
Mindfulness-Based Interventions to Reduce Burnout in Primary Healthcare Professionals: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
- Population (P): studies that included PHCP.
- Intervention (I): studies that analyzed the effects of MBIs on burnout in PHCP.
- Comparison (C): studies that presented the pre- and post-test results of the Maslach Burnout Inventory.
- Outcomes (O): studies that measured the emotional exhaustion, depersonalization, and personal accomplishment domains of the Maslach Burnout Inventory.
- Study design (S): randomized controlled trials (RCTs) and non-RCTs.
2.3. Study Selection and Data Extraction
2.4. Study Quality and Strength of Recommendation
2.5. Statistical Analysis
3. Results
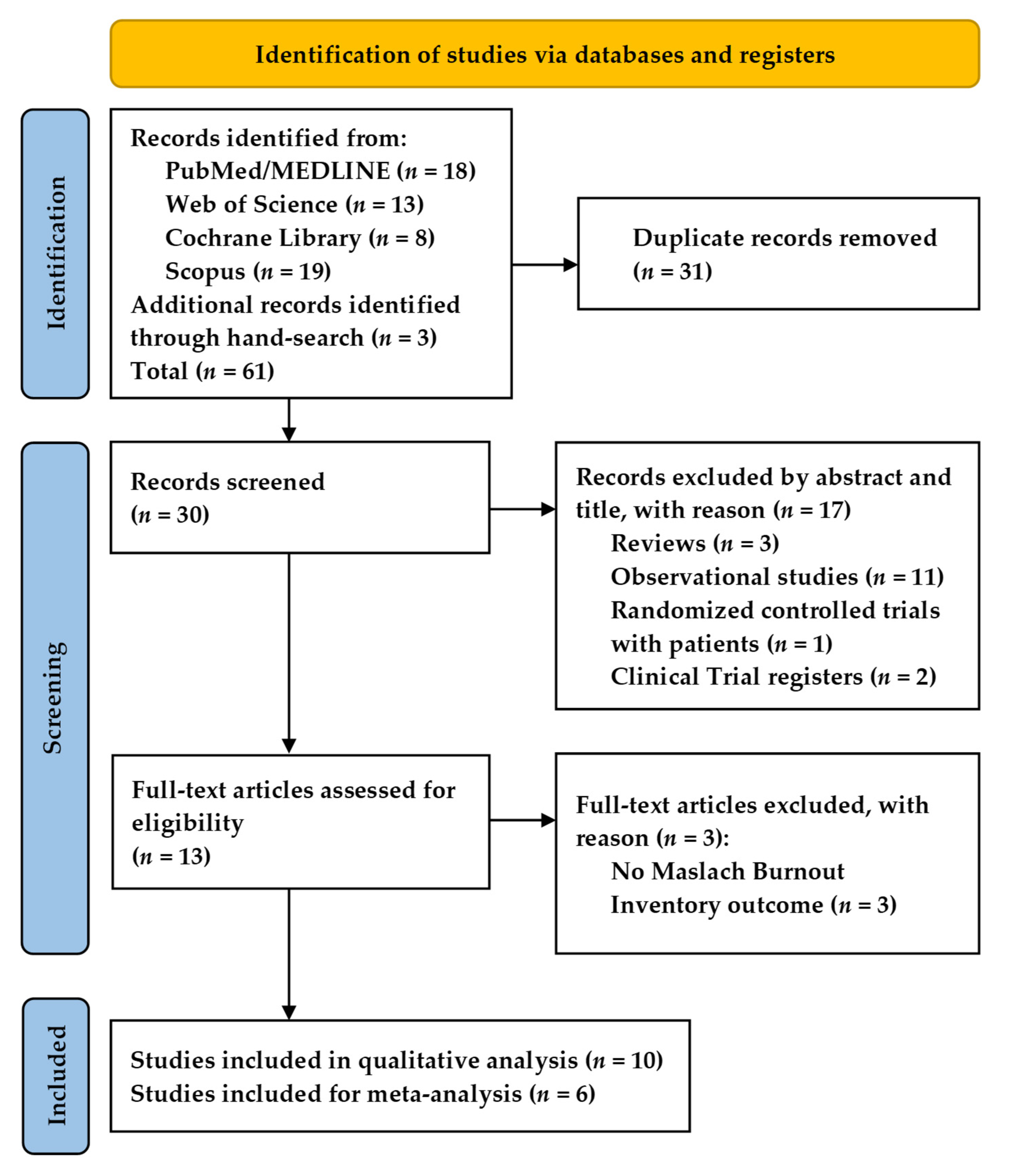
3.1. Study Search Results
3.2. Characteristics of the Included Studies
3.3. Risk of Bias, Level of Evidence, and Strength of Recommendation Assessment
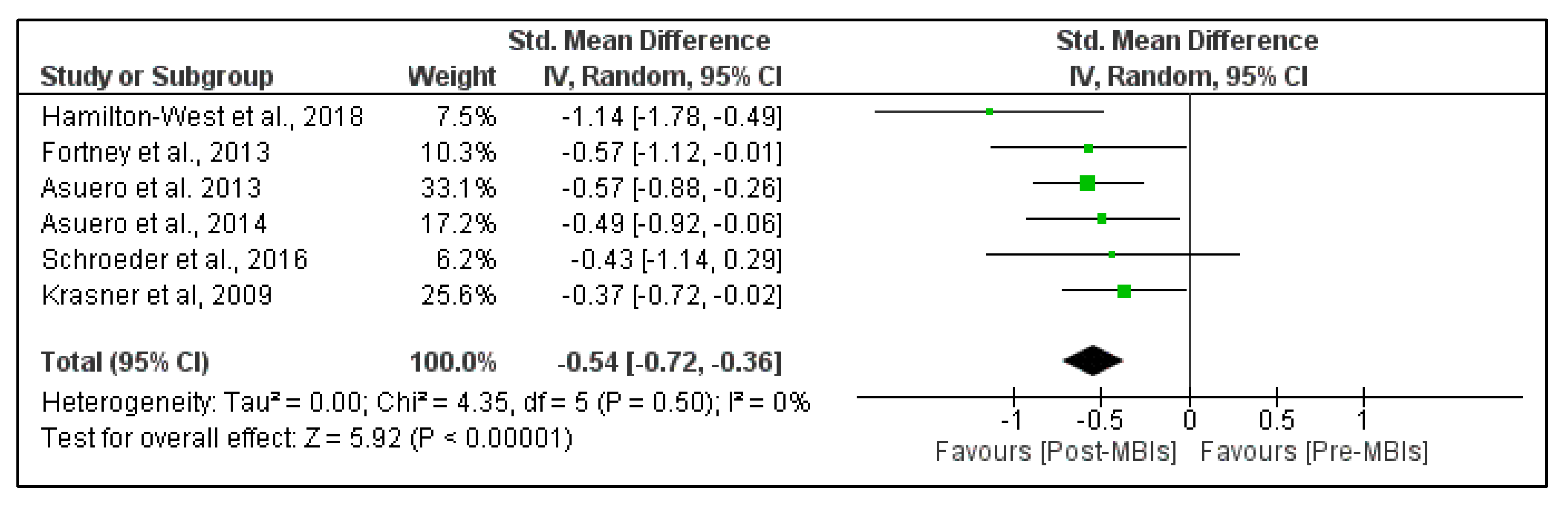
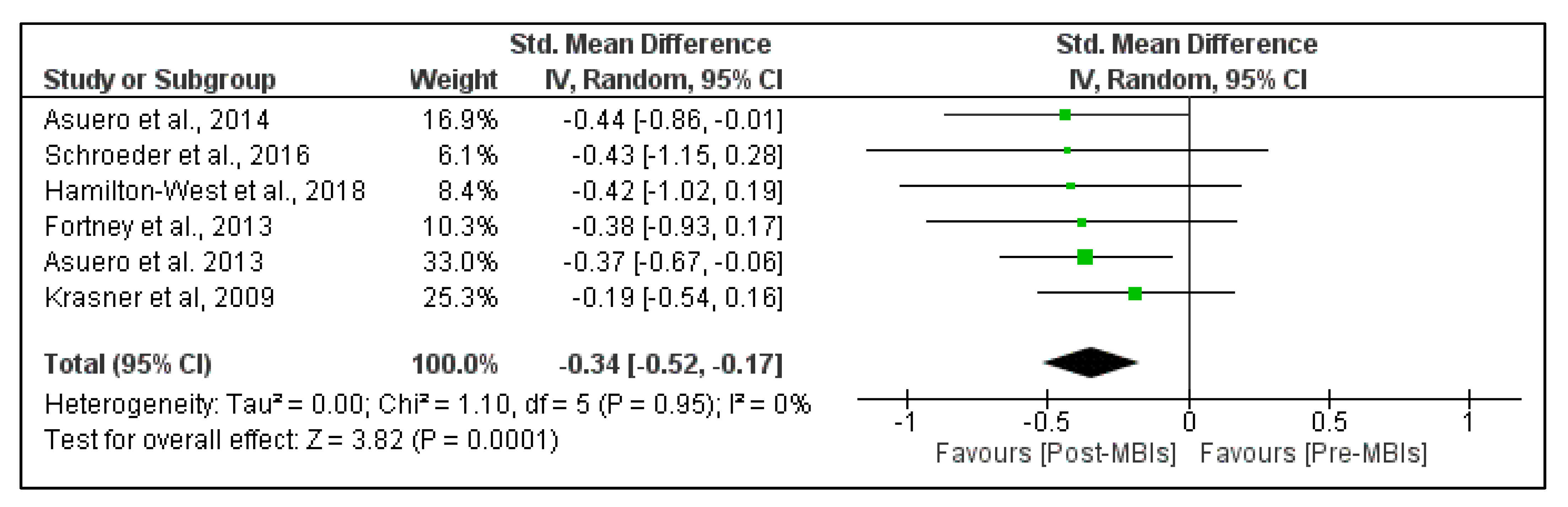
3.4. Meta-Analysis Results
4. Discussion
4.1. Main Findings
4.2. Effectiveness of MBIs on Emotional Exhaustion
4.3. Effectiveness of MBIs on Depersonalization
4.4. Effectiveness of MBIs on Personal Accomplishment
4.5. Strengths and Limitations
4.6. Practical Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2015, 4, CD002892. [Google Scholar] [CrossRef]
- Portoghese, I.; Galletta, M.; Coppola, R.C.; Finco, G.; Campagna, M. Burnout and Workload Among Health Care Workers: The Moderating Role of Job Control. Saf. Health Work 2014, 5, 152–157. [Google Scholar] [CrossRef]
- Cocchiara, R.; Peruzzo, M.; Mannocci, A.; Ottolenghi, L.; Villari, P.; Polimeni, A.; Guerra, F.; La Torre, G. The Use of Yoga to Manage Stress and Burnout in Healthcare Workers: A Systematic Review. J. Clin. Med. 2019, 8, 284. [Google Scholar] [CrossRef] [Green Version]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Han, S.; Shanafelt, T.D.; Sinsky, C.A.; Awad, K.M.; Dyrbye, L.N.; Fiscus, L.C.; Trockel, M.; Goh, J. Estimating the Attributable Cost of Physician Burnout in the United States. Ann. Intern. Med. 2019, 170, 784. [Google Scholar] [CrossRef]
- Canu, I.G.; Mesot, O.; Györkös, C.; Mediouni, Z.; Mehlum, I.S.; Bugge, M.D. Burnout syndrome in Europe: Towards a harmonized approach in occupational health practice and research. Ind. Health 2019, 57, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Jackson, S.; Leiter, M. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Asuero, A.M.; Queraltó, J.M.; Pujol-Ribera, E.; Berenguera, A.; Rodriguez-Blanco, T.; Epstein, R.M. Effectiveness of a Mindfulness Education Program in Primary Health Care Professionals: A Pragmatic Controlled Trial. J. Contin. Educ. Health Prof. 2014, 34, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Fortney, L.; Luchterhand, C.; Zakletskaia, L.; Zgierska, A.; Rakel, D. Abbreviated Mindfulness Intervention for Job Satisfaction, Quality of Life, and Compassion in Primary Care Clinicians: A Pilot Study. Ann. Fam. Med. 2013, 11, 412–420. [Google Scholar] [CrossRef]
- Ferreira, P.L.; Raposo, V.; Tavares, A.I.; Pinto, A. Burnout and health status differences among primary healthcare professionals in Portugal. BMC Fam. Pract. 2021, 22, 81. [Google Scholar] [CrossRef]
- Monsalve-Reyes, C.S.; San Luis-Costas, C.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo, R.; Cañadas-De la Fuente, G.A. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef] [Green Version]
- Soler, J.K.; Yaman, H.; Esteva, M.; Dobbs, F.; Asenova, R.S.; Katic, M.; Ozvacic, Z.; Desgranges, J.P.; Moreau, A.; Lionis, C.; et al. Burnout in European family doctors: The EGPRN study. Fam. Pract. 2008, 25, 245–265. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Boone, S.; Tan, L.; Dyrbye, L.N.; Sotile, W.; Satele, D.; West, C.P.; Sloan, J.; Oreskovich, M.R. Burnout and Satisfaction With Work-Life Balance Among US Physicians Relative to the General US Population. Arch. Intern. Med. 2012, 172, 1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, W.Y.; Ong, J.; Ong, S.; Hao, Y.; Abdullah, H.R.; Koh, D.L.; Mok, U.S.M. The Abbreviated Maslach Burnout Inventory Can Overestimate Burnout: A Study of Anesthesiology Residents. J. Clin. Med. 2019, 9, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasner, M.S.; Epstein, R.M.; Beckman, H.; Suchman, A.L.; Chapman, B.; Mooney, C.J.; Quill, T.E. Association of an Educational Program in Mindful Communication With Burnout, Empathy, and Attitudes Among Primary Care Physicians. JAMA 2009, 302, 1284. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, D.A.; Stephens, E.; Colgan, D.; Hunsinger, M.; Rubin, D.; Christopher, M.S. A Brief Mindfulness-Based Intervention for Primary Care Physicians: A Pilot Randomized Controlled Trial. Am. J. Lifestyle Med. 2016, 12, 83–91. [Google Scholar] [CrossRef] [Green Version]
- Martín Asuero, A.; Rodríguez Blanco, T.; Pujol-Ribera, E.; Berenguera, A.; Moix Queraltó, J. Evaluación de la efectividad de un programa de mindfulness en profesionales de atención primaria. Gac. Sanit. 2013, 27, 521–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranda Auserón, G.; Elcuaz Viscarret, M.R.; Fuertes Goñi, C.; Güeto Rubio, V.; Pascual Pascual, P.; Sainz de Murieta García de Galdeano, E. Evaluación de la efectividad de un programa de mindfulness y autocompasión para reducir el estrés y prevenir el burnout en profesionales sanitarios de atención primaria. Atención Primaria 2018, 50, 141–150. [Google Scholar] [CrossRef]
- Fuertes, C.; Aranda, G.; Rezola, N.; Erramuzpe, A.; Palacios, C.; Ibáñez, B. Long-term effects of a mindfulness and self-compassion program with Primary Healthcare professionals. An. Sist. Sanit. Navar. 2019, 42, 269–280. [Google Scholar] [CrossRef] [Green Version]
- Verweij, H.; Waumans, R.C.; Smeijers, D.; Lucassen, P.L.; Donders, A.R.T.; van der Horst, H.E.; Speckens, A.E. Mindfulness-based stress reduction for GPs: Results of a controlled mixed methods pilot study in Dutch primary care. Br. J. Gen. Pract. 2016, 66, e99–e105. [Google Scholar] [CrossRef] [Green Version]
- Hamilton-West, K.; Pellatt-Higgins, T.; Pillai, N. Does a modified mindfulness-based cognitive therapy (MBCT) course have the potential to reduce stress and burnout in NHS GPs? Feasibility study. Prim. Health Care Res. Dev. 2018, 19, 591–597. [Google Scholar] [CrossRef] [Green Version]
- Sopezki, D.; Andreoni, S.; Montero-Marin, J.; Dias de Castro Filho, E.; Fortes, S.; de Lima, G.G.; Pizutti, L.; Girão, Á.C.; Silva, T.F.; García-Campayo, J.; et al. Feasibility and Effectiveness of a Mindfulness-Based Program Vs. Relaxation in the Treatment of Burnout in Brazilian Primary Care Providers: A Mixed-Methods Pragmatic Controlled Study. Mindfulness 2020, 11, 2573–2588. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Gómez, A.F. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatr. Clin. N. Am. 2017, 40, 739–749. [Google Scholar] [CrossRef]
- Nassim, M.; Park, H.; Dikaios, E.; Potes, A.; Elbaz, S.; Mc Veigh, C.; Lipman, M.; Novak, M.; Trinh, E.; Alam, A.; et al. Brief Mindfulness Intervention vs. Health Enhancement Program for Patients Undergoing Dialysis: A Randomized Controlled Trial. Healthcare 2021, 9, 659. [Google Scholar] [CrossRef] [PubMed]
- Shapero, B.G.; Greenberg, J.; Pedrelli, P.; de Jong, M.; Desbordes, G. Mindfulness-Based Interventions in Psychiatry. Focus 2018, 16, 32–39. [Google Scholar] [CrossRef]
- Ludwig, D.S. Mindfulness in Medicine. JAMA 2008, 300, 1350. [Google Scholar] [CrossRef]
- Del Mar Molero Jurado, M.; Pérez-Fuentes, M.D.C.; Barragán Martín, A.B.; Soriano Sánchez, J.G.; Oropesa Ruiz, N.F.; Sisto, M.; Gázquez Linares, J.J. Mindfulness in Family Caregivers of Persons with Dementia: Systematic Review and Meta-Analysis. Healthcare 2020, 8, 193. [Google Scholar] [CrossRef]
- Amutio-Kareaga, A.; García-Campayo, J.; Delgado, L.; Hermosilla, D.; Martínez-Taboada, C. Improving Communication between Physicians and Their Patients through Mindfulness and Compassion-Based Strategies: A Narrative Review. J. Clin. Med. 2017, 6, 33. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.; Li, T.; Deeks, J. Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions; Higgins, J., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M., Welch, V., Eds.; John Wiley & Sons: Chichester, UK, 2019; pp. 143–176. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Ebell, M.H.; Siwek, J.; Weiss, B.D.; Woolf, S.H.; Susman, J.; Ewigman, B.; Bowman, M. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am. Fam. Physician 2004, 69, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, N.; Sozu, T.; Tajika, A.; Ogawa, Y.; Hayasaka, Y.; Furukawa, T.A. Which is more generalizable, powerful and interpretable in meta-analyses, mean difference or standardized mean difference? BMC Med. Res. Methodol. 2014, 14, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J. Statistical Power Analysis in the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates, Inc.: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Higgins, J.P.T. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lomas, T.; Medina, J.C.; Ivtzan, I.; Rupprecht, S.; Eiroa-Orosa, F.J. A Systematic Review and Meta-analysis of the Impact of Mindfulness-Based Interventions on the Well-Being of Healthcare Professionals. Mindfulness 2019, 10, 1193–1216. [Google Scholar] [CrossRef] [Green Version]
- Spinelli, C.; Wisener, M.; Khoury, B. Mindfulness training for healthcare professionals and trainees: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2019, 120, 29–38. [Google Scholar] [CrossRef]
- Fendel, J.C.; Bürkle, J.J.; Göritz, A.S. Mindfulness-Based Interventions to Reduce Burnout and Stress in Physicians: A Systematic Review and Meta-Analysis. Acad. Med. 2021, 96, 751–764. [Google Scholar] [CrossRef]
- Panagioti, M.; Panagopoulou, E.; Bower, P.; Lewith, G.; Kontopantelis, E.; Chew-Graham, C.; Dawson, S.; van Marwijk, H.; Geraghty, K.; Esmail, A. Controlled Interventions to Reduce Burnout in Physicians. JAMA Intern. Med. 2017, 177, 195. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.G.; Kynoch, K.; Tuckett, A.; Eley, R. Effectiveness of interventions to reduce emergency department staff occupational stress and/or burnout: A systematic review. JBI Evid. Synth. 2020, 18, 1156–1188. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job Burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [Green Version]
- Welp, A.; Meier, L.L.; Manser, T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front. Psychol. 2015, 5, 1573. [Google Scholar] [CrossRef] [Green Version]
- West, C.P.; Dyrbye, L.N.; Shanafelt, T.D. Physician burnout: Contributors, consequences and solutions. J. Intern. Med. 2018, 283, 516–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotstein, S.; Hudaib, A.-R.; Facey, A.; Kulkarni, J. Psychiatrist burnout: A meta-analysis of Maslach Burnout Inventory means. Australas. Psychiatry 2019, 27, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D. Special Report: Suicidal Ideation Among American Surgeons. Arch. Surg. 2011, 146, 54. [Google Scholar] [CrossRef] [PubMed]
- West, C.P. Association of Resident Fatigue and Distress With Perceived Medical Errors. JAMA 2009, 302, 1294. [Google Scholar] [CrossRef] [Green Version]
- Shanafelt, T.D.; Mungo, M.; Schmitgen, J.; Storz, K.A.; Reeves, D.; Hayes, S.N.; Sloan, J.A.; Swensen, S.J.; Buskirk, S.J. Longitudinal Study Evaluating the Association Between Physician Burnout and Changes in Professional Work Effort. Mayo Clin. Proc. 2016, 91, 422–431. [Google Scholar] [CrossRef]
- Poghosyan, L.; Aiken, L.H.; Sloane, D.M. Factor structure of the Maslach burnout inventory: An analysis of data from large scale cross-sectional surveys of nurses from eight countries. Int. J. Nurs. Stud. 2009, 46, 894–902. [Google Scholar] [CrossRef] [Green Version]
- Romani, M.; Ashkar, K. Burnout among physicians. Libyan J. Med. 2014, 9, 23556. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.J.; Sloan, J.; Freischlag, J. Burnout and Medical Errors Among American Surgeons. Ann. Surg. 2010, 251, 995–1000. [Google Scholar] [CrossRef] [Green Version]
- Edwards, P.; Clarke, M.; DiGuiseppi, C.; Pratap, S.; Roberts, I.; Wentz, R. Identification of randomized controlled trials in systematic reviews: Accuracy and reliability of screening records. Stat. Med. 2002, 21, 1635–1640. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Cathébras, P.; Begon, A.; Laporte, S.; Bois, C.; Truchot, D. Épuisement professionnel chez les médecins généralistes. Presse Med. 2004, 33, 1569–1574. [Google Scholar] [CrossRef]
- Lheureux, F.; Truchot, D.; Borteyrou, X. Suicidal tendency, physical health problems and addictive behaviours among general practitioners: Their relationship with burnout. Work Stress 2016, 30, 173–192. [Google Scholar] [CrossRef]
- van der Heijden, F.; Dillingh, G.; Bakker, A.; Prins, J. Suicidal Thoughts Among Medical Residents with Burnout. Arch. Suicide Res. 2008, 12, 344–346. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Thomas, M.R.; Massie, F.S.; Power, D.V.; Eacker, A.; Harper, W.; Durning, S.; Moutier, C.; Szydlo, D.W.; Novotny, P.J.; et al. Burnout and Suicidal Ideation among U.S. Medical Students. Ann. Intern. Med. 2008, 149, 334. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; West, C.P.; Satele, D.; Boone, S.; Tan, L.; Sloan, J.; Shanafelt, T.D. Burnout Among U.S. Medical Students, Residents, and Early Career Physicians Relative to the General U.S. Population. Acad. Med. 2014, 89, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Scheepers, R.A.; Emke, H.; Epstein, R.M.; Lombarts, K.M.J.M.H. The impact of mindfulness-based interventions on doctors’ well-being and performance: A systematic review. Med. Educ. 2020, 54, 138–149. [Google Scholar] [CrossRef]
- Baptista, S.; Teixeira, A.; Castro, L.; Cunha, M.; Serrão, C.; Rodrigues, A.; Duarte, I. Physician Burnout in Primary Care during the COVID-19 Pandemic: A Cross-Sectional Study in Portugal. J. Prim. Care Community Health 2021, 12. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year, Country | Design | Sample | Mindfulness-Based Intervention | Outcomes | Results (Δ; p-Value) |
|---|---|---|---|---|---|
| Krasner et al. [15], 2009, USA | Non-RCT | 70 PHCP (46% women; 100% physicians) | CME course of 8 weeks (27 h): 1 weekly session of 2.5 h, plus 1 extra session of 7 h; mindfulness meditation, didactic and narrative exercises, dialogue groups. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −14.7%; <0.01 D: −11.6%; >0.05 PA: 1.9%; <0.01 |
| Asuero et al. [17], 2013, Spain | Non-RCT | 87 PHCP (90% women; 55% physicians; 39% nurses; 6% social workers and psychologists); 47.3 ± 8.2 years | MBSR course of 8 weeks (28 h): 1 weekly session of 2.5 h, plus 1 extra session of 8 h; contemplation meditation exercises, dialogue groups. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −24.1%; <0.001 D: −23.3%; <0.001 PA: 6.5%; <0.001 |
| Fortney et al. [9], 2013, USA | Non-RCT | 30 PHCP (60% women; 97% physicians; 3% nurses); 40.5 ± 10.1 years | MMC course of 3 sessions (18 h): Friday (3 h) + Saturday (7 h) + Sunday (4 h) + 2 extra sessions of 2 h after the 2 and 4 weeks of the last sessions; mindfulness practices (sitting, movement, breathing, speaking, listening, observing, compassion). | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −17.2%; <0.01 D: −18.3%; <0.05 PA: 8.1%; <0.001 |
| Asuero et al. [8], 2014, Spain | RCT | 43 PHCP (53% physicians; 40% nurses; 7% other); 48.8 ± 7.8 years | MBSR course of 8 weeks (28 h): 1 weekly session of 2.5 h, plus 1 extra session of 8 h; contemplation meditation exercises, dialogue groups. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −22.3%; <0.01 D: −26.5%; <0.01 PA: 5.4%; <0.01 |
| Schroeder et al. [16], 2016, USA | RCT | 16 PHCP (73% women; 100% physicians); 42.8 ± 8.4 years | MMC course of 3 sessions (18 h): Friday (3 h) + Saturday (7 h) + Sunday (4 h) + 2 extra sessions of 2 h after the 2 and 4 weeks of the last sessions; mindfulness practices (sitting, movement, breathing, speaking, listening, observing, compassion). | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −15.8%; <0.001 D: −19.5%; <0.001 PA: 6.2%; <0.001 |
| Verweij et al. [20], 2016, Netherlands | Non-RCT | 23 PHCP (30% women; 100% physicians); 54.5 ± 5.3 years | MBSR course of 8 weeks (28 h): 1 weekly session of 2.5 h, plus 1 extra session of 8 h; contemplation meditation exercises, dialogue groups. | 20-item Maslach Burnout Inventory Dutch version (EE, D, PA); | EE: −4.6%; >0.05 D: −11.2%; <0.05 PA: 3.4%; >0.05 |
| Auserón et al. [18], 2017, Spain | RCT | 23 PHCP (74% women; 52% physicians; 48% nurses); 50.0 ± 7.9 years | Modified MBSR course of 8 weeks (20 h): 1 weekly session of 2.5 h; contemplation meditation exercises, dialogue groups. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: NA; <0.05 D: NA; >0.05 PA: NA; >0.05 |
| Hamilton-West et al. [21], 2018, UK | Non-RCT | 22 PHCP (64% women; 100% physicians); 44.5 ± 7.4 years | Modified MBCT course of 8 weeks (16 h): 1 weekly session of 2 h; contemplation meditation exercises, mindfulness practices, yoga. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: −38.4%; <0.001 D: −27.7%; <0.05 PA: 5.6%; >0.05 |
| Fuertes et al. [19], 2019, Spain | RCT | 41 PHCP (83% women; 49% physicians; 51% nurses); 49.6 ± 8.2 years | Modified MBSR course of 8 weeks (20 h): 1 weekly session of 2.5 h; contemplation meditation exercises, dialogue groups. | 22-item Maslach Burnout Inventory (EE, D, PA) | EE: NA; >0.05 D: NA; >0.05 PA: NA; >0.05 |
| Sopezki et al. [22], 2020, Brazil | Non-RCT | 62 PHCP (95% women); 41.7 ± 11.7 years | Modified MBCT course of 8 weeks (16 h): 1 weekly session of 2 h; mindfulness practices (breathing, speaking, listening, observing, compassion). | 16-item Maslach Burnout Inventory Brazilian version (EE, D, PA) | EE: −9.6%; >0.05 D: −22.4%; >0.05 PA: 0.4%; >0.05 |
| Cochrane Risk of Bias Tool 2.0 | SORT | |||||||
|---|---|---|---|---|---|---|---|---|
| Study, Year | Randomization Process | Deviations from Intended Interventions | Missing Data | Measurement of Outcome | Selection of Reported Results | Overall Risk of Bias | Level of Evidence | Strength of Recommendation |
| Asuero et al. [8], 2014 | Low risk | Some concerns | Low risk | High risk | Low risk | High risk | 2 | B |
| Schroeder et al. [16], 2016 | Low risk | Some concerns | Low risk | High risk | Low risk | High risk | 2 | B |
| Auserón et al. [18], 2017 | Low risk | Some concerns | Low risk | High risk | Low risk | High risk | 2 | B |
| Fuertes et al. [19], 2019 | Low risk | Some concerns | Low risk | High risk | Low risk | High risk | 2 | B |
| Risk of Bias in Non-Randomized Studies of Interventions | SORT | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study, Year | Confounding | Selection of Participants | Classification of Intervention | Deviations from Intended Interventions | Missing Data | Measurement of Outcome | Selection of Reported Result | Overall Risk of Bias | Level of Evidence | Strength of Recommendation |
| Krasner et al. [15], 2009 | Moderate risk | Low risk | Low risk | Moderate risk | Low risk | Serious risk | Low risk | Serious Risk | 2 | B |
| Asuero et al. [17], 2013 | Moderate risk | Low risk | Low risk | Moderate risk | Moderate risk | Serious risk | Low risk | Serious Risk | 2 | B |
| Fortney et al. [9], 2013 | Moderate risk | Low risk | Low risk | Moderate risk | Low risk | Serious risk | Low risk | Serious Risk | 2 | B |
| Verweij et al. [20], 2016 | Moderate risk | Low risk | Low risk | Moderate risk | Low risk | Serious risk | Low risk | Serious Risk | 2 | B |
| Hamilton-West et al. [21], 2018 | Moderate risk | Low risk | Low risk | Moderate risk | Moderate risk | Serious risk | Low risk | Serious Risk | 2 | B |
| Sopezki et al. [22], 2020 | Moderate risk | Low risk | Low risk | Moderate risk | Low risk | Serious risk | Low risk | Serious Risk | 2 | B |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvado, M.; Marques, D.L.; Pires, I.M.; Silva, N.M. Mindfulness-Based Interventions to Reduce Burnout in Primary Healthcare Professionals: A Systematic Review and Meta-Analysis. Healthcare 2021, 9, 1342. https://doi.org/10.3390/healthcare9101342
Salvado M, Marques DL, Pires IM, Silva NM. Mindfulness-Based Interventions to Reduce Burnout in Primary Healthcare Professionals: A Systematic Review and Meta-Analysis. Healthcare. 2021; 9(10):1342. https://doi.org/10.3390/healthcare9101342
Chicago/Turabian StyleSalvado, Mafalda, Diogo Luís Marques, Ivan Miguel Pires, and Nádia Mendes Silva. 2021. "Mindfulness-Based Interventions to Reduce Burnout in Primary Healthcare Professionals: A Systematic Review and Meta-Analysis" Healthcare 9, no. 10: 1342. https://doi.org/10.3390/healthcare9101342