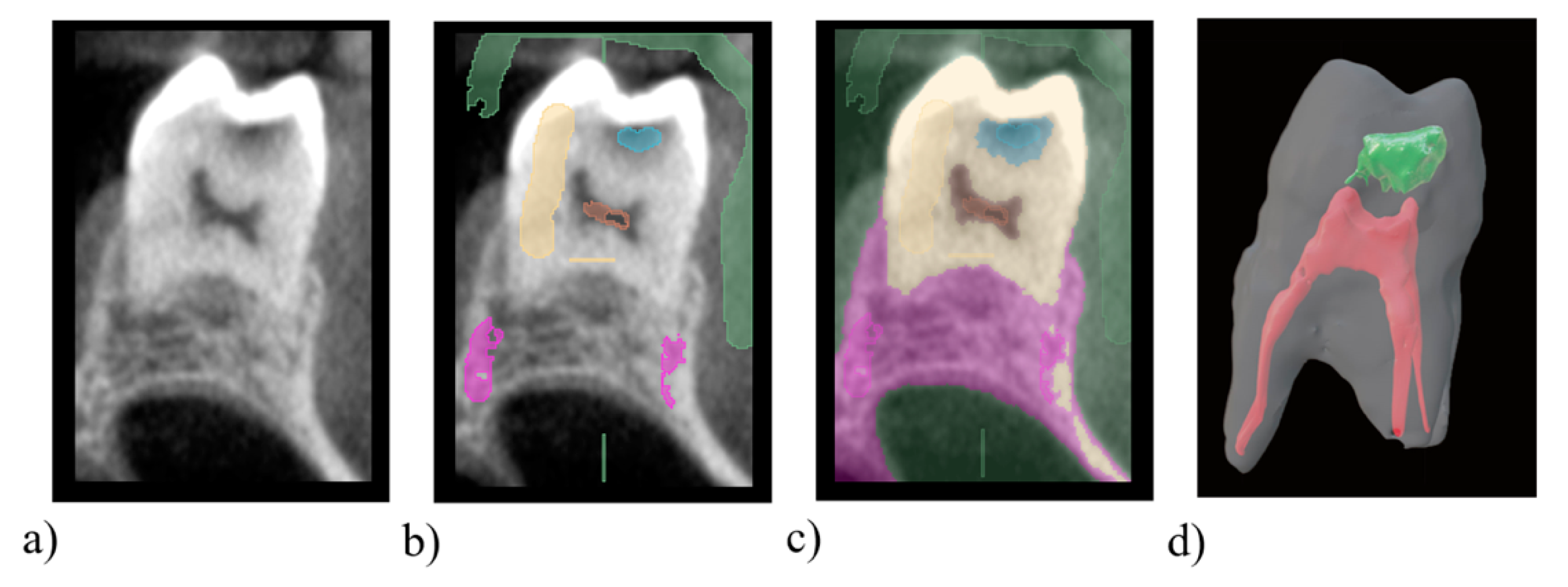
2.4. Scan with a CBCT
2.5. Post Treatement
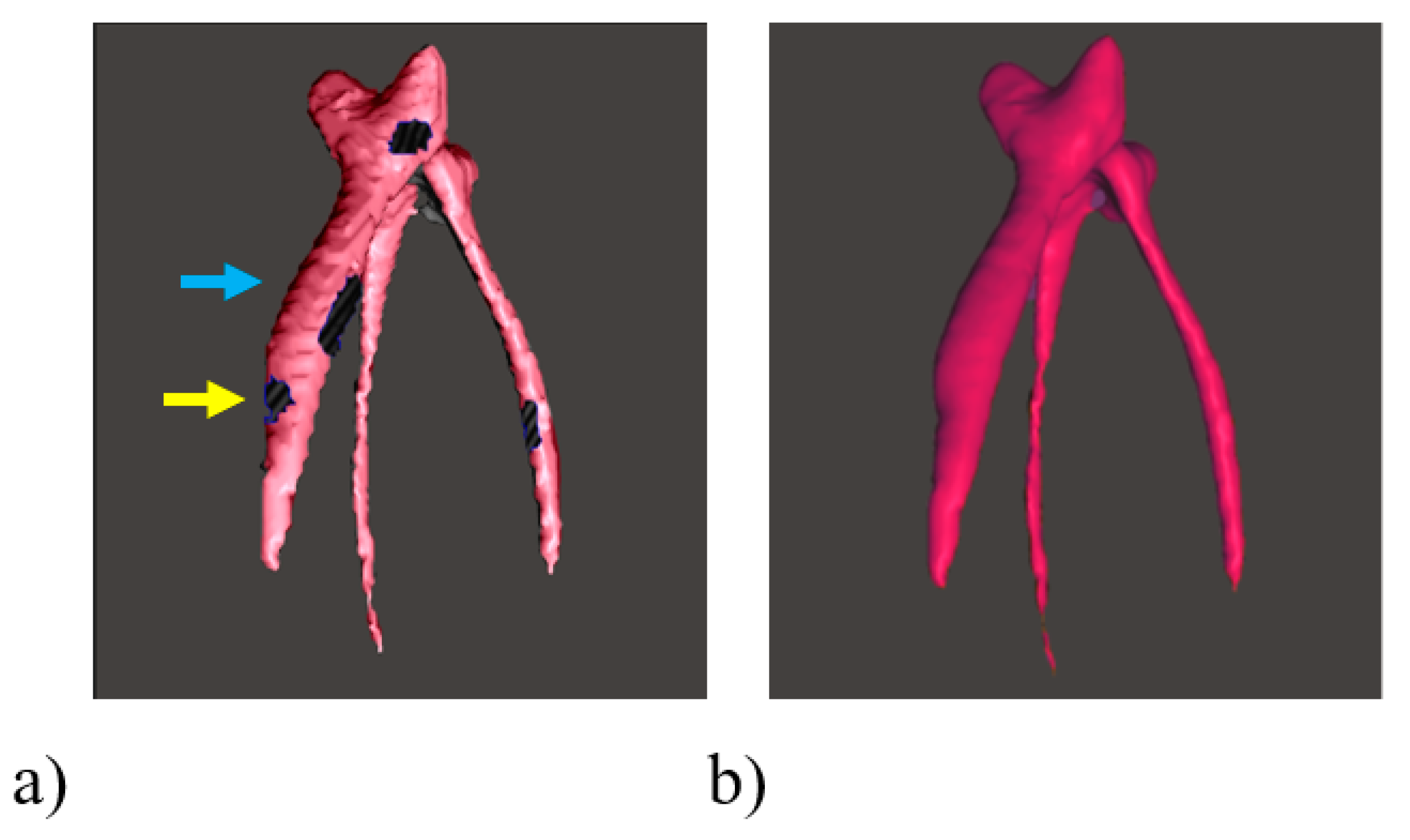
2.5.1. Quality Analysis of 3D File
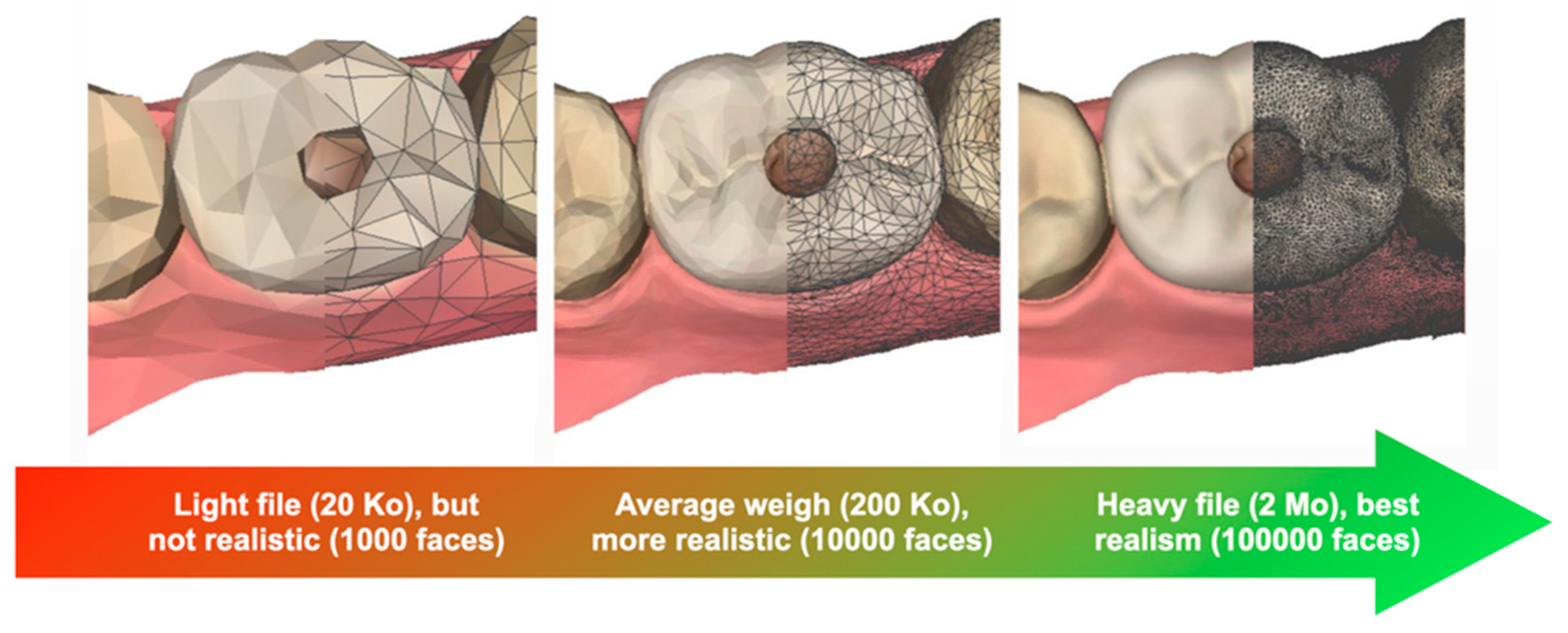
2.5.2. Re-Meshing and Simplification
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wulfman, C.; Bonnet, G.; Carayon, D.; Lance, C.; Fages, M.; Virard, F.; Daas, M.; Rignon-Bret, C.; Naveau, A.; Millet, C.; et al. Digital removable complete denture: A narrative review. Fr. J. Dent. Med. 2020. [Google Scholar] [CrossRef]
- Rekow, E.D. Digital Dentistry: The New State of the Art—Is It Disruptive or Destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef]
- Bogomolova, K.; Hierck, B.P.; van der Hage, J.A.; Hovius, S.E.R. Anatomy Dissection Course Improves the Initially Lower Levels of Visual-Spatial Abilities of Medical Undergraduates. Anat. Sci. Educ. 2020, 13, 333–342. [Google Scholar] [CrossRef]
- Kato, A.; Ziegler, A.; Utsumi, M.; Ohno, K.; Takeichi, T. Three-Dimensional Imaging of Internal Tooth Structures: Applications in Dental Education. J. Oral Biosci. 2016, 58, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Laeng, B.; Latham, K.; Jackson Zaiyouna, R.; Richarson, C. A Redrawn Vandenberg and Kuse Mental Rotations Test: Different Versions and Factors That Affect Performance. Brain Cogn. 1995, 28, 39–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef] [PubMed]
- Elbashti, M.; Aswehlee, A.; Nguyen, C.T.; Ella, B.; Naveau, A. Technical Protocol for Presenting Maxillofacial Prosthetics Concepts to Dental Students Using Interactive 3D Virtual Models within a Portable Document Format. J. Prosthodont. 2020, 29, 546–549. [Google Scholar] [CrossRef]
- Goodacre, C.J. Digital Learning Resources for Prosthodontic Education: The Perspectives of a Long-Term Dental Educator Regarding 4 Key Factors. J. Prosthodont. 2018, 27, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Iozzino, R.; Champin, P.A.; Richert, R.; Bui, R.; Palombi, O.; Charlin, B.; Tamimi, F.; Ducret, M. Assessing Decision-Making in Education of Restorative and Prosthetic Dentistry: A Pilot Study. Int. J. Prosthodont. 2020. [Google Scholar] [CrossRef]
- Schwindling, F.S.; Deisenhofer, U.K.; Porsche, M.; Rammelsberg, P.; Kappel, S.; Stober, T. Establishing CAD/CAM in Preclinical Dental Education: Evaluation of a Hands-On Module. J. Dent. Educ. 2015, 79, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Biggs, J. Enhancing Teaching through Constructive Alignment. High. Educ. 1996, 32, 347–364. [Google Scholar] [CrossRef]
- Biggs, J. What the Student Does: Teaching for Enhanced Learning. Int. J. Phytoremediation 1999, 21, 57–75. [Google Scholar] [CrossRef] [Green Version]
- Decurcio, D.A.; Lim, E.; Chaves, G.S.; Nagendrababu, V.; Estrela, C.; Rossi-Fedele, G. Pre-Clinical Endodontic Education Outcomes between Artificial versus Extracted Natural Teeth: A Systematic Review. Int. Endod. J. 2019, 52, 1153–1161. [Google Scholar] [CrossRef] [Green Version]
- Bücking, T.M.; Hill, E.R.; Robertson, J.L.; Maneas, E.; Plumb, A.A.; Nikitichev, D.I. From Medical Imaging Data to 3D Printed Anatomical Models. PLoS ONE 2017, 12, e0178540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rengier, F.; Mehndiratta, A.; Von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.U.; Giesel, F.L. 3D Printing Based on Imaging Data: Review of Medical Applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K. Accuracy of 3D-Dimensiobally printed full-arch dental models: A systematic review. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef]
- Khalaf, K.; El-Kishawi, M.; Mustafa, S.; Al Kawas, S. Effectiveness of Technology-Enhanced Teaching and Assessment Methods of Undergraduate Preclinical Dental Skills: A Systematic Review of Randomized Controlled Clinical Trials. BMC Med. Educ. 2020, 20, 286. [Google Scholar] [CrossRef]
- Hoyek, N.; Collet, C.; Rastello, O.; Fargier, P.; Thiriet, P.; Guillot, A. Enhancement of Mental Rotation Abilities and Its Effect on Anatomy Learning. Teach. Learn. Med. 2009, 21, 201–206. [Google Scholar] [CrossRef]
- Versiani, M.A.; Basrani, B.; Sousa-Neto, M.D. The Root Canal Anatomy in Permanent Dentition. Root Canal Anat. Perm. Dentition; Springer International Publishing: Cham, Switzerland, 2018; pp. 391–425. [Google Scholar]
- Kustra, P.; Dobroś, K.; Zarzecka, J. Making Use of Three-Dimensional Models of Teeth, Manufactured by Stereolithographic Technology, in Practical Teaching of Endodontics. Eur. J. Dent. Educ. 2020. [Google Scholar] [CrossRef]
- Wanzel, K.R.; Hamstra, S.J.; Anastakis, D.J.; Matsumoto, E.D.; Cusimano, M.D. Effect of Visual-Spatial Ability on Learning of Spatially Complex Surgical Skills. Lancet 2002, 359, 230–231. [Google Scholar] [CrossRef]
- Yee, S.; Richert, R.; Viguie, G.; Couraud, S.; Dehurtevent, M.; Fages, M.; Corne, P.; Ducret, M. Evaluation of the Use of a Guided Bur during Preclinical Teaching of Tooth Preparation: A Pilot Study. Clin. Exp. Dent. Res. 2019, 5, 588–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schepke, U.; van Wulfften Palthe, M.E.; Meisberger, E.W.; Kerdijk, W.; Cune, M.S.; Blok, B. Digital Assessment of a Retentive Full Crown Preparation—An Evaluation of PrepCheck in an Undergraduate Pre-Clinical Teaching Environment. Eur. J. Dent. Educ. 2020, 24, 407–424. [Google Scholar] [CrossRef] [Green Version]
- Seet, R.H.; Soo, P.R.; Leong, K.J.M.; Pang, J.J.H.; Lee, F.K.F.; Tan, M.Y. Crown Preparations by Undergraduate Dental Students: A Comparison of Conventional versus Digital Assessment via an Intraoral Scanner. J. Dent. Educ. 2020, 84, 1303–1313. [Google Scholar] [CrossRef]
- López Chávez, O.; Rodríguez, L.F.; Gutierrez-Garcia, J.O. A Comparative Case Study of 2D, 3D and Immersive-Virtual-Reality Applications for Healthcare Education. Int. J. Med. Inform. 2020, 141, 104226. [Google Scholar] [CrossRef]
- Höhne, C.; Schmitter, M. 3D Printed Teeth for the Preclinical Education of Dental Students. J. Dent. Educ. 2019, 83, 1100–1106. [Google Scholar] [CrossRef]
- Hanisch, M.; Kroeger, E.; Dekiff, M.; Timme, M.; Kleinheinz, J.; Dirksen, D. 3D-Printed Surgical Training Model Based on Real Patient Situations for Dental Education. Int. J. Environ. Res. Public Health 2020, 17, 2901. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, A.; Pulijala, Y. The Application of Virtual Reality and Augmented Reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 1–8. [Google Scholar]
- Elbashti, M.E.; Itamiya, T.; Aswehlee, A.M.; Sumita, Y.I.; Ella, B.; Naveau, A. Augmented Reality for Interactive Visualization of 3D Maxillofacial Prosthetic Data. Int. J. Prosthodont. 2020, 33, 680–683. [Google Scholar] [CrossRef] [PubMed]
- Tauber, Z.; Lacey, H.; Lichnovska, R.; Erdosova, B.; Zizka, R.; Sedy, J.; Cizkova, K. Students’ Preparedness, Learning Habits and the Greatest Difficulties in Studying Histology in the Digital Era: A Comparison between Students of General and Dental Schools. Eur. J. Dent. Educ. 2020. [Google Scholar] [CrossRef]
- Bonnet, G.; Lance, C.; Bessadet, M.; Tamini, F.; Veyrune, J.L.; Francois, O.; Nicolas, E. Teaching Removable Partial Denture Design: “METACIEL”, a Novel Digital Procedure. Int. J. Med. Educ. 2018, 9, 24–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barour, S.; Richert, R.; Virard, F.; Wulfman, C.; Iozzino, R.; Elbashti, M.; Naveau, A.; Ducret, M. Immersive 3D Educational Contents: A Technical Note for Dental Educators. Healthcare 2021, 9, 178. https://doi.org/10.3390/healthcare9020178
Barour S, Richert R, Virard F, Wulfman C, Iozzino R, Elbashti M, Naveau A, Ducret M. Immersive 3D Educational Contents: A Technical Note for Dental Educators. Healthcare. 2021; 9(2):178. https://doi.org/10.3390/healthcare9020178
Chicago/Turabian StyleBarour, Sabira, Raphaël Richert, François Virard, Claudine Wulfman, Régis Iozzino, Mahmoud Elbashti, Adrien Naveau, and Maxime Ducret. 2021. "Immersive 3D Educational Contents: A Technical Note for Dental Educators" Healthcare 9, no. 2: 178. https://doi.org/10.3390/healthcare9020178