
COVID-19 Delta Variant: Perceptions, Worries, and Vaccine-Booster Acceptability among Healthcare Workers

 ,
,  , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. Statistical Analyses
3. Results
4. Discussion
Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CDC | Centers for Disease Control and Prevention. |
| COVID-19 | coronavirus disease 2019. |
| MOH | Ministry of Health |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2. |
| WHO | World Health Organization. |
Appendix A


{kind=link}
{kind=link}
| Variables | t-Value/df | p-Value |
|---|---|---|
| Worry from Original strain vs. Alpha strain | 8.52/1277 | <0.001 |
| Worry from alpha strain vs. Delta | 1277/14.31 | <0.001 |
| Worry from Delta strain vs. Original strain | 1277/22.62 | <0.001 |
References
- Adam, D. What Scientist Know About New, Fast-Spreading Coronavirus Variants. Available online: https://www.nature.com/articles/d41586-021-01390-4 (accessed on 4 September 2021).
- CDC. Emerging SARS-CoV-2 Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/scientific-brief-emerging-variants.html (accessed on 14 January 2021).
- Lopez, B.J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Lou, F.; Fan, H. SARS-CoV-2 Variants of Concern Delta: A great challenge to prevention and control of COVID-19. Signal Transduct. Target. Ther. 2021, 6, 349. [Google Scholar] [CrossRef] [PubMed]
- Dhar, M.S.; Marwal, R.; Radhakrishnan, V.S.; Ponnusamy, K.; Jolly, B.; Bhoyar, R.C.; Sardana, V.; Naushin, S.; Rophina, M.; Mellan, T.A.; et al. Genomic characterization and epidemiology of an emerging SARS-CoV-2 variant in Delhi, India. Science 2021, eabj9932. [Google Scholar] [CrossRef] [PubMed]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2021, 1–9. [Google Scholar] [CrossRef]
- Alhamlan, F.; Al, -Q.A.; Obeid, D.; Aljumaah, S.; Alghamdi, S.; Alnafee, K.; Alsanea, M.; Alahideb, B.; Almutairi, S.; Alsuwairi, F. SARS-CoV-2 Delta Variant Predominant at a Tertiary-Care Hospital in Saudi Arabia. Res. Sq. Prepr. 2021, 1–20. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Liu, Y.; Rocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021, 28, taab124. [Google Scholar] [CrossRef]
- Dougherty, K.; Mannell, M.; Naqvi, O.; Matson, D.; Stone, J. SARS-CoV-2 B.1.617.2 (Delta) Variant COVID-19 Outbreak Associated with a Gymnastics Facility-Oklahoma. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 1004–1007. [Google Scholar] [CrossRef]
- Farinholt, T.; Doddapaneni, H.; Qin, X.; Menon, V.; Meng, Q.; Metcalf, G.; Chao, H.; Gingras, M.C.; Farinholt, P.; Agrawal, C.; et al. Transmission event of SARS-CoV-2 Delta variant reveals multiple vaccine breakthrough infections. medRxiv 2021, 19, 1–6. [Google Scholar] [CrossRef]
- Delta Variant: What We Know About the Science. Centers for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/delta-variant.html (accessed on 9 August 2021).
- CDC. What You Need to Know About Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant.html (accessed on 4 September 2021).
- Angell, A.L. Rising Cases and the Delta Variant Spur Over 50 Health Care Groups to Support Mandatory Vaccinations for Health Care Employees. Available online: https://www.natlawreview.com/article/rising-cases-and-delta-variant-spur-over-50-health-care-groups-to-support-mandatory (accessed on 4 September 2021).
- Temsah, M.H.; Barry, M.; Aljamaan, F.; Alhuzaimi, A.N.; Al-Eyadhy, A.; Saddik, B.; Alsohime, F.; Alhaboob, A.; Alhasan, K.; Alaraj, A.; et al. SARS-CoV-2 B.1.1.7 UK Variant of Concern Lineage-Related Perceptions, COVID-19 Vaccine Acceptance and Travel Worry Among Healthcare Workers. Fr. Public Health 2021, 9, 686958. [Google Scholar] [CrossRef]
- Temsah, M.H.; Alhuzaimi, A.N.; Alamro, N.; Alrabiaah, A.; Al-Sohime, F.; Alhasan, K.; Kari, J.A.; Almaghlouth, I.; Aljamaan, F.; Al Amri, M.; et al. Knowledge, Attitudes, and Practices of Healthcare Workers During the Early COVID-19 Pandemic in a Main, Academic Tertiary Care Centre in Saudi Arabia. Epidemiol. Infect. 2020, 148, 1–29. [Google Scholar] [CrossRef]
- Temsah, M.H.; Al-Sohime, F.; Alamro, N.; Al-Eyadhy, A.; Al-Hasan, K.; Jamal, A.; Al-Maglouth, I.; Aljamaan, F.; Al Amri, M.; Barry, M.; et al. The psychological impact of COVID-19 pandemic on health care workers in a MERS-CoV endemic country. J. Infect. Public Health 2020, 13, 877–882. [Google Scholar] [CrossRef]
- Barry, M.; Temsah, M.H.; Aljamaan, F.; Saddik, B.; Al-Eyadhy, A.; Alenezi, S.; Alamro, N.; Alhuzaimi, A.N.; Alhaboob, A.; Alhasan, K.; et al. COVID-19 vaccine uptake among healthcare workers in the fourth country to authorize BNT162b2 during the first month of rollout. Vaccine 2021, 39, 5762–5768. [Google Scholar] [CrossRef]
- Temsah, M.H.; Barry, M.; Aljamaan, F.; Alhuzaimi, A.; Al-Eyadhy, A.; Saddik, B.; Alrabiaah, A.; Alsohime, F.; Alhaboob, A.; Alhasan, K.; et al. Adenovirus and RNA-based COVID-19 vaccines’ perceptions and acceptance among healthcare workers in Saudi Arabia: A national survey. BMJ Open 2021, 11, e048586. [Google Scholar] [CrossRef]
- Rabinowitz, L.G.; Rabinowitz, D.G. Women on the Frontline: A Changed Workforce and the Fight Against COVID-19. Acad. Med. 2021, 96, 808–812. [Google Scholar] [CrossRef]
- Parliament, E. Understanding COVID-19s Impact on Women (infographics). Available online: https://www.europarl.europa.eu/news/en/headlines/society/20210225STO98702/understanding-the-impact-of-covid-19-on-women-infographics (accessed on 4 September 2021).
- Barry, M.; Robert, A.A.; Temsah, M.H.; Abdul, B.S.; Akhtar, M.Y.; Al, N.F.; Erlandez, R.; Al, -T.J.A.; Al, K.A.; Al, H.Y. COVID-19 Community Transmission among Healthcare Workers at a Tertiary Care Cardiac Center. Med. Sci. 2021, 9, 49. [Google Scholar] [CrossRef]
- Al Maskari, Z.; Al Blushi, A.; Khamis, F.; Al Tai, A.; Al Salmi, I.; Al Harthi, H.; Al Saadi, M.; Al Mughairy, A.; Gutierrez, R.; Al Blushi, Z. Characteristics of healthcare workers infected with COVID-19: A cross-sectional observational study. Int. J. Infect. Dis. 2021, 102, 32–36. [Google Scholar] [CrossRef]
- Alserehi, H.A.; Alqunaibet, A.M.; Al-Tawfiq, J.A.; Alharbi, N.K.; Alshukairi, A.N.; Alanazi, K.H.; Bin, S.G.M.; Alshehri, A.M.; Almasoud, A.; Hashem, A.M.; et al. Seroprevalence of SARS-CoV-2 (COVID-19) among healthcare workers in Saudi Arabia: Comparing case and control hospitals. Diagn Microbiol. Infect. Dis. 2021, 99, 115273. [Google Scholar] [CrossRef]
- Farsi, S.H.; Alandijany, T.A.; Radwi, M.; Farsi, A.; Bahaaziq, W.; Abushoshah, I.; El-Kafrawy, S.A.; Alsayed, S.; Azhar, E.I.; Boker, A. Prevalence of COVID-19 antibodies among operating room and critical care staff at a tertiary teaching hospital: A cross-sectional study. Saudi Med. J. 2021, 42, 742–749. [Google Scholar] [CrossRef]
- Mohsin, S.F.; Agwan, M.A.; Alsuwaydani, Z.A. Knowledge towards COVID-19 among healthcare students in the central region of Saudi Arabia: A cross-sectional observational study. Postgrad. Med. J. 2021, 97, 448–451. [Google Scholar] [CrossRef]
- Batais, M.A.; Temsah, M.H.; Al-Ghofili, H.; Al-Ruwayshid, N.; Alsohime, F.; Almigbal, T.H.; Al-Rabiaah, A.; Al-Eyadhy, A.A.; Mujammami, M.H.; Halwani, R.; et al. The coronavirus disease of 2019 pandemic-associated stress among medical students in middle east respiratory syndrome-CoV endemic area: An observational study. Medicine 2021, 100, e23690. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Chen, Z.; Fan, Y.; Hu, X.; Wu, T.; Kang, S.; Xiao, B.; Zhang, M. Knowledge, attitudes and anxiety toward COVID-19 among domestic and overseas Chinese college students. J. Public Health 2021, 43, 466–471. [Google Scholar] [CrossRef] [PubMed]
- Le, A.P.; Huynh, G.; Nguyen, H.T.N.; Pham, B.D.U.; Nguyen, T.V.; Tran, T.T.T.; Tran, T.D. Knowledge, Attitude, and Practice Towards COVID-19 Among Healthcare Students in Vietnam. Infect. Drug Resist 2021, 14, 3405–3413. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Pritchard, E.; Matthews, P.; Stoesser, N.B.; Eyre, D.W.; Vihta, K.-D.; House, T.; Hay, J.; Bell, J.; Newton, J. Impact of Delta on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. medRxiv 2021, 1–39. [Google Scholar] [CrossRef]
- Ewen, C. Delta Coronavirus Variant: Scientists Brace for Impact. Available online: https://www.nature.com/articles/d41586-021-01696-3 (accessed on 4 September 2021).
- Del Rio, C.; Malani, P.N.; Omer, S.B. Confronting the Delta Variant of SARS-CoV-2, Summer 2021. JAMA 2021, 326, 1001–1002. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Krammer, F. SARS-CoV-2 vaccines in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef]
- Liu, C.; Ginn, H.M.; Dejnirattisai, W.; Supasa, P.; Wang, B.; Tuekprakhon, A.; Nutalai, R.; Zhou, D.; Mentzer, A.J.; Zhao, Y.; et al. Reduced neutralization of SARS-CoV-2 B.1.617 by vaccine and convalescent serum. Cell 2021, 184, 4220–4236.e4213. [Google Scholar] [CrossRef]
- Ying, B.; Whitener, B.; VanBlargan, L.A.; Hassan, A.O.; Shrihari, S.; Liang, C.Y.; Karl, C.E.; Mackin, S.; Chen, R.E.; Kafai, N.M.; et al. Protective activity of mRNA vaccines against ancestral and variant SARS-CoV-2 strains. bioRxiv 2021, 1–47. [Google Scholar] [CrossRef]
- Iketani, S.; Liu, L.; Nair, M.S.; Mohri, H.; Wang, M.; Huang, Y.; Ho, D.D. A third COVID-19 vaccine shot markedly boosts neutralizing antibody potency and breadth. medRxiv 2021, 1–12. [Google Scholar] [CrossRef]
- CDC. Joint Statement from HHS Public Health and Medical Experts on COVID-19 Booster Shots. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/media/releases/2021/s0818-covid-19-booster-shots.html (accessed on 1 September 2021).
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; Al-Mukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al-Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al-Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 1–15. [Google Scholar] [CrossRef]
- WHO. Delta Variant, a Warning the COVID-19 Virus Is Getting ‘Fitter and Faster’. Available online: https://news.un.org/en/story/2021/07/1096792 (accessed on 2 August 2021).
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Alenezi, S. Understanding the Psychological Stress and Optimizing the Psychological Support for the Acute-Care Health-Care Workers during the COVID-19 Pandemic. Saudi Crit. Care J. 2020, 4, 25. [Google Scholar]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Al, Q.R.M.; Saadon, A.A.; Alarifi, M.I.; Muaygil, R.; Altaymani, Y.K.M.; Elsaid, M.A.M.; Alsohime, F.; Temsah, M.-H.; Aljerian, K. Moral distress among health care workers in the intensive care unit; a systematic review and meta-analysis. Signa Vitae 2021, 17, 192–202. [Google Scholar] [CrossRef]
- Sahashi, Y.; Endo, H.; Sugimoto, T.; Nabeta, T.; Nishizaki, K.; Kikuchi, A.; Matsumoto, S.; Sato, H.; Goto, T.; Hasegawa, K.; et al. Worries and concerns among healthcare workers during the coronavirus 2019 pandemic: A web-based cross-sectional survey. Humanit. Soc. Sci. Commun. 2021, 8, 41. [Google Scholar] [CrossRef]
- Kupferschmidt, K.; Wadman, M. Delta Variant Triggers New Phase in the Pandemic. Available online: https://www.science.org/lookup/doi/10.1126/science.372.6549.1375 (accessed on 4 September 2021).
- Schmidt, T.; Klemis, V.; Schub, D.; Mihm, J.; Hielscher, F.; Marx, S.; Abu, A.-O.; Ziegler, L.; Guckelmus, C.; Urschel, R.; et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 2021, 27, 1530–1535. [Google Scholar] [CrossRef]
- Salerno, L.; Craxì, L.; Amodio, E.; Lo Coco, G. Factors Affecting Hesitancy to mRNA and Viral Vector COVID-19 Vaccines among College Students in Italy. Vaccines 2021, 9, 927. [Google Scholar] [CrossRef]
- Suryadevara, M. Vaccine Mandates. In Vaccines; Springer: Cham, Switzerland, 2021; pp. 441–446. [Google Scholar] [CrossRef]
- MoH. COVID-19 Guidelines. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Pages/covid19.aspx (accessed on 4 September 2021).
- CDC. Healthcare Workers: Information on COVID-19. Available online: https://www.cdc.gov/coronavirus/2019-nCoV/hcp/index.html (accessed on 4 September 2021).
- Datta, R.; Yadav, A.K.; Singh, A.; Datta, K.; Bansal, A. The infodemics of COVID-19 amongst healthcare professionals in India. Med. J. Armed Forces India 2020, 76, 276–283. [Google Scholar] [CrossRef]
- MoH. MOH Urges People to Seek Health Information from Official and Reliable Sources. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-06-15-003.aspx (accessed on 4 September 2021).
- Elharake, J.A.; Galal, B.; Alqahtani, S.A.; Kattan, R.F.; Barry, M.A.; Temsah, M.H.; Malik, A.A.; McFadden, S.M.; Yildirim, I.; Khoshnood, K.; et al. COVID-19 Vaccine Acceptance among Health Care Workers in the Kingdom of Saudi Arabia. Int. J. Infect. Dis. 2021, 109, 286–293. [Google Scholar] [CrossRef]
- Zdziarski, K.; Landowski, M.; Zabielska, P.; Karakiewicz, B. Subjective Feelings of Polish Doctors after Receiving the COVID-19 Vaccine. Int. J. Environ. Res. Public Health 2021, 18, 6291. [Google Scholar] [CrossRef]
- Cavanaugh, A.M.; Spicer, K.B.; Thoroughman, D.; Glick, C.; Winter, K. Reduced risk of reinfection with SARS-CoV-2 after COVID-19 vaccination—Kentucky, May–June 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1081. [Google Scholar] [CrossRef]
- CDC. COVID-19 Vaccine Booster Shot. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 4 September 2021).
- Chiu, N.C.; Chi, H.; Tu, Y.K.; Huang, Y.N.; Tai, Y.L.; Weng, S.L.; Chang, L.; Huang, D.T.; Huang, F.Y.; Lin, C.Y. To mix or not to mix? A rapid systematic review of heterologous prime-boost COVID-19 vaccination. Expert Rev. Vaccines 2021, 1–10. [Google Scholar] [CrossRef]
- Neidleman, J.; Luo, X.; McGregor, M.; Xie, G.; Murray, V.; Greene, W.C.; Lee, S.A.; Roan, N.R. mRNA vaccine-induced T cells respond identically to SARS-CoV-2 variants of concern but differ in longevity and homing properties depending on prior infection status. bioRxiv 2021, 1–62. [Google Scholar] [CrossRef]
- MoH. MOH Spokesman: One Vaccine Dose Not Enough for Protection Against Delta Variant. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-08-15-007.aspx (accessed on 4 September 2021).

| Parameter | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Female | 795 | 62.2 |
| Male | 484 | 37.8 |
| Age (years), mean (SD) | 38.56 (9.17) | |
| Age group | ||
| 20–30 years | 253 | 19.8 |
| 31–40 years | 581 | 45.4 |
| 41–50 years | 280 | 21.9 |
| >50 years | 165 | 12.9 |
| Nationality | ||
| Saudi | 578 | 45.2 |
| Expatriate | 701 | 54.8 |
| Clinical Role | ||
| Consultant | 316 | 24.7 |
| Assistant consultant/fellow | 93 | 7.3 |
| Resident/registrar/physician in training | 244 | 19.1 |
| Nurse | 533 | 41.7 |
| Others: pharmacist, lab technician (radiology and anesthesia) | 92 | 7.2 |
| Health institution working area | ||
| ICU | 228 | 17.8 |
| ER | 126 | 9.9 |
| OR | 79 | 6.2 |
| Isolation ward | 48 | 3.8 |
| General ward | 363 | 28.4 |
| OPD | 287 | 22.5 |
| Non-clinical area | 66 | 5.2 |
| Hospital auxiliary units: radiology, sleep lab, pharmacy | 81 | 6.3 |
| Hospital setting | ||
| Private | 254 | 19.9 |
| Public/governmental | 448 | 35 |
| University hospital | 577 | 45.1 |
| Hospital type of practice | ||
| Primary healthcare center | 192 | 15 |
| Secondary-care hospital | 204 | 15.9 |
| Tertiary hospital | 883 | 69 |
| Travel during the last three months to a country where the Delta variant has been recorded | ||
| No | 1187 | 92.9 |
| Yes | 91 | 7.1 |
| Have you been in contact with people infected with COVID-19? | ||
| Never | 303 | 23.7 |
| Yes, with patients or family members | 975 | 76.3 |
| Have you previously been diagnosed with PCR-positive COVID-19? | ||
| No | 982 | 76.8 |
| Yes | 296 | 23.2 |
| HCWs’ Perceived Travel Worry Level. Mean (SD) | 2.32 (1.1) |
|---|---|
| HCWs’ perceived worry level relating to COVID-19 strains | |
| The original COVID-19 strain. Mean (SD) | 3.14 (1.12) |
| The Alpha variant. Mean (SD) | 1.98 (1.1) |
| The Delta variant. Mean (SD) | 1.79 (1.00) |
| HCW Practices/Perception | Frequency | Percentage |
|---|---|---|
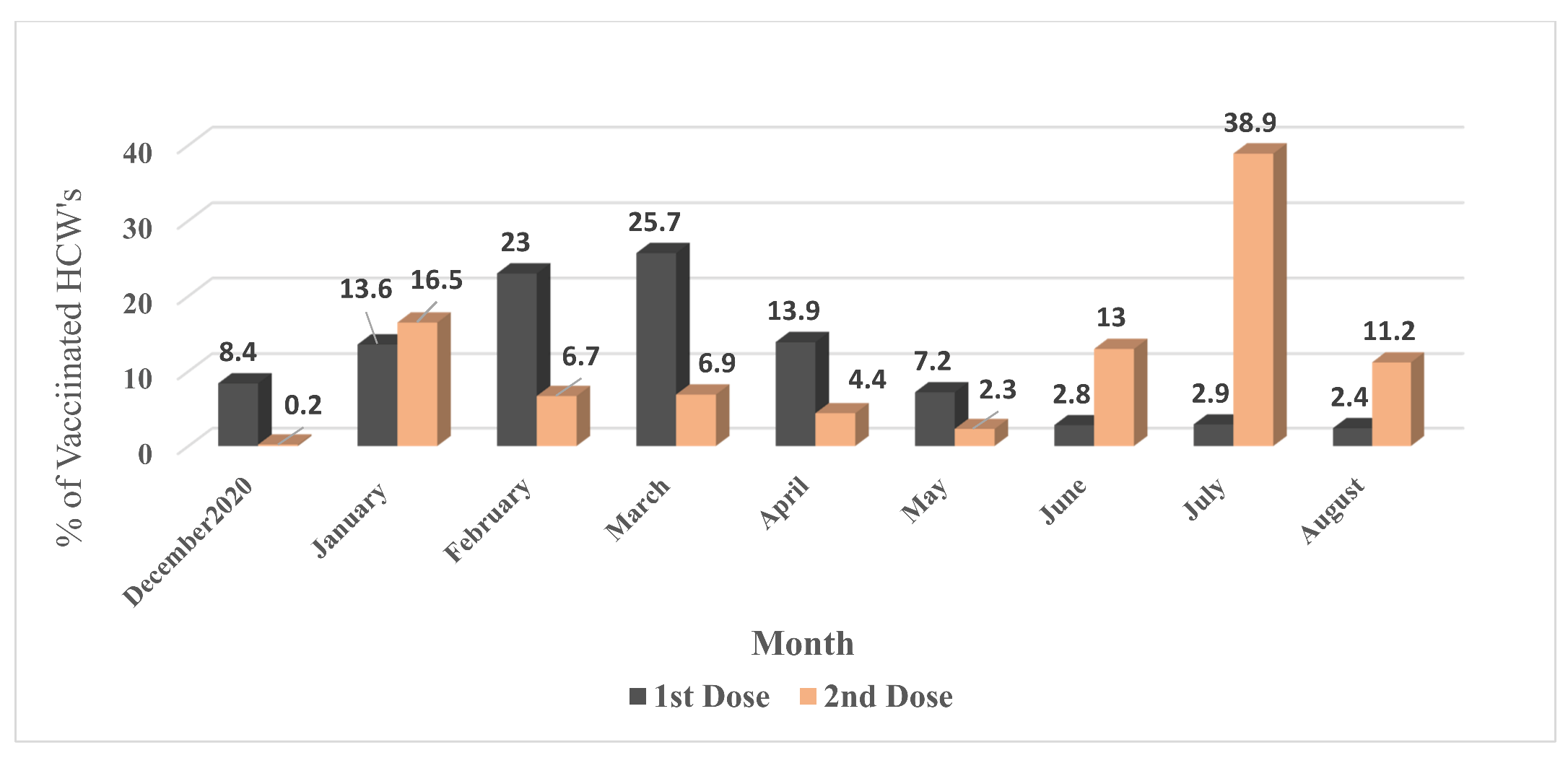
| What vaccine type did you take for your first dose of COVID-19 vaccine? | ||
| Pfizer | 683 | 53.4 |
| AstraZeneca | 587 | 45.9 |
| Not received | 8 | 0.6 |
| What was the type of the second dose of COVID-19 vaccine you took? | ||
| Pfizer | 884 | 69.2 |
| AstraZeneca | 194 | 15.2 |
| Not received Yet | 200 | 15.6 |
| Have you heard about/do you know about the Delta COVID-19 viral mutant? | ||
| Yes: I know a lot about this topic | 367 | 28.7 |
| Yes: I know limited information | 815 | 63.8 |
| No | 96 | 7.5 |
| Have you heard about/do you know about the New Delta-Plus COVID-19 viral mutant? | ||
| Yes: I know a lot about this topic | 187 | 14.6 |
| Yes: I know limited information | 612 | 47.9 |
| No | 479 | 37.5 |
| The AstraZeneca COVID-19 vaccine is effective against the Delta variant, mean (S.D.) Likert agreement score | 3.59 (0.76) | |
| The Pfizer COVID-19 vaccine is effective against the Delta variant, mean (S.D.) Likert agreement score | 3.71 (0.76) | |
| Mixing and matching one AstraZeneca vaccine and one Pfizer vaccine is effective against the Delta variant, mean (S.D.) Likert agreement score | 3.66 (0.80) | |
| To help prevent the further spread of the Delta variant, a third booster dose of the COVID-19 vaccine will likely be needed, mean (S.D.) Likert agreement score | 3.67 (0.94) | |
| What type of vaccine would you prefer to receive for the third booster COVID-19 vaccine? n = 708 | ||
| Same as the first vaccine type | 229 | 32.3 |
| Same as the second vaccine type | 131 | 18.5 |
| A new mRNA vaccine that is developed to cover the Delta variant better | 223 | 31.5 |
| Another vaccine, not mRNA type | 6 | 0.8 |
| It does NOT matter; I would be okay with receiving any mRNA vaccine as a third booster | 119 | 16.8 |
| In your opinion, who should receive a third booster COVID-19 vaccine dose? | ||
| Elderly people | 546 | 77.1 |
| Patients with diabetes | 466 | 65.8 |
| Patients with cardiovascular disease such as hypertension | 442 | 62.4 |
| Patients with chronic renal disease | 442 | 62.4 |
| Patients with immune deficiency | 488 | 68.9 |
| Healthcare workers | 551 | 77.8 |
| Obesity | 255 | 36 |
| All people and JCW travel jobs | 58 | 8.2 |
| Children | 11 | 1.6 |
| HCW Practices/Perceptions | Frequency | Percentage |
|---|---|---|
| To the best of your knowledge, is the Delta variant currently circulating in the KSA | ||
| Unsure | 39 | 3.1 |
| Yes | 511 | 40 |
| No | 728 | 57 |
| This Delta variant has the potential to cause a new COVID-19 wave in the KSA | ||
| Agree | 844 | 66 |
| Neither agree nor disagree | 368 | 28.8 |
| Disagree | 66 | 5.2 |
| A second national lockdown may be implemented if a Delta variant outbreak occurs | ||
| Agree | 708 | 55.4 |
| Neither agree nor disagree | 408 | 31.9 |
| Disagree | 162 | 12.7 |
| Due to the new COVID-19 mutations, healthcare workers should continue universal masking | ||
| Agree | 1076 | 84.2 |
| Neither agree or disagree | 190 | 14.9 |
| Disagree | 12 | 0.9 |
| Respondents’ Knowledge Statement (TRUE or FALSE) * | Incorrect Answer (%) | Correct Answer (%) |
|---|---|---|
| This COVID-19 Delta variant was first described in India (TRUE) | 268 (21) | 1010 (79) |
| The Delta variant is as transmissible as chickenpox (TRUE) | 591 (46.2) | 687 (53.8) |
| Mixing and matching the COVID-19 vaccine offers more protection against the Delta variant (TRUE) | 460 (36) | 818 (64) |
| The signs and symptoms of the Delta strain of COVID-19 are the same as those of the original strain (FALSE) | 933 (73) | 345 (27) |
| The COVID-19 mutations are expected (TRUE) | 122 (9.5) | 1156 (90.5) |
| The Delta variant causes more severe disease than the original strain (TRUE) | 276 (21.6) | 1002 (78.4) |
| The appearance of mutagenic viruses is a sign that herd immunity is occurring (FALSE) | 1068 (83.6) | 210 (16.4) |
| The mutation may cause a false negative PCR result (TRUE) | 1072 (83.9) | 206 (16.1) |
| Treatment for the disease caused by the mutation is similar to the protocol used for COVID-19 treatment (TRUE). | 423 (33.1) | 855 (66.9) |
| Clinical Role No. (%) Knowledge Parameter | Consultant | Assistant Consultant/Fellow | Resident/Registrar/ Physician in Training | Nurses | Technicians | p-Value |
|---|---|---|---|---|---|---|
| HCWs’ Delta variant knowledge score | ||||||
| Low score (≤55.6%) | 177 (56) | 55 (59.1) | 163 (66.8) | 342 (64.2) | 67 (72.8) | 0.012 |
| High score (>55.6%) | 139 (44) | 38 (40.9) | 81 (33.2) | 191 (35.8) | 25 (27.2) | |
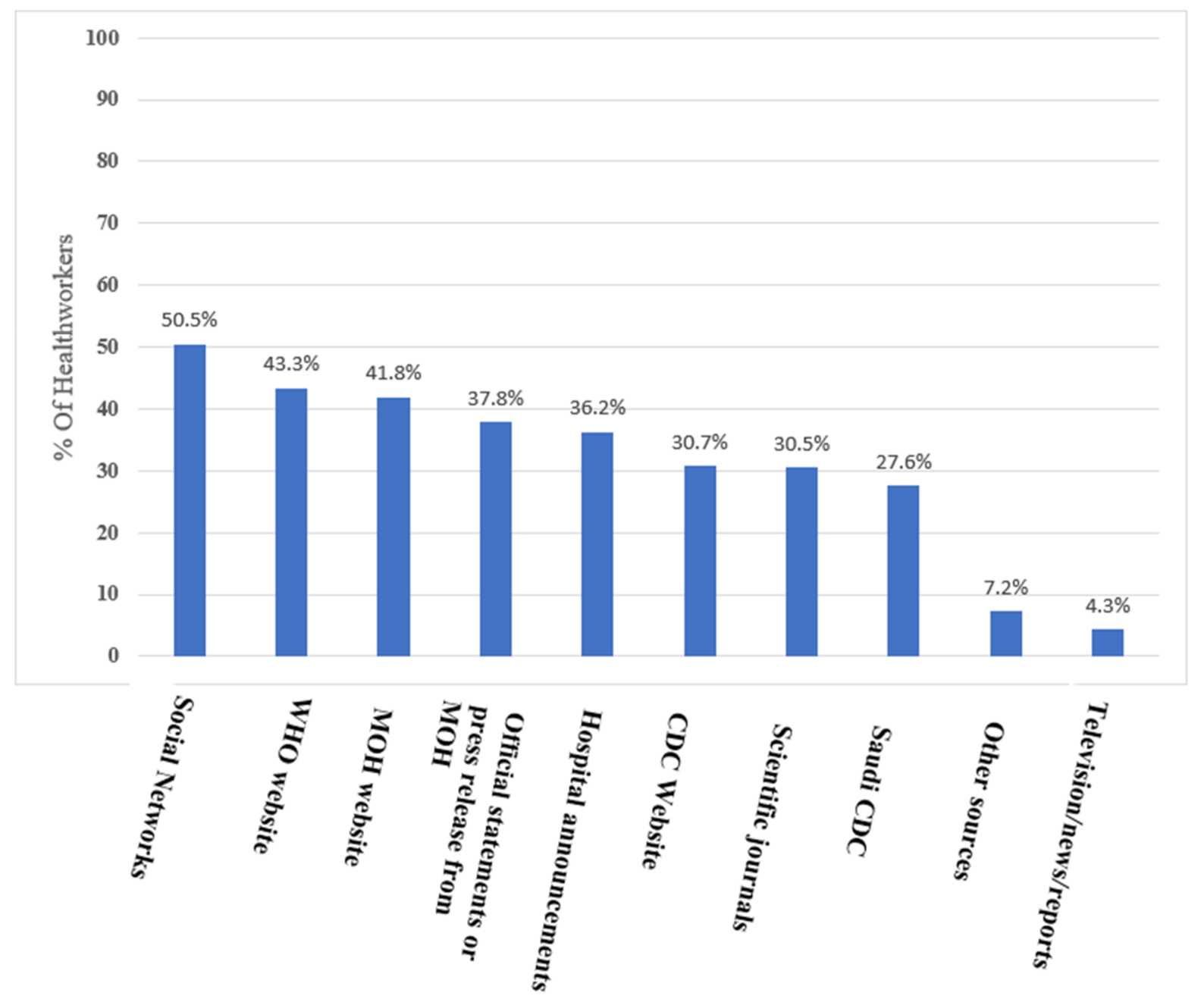
| Source of information | ||||||
| Hospital announcements (e.g., roll-ups or newsletters) | 107 (33.9) | 23 (24.7) | 68 (27.9) | 202 (37.9) | 33 (35.9) | 0.022 |
| Official statements or press release from MOH (e.g., through SMS or newspapers) | 123 (38.9) | 40 (43) | 90 (36.9) | 163 (30.6) | 36 (39.1) | 0.036 |
| MOH website | 111 (35.1) | 33 (35.5) | 90 (36.9) | 225 (42.2) | 41 (44.6) | 0.169 |
| WHO website | 122 (38.6) | 26 (28) | 91 (37.3) | 243 (45.6) | 36 (39.1) | 0.010 |
| CDC Website | 117 (37) | 26 (28) | 68 (27.9) | 131 (24.6) | 25 (27.2) | 0.004 |
| Saudi CDC | 96 (30.4) | 23 (24.7) | 68 (27.9) | 120 (22.5) | 22 (23.9) | 0.123 |
| Social Networks (such as YouTube, Facebook, Twitter, WhatsApp) | 104 (32.9) | 36 (38.7) | 98 (40.2) | 326 (61.2) | 39 (42.4) | <0.001 |
| Scientific journals | 151 (47.8) | 32 (34.4) | 69 (28.3) | 87 (16.3) | 25 (27.2) | <0.001 |
| Other sources | 17 (5.4) | 5 (5.4) | 10 (4.1) | 53 (9.9) | 1 (1.1) | 0.002 |
| Television/news/reports | 13 (4.1) | 5 (5.4) | 7 (2.9) | 24 (4.5) | 4 (4.3) | 0.820 |
| Parameters | HCWs’ Perception Third Dose is Needed to Prevent the Spread of the Delta Variant | Knowledge of Delta Variant | Travel Worry Level | COVID-19 Original Strain Worry Level | Alpha Strain Worry Level | Delta Strain Worry Level | AstraZeneca Vaccine Effective Against Delta | Pfizer Vaccine Effective Against Delta |
|---|---|---|---|---|---|---|---|---|
| Knowledge of Delta variant | 0.143 ** | |||||||
| Travel worry level | 0.048 | 0.114 ** | ||||||
| COVID-19 original strain worry level | 0.049 | −0.077 ** | 0.629 ** | |||||
| Alpha strain worry level | 0.012 | −0.128 ** | 0.570 ** | 0.722 ** | ||||
| Delta strain worry level | 0.072 * | 0.066 * | 0.696 ** | 0.677 ** | 0.679 ** | |||
| AstraZeneca vaccine effective against Delta | 0.201 ** | 0.172 ** | −0.029 | −0.055 * | −0.081 ** | −0.073 ** | ||
| Pfizer vaccine effective against Delta | 0.295 ** | 0.213 ** | −0.010 | −0.042 | −0.091 ** | −0.036 | 0.649 ** | |
| Vaccine mix/match effective against Delta | 0.295 ** | 0.259 ** | 0.017 | −0.048 | −0.087 ** | −0.012 | 0.565 ** | 0.579 ** |
| Variable | Unstandardized Beta Coefficients | 95.0% C.l. for Beta Coefficient | p-Value | |
|---|---|---|---|---|
| Lower Bound | Upper Bound | |||
| Sex = Male | 0.089 | −0.019 | 0.196 | 0.106 |
| Age (years) | −0.002 | −0.008 | 0.003 | 0.450 |
| Nationality = Saudi | −0.117 | −0.220 | −0.013 | 0.027 |
| Previous exposure to people infected with COVID-19 | 0.077 | −0.038 | 0.193 | 0.189 |
| To the best of your knowledge, is the Delta variant currently circulating in KSA | −0.081 | −0.172 | 0.010 | 0.081 |
| Overall knowledge of Delta COVID-19 mutation | 0.006 | −0.029 | 0.042 | 0.723 |
| Had taken first and second COVID-19 vaccine doses | 0.182 | 0.048 | 0.316 | 0.008 |
| Delta variant has the potential to cause a new wave in the KSA | 0.073 | −0.018 | 0.163 | 0.116 |
| A second national lockdown may be implemented if a Delta variant outbreak occurs | 0.124 | 0.051 | 0.198 | 0.001 |
| Due to the new COVID-19 mutations, HCWs should continue universal masking | 0.141 | 0.006 | 0.277 | 0.041 |
| Awareness about the Delta variant | 0.097 | 0.007 | 0.186 | 0.034 |
| The AstraZeneca vaccine is effective against the Delta variant | −0.059 | −0.147 | 0.029 | 0.188 |
| The Pfizer vaccine is effective against the Delta variant | 0.224 | 0.134 | 0.314 | <0.001 |
| Vaccine mixing/matching is effective against the Delta variant | 0.220 | 0.141 | 0.298 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhasan, K.; Aljamaan, F.; Temsah, M.-H.; Alshahrani, F.; Bassrawi, R.; Alhaboob, A.; Assiri, R.; Alenezi, S.; Alaraj, A.; Alhomoudi, R.I.; et al. COVID-19 Delta Variant: Perceptions, Worries, and Vaccine-Booster Acceptability among Healthcare Workers. Healthcare 2021, 9, 1566. https://doi.org/10.3390/healthcare9111566
Alhasan K, Aljamaan F, Temsah M-H, Alshahrani F, Bassrawi R, Alhaboob A, Assiri R, Alenezi S, Alaraj A, Alhomoudi RI, et al. COVID-19 Delta Variant: Perceptions, Worries, and Vaccine-Booster Acceptability among Healthcare Workers. Healthcare. 2021; 9(11):1566. https://doi.org/10.3390/healthcare9111566
Chicago/Turabian StyleAlhasan, Khalid, Fadi Aljamaan, Mohamad-Hani Temsah, Fatimah Alshahrani, Rolan Bassrawi, Ali Alhaboob, Rasha Assiri, Shuliweeh Alenezi, Ali Alaraj, Reham I. Alhomoudi, and et al. 2021. "COVID-19 Delta Variant: Perceptions, Worries, and Vaccine-Booster Acceptability among Healthcare Workers" Healthcare 9, no. 11: 1566. https://doi.org/10.3390/healthcare9111566