1. Introduction
Growing evidence exists in the literature regarding the use of short dental implants (usually considered as <10 mm in length) for the prosthetic rehabilitation of jaws with reduced vertical bone dimension [
1,
2,
3,
4,
5,
6,
7,
8]. Generally, one of the most challenge clinical condition for implant placement is surely the atrophic posterior maxilla, usually after teeth extraction or jaw surgery, and when the residual bone measures 4.5–6 mm in height on radiograms [
1,
3,
8]. Over time, many surgical techniques as well implant morphologies have been suggested, mostly aimed to avoid sinus floor elevation in such situations, as the latter is frequently characterized by high postoperative morbidity and costs, as well as delayed prosthetic rehabilitation [
1,
2,
3]. Surely, intraoperative (mostly tearing of the Schneiderian membrane as occurring in 7–44% of the procedures, in addition to antral or nasal penetration, bleeding, fenestration, dehiscence or perforation of the alveolar bone, insufficient implant primary stability, etc.) and postoperative complications (pain, swelling, bleeding, edema, hemosinus, sinus infection, sinusitis, graft or fixture migration or loss, oroantral fistula, etc.) are the main factors to consider when a maxillary sinus augmentation is required for implant placement [
4,
5,
6].
In the last two decades, the use of minimally invasive techniques is becoming increasingly widespread in all fields of dentistry, and growing evidence in the literature supports such use [
7,
8].
The current study describes a minimally invasive surgical procedure for the insertion of 80 short spiral implants in the posterior atrophic maxilla (all for single tooth restorations) using a surgical technique of progressive steps that promotes crestal sinus lifting, with a follow-up of 10 years.
2. Materials and Methods
The main inclusion criteria were a residual vertical bone height minimum of 4.5 mm (with a range of from 4.5 to 6 mm) as measured on radiograms (computed tomography (CT) or cone beam computed tomography (CBCT)). No data regarding osteoporosis and possible medical treatments in females were collected, as such information was deemed unnecessary. There were 49 males and 31 females patients with an age range of 27–63 y.o. (median of 37 y.o.). Patients taking oral or i.v. bisphosphonates were excluded from the study. Surgery was conventional (scalpel incision, periosteal flap elevation and stitches) in 30 cases and flapless in the remaining 50 (with software assisted surgical guides—Modelguide, Bionova s.r.l., Italy), always with low-speed drilling and irrigation; adjunctive bio-material has never been used as bone graft. Surgical and prosthetic procedures were performed by the same oral surgeon (SC) to avoid interpersonal differences.
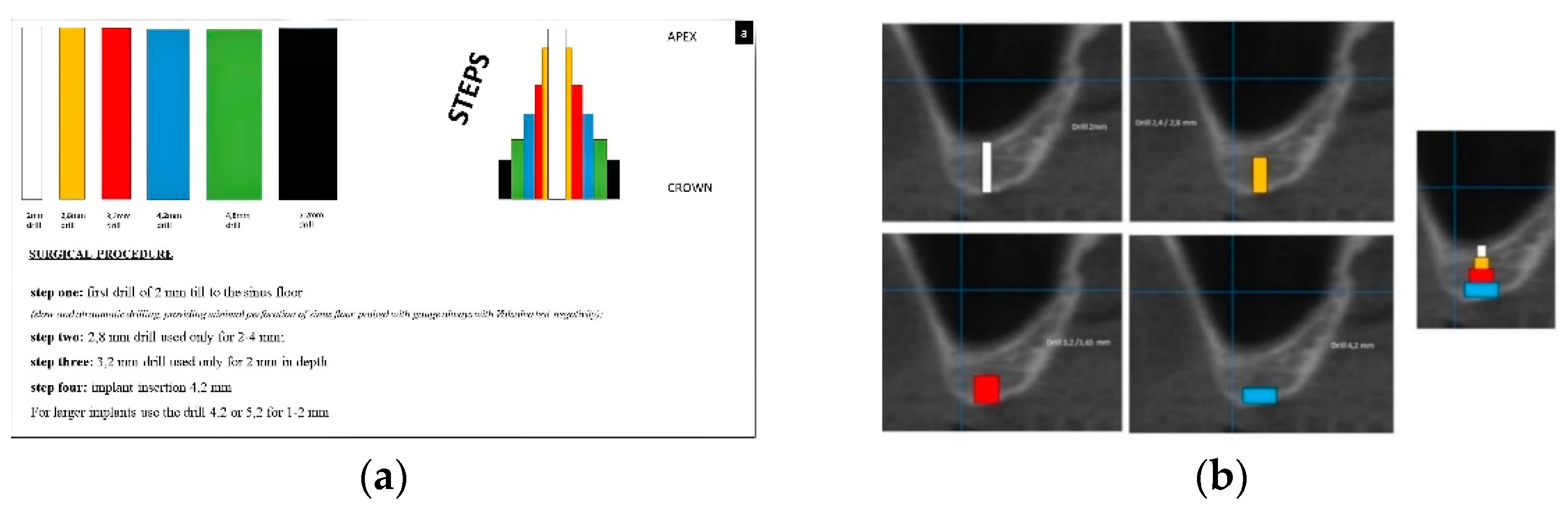
The surgical technique included the following steps:
- -
Step one—the first drill (2 mm in diameter) was used until the sinus floor was reached with atraumatic perforation, the latter probed with a gauge, and the negative status of Valsalva’s test was continuously checked;
- -
Step two—the second drill (2.8 mm in diameter) was used only for a depth of 2–4 mm;
- -
Step three—the third drill (3.2 mm in diameter) was used for only 2 mm in depth;
- -
Step four (optional, only for insertion of an implant of 5 mm in diameter)—the fourth drill (4.1 mm in diameter) was used for 1 mm in depth.
As for the follow-up, peri-implant bone loss was measured directly on a periapical radiograph (as peri-implant bone loss from the fixture–abutment connection to the depth) at the time of re-opening (second surgery for submucosal implants) and two years after prosthetic rehabilitation. Data regarding implant survival after ten years were mostly collected by phone recall (asking the patient if implant rehabilitation was still present or not) as some patients refused additional radiograph or clinical follow-up; thus, data regarding bone loss measurement after ten years are missing.
3. Results
The surgical procedure is explained in detail in
Figure 1a,b.
In all cases, a longer implant (from 2 to 4 mm) than the pre-operative radiological measures was positioned. Only two implants both placed by flapless surgery and with healing cap positioning were lost before the prosthetic rehabilitation, but they were repositioned after 45 days.
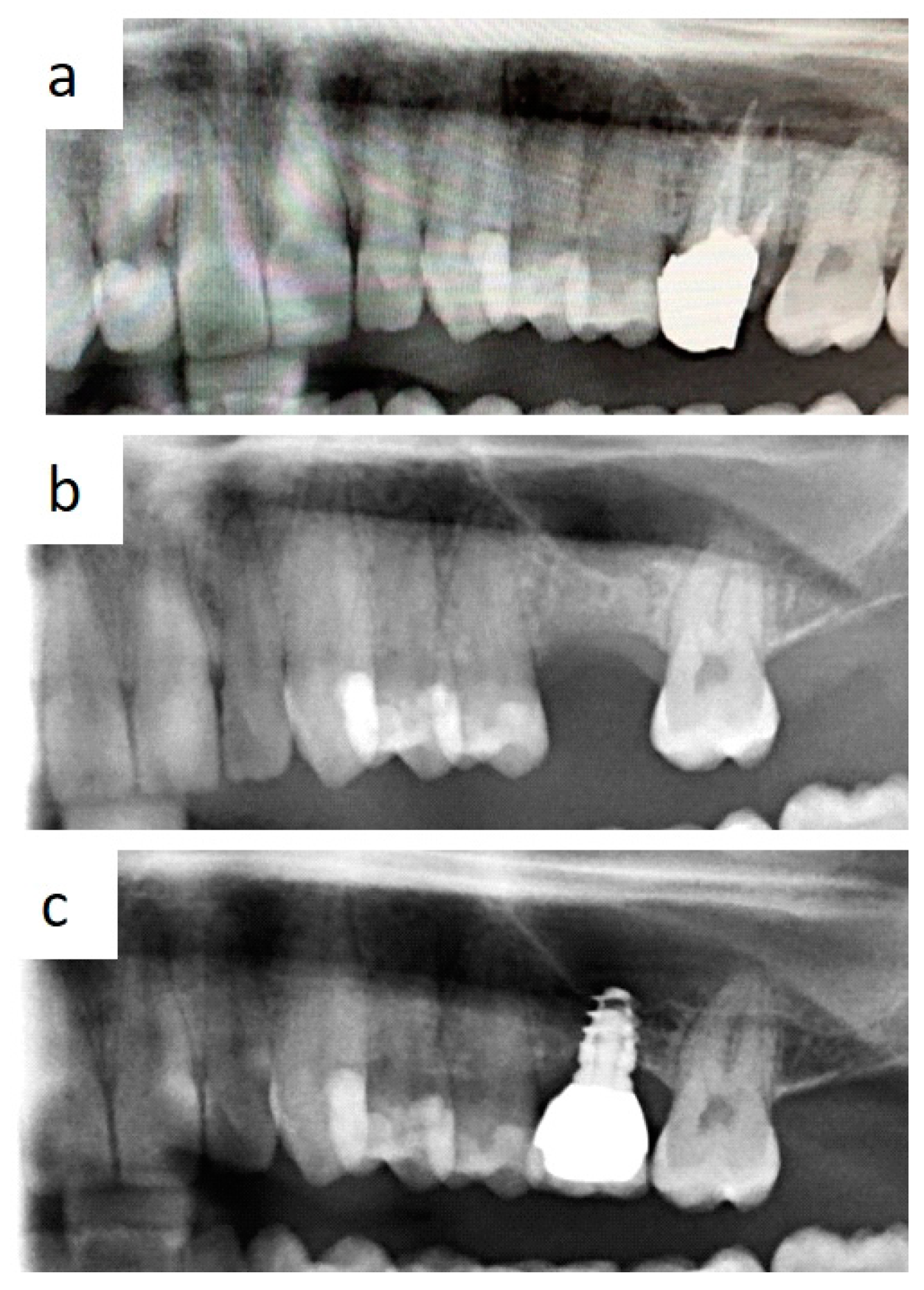
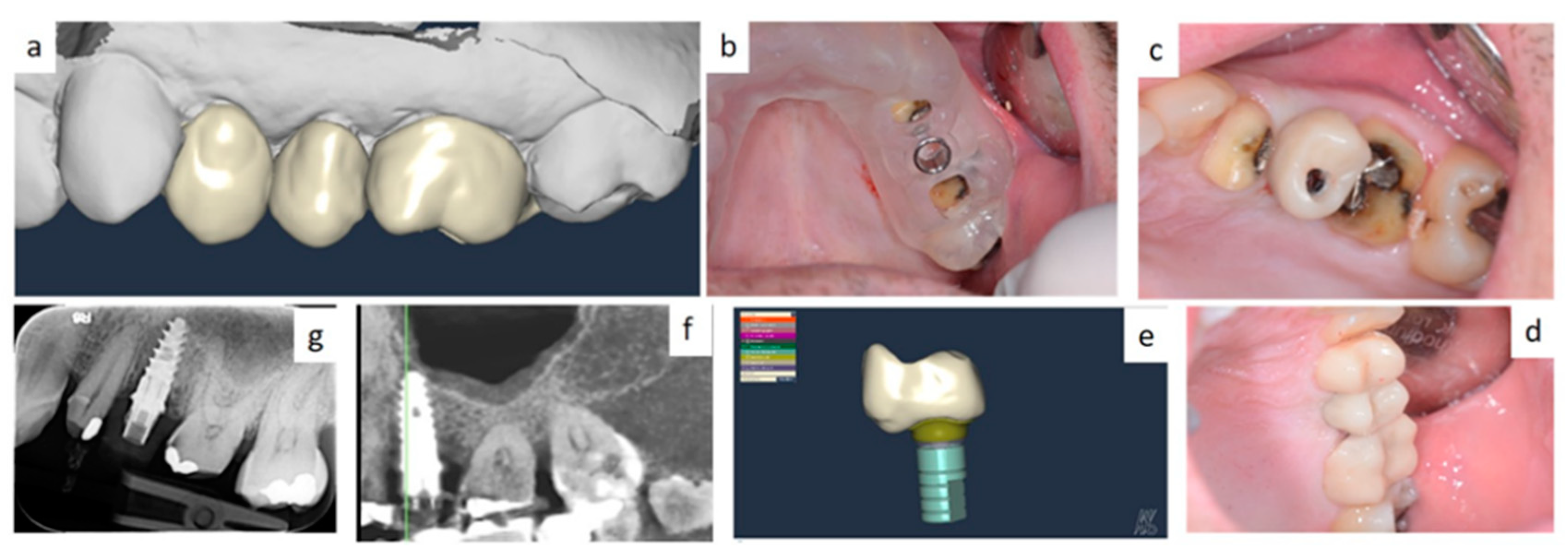
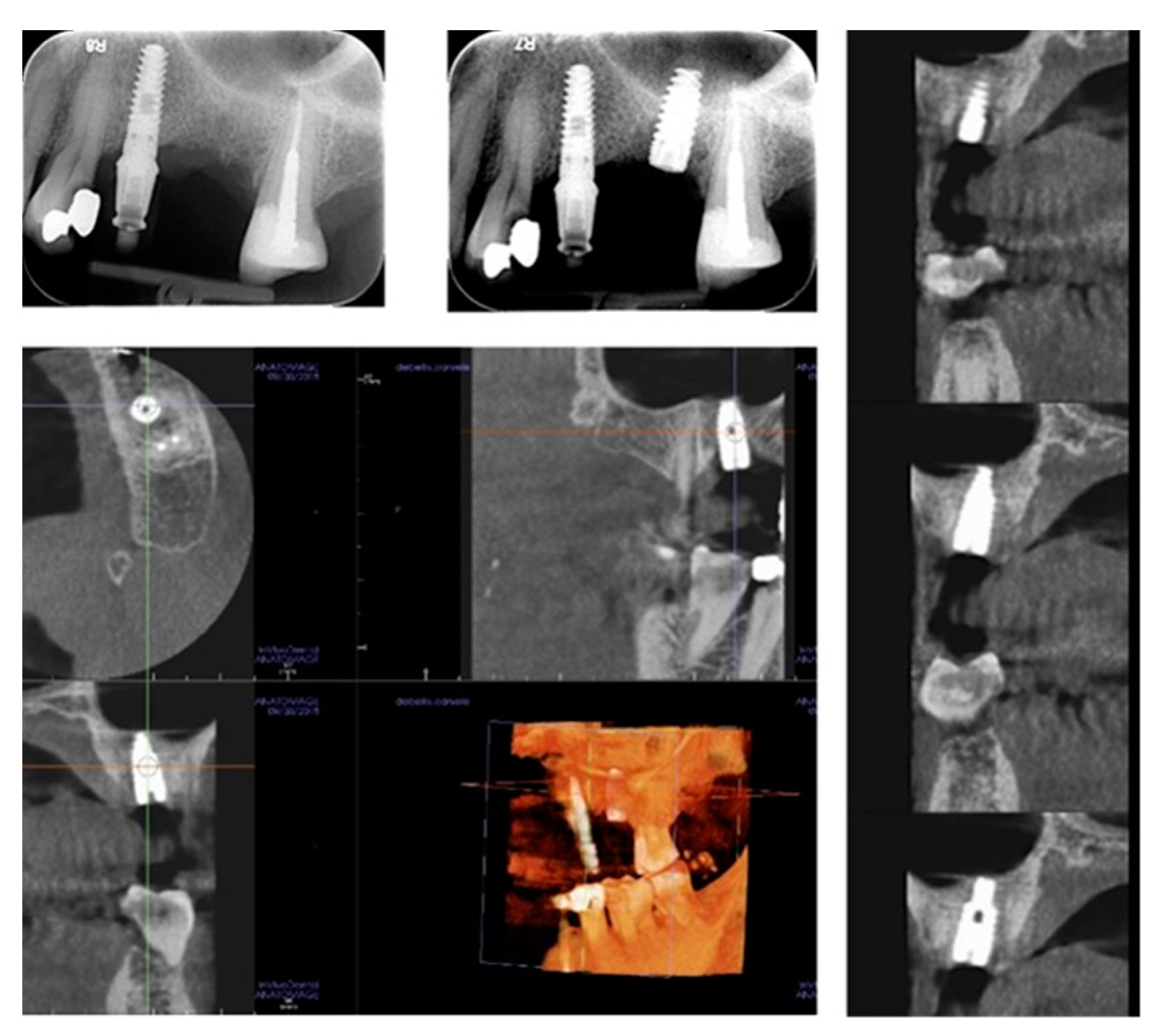
In all cases, fixtures were placed with high insertion torque (up to 50 Ncm) and with atraumatic crestal lifting of the sinus membrane (
Figure 2a–c and
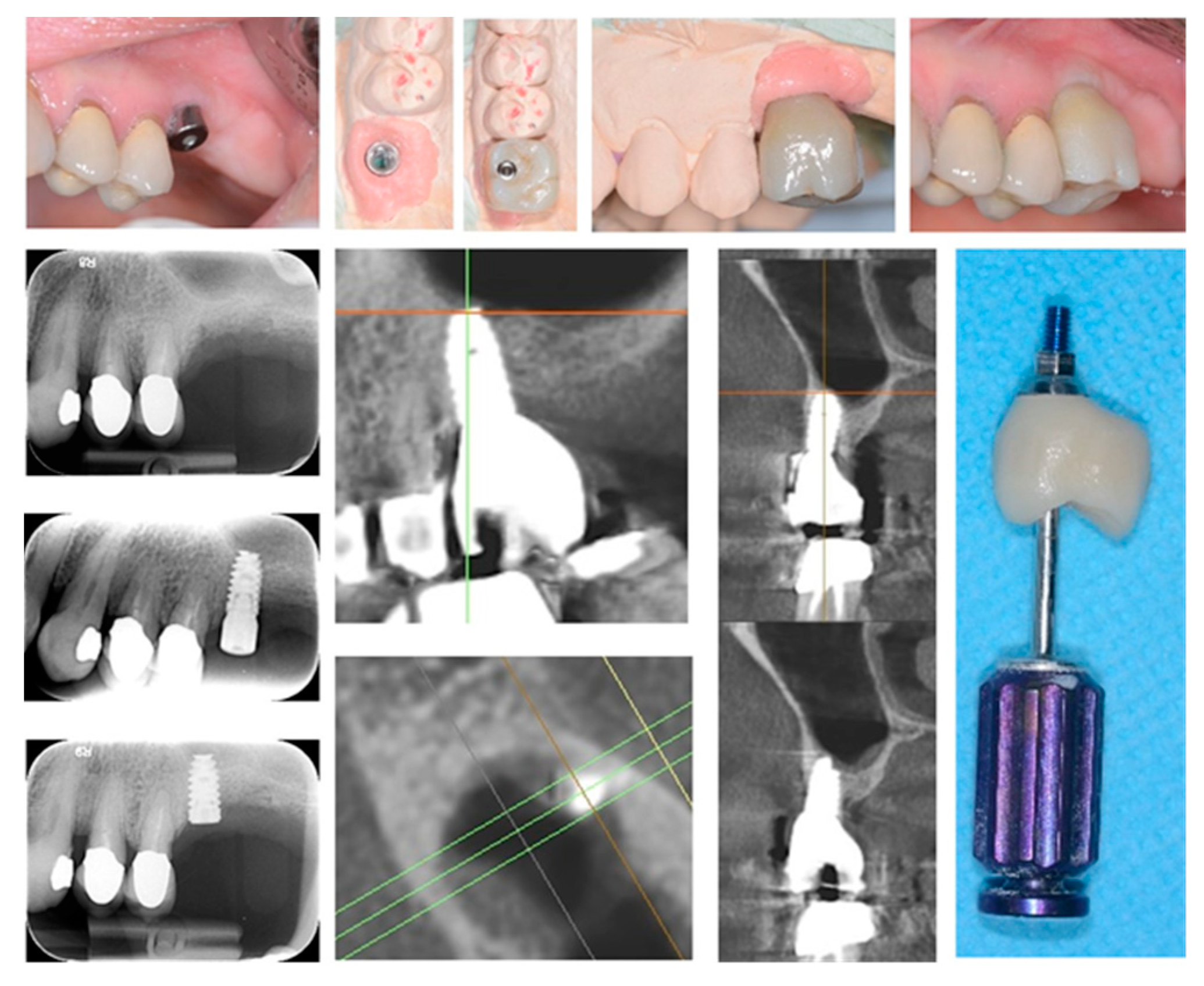
Figure 3a–f). Prostheses were placed 3 months after surgery; more precisely, 40 were cemented metal–ceramic crowns, and the remaining were screwed hybrid ceramic crowns (Vita Enamic Multicolor) with glued titanium bases (
Figure 4). All implants had a diameter of 4.2 mm, and 35 were 6.25 mm in length, while the remaining 45 had a length of 8 mm (
Figure 5).
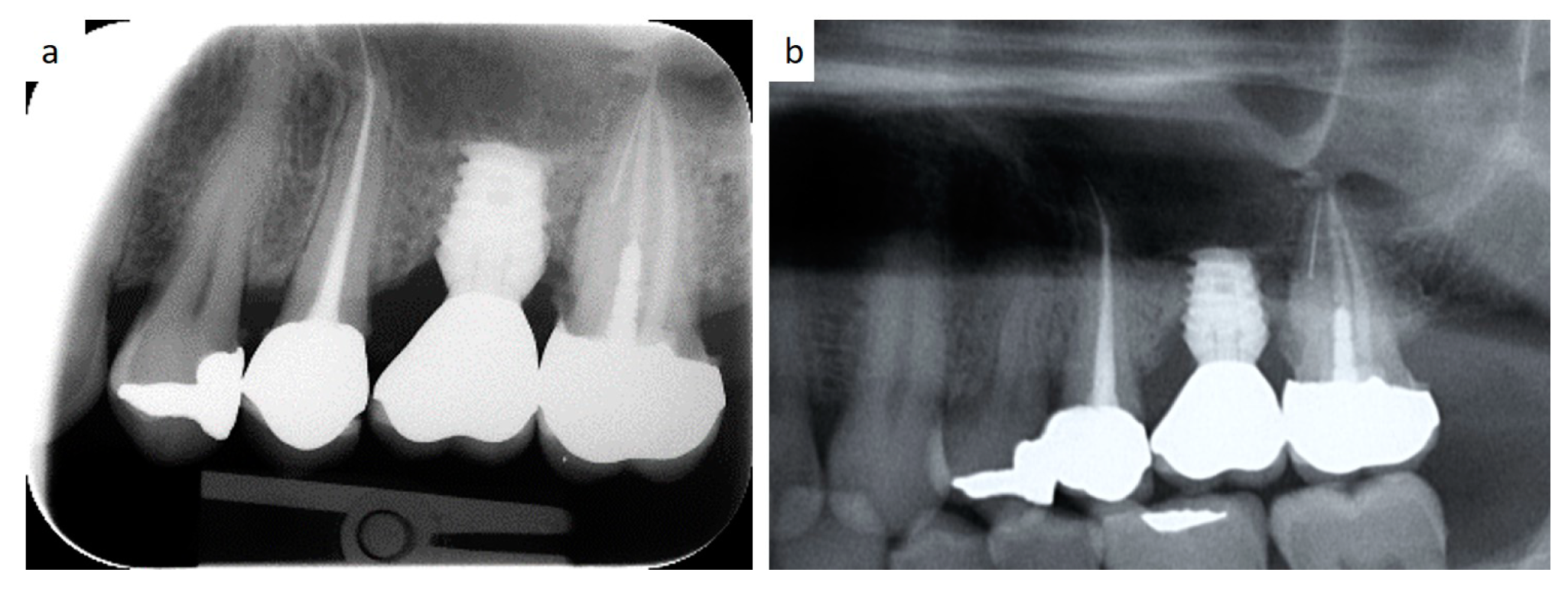
Overall, a good peri-implant bone level was observable throughout the follow-up in all cases.
Bone loss around implant was measured at the time of second surgery (three months later) with healing cup positioning (values ranging from 0 to 0.6 mm; median value: 0.1 mm) and also after two years (values ranging from 0.4 to 1.3 mm; median value: 0.7 mm). Clinical post-operative complications did not occur. (
Figure 6a–e and
Figure 7a,b) To date, no implant failure has occurred during the ten-year follow-up, as summarized in
Table 1.
4. Discussion
Molar areas of the maxilla frequently show severe vertical loss of the alveolar bone after tooth removal. Vertical dimensions of 4–6 mm of residual bone are difficult to treat when implant insertion is required [
1,
2,
5]. Various techniques have overtime been reported in the literature to allow implant insertion in such atrophic areas and especially to avoid sinus floor elevation by lateral access in addition to the related possible complications [
6,
7,
8].
Moreover, the global time of rehabilitation (from the implant insertion to the final prosthetic rehabilitation) is certainly reduced, as it decreases from about 10–12 months for conventional sinus elevation to about 3–4 months without it [
3,
4,
6].
Notably, in the last two decades there has been a general tendency to make such treatments less and less invasive thanks to both the innovation in implant design and superficial treatments of the fixtures [
1,
2,
9].
Overall, the surgical technique described in this preliminary report is a combination of previously reported techniques of under-preparation of the implant sites aimed to improve fixture primary stability and crestal approach to sinus floor elevation as an alternative to the conventional lateral window, regardless of the thickness of the sinus membrane and always without heterologous bone graft [
10,
11,
12,
13,
14,
15,
16]. More precisely, the technique we used is essentially based on a careful drilling at different depths (steps) of the residual alveolar bone in order to obtain a minimal implant site preparation, thus creating progressive steps. Subsequently, the high torque insertion of a self-tapering fixture with spiral morphology and with a smaller diameter than the preparation promotes bone displacement in the apical direction following traumatic sinus membrane elevation, thus allowing the possibility to insert a longer fixture (from 2 to 4 mm) than the measurements detected on radiographs.
In fact, it is generally accepted that spiral implants, due to their morphology (and also when of reduced length), promote bone dislocation during insertion towards the bottom of the implant site with an increase in the exploitable vertical dimension, contextually leading to both the aforementioned placement of a longer implant and to a high primary stability of the fixture [
6,
7,
8,
9,
14,
15,
16,
17,
18].
In the past, some concerns regarding complications due to the increased crown–implant ratio in prosthetic rehabilitation supported by short implants were reported. In this regard, the recent literature demonstrated that no correlation exists between occurrence of biological and technical complications and the crown–implant ratio of implant-supported reconstructions, in addition to the fact that the crown–implant ratio does not influence peri-implant crestal bone loss [
19,
20,
21,
22]. Besides, several studies reported on the efficacy of short implants compared to 10 mm or longer implants placed in crestally lifted sinuses, also showing no significant differences regarding prosthesis and implant failures, complications, and radiographic peri-implant marginal bone lose [
1,
2,
3,
9,
10,
15,
16,
17,
18,
19].
Regarding the data literature, some recent studies (systemic reviews and meta-analyses) on short implants used for the rehabilitation of the atrophic maxilla were published by Ravidà A. et al. and Yan Q. et al. in 2019, [
1,
3]. In both studies, the authors agree on the comparable survival rate of maxillary short implants in comparison to longer implants, as well on the reduced biological complications, reduction of the rehabilitation time and costs and marginal bone loss. Nevertheless, the high variability of the fixture design, length and diameter, operator-related surgical technique, timing and materials of the prosthetic rehabilitation and possible parafunctional habits, in our opinion, are important variables which may highly influence data collection as well as comparisons.
Therefore, despite the limitations of the current study—especially those related to the low number of patients/implants and the missing comparable data/cases and follow-up values of bone loss for a statistical comparison—the therapeutic protocol herein described, including implants with spiral morphology and placement of progressive steps, seem to show good outcomes in terms of mini-invasiveness, predictability and acceptability by patients for single tooth restoration of the posterior atrophic maxilla. Further studies are needing to confirm or improve data regarding the long-term effectiveness and safety of short dental implants for the prosthetic rehabilitation of the atrophic maxilla.
Author Contributions
Conceptualization, S.C. and L.L.; methodology, M.C., D.D.V. and G.F.; validation, G.F. and M.C.; investigation, D.D.V., S.C., M.D. and S.D.; data curation, L.L. and A.T.; writing—original draft preparation, S.C. and M.C.; writing—review and editing, G.F., S.C. and M.C.; supervision, G.F., S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The current study was carried out in accordance to the guidelines of the Declaration of Helsinki, and approved by our internal ethical committee (study number 4652, prot.66/C.E.-14/1/15).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are not publicly available due to privacy reasons.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yan, Q.; Wu, X.; Su, M.; Hua, F.; Shi, B. Short implants (≤6 mm) versus longer implants with sinus floor elevation in atrophic posterior maxilla: A systematic review and meta-analysis. BMJ Open 2019, 9, e029826. [Google Scholar] [CrossRef] [PubMed]
- Gürlek, Ö.; Kaval, M.E.; Buduneli, N.; Nizam, N. Extra-short implants in the prosthetic rehabilitation of the posterior maxilla. Aust. Dent. J. 2019, 64, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Ravidà, A.; Wang, I.C.; Sammartino, G.; Barootchi, S.; Tattan, M.; Troiano, G.; Laino, L.; Marenzi, G.; Covani, U.; Wang, H.L. Prosthetic Rehabilitation of the Posterior Atrophic Maxilla, Short (≤6 mm) or Long (≥10 mm) Dental Implants? A Systematic Review, Meta-analysis, and Trial Sequential Analysis: Naples Consensus Report Working Group A. Implant. Dent. 2019, 28, 590–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Jang, H. A review of complications of maxillary sinus augmentation and available treatment methods. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 220–224. [Google Scholar] [CrossRef] [Green Version]
- Schwartz-Arad, D.; Herzberg, R.; Dolev, E. The Prevalence of Surgical Complications of the Sinus Graft Procedure and Their Impact on Implant Survival. J. Periodontol. 2004, 75, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P.; Lozada, J.; Kim, J.; Rohrer, M.D. Repair of the perforated sinus membrane with a resorbable collagen membrane: A human study. Int. J. Oral Maxillofac. Implant. 2004, 19, 413–420. [Google Scholar]
- Cassetta, M.; Altieri, F.; Di Giorgio, R.; Barbato, E. Palatal orthodontic miniscrew insertion using a CAD-CAM surgical guide: Description of a technique. Int. J. Oral Maxillofac. Surg. 2018, 47, 1195–1198. [Google Scholar] [CrossRef]
- Cassetta, M.; Altieri, F.; Pandolfi, S.; Giansanti, M. The combined use of computer-guided, minimally invasive, flapless corticotomy and clear aligners as a novel approach to moderate crowding: A case report. Korean J. Orthod. 2017, 47, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Sierra-Sánchez, J.L.; García-Sala-Bonmatí, F.; Martínez-González, A.; García-Dalmau, C.; Mañes-Ferrer, J.F.; Brotons-Oliver, A. Predictability of short implants (<10 mm) as a treatment option for the rehabilitation of atrophic maxillae. A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e392–e402. [Google Scholar]
- Herrero-Climent, M.; Lemos, B.F.; Herrero-Climent, F.; Falcao, C.; Oliveira, H.; Herrera, M.; Gil, F.J.; Ríos-Carrasco, B.; Ríos-Santos, J.V. Influence of Implant Design and Under-Preparation of the Implant Site on Implant Primary Stability. An In Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 4436. [Google Scholar] [CrossRef]
- Salgar, N. Osseodensified Crestal Sinus Window Augmentation: An Alternative Procedure to the Lateral Window Technique. J. Oral Implant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Boyacıgil, D.U.; Er, N.; Karaca, Ç.; Koç, O. The effect of residual bone height and membrane thickness on sinus membrane perforation in crestal sinus grafting: A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Soardi, C.M.; Soardi, B.; Wang, H.-L. Crestal Window Sinus Lift and Its Long-Term Clinical Outcomes. Int. J. Periodontics Restor. Dent. 2020, 40, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Arab, H.R.; Moeintaghavi, A.; Shiezadeh, F.; Nezhad, M.H. Crestal Sinus Floor Elevation with Autogenous Press-Fit Dowel Bone Harvested Using Trephine Drills: A New Method. J. Long Term Eff. Med. Implant. 2018, 28, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.; Blume, M.; Korzinskas, T.; Ghanaati, S.; Sader, R.A. Short implants in the posterior maxilla to avoid sinus augmentation procedure: 5-year results from a retrospective cohort study. Int. J. Implant. Dent. 2019, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.M.; Shi, J.Y.; Gu, Y.X.; Qiao, S.C.; Mo, J.J.; Lai, H.C. Clinical Investigation and Patient Satisfaction of Short Implants Versus Longer Implants with Osteotome Sinus Floor Elevation in Atrophic Posterior Maxillae: A Pilot Randomized Trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 161–166. [Google Scholar] [CrossRef]
- Nedir, R.; Nurdin, N.; Najm, S.A.; El Hage, M.; Bischof, M. Short implants placed with or without grafting into atrophic sinuses: The 5-year results of a prospective randomized controlled study. Clin. Oral Implant. Res. 2017, 28, 877–886. [Google Scholar] [CrossRef]
- Fan, T.; Li, Y.; Deng, W.W.; Wu, T.; Zhang, W. Short Implants (5 to 8 mm) Versus Longer Implants (>8 mm) with Sinus Lifting in Atrophic Posterior Maxilla: A Meta-Analysis of RCTs. Clin. Implant. Dent. Relat. Res. 2017, 19, 207–215. [Google Scholar] [CrossRef]
- Cenkoglu, B.G.; Balcioglu, N.B.; Ozdemir, T.; Mijiritsky, E. The Effect of the Length and Distribution of Implants for Fixed Prosthetic Reconstructions in the Atrophic Posterior Maxilla: A Finite Element Analysis. Materials 2019, 12, 2556. [Google Scholar] [CrossRef] [Green Version]
- Blanes, R.J. To what extent does the crown-implant ratio affect the survival and complications of implant-supported reconstructions? A systematic review. Clin. Oral Implant. Res. 2009, 20, 67–72. [Google Scholar] [CrossRef]
- Capodiferro, S.; Favia, G.; Scivetti, M.; De Frenza, G.; Grassi, R. Clinical management and microscopic characterisation of fatique-induced failure of a dental implant. Case report. Head Face Med. 2006, 2, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, M.; Almeida, R.F.; Felino, A.C.; Malo, P.; de Araújo Nobre, M. The Influence of Crown-to-Implant Ratio on Short Implant Marginal Bone Loss. Int. J. Oral Maxillofac. Implant. 2016, 31, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}