Mindfulness in Family Caregivers of Persons with Dementia: Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
1.1. Mindfulness-Based Intervention and Family Caregivers of Persons with Dementia
1.2. The Present Study
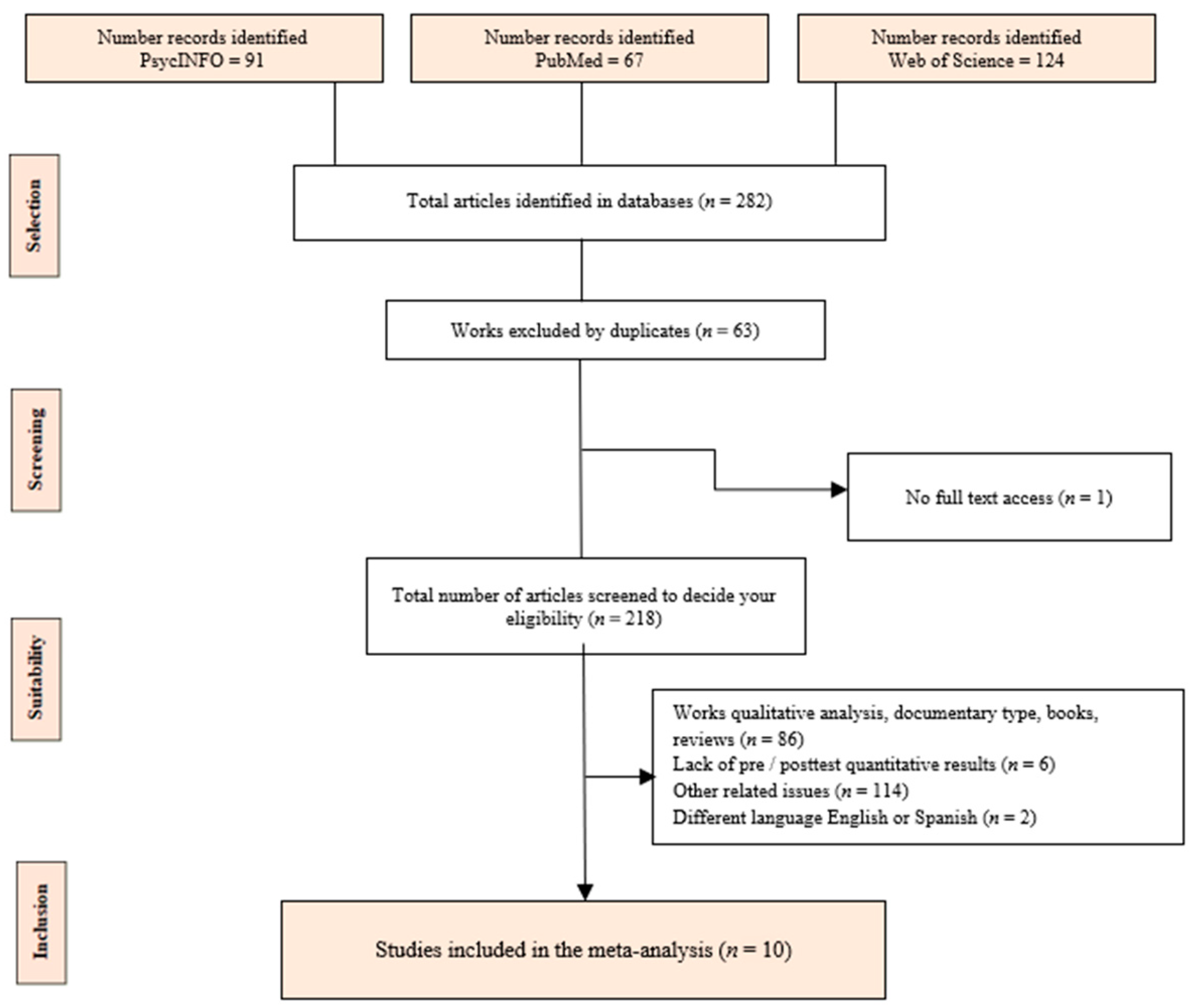
2. Materials and Methods
2.1. Procedure
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias
2.5. Data Analysis: Meta-Analysis
3. Results
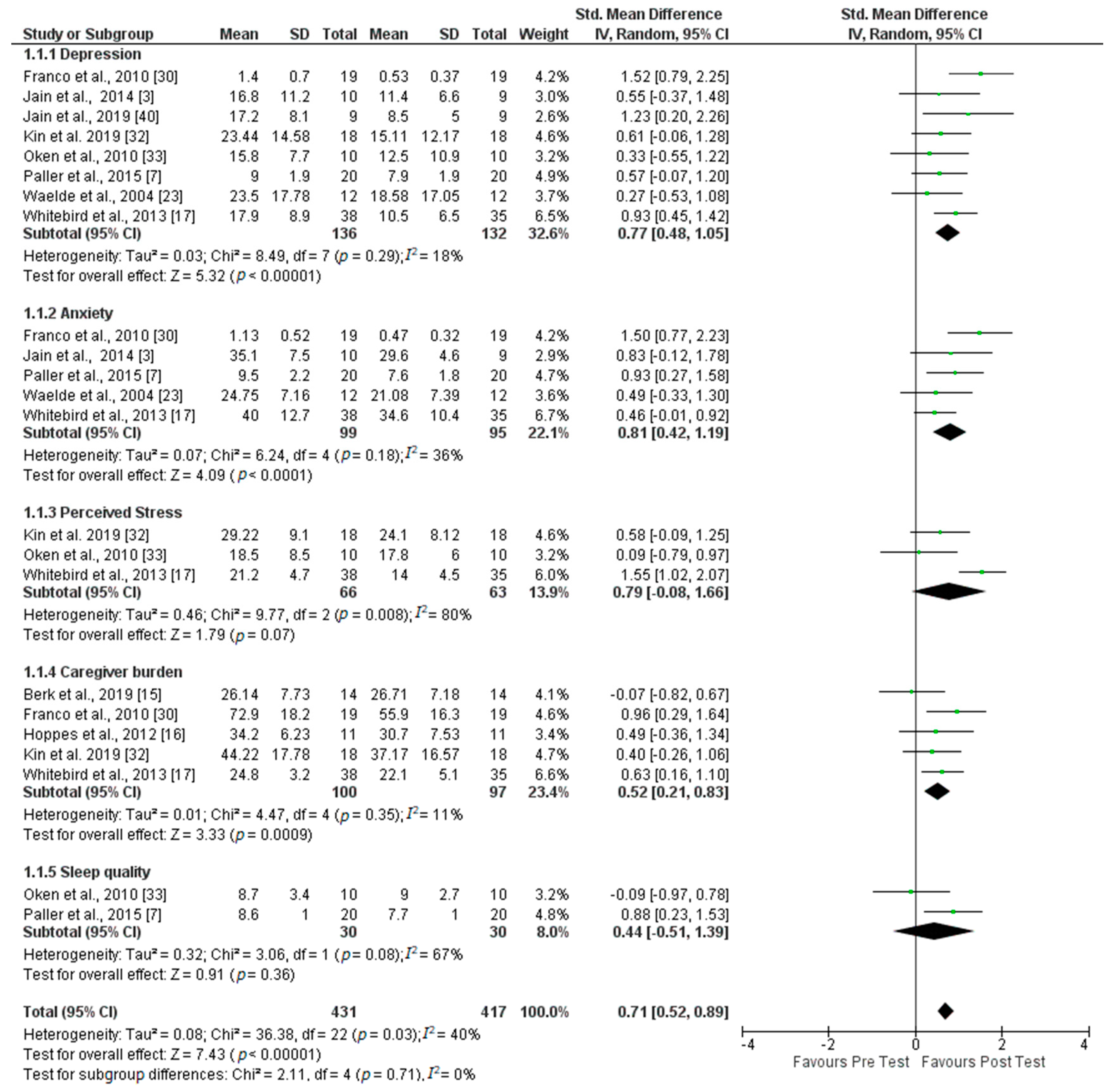
3.1. Summary of Results: Meta-Analysis
3.2. Result Variables for Depression, Anxiety, Perceived Stress, Caregiver Burden and Sleep Quality
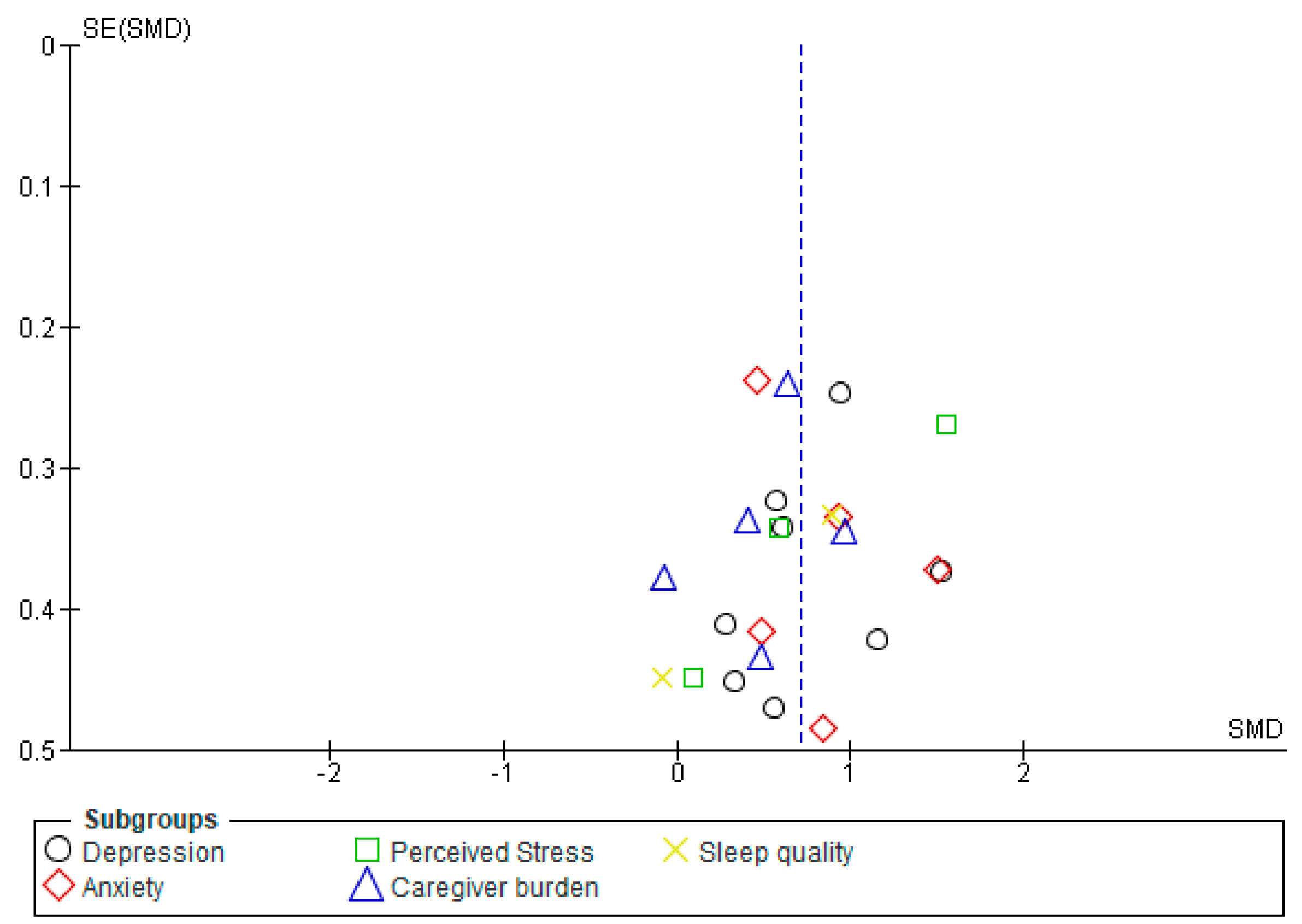
3.3. Risk of Bias in Variables
4. Discussion
4.1. Limitations
4.2. Recommendations for Future Research
4.3. Practical Applications of Results
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amutio, A.; Franco, C.; Sánchez, L.C.; Pérez-Fuentes, M.C.; Gázquez, J.J.; Van Gordon, W.; Molero, M.M. Effects of Mindfulness Training on Sleep Problems in Patients with Fibromyalgia. Front. Psychol. 2018, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Macías, J.J.; Valero-Aguayo, L.; Bond, F.W.; Blanca, M.J. The efficacy of functional-analytic psychotherapy and Acceptance and commitment therapy (FACT) for public employees. Psicothema 2019, 31, 24–29. [Google Scholar] [CrossRef]
- Jain, F.A.; Nazarian, N.; Lavretsky, H. Feasibility of Central Mediation and Imagery Therapy for dementia caregivers. Int. J. Geriatr. Psychiatry 2014, 29, 870–876. [Google Scholar] [CrossRef] [Green Version]
- Franco, C.; Amutio, A.; Mañas, I.; Gázquez, J.J.; Pérez-Fuentes, M.C. Reducing anxiety, geriatric depression and worry in a sample of older adults through a mindfulness training program. Ter. Psicol. 2017, 35, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Martín-Asuero, A.; de la Banda, G.G. Las ventajas de estar presente: Desarrollando una conciencia plena para reducir el malestar psicológico (The Advantages of Being Present: Developing Mindfulness to Reduce Psychological Discomfort). Int. J. Clin. Health Psychol. 2007, 7, 369–384. [Google Scholar]
- Pagnini, F.; Cavalera, C.; Rovaris, M.; Mendozzi, L.; Molinari, E.; Phillips, D.; Langer, E. Longitudinal associations between mindfulness and well-being in pleople with multiple scleroris. Int. J. Clin. Health Psychol. 2019, 19, 22–30. [Google Scholar] [CrossRef]
- Paller, K.A.; Creery, J.D.; Florczak, S.M.; Weintraub, S.; Mesulam, M.M.; Reber, P.J.; Kiragu, J.; Rooks, J.; Safron, A.; Morhardt, D.; et al. Benefits of Mindfulness Training for Patients with Progressive Cognitive Decline and their Caregivers. Am. J. Alzheimers Dis. Other Dement. 2015, 30, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Strawn, J.R.; Cotton, S.; Luberto, C.M.; Patino, L.R.; Stahl, L.A.; Weber, W.A.; Eliassen, J.C.; Sears, R.; DelBello, M.P. Neural function before and after mindfulness based cognitive therapy in anxious adolescents at risk for developing bipolar disorder. J. Child Adolesc. Psychopharmacol. 2016, 26, 1–8. [Google Scholar] [CrossRef]
- Huang, F.Y.; Hsu, A.L.; Hsu, L.M.; Tsai, J.S.; Huang, C.M.; Chao, Y.P.; Hwang, T.J.; Wu, C.W. Mindfulness improves emotion regulation and executive control on bereaved individuals: An fMRI study. Front. Hum. Neurosci. 2019, 12, 541. [Google Scholar] [CrossRef] [Green Version]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Curriculum outline. In Mindfulness-Based Stress Reduction Professional Training Resource Manual; Center for Mindfulness in Medicine, Health Care, and Society: Worceste, MA, USA, 1993. [Google Scholar]
- Linehan, M.M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; The Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change; The Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Safran, J.D.; Muran, J.C. The Therapeutic Alliance. A Guide to Relational Treatment; Desclée de Brouwer: Bilbao, Spain, 2005. [Google Scholar]
- Berk, L.; Warmenhoven, F.; Stiekema, A.P.M.; van Oorsuow, K.; van Os, J.; de Vugt, M.; van Boxtel, M. Mindfulness-Based Intervention for People with Dementia and Their Partners: Results of a Mixed-Methods Study. Front. Aging Neurosci. 2019, 11, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoppes, S.; Bryce, H.; Hellman, C.; Finlay, E. The Effects of Brief Mindfulness Training on Caregivers’ Well-Being. Act. Adapt. Aging 2012, 36, 147–166. [Google Scholar] [CrossRef]
- Whitebird, R.R.; Kreitzer, M.; Crain, A.L.; Lewis, B.A.; Hanson, L.R.; Enstad, C.J. Mindfulness-Based Stress Reduction for Family Caregivers. A Randomized Controlled Trial. Gerontologist 2013, 53, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Larrubia, A. Mindfulness Based Intervention (MBI). Desarrollo profesional y salud laboral (Professional development and occupational health). J. Res. Educ. Health Sci. 2019, 4, 4–27. [Google Scholar]
- Pardo, C.; González, R. El impacto de un programa de meditación Mindfulness sobre las estrategias de afrontamiento en estudiantes universitarios (The impact of a Mindfulness meditation program on coping strategies in university students). Eur. J. Health Res. 2019, 5, 51–61. [Google Scholar] [CrossRef]
- Virgili, M. Mindfulness-based interventions reduce psychological distress in working adults: A meta-analysis of intervention studies. Mindfulness 2015, 6, 326–337. [Google Scholar] [CrossRef]
- Vizoso-Gómez, C.; Arias-Gundín, O. Resiliencia, optimismo y burnout académico en estudiantes universitarios (Resilience, optimism and academic burnout in university students). Eur. J. Educ. Psychol. 2018, 11, 47–59. [Google Scholar] [CrossRef]
- Martos, A.; Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M.; Barragán, A.B. Burnout y engagement en estudiantes de Ciencias de la Salud (Burnout and engagement in Health Sciences students). Eur. J. Investig. Health Psychol. Educ. 2018, 8, 23–36. [Google Scholar] [CrossRef] [Green Version]
- Waelde, L.C.; Gallagher-Thompson, D. A Pilot Study of a Yoga and Mediation Intervention for Dementia Caregiver Stress. J. Clin. Psychol. 2004, 60, 677–687. [Google Scholar] [CrossRef]
- Demencia. Ginebra: World Health Organization. Available online: https://www.who.int/es/news-room/fact-sheets/detail/dementia (accessed on 24 June 2020).
- Sandoval, J.J.; Maldonado, C.; Helena, R. Tasas corregidas de mortalidad atribuible a la demencia por la enfermedad de Alzheimer, Brasil, 2009–2013 (Corrected mortality rates attributable to dementia from Alzheimer’s disease, Brazil, 2009–2013). Cad Saude Publica 2019, 35, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Navarro, M.; Jiménez, L.; García, M.C.; Perosanz, M.; Blanco, E. Los enfermos de Alzheimer y sus cuidadores: Intervenciones de enfermería (Alzheimer’s patients and their caregivers: Nursing interventions). Gerokomos 2018, 29, 79–82. [Google Scholar]
- Peinado, A.I.; de los Fayos, G.E.J. Burnout en cuidadores principales de pacientes con Alzheimer: El síndrome del asistente desasistido (Burnout in primary caregivers of Alzheimer’s patients: The unattended assistant syndrome). An. Psicol. (Spain) 1998, 14, 3–93. [Google Scholar]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Ruiz, M.D.; Molero, M.M. Inventory of Overburden in Alzheimer’s Patient Family Caregivers with no Specialized Training. Int. J. Clin. Health Psychol. 2017, 17, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera, M.C.; Herrera, A.; Expósito, F. To Confront Versus not to Confront: Women’s Perception of Sexual Harassment. Eur. J. Psychol. Appl. Legal Context 2018, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Franco, C.; Sola, M.M.; Justo, E. Reducción del malestar psicológico y de la sobrecarga en familiares cuidadores de enfermo de Alzheimer mediante la aplicación de un programa de entrenamiento en Mindfulness (conciencia plena) (Reduction of psychological distress and overload in family caregivers of Alzheimer’s patients through the application of a training program in Mindfulness (full consciousness)). Rev. Esp. Geriatr. Gerontol. 2010, 45, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Danucalov, M.A.D.; Kozasa, E.H.; Afonso, R.F.; Galduroz, J.C.F.; Leite, J.R. Yoga and compassion meditation program improve quality of life and self-compassion in family caregivers of Alzheimer’s disease patients: A randomized controlled trial. Geriatr. Gerontol. Int. 2017, 17, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Kin, P.P.; Wa, J.Y.; Tong, W. Effects of modified mindfulness-based cognitive therapy for Family caregivers of pleople with dementia: A pilot radomized controlled trial. Int. J. Nurs. Stud. 2019, 98, 107–117. [Google Scholar] [CrossRef]
- Oken, B.S.; Fonareva, I.; Haas, M.; Wahbeh, H. Pilot Controlled Trial of Mindfulness Mediation and Education for Dementia Caregivers. J. Altern. Complementary Med. 2010, 16, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Pampliega, A.; Ugarte, I.; Merino, L.; Herrero-Fernández, D. Conciliación familia-trabajo y sintomatología externalizante de los hijos e hijas: Papel mediador del clima familiar (Family-work conciliation and externalizing symptoms of sons and daughters: Mediating role of the family climate). Rev. Iberoam Psicol. Salud. 2019, 10, 27–36. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Meca, J.; Ato, M. Meta-análisis: Una alternativa metodológica a las revisiones tradicionales de la investigación (Meta-analysis:A methodological alternative to traditional research reviews). In Tratado de Psicología General I: Historia, Teoría y Método; Arnau, J., Carpintero, H., Eds.; Madrid Alhambra: Madrid, Spain, 1989; pp. 617–669. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Jain, F.A.; Connolly, C.G.; Moore, L.C.; Leuchter, A.F.; Abrams, M.; Ben-Yelles, R.W.; Chan, S.E.; Ramirez, L.A.; Lavretsky, H.; Lacobini, M. Grief, Mindfulness and Neural Predictors of Improvement in Family Dementia Caregivers. Front. Hum. Neurosci. 2019, 13, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Authors, (Publication Year) [Reference] | Study Design | Place | Variables Evaluated | N | Duration | Most Characteristic Results |
|---|---|---|---|---|---|---|
| Berk, Warmenhoven, Stiekema, van Oorsuow, van Os, de Vugt, and van Boxtel, 2019 [15] | Uncontrolled trial, 1 group | Mexico | Psychological distress, mindfulness, self-compassion, mental health, worry, caregiver burden and self-esteem | 14 | 8 weeks (2.5 h/week) | Caregivers show less psychological distress and increased attention to quality of life |
| Jain, Nazarian and Lavretsky, 2014 [3] | Uncontrolled trial, 1 group | Germany | Depression, anxiety, quality of life, enjoyment and satisfaction, insomnia and mindfulness | 10 | 8 weeks (3 weekly sessions of 1 h–15 min sessions) | Pain, depression and mindfulness were interrelated, but their neural mechanisms did not overlap, at least partly |
| Whitebird, Kreitzer, Crain, Lewis, Hanson, and Enstad, 2013 [17] | Uncontrolled trial, 2 groups | New York | Mindfulness, stress, depression, anxiety and caregiver burden | 38 | 2 months (8 weekly sessions of 2.5 h) | Caregivers showed lower stress and depression |
| Hoppes, Bryce, Helman and Finlay, 2012 [16] | Uncontrolled trial, 2 groups | UK | Burden, hope, optimism and mindfulness | 11 | 4 weeks (1 h/week) | Caregivers showed greater acceptance, presence, peace and hope, and decreased caregiver burden |
| Oken, Fonareva, Haas, and Wahbeh, 2010 [33] | Uncontrolled trial, 3 groups | Portland | Mindfulness, cognitive means, physiological means, expectations and sampling based on experience | 10 | 7 weeks (90 min/week) | Caregivers showed higher self-efficacy and cognitive means |
| Waelde and Gallagher-Thompson, 2004 [23] | Uncontrolled trial, 1 group | San Francisco | Depression, anxiety, self-efficacy and mindfulness, caregiver burden and subjective improvement of perceived self-efficacy | 12 | 2 years (30 min/week) | Caregivers revealed significant reductions in depression and anxiety, and improvement in perceived self-efficacy |
| Franco, Sola, and Justo, 2010 [30] | Controlled trial, 2 groups | Spain | Caregiver load, self-efficacy, somatization, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation distress | 19 | 10 weeks (10 sessions of 2 h) | Caregivers showed less psychological distress in general, and less overburden |
| Jain, Connolly, Moore, Leuchter, Abrams, Ben-Yelles, Chan, Ramirez, Lavretsky and Lacobini, 2019 [40] | Uncontrolled trial, 1 group | Los Angeles | Mourning, depression and mindfulness | 9 | 4 weeks (2 h/week) | Caregivers showed lower levels of depression, sorrow for loss, and increased mindfulness |
| Kin, Wa, and Tong (2019) [32] | One-group randomized controlled trial | China | Stress, caregiver burden, depression, anxiety, resilience, quality of life and mindfulness | 18 | 10 weeks (7 sessions of 2 h) | Caregivers showed reduction in stress levels and improved psychological wellbeing |
| Paller, Creery, Florczak, Weintraub, Mesulam, Reber, Kiragu, Rooks, Safron, Morhardt, and O’Hara, 2015 [7] | Uncontrolled trial, 4 groups | Evanston | Quality of life, depression, anxiety, subjective sleep quality, visual attention and socioemotional and physical health | 20 | 8 weeks (8 weekly sessions of 1 h–30 min sessions) | Caregivers showed reduction in anxiety levels, lighter symptoms of distress and better sleep quality and quality of life |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molero Jurado, M.d.M.; Pérez-Fuentes, M.d.C.; Barragán Martín, A.B.; Soriano Sánchez, J.G.; Oropesa Ruiz, N.F.; Sisto, M.; Gázquez Linares, J.J. Mindfulness in Family Caregivers of Persons with Dementia: Systematic Review and Meta-Analysis. Healthcare 2020, 8, 193. https://doi.org/10.3390/healthcare8030193
Molero Jurado MdM, Pérez-Fuentes MdC, Barragán Martín AB, Soriano Sánchez JG, Oropesa Ruiz NF, Sisto M, Gázquez Linares JJ. Mindfulness in Family Caregivers of Persons with Dementia: Systematic Review and Meta-Analysis. Healthcare. 2020; 8(3):193. https://doi.org/10.3390/healthcare8030193
Chicago/Turabian StyleMolero Jurado, María del Mar, María del Carmen Pérez-Fuentes, Ana Belén Barragán Martín, José Gabriel Soriano Sánchez, Nieves Fátima Oropesa Ruiz, Maria Sisto, and José Jesús Gázquez Linares. 2020. "Mindfulness in Family Caregivers of Persons with Dementia: Systematic Review and Meta-Analysis" Healthcare 8, no. 3: 193. https://doi.org/10.3390/healthcare8030193