To Develop Health Education Tools for Nasogastric Tube Home Caring Through Participatory Action Research

Abstract
:1. Introduction
- Using the participatory action research (PAR) method as the research tool, to design the graphics of procedures and considerations of nasogastric tube caring at home, explore a reasonable method of cooperation between design researchers and nurses, and develop a health education tool.
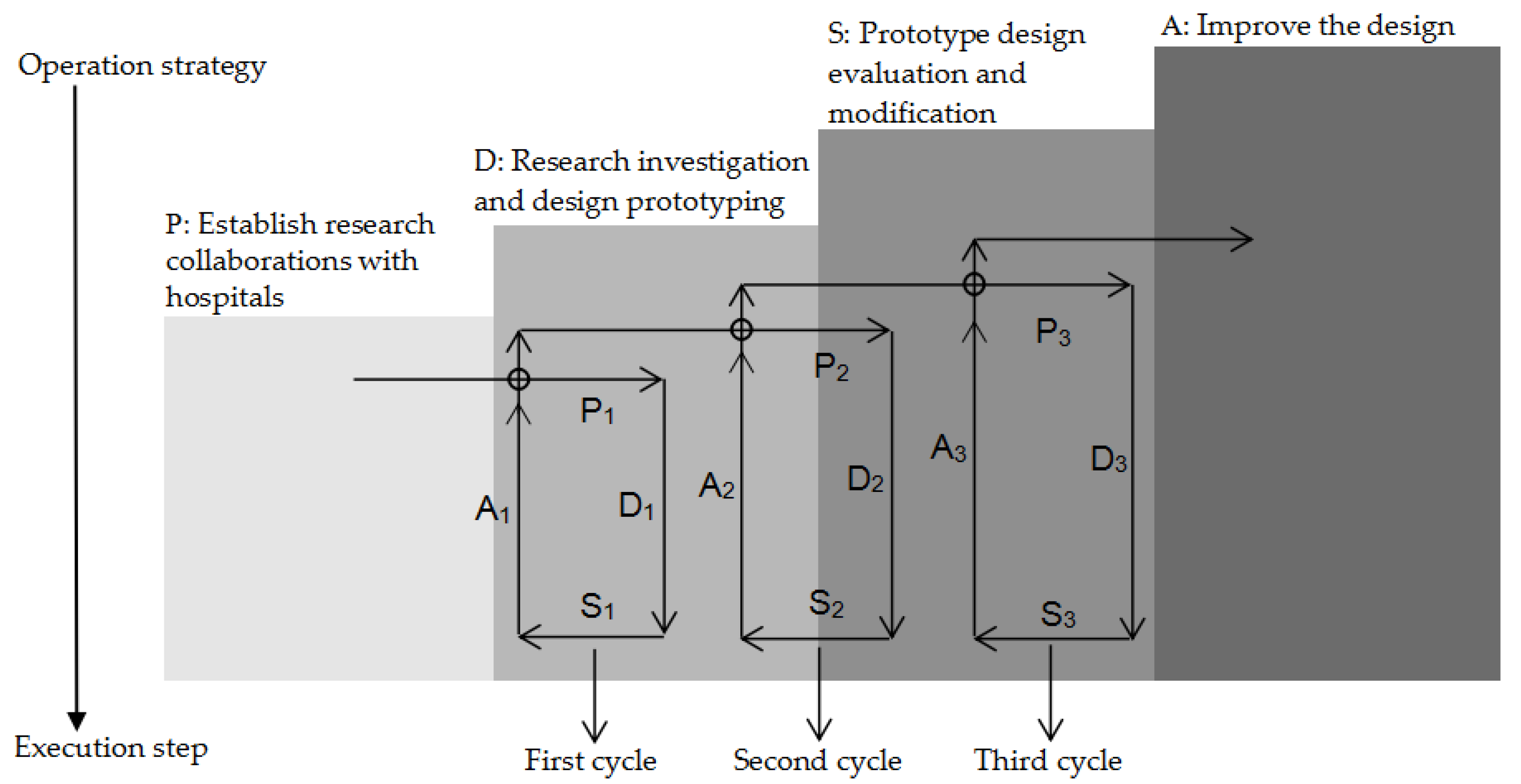
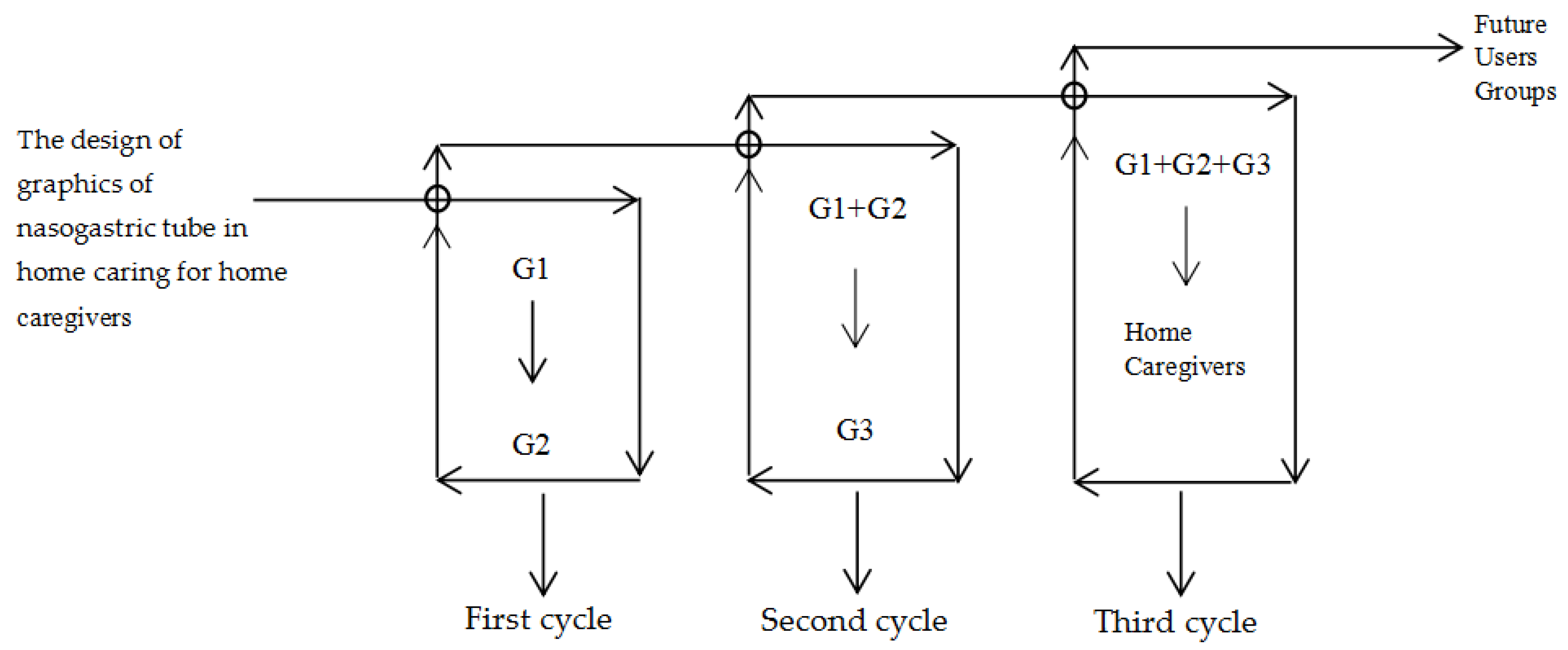
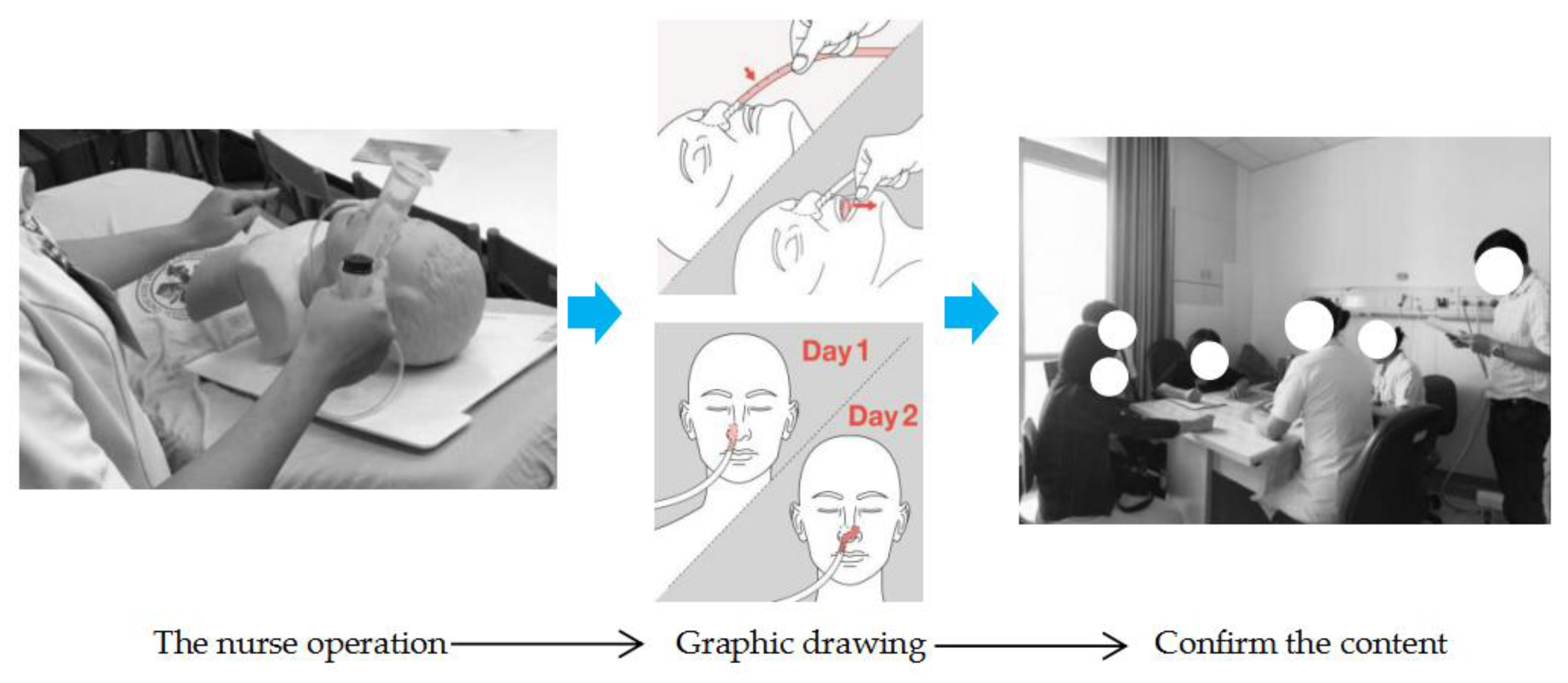
- The PAR in three cycles, in combination with the PDSA (Plan, Do, Study, Act) quality management steps and methods, continue to confirm the research objectives, repeatedly confirming and providing feedback on the contents of the graphics and texts, inspecting the quality of cooperation, and ensuring the accuracy and effectiveness of the process graphics drawing in the research process.
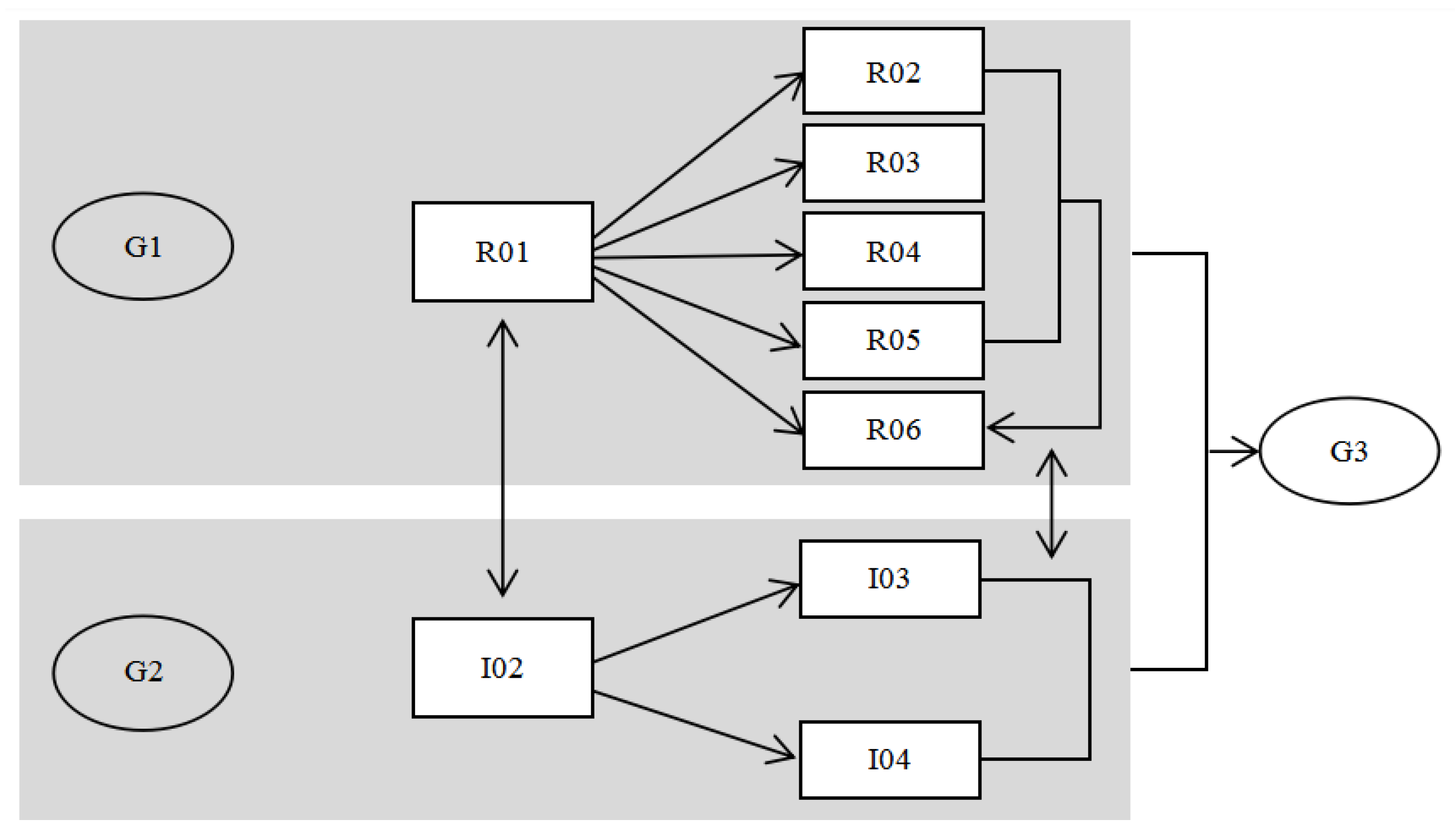
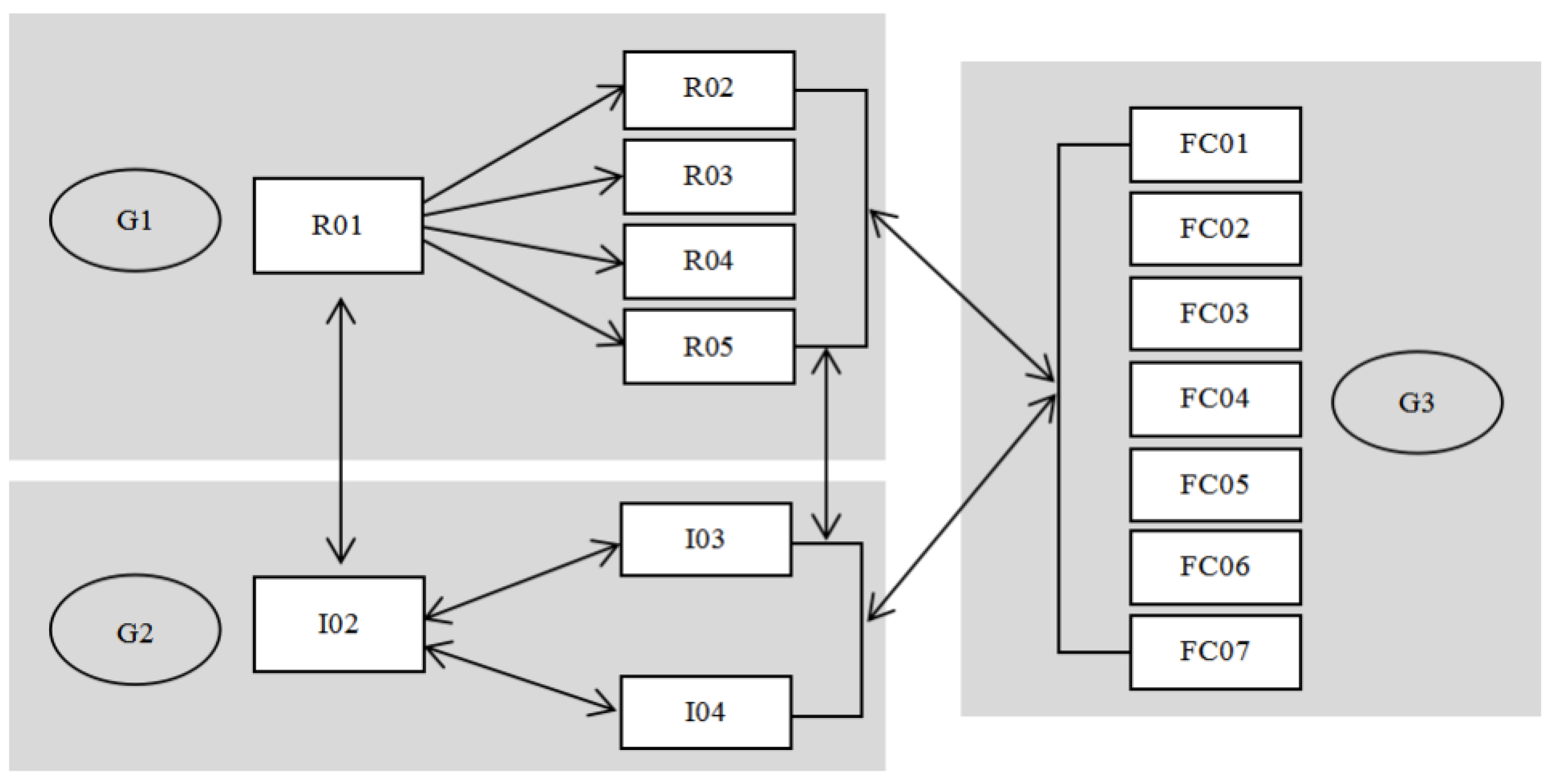
- The degree of participation, leadership, and knowledge exchange in each cycle by each of the participants are in different proportions; each participants’ position is revisited in the different cycles by the intervention of the researchers and the research tools. The relationships between nurses and home caregivers are transformed to improve the health education tools in the spirit of cooperation.
2. Literature Review
2.1. The Present Situation of Nasogastric Tube Home Caring
2.2. Participatory Action Research
2.3. PDSA
2.4. Application of Health Education Tool Graphic in the Caring Process
3. Material and Methods
3.1. Research Steps and Framework
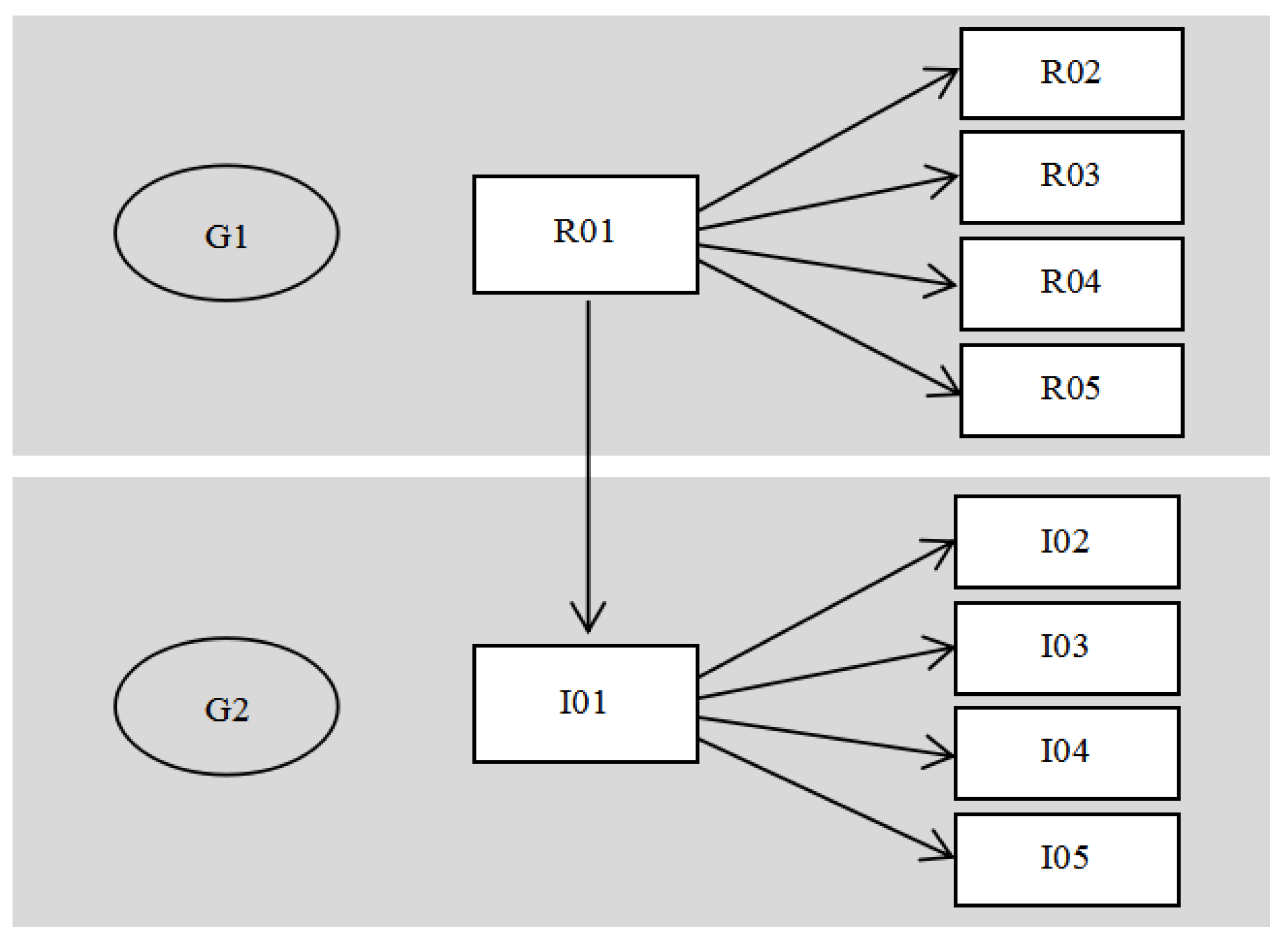
3.2. Participants
3.3. Research Tools and Data Processing
3.4. Research Limitations
4. Results
4.1. Cycle 1: Make a Plan for the Graphics Development of Home Caregivers
During the implementation of the design, user convenience should be taken as the centre. For example, previously during the use of the hospital registration system, the registered machine was purchased but it could not be further promoted due to the problems in the operation process, resulting in the loss of the hospital after the purchase of equipment. In the process of cross-discipline cooperation, effective designs should be made to help solve the needs of patients, doctors, and nurses. Otherwise, if all the designs cannot be applied, there will be no good cooperation cases or the hospital will suffer losses.
4.2. Cycle 2: Design and Revision of Nasogastric Tube Home Caring Procedure Graphics
4.3. Cycle 3: Developing Sample and Evaluation of Graphical Health Education Tools
4.4. Combined with PDSA’s Introspection on Participatory Action Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cianfrocca, C.; Caponnetto, V.; Donati, D.; Lancia, L.; Tartaglini, D.; Di Stasio, E. The effects of a multidisciplinary education course on the burden, health literacy and needs of family caregivers. Appl. Nurs. Res. 2018, 44, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Akgun-Citak, E.; Attepe-Ozden, S.; Vaskelyte, A.; van Bruchem-Visser, R.L.; Pompili, S.; Kav, S.; Mattace-Raso, F.U.S. Challenges and needs of informal caregivers in elderly care: Qualitative research in four European countries, the TRACE project. Arch. Gerontol. Geriatr. 2020, 87, 103971. [Google Scholar] [CrossRef] [PubMed]
- Richardson, T.J.; Lee, S.J.; Berg-Weger, M.; Grossberg, G.T. Caregiver Health: Health of Caregivers of Alzheimer’s and Other Dementia Patients. Curr. Psychiatry Rep. 2013, 15, 367. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Winter, L.; Dennis, M.P.; Hodgson, N.; Hauck, W.W. Targeting and Managing Behavioral Symptoms in Individuals with Dementia: A Randomized Trial of a Nonpharmacological Intervention. J. Am. Geriatr. Soc. 2010, 58, 1465–1474. [Google Scholar] [CrossRef]
- Nakarada-Kordic, I.; Patterson, N.; Wrapson, J.; Reay, S.D. A Systematic Review of Patient and Caregiver Experiences with a Tracheostomy. Patient-Patient-Cent. Outcomes Res. 2017, 11, 175–191. [Google Scholar] [CrossRef]
- Schlager, A.; Metzger, Y.; Adler, S. Use of surface acoustic waves to reduce pain and discomfort related to indwelling nasogastric tube. Endoscopy 2010, 42, 1045–1048. [Google Scholar] [CrossRef] [Green Version]
- Pai, S.-F.; Chang, K.-H.; Lim, S.-N.; Tsai, M.-C.; Chang, H.-J. Risk Factors Associated with Hospitalization in Elderly Patients Receiving Home Care Nursing. J. Long-Term Care 2017, 21, 53–75. [Google Scholar]
- Kongsuwan, W.; Borvornluck, P.; Locsin, R.C. The lived experience of family caregivers caring for patients dependent on life-sustaining technologies. Int. J. Nurs. Sci. 2018, 5, 365–369. [Google Scholar] [CrossRef]
- Hagedoorn, E.I.; Keers, J.C.; Jaarsma, T.; van der Schans, C.P.; Luttik, M.L.A.; Paans, W. The association of collaboration between family caregivers and nurses in the hospital and their preparedness for caregiving at home. Geriatr. Nurs. 2019, in press. [Google Scholar] [CrossRef]
- Almomani, B.A.; Mokhemer, E.; Al-Sawalha, N.A.; Momany, S.M. A novel approach of using educational pharmaceutical pictogram for improving inhaler techniques in patients with asthma. Respir. Med. 2018, 143, 103–108. [Google Scholar] [CrossRef]
- Roberts, N.J.; Evans, G.; Blenkhorn, P.; Partridge, M.R. Development of an electronic pictorial asthma action plan and its use in primary care. Patient Educ. Couns. 2010, 80, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Cloyes, K.G.; Hart, S.E.; Jones, A.K.; Ellington, L. Where are the family caregivers? Finding family caregiver-related content in foundational nursing documents. Journal of Professional Nursing. 2020, 36, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Ang, S.Y.; Lim, S.H.; Lim, M.L.; Ng, X.P.; Madeleine, L.; Chan, M.M.; Lopez, V. Health care professionals’ perceptions and experience of initiating different modalities for home enteral feeding. Clin. Nutr. Espen. 2019, 30, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Hsiung, H.-F. Utilization of Home Health Care among Disabled Adults. Ph.D. Thesis, National Tainan University, Taipei, Taiwan, 2010. (Unpublished). [Google Scholar]
- Yang, F.-H.; Lin, F.-Y.; Hwu, Y.-J. Knowledge, Attitude, and Behavior of Taiwan Nurses toward Nasogastric Tube Placement Verification. Cheng Ching Med. J. 2017, 13, 55–63. [Google Scholar]
- Ho, M.-M.; Hor, Y.-S.; Li, S.-C.; Hu, L.-H.; Hwang, P.-C.; Wang, M.-H.; Chen, M.-L. The Exploration of Home Care Patients’ Unplanned Ex-tubation and the Primary Caregivers’ Knowledge, and Learning Needs Related to Tubing Care. J. Long-Term Care 2008, 12, 72–90. [Google Scholar]
- Lin, Y.-C.; Tsai, Y.-C. Home Care Experience of Assisting a Patient to Weaning NG Tube and Tracheostomy Tube. St. Joseph’s Hosp. Med. Nurs. J. 2012, 6, 72–83. [Google Scholar]
- Chen, J.-C.; Jo, L.-H.; Hu, S.-C. Using Nursing Process to Deal with Common Nursing Problems in Hospital-Based Home Nursing Program: A Study. Nurs. Res. 1994, 2, 6–16. [Google Scholar]
- Klima Ronen, I. Action research as a methodology for professional development in leading an educational process. Stud. Educ. Eval. 2020, 64, 100826. [Google Scholar] [CrossRef]
- Maestrini, V.; Luzzini, D.; Shani, A.B.; Canterino, F. The action research cycle reloaded: Conducting action research across buyer-supplier relationships. J. Purch. Supply Manag. 2016, 22, 289–298. [Google Scholar] [CrossRef] [Green Version]
- Li, I.-C. Application of Action Research in Nursing. Nurs. Res. 1997, 5, 463–468. [Google Scholar]
- Eden, C.; Ackermann, F. Theory into practice, practice to theory: Action research in method development. Eur. J. Oper. Res. 2018, 271, 1145–1155. [Google Scholar] [CrossRef]
- Whyte, W.F. Participation, Action, and Research in the Classroom. Stud. Contin. Educ. 1997, 1, 1–50. [Google Scholar]
- Noguchi, A.; Inoue, T.; Yokota, I. Promoting a nursing team’s ability to notice intent to communicate in lightly sedated mechanically ventilated patients in an intensive care unit: An action research study. Intensive Crit. Care Nurs. 2019, 51, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.-F.; Wu, K.-M.; Hung, C.-C.; Wang, Y.-H.; Peng, N.-H. Resilience enhancement among student nurses during clinical practices: A participatory action research study. Nurse Educ. Today 2019, 75, 22–27. [Google Scholar] [CrossRef]
- Norbye, B. Healthcare students as innovative partners in the development of future healthcare services: An action research approach. Nurse Educ. Today 2016, 46, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Yeh, L.-L. Participatory Action Research and Its Utilization. New Taipei J. Nurs. 2010, 12, 59–68. [Google Scholar]
- Villasante, T.R.; Garcia, F.J.G. Methodologies for the Participant Construction of Knowledge. Syst. Pract. Action Res. 2001, 14, 483–493. [Google Scholar] [CrossRef]
- Schafft, K.A.; Greenwood, D.J. Promises and Dilemmas of Participation: Action Research, Search Conference Methodology, and Community Development. Community Dev. Soc. J. 2003, 34, 18–35. [Google Scholar] [CrossRef]
- Ottosson, S. Participation action research-: A key to improved knowledge of management. Technovation 2003, 23, 87–94. [Google Scholar] [CrossRef]
- Leis, J.A.; Shojania, K.G. A primer on PDSA: Executing plan–do–study–act cycles in practice, not just in name. BMJ Qual. Saf. 2017, 26, 572–577. [Google Scholar] [CrossRef]
- Byrne, J.; Xu, G.; Carr, S. Developing an intervention to prevent acute kidney injury: Using the Plan, Do, Study, Act (PDSA) service improvement approach. J. Ren. Care 2015, 41, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Cleary, B.A. Supporting empowerment with Deming′s PDSA cycle. Empower. Organ. 1995, 3, 34–39. [Google Scholar] [CrossRef]
- Donnelly, P.; Kirk, P. Use the PDSA model for effective change management. Educ. Prim. Care 2015, 26, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Cleghorn, G.D.; Headrick, L.A. The PDSA Cycle at the Core of Learning in Health Professions Education. Jt. Comm. J. Qual. Improv. 1996, 22, 206–212. [Google Scholar] [CrossRef]
- Walley, P.; Gowland, B. Completing the circle: From PD to PDSA. Int. J. Health Care Qual. Assur. 2004, 17, 349–358. [Google Scholar] [CrossRef]
- Speroff, T.; Oconnor, G.T. Study designs for PDSA quality improvement research. Qual. Manag. Health Care 2004, 13, 17–32. [Google Scholar] [CrossRef] [Green Version]
- Moen, R.; Norman, C. Evolution of the PDCA cycle. Available online: https://www.westga.edu/~dturner/PDCA.pdf (accessed on 9 August 2020).
- Reed, J.E.; Card, A.J. The problem with Plan-Do-Study-Act cycles. BMJ Qual. Saf. 2016, 25, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Houts, P.S.; Doak, C.C.; Doak, L.G.; Loscalzo, M.J. The role of pictures in improving health communication: A review of research on attention, comprehension, recall, and adherence. Patient Educ. Couns. 2006, 61, 173–190. [Google Scholar] [CrossRef]
- Lin, J.-L.; Hsieh, P.-S.; Lin, S.-H.; Song, M.-H.; Wang, S.-F. The Effectiveness of Caregiver Education for Caring Nasogastric Tube. Tzu Chi Nurs. J. 2005, 4, 49–56. [Google Scholar]
- Chen, M.-F.; Chen, Y.-H.; Wu, R.-Y.; Yu, H.-C.; Chen, S. Naso-Gastric Tube Care Assistant: “My NG is Not NG” Model. Qual. Mag. 2014, 50, 29–32. [Google Scholar]
- Chen, M.-J.; Lu, Y.-H.; Chen, C.-C.; Li, A.-C. A Project to Reduce the Incidence of Intubation Care Errors among Foreign Health Aides. J. Nurs. 2014, 61, 66–73. [Google Scholar]
- Huang, S.-W.; Lee, H.-Y.; Liu, C.-Y.; Hsieh, H.-C.; Yeh, S.-H.; Chiang, S.-C.; Hsieh, C.-C.; Hsu, C.-M. Improvement of The Accuracy Rate of Correcting Nasogastric Tube Feeding Care Among Elder Family Caregivers. Show Chwan Med. J. 2015, 14, 1–11. [Google Scholar]
- Barros, I.M.C.; Alcântara, T.S.; Mesquita, A.R.; Santos, A.C.O.; Paixão, F.P.; Lyra, D.P. The use of pictograms in the health care: A literature review. Res. Soc. Adm. Pharm. 2014, 10, 704–719. [Google Scholar] [CrossRef] [PubMed]
- Chein, I.; Cook, S.W.; Harding, J. The field of action research. Am. Psychol. 1948, 3, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.; Weyant, D.; Sterrett, S.; Ambrose, H.; Apfel, A. Perceptions of interprofessional collaborative practice and patient/family satisfaction. J. Interprofessional Educ. Pract. 2017, 8, 95–102. [Google Scholar] [CrossRef]
- Cornwall, A.; Jewkes, R. What is participatory research? Soc. Sci. Med. 1995, 41, 1667–1676. [Google Scholar] [CrossRef]
- Ateah, C.A.; Snow, W.; Wener, P.; MacDonald, L.; Metge, C.; Davis, P.; Anderson, J. Stereotyping as a barrier to collaboration: Does interprofessional education make a difference? Nurse Educ. Today 2011, 31, 208–213. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Groups | Participant Code | Gender | Age | Working Experience: Year | Participate in the Division of Labour and Work Background |
|---|---|---|---|---|---|
| Participant groups G1: design background, researcher) | Researcher-R01 | Female | 50–60 | Design (>30) | Establish cooperation and liaison with hospitals, establish research plans, interview, observation and design guidance. |
| Researcher-R02 | Female | 20–30 | Design (>7) | Participate in interviews, records, verbatim manuscripts, home care assessment, text writing and collation, data consolidation, design graphics manual. | |
| Researcher-R03 | Female | 20–30 | Design (>7) | Participate in interviews, records, verbatim manuscripts, home care assessment, text writing and collation, data consolidation, design graphics manual, graphics correction. | |
| Researcher-R04 | Male | 20–30 | Design (>3) | Participate in interviews, records, verbatim manuscripts, home care assessment, text writing and collation, data consolidation, design graphics manual, graphics correction. | |
| Researcher-R05 | Female | 30–40 | Design (>15) | Participate in interviews, records, verbatim manuscripts, home care assessment, text writing and collation, data consolidation, design graphics manual. | |
| Researcher-R06 | Male | 20–30 | Graphic design (>10) | Draw graphics, professional graphic designer. | |
| Participant groups G2: 6medical backgrounds | Doctor-I01 | Male | 50–60 | Doctor/Hospital administrator (>30) | Establishment of cooperation, hospital management, participation in interviews. |
| Nursing supervisor-I02 | Male | 30–40 | Nursing supervisor (>10) | Participate in interviews and supervise the implementation of the overall research process. | |
| Nurse-I03 | Female | 30–40 | Nurse (>10) | Nursing operation, participation in interviews, correction of operation graphics, home care assessment. | |
| Nurse-I04 | Female | 30–40 | Nurse (>10) | Nursing operation, participation in interviews, correction of operation graphics, home care assessment. | |
| Nurse-I05 | Female | 30–40 | Nurse (>10) | Participation in interviews, correction of operation graphics. | |
| Participant groups G3: home caregivers | Home caregiver-FC01 | Female | unknown | Foreign home caregiver (>0.2) | Participated in home caring study, interview and evaluation. New home caregivers, lack of home care experience. Nurses combined with graphics teaching; home caregiver needs to learn from the basics. |
| Home caregiver-FC02 | Female | unknown | Foreign home caregiver (>5) | Participated in home caring study, interview and evaluation. Experienced in home care to assist in the evaluation and revision of this study. The nurse teaches in conjunction with graphics, and the caregiver provides corrections to the graphics. | |
| Home caregiver-FC03 | Female | unknown | Foreign home caregiver (>2) | Participated in home caring study, interview and evaluation. Has home care experience but the operational details are not in place to assist this study evaluation. The nurse corrects the details of the operation by teaching them with graphics. | |
| Home caregiver-FC04 | Female | unknown | Foreign home caregiver (0) | Participated in home caring study, interview and evaluation. The patient had never used a nasogastric tube before and home caregiver lacked experience in nasogastric tube care. | |
| Home caregiver-FC05 | Female | unknown | Home caregiver (>5) | Participated in home caring study, interview and evaluation. At present, the family members of the patient are taking care of the patient by themselves. When there is a foreign caregiver, the family members teach them, and the family members learn from the nurse in this study to assist the evaluation and revision. Nurses combined with graphics teaching; patients’ families use the graphics teaching new home caregivers’ operation steps. | |
| Home caregiver-FC06 | Female | unknown | Foreign home caregiver (>5) | Participated in home caring study, interview and evaluation. Skilled in home-care operation, 2 weeks of training in home care, 3 weeks of adaptation in the home environment, there will be a new caregiver to take over the work in the future to assist this study evaluation and correction. After the nurse combined the graphics instruction, the caregiver provided corrections to the graphic. | |
| Home caregiver-FC07 | Female | 50–60 | Foreign home caregiver (>7) | Participated in home caring study, interview and evaluation. Specific learning time of nasogastric tube operation is unknown, but relevant experience has been gained in home care, which will assist in this study to evaluate and modify. After the nurse combined the graphics instruction, the nurse provided corrections to the graphics. |
| Time | Before Correction | After Correction |
|---|---|---|
| First correction |  | |
 | ||
| Second correction |  | |
| Participants | Effectiveness | Operating Performance | Process Satisfaction | Observation Time (s) | Feedback Time(s) | ||
|---|---|---|---|---|---|---|---|
| Performance (M) | Learning (M) | Nurses | Home Caregivers | ||||
| FC01 | Yes | 4 | 5 | 8 | 8 | 15 | 10 |
| FC02 | Not given | 4 | 5 | 8 | 8 | 20 | 15 |
| FC03 | Yes | 4 | 5 | 8 | 8 | 10 | 5 |
| FC04 | Yes | 3.56 | 4 | 8 | 8 | 30 | 15 |
| FC05 | Yes | 4.67 | 4 | 6 | 7 | 5 | 5 |
| FC06 | Yes | 4 | 5 | 8 | 8 | 10 | 5 |
| FC07 | Yes | 4.11 | 4.2 | 8 | 8 | 10 | 10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, F.-S.; Shi, H.-C. To Develop Health Education Tools for Nasogastric Tube Home Caring Through Participatory Action Research. Healthcare 2020, 8, 261. https://doi.org/10.3390/healthcare8030261
Lin F-S, Shi H-C. To Develop Health Education Tools for Nasogastric Tube Home Caring Through Participatory Action Research. Healthcare. 2020; 8(3):261. https://doi.org/10.3390/healthcare8030261
Chicago/Turabian StyleLin, Fang-Suey, and Hong-Chun Shi. 2020. "To Develop Health Education Tools for Nasogastric Tube Home Caring Through Participatory Action Research" Healthcare 8, no. 3: 261. https://doi.org/10.3390/healthcare8030261