
Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
- Papers published in peer-reviewed journal
- Papers written in the English language
- Papers published from 2004 to 2015 (focus on more recent knowledge)
- Human epidemiological studies
- Studies used a quantitative methodology reporting the leadership style and healthcare quality measures
3. Results
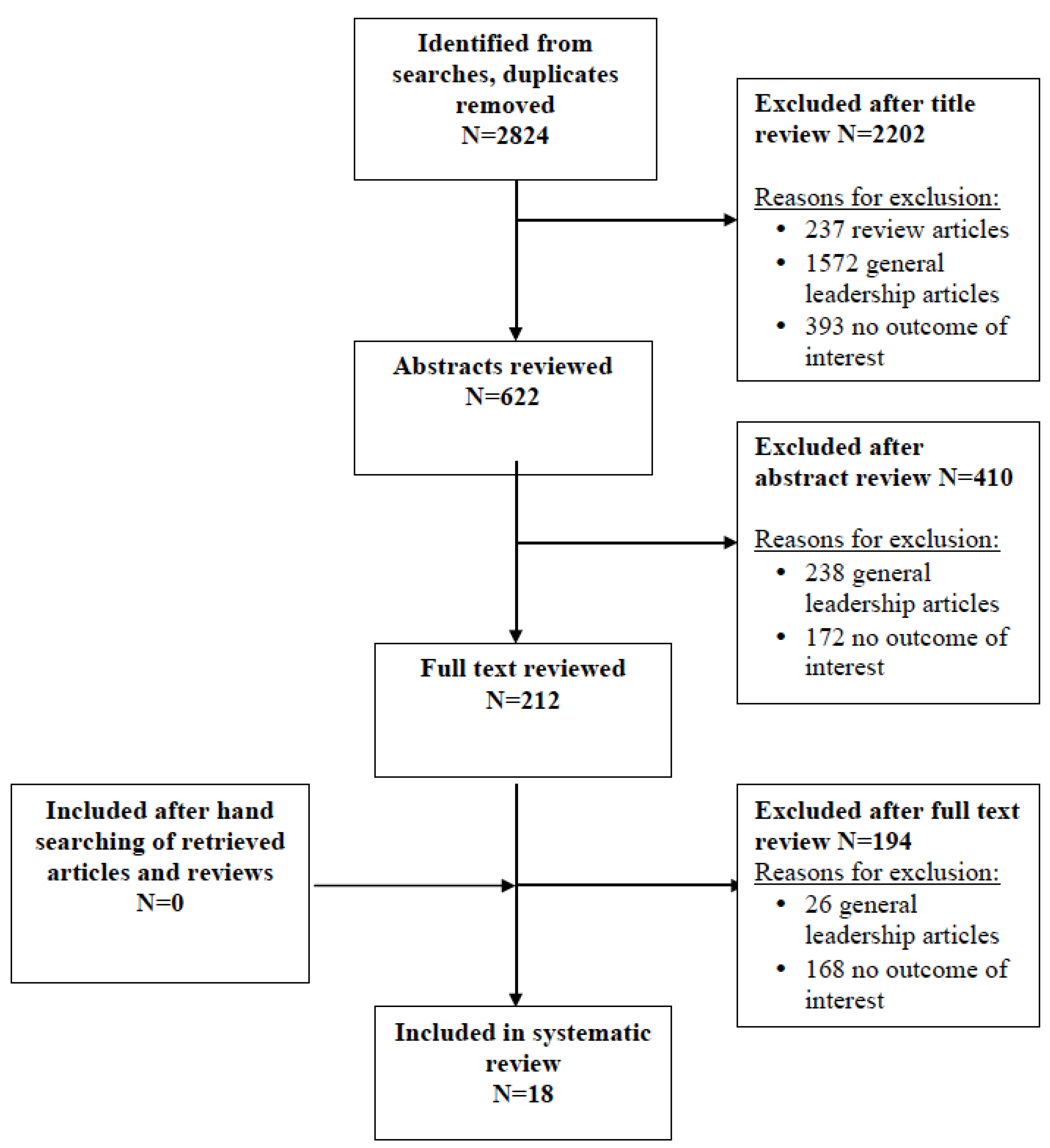
3.1. Bibliographic Search
3.2. Overview of the Included Studies
3.3. Leadership Style and Patients Outcomes
3.4. Organizational Culture and Quality of Care
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kouzes, J.M.; Posner, B.Z. The Leadership Challenge, 3rd ed.; Jossey-Bass: San Francisco, CA, USA, 2002. [Google Scholar]
- Al-Sawai, A. Leadership of Healthcare Professionals: Where Do We stand? Oman Med. J. 2013, 28, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Burns, J.M. Leadership; Harper & Row: New York, NY, USA, 1978. [Google Scholar]
- Frandsen, B. Nursing Leadership Management & Leadership Styles; AANAC, American Association of Nurse Assessment Coordination: Denver, CO, USA, 2014. [Google Scholar]
- Yukl, G.A. Leadership in Organizations; Pearson Education: Upper Saddle River, NJ, USA, 2010. [Google Scholar]
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academy Press: Washington, D.C., USA, 2001. [Google Scholar]
- Lang, T.A.; Hodge, M.; Olson, V.; Romano, P.S.; Kravitz, R.L. Nurse-patient ratios: A systematic review on the effects of nurse staffing on patient, nurse employee and hospital. J. Nurs. Adm. 2004, 34, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.A.; Cummings, G.G. The relationship between nursing leadership and patient outcomes: A systematic review. J. Nurs. Manag. 2007, 15, 508–521. [Google Scholar] [CrossRef] [PubMed]
- Havig, A.; Skogstad, A.; Kjekshus, L.A.; Romoren, L.E. Leadership, staffing and quality of care in nursing homes. BMC Health Serv. Res. 2011, 11, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, A.E.K. Transforming nurses’ work environments to improve patient safety: The Institute of Medicine recommendations. Policy, Politics Nurs. Pract. 2004, 5, 250–258. [Google Scholar] [CrossRef]
- Houser, J. A model for evaluating the context of nursing care delivery. J. Nurs. Adm. 2003, 33, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Al-Mailam, F. Transactional Versus Transformational Style of Leadership—Employee Perception of Leadership Efficacy in Public and Private Hospitals in Kuwait. Qual. Manag. Healthc. 2004, 13, 278–284. [Google Scholar] [CrossRef]
- Armstrong, K.; Laschinger, H. Structural Empowerment, Magnet Hospital Characteristics, and Patient Safety Culture Making the Link. J. Nurs. Care Qual. 2006, 21, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Keroack, M.; Youngberg, B.; Cerese, J.; Krsek, C.; Prellwitz, L.; Trevelyan, E. Organizational factors associated with high performance in quality and safety in academic medical centers. Acad. Med. 2007, 82, 1178–1186. [Google Scholar] [CrossRef] [PubMed]
- Kvist, T.; Vehvilainen-Julkunen, K.; Jokela, V. Do organizational factors explain the quality of care? J. Nurs. Care Qual. 2007, 22, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Vogus, T.; Sutcliffe, K. The impact of safety organizing, trusted leadership, and care pathways on reported medication errors in hospital nursing units. Med. Care 2007, 45, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Casida, J.; Pinto-Zipp, G. Leadership-organizational culture relationship in nursing units of acute care hospitals. Nurs. Econ. 2008, 26, 7–15. [Google Scholar] [PubMed]
- Raup, G. The impact of ED nurse manager leadership style on staff nurse turnover and patient satisfaction in academic health center hospitals. J. Emerg. Nurs. 2008, 34, 403–409. [Google Scholar] [CrossRef] [PubMed]
- McCutcheon, A.; Doran, D.; Evans, M.; McGillis-Hall, L.; Pringle, D. Effects of leadership and span of control on nurses job satisfaction and patient satisfaction. Can. J. Nurs. Leadersh. 2009, 22, 48–67. [Google Scholar] [CrossRef]
- Singer, S.; Falwell, A.; Gaba, D.; Meterko, M.; Rosen, A.; Hartmann, C.; Baker, L. Identifying organizational cultures that promote patient safety. Healthc. Manag. Rev. 2009, 34, 300–311. [Google Scholar] [CrossRef] [PubMed]
- Alahmadi, H.A. Assessment of patient safety culture in Saudi Arabian hospitals. Qual. Saf. Healthc. 2010, 19, e17. [Google Scholar] [CrossRef] [PubMed]
- Armellino, D.; Quinn Griffin, M.T.; Fitzpatrick, J.J. Structural empowerment and patient safety culture among registered nurses working in adult critical care units. J. Nurs. Manag. 2010, 18, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Cummings, G.; Midodzi, W.; Wong, C.; Estabrooks, C. The contribution of hospital nursing leadership styles to 30-day patient mortality. Nurs. Res. 2010, 59, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, L.; Chuang, Y.; Berta, W.; Norton, P.; Ng, P.; Tregunno, D.; Richardson, J. The relationship between organizational leadership for safety and learning from patient safety events. Health Serv. Res. 2010, 45, 607–632. [Google Scholar] [CrossRef] [PubMed]
- Purdy, N.; Spence-Laschinger, H.; Finegan, J.; Kerr, M.; Olivera, F. Effects of work environments on nurse and patient outcomes. J. Nurs. Manag. 2010, 18, 901–913. [Google Scholar] [CrossRef] [PubMed]
- Squires, M.; Tourangeau, A.; Spence-Laschinger, H.; Doran, D. The link between leadership and safety outcomes in hospitals. J. Nurs. Manag. 2010, 18, 914–925. [Google Scholar] [CrossRef] [PubMed]
- Castle, N.; Decker, F. Top management leadership style and quality of care in nursing homes. Gerontologist 2011, 51, 630–642. [Google Scholar] [CrossRef] [PubMed]
- Kvist, T.; Mantynen, R.; Turunen, H.; Partanen, P.; Miettinen, M.; Wolf, G.; Vehvilainen-Julkunen, K. How magnetic are Finnish hospitals measured by transformational leadership and empirical quality outcomes? J. Nurs. Manag. 2013, 21, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Wade, G.; Osgood, B.; Avino, K.; Bucher, G.; Bucher, L.; Foraker, T.; French, D.; Sirkowski, C. Influence of organizational characteristics and caring attributes of managers on nurses’ job enjoyment. J. Nurs. Manag. 2008, 64, 344–353. [Google Scholar] [CrossRef] [PubMed]
- O’Brien-Pallas, L.; Murphy, G.; Shamian, J.; Li, X.; Hayes, L. Impact and determinants of nurse turnover: A pan-Canadian study. J. Nurs. Manag. 2010, 18, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Kanste, O.; Kyngas, H.; Nikkila, J. The relationship between multidimensional leadership and burnout among nursing staff. J. Nurs. Manag. 2007, 15, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Schreuder, J.; Roelen, C.; van Zweeden, N.; Jongsma, D.; van der Klink, J.; Groothoff, J. Leadership styles of nurse managers and registered sickness absence among their nursing staff. Healthc. Manag. Rev. 2011, 36, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; McNicholas, C.; Nicolay, C.; Darzi, A.; Bell, D.; Reed, J.E. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual. Saf. 2014, 23, 290–298. [Google Scholar] [CrossRef] [PubMed]
- Vance, C.; Larson, E. Leadership research in business and health care. J. Nurs. Scholarsh. 2002, 34, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Heath, J.; Johanson, W.; Blake, N. Healthy work environments: A validation of the literature. J. Nurs. Adm. 2004, 34, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.A. Connecting nursing leadership and patient outcomes: State of the science. J. Nurs. Manag. 2015, 23, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Moneke, N.; Umeh, O. Factors influencing critical care nurses’ perception of their overall job satisfaction: An empirical study. J. Nurs. Adm. 2013, 43, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J.L.; Martin, D.K.; Singer, P.A. Setting priorities in health care organizations: Criteria, processes, and parameters of success. BMC Health Serv. Res. 2004, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Singer, P. A strategy to improve priority setting in health care institution. Healthc. Anal. 2003, 11, 59–68. [Google Scholar] [CrossRef] [PubMed]
- McFadden, K.L.; Stock, G.N.; Gowen, C.R., III. Leadership, safety climate, and continuous quality improvement: Impact on process quality and patient safety. Healthc. Manag. Rev. 2015, 40, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Baker, G.R.; Norton, P.G.; Flintoft, V.; Blais, R.; Brown, A.; Cox, J.; Etchells, E.; Ghali, W.A.; Hébert, P.; Majumdar, S.R.; et al. The Canadian Adverse Events Study: The incidence of adverse events among hospital patients in Canada. Can. Med. Assoc. J. 2004, 170, 1678–1686. [Google Scholar] [CrossRef]
- Wong, C.A.; Cummings, G.G.; Ducharme, L. The relationship between nursing leadership and patient outcomes: A systematic review update. J. Nurs. Manag. 2013, 21, 709–724. [Google Scholar] [CrossRef] [PubMed]
- Tjosvold, D.; MacPherson, R.C. Joint hospital management by physicians and nursing administrators. Healthc. Manag. Rev. 1996, 21, 43–54. [Google Scholar] [CrossRef]


{kind=link}
| Author et al. (year) | Main Study Characteristics | Aim of the Study | Leadership Style Definition | Outcome Definition | Main Findings |
|---|---|---|---|---|---|
| Al-Mailam (2004) [13] | Kuwait, cross-sectional study Four public and private hospitals 266 administrators and physicians | To explore the impact of leadership styles on employee perception of leadership efficacy. | Two categories of administrators’ and physicians’ leadership style:
| Leadership style (Multifactor Leadership Questionnaire) | Leadership style (midpoint = 33, average score) Hospital director: 26.89 Department Head: 25.74 Leadership efficacy [midpoint = 6.0 average score, (F-value)] Both Medical director and Department Head = 4.44, (32.41 and 48.43) Type of hospital and transformational leadership style (average score, (SE)) public vs. private hospital Hospital director: 29.48 (0.71) vs. 24.62 (0.73) Department head: 27.28 (0.71) vs. 24.41 (0.67) |
| Armstrong et al. (2006) [14] | Central Canada, Small community hospital 40 staff nurses | To test a theoretical model. | Structural empowerment (Conditions of Work Effectiveness Questionnaire-II) Magnet hospital characteristics—Practice Environment (Lake’s Practice Environment Scale of the Nursing Work Index, PES of NWI) Safety climate (The Safety Climate Survey) | Total Empowerment scale [mean score (SD)] 17.1 (4.26) Cronbach α = 0.94 Total PES [mean score(SD)] 2.5 (0.64) Cronbach α = 0.85 Safety Climate [mean score(SD)] 3.53 (0.80) Cronbach α = 0.81 Empowerment and professional practice characteristics [r (p-value)] Nursing model of care 0.61 (<0.01) Management ability 0.52 (<0.01) Collaborative relationships 0.316 (<0.005) Empowerment and patient safety culture [r (p-value)] Patient safety culture 0.50 (<0.01) Support 0.51 (<0.01) Informal power 0.43 (<0.01) Opportunity 0.45 (<0.01) Combined effect of magnet hospital characteristics on patient safety culture and empowerment 46% of variance, F = 13.32, dF = 1.31 p = 0.0001 | |
| Keroack et al. (2007) [15] | US, 2003–2005 Exploratory investigation 79 Academic Medical Centers patient-level data site visits | To identify organizational factors associated with quality and safety performance. | Hospitals’ leadership style:
| Patient safety (Agency for health Care Research and Quality, AHRQ-preventable complications, and Patient Safety Indicators) Mortality (mortality rates bases on AHRQ and inpatient quality indicators, IQIs) Effectiveness (The Joint Commission Hospital Core Measures) Equity (Measures) | Composite scores for quality and safety CI 95% (median score %) Group 1 vs. Group 2 vs. Group 3 vs. Group 4 vs. Group 5 67.18% vs. 62.36% vs. 60.22% vs. 58.68% vs. 56.05% Factors associated with top performing organizations:
|
| Kvist et al. (2007) [16] | Finland Kuopio University Hospital 631 patients 690 nurses 76 managers 128 doctors | To investigate the perception of the quality of care and the relationships between organizational factors and quality of care. | Quality of care (measured by Humane Caring Scale) Organizational factors (by using questionnaires) | Quality of care (ratings) Patients 1.51 to1.66 Nurses 1.81 to2.19 Managers 1.82 to 2.08 Organizational factors an Quality of care
Nursing staff: work vs. values 0.248 (0.01) vs. 0.447 (0.001) Managers: Work vs. leadership 0.472 (0.05) vs. 0.568 (0.05 Physicians: work vs. values 0.289 (0.05) vs. 0.539 (0.05) | |
| Vogus, Sutcliffe (2007) [17] | US, 2003–2004 cross-sectiona l1033 RNs 78 nursing managers 78 care units | To examine the benefits of bundling safety organizing with leadership and design factors on reported medication errors. | Safety organizing (Safety organizing Scale) Trust in manager (2 survey items assessing perceptions for nurse manager) Use of care pathways (Seven-point Likert Scale, single survey item) Reported Medications errors (number of errors reported to a unit's incident reporting system) | Medications errors (mean, SD) 12.04, 11.31 Safety organizing and trusted leadership (β, coefficient, p-value) −0.60, 0.18, p < 0.001 Safety organizing and care pathways −0.82, 0.25, p < 0.001 | |
| Casida, Pinto-Zipp (2008) [18] | New Jersey, US, 2006 Four acute care hospitals 37 Nurse Managers 278 staff nurses | To explore the relationship between nursing leadership styles and organizational culture. | Three categories of nurse managers’ leadership style:
| Leadership style (Multifactor Leadership Questionnaire) Nursing unit Organizational culture (the Denison’s Organizational Culture Survey) | Leadership style [MLQ scores, mean (SD)] Transformational vs. transactional vs. laissez-faire 2.8 (0.83) vs. 2.1 (0.47) vs. 0.83 (0.90) NMs’ leadership style and organizational culture (r, p-value) Transformational vs. transactional vs. laissez-faire 0.60 (p = 0.00) vs.0.16 p = 0.006) vs.−0.34 (p = 0.000) |
| Raup (2008) [19] | US 15 academic health centers 15 managers 15 staff nurses | To explore the role of leadership styles used by nurse managers in nursing turnover and patient satisfaction. | Two categories of ED nurse managers’ leadership style:
| Leadership style (Multifactor Leadership Questionnaire, MLQ) Nurse staff turnover and patient satisfaction (managers’ data for nurse turnover and patient safety scores) | Leadership style (% ED nurse managers) transformational vs. Non-transformational 80% vs. 20% Nurse staff turnover and patient satisfaction [impact of leadership style: Fisher’s exact test = 0.569] Mean staff nurse turnover (%) transformational vs. Non-transformational 13% vs. 29% Mean ED overall patient satisfaction (%) transformational vs. Non-transformational76.68% vs. 76.50% |
| McCutcheon et al. (2009) [20] | Canada Correlation survey Seven hospitals 51 units 41 nurse managers 717 nurses 680 patients | To assess the relationship between leadership style, nurses’ job satisfaction, span of control, and patient satisfaction. | Four categories of managers’ leadership style:
| Nurses’ Job Satisfaction (measured by McCloskey-Mueller Satisfaction Scale Patient Satisfaction (measured by the Patient Judgments of Hospital Quality Questionnaire) | Nurses’ Job Satisfaction (Mean) 3.2 Patient Satisfaction (mean) 2.16 (moderate satisfaction) JS and leadership style Transformational vs. transactional vs. management by exception vs. laissez-faire (Beta) 0.20 vs. 0.12 vs. −0.08 vs. 0.02 Span of control and leadership style on JS Transformational vs. transactional vs. management by exception vs. laissez-faire [coefficient, (p-value)] −0.0024 (<0.01) vs. −0.0015 (<0.05) vs. 0.0026 (<0.01) vs. 0.0014 (<0.05) Span of control and leadership style on patient satisfaction [coefficient, (p-value)] Transformational vs. transactional vs. management by exception vs. laissez-faire −0079(<0.05) vs. −0070 vs. −0103 vs. 0.0045 |
| Singer et al. (2009) [21] | US, 2004–2005 92 hospitals senior managers, physicians, hospital workers questionnaires 18361 safety climate surveys 5637 organizational culture surveys | To assess the aspects of general organizational culture that are related to hospital patient safety climate. | Safety climate (Patient Safety Climate in Healthcare Organization) Organizational culture (Competing Values Framework) | Organisational culture (average score) hierarchical organizational culture vs. entrepreneurial culture 31.6 points vs. 15.7points Safety climate (% PPR-percent problematic response) (higher PPR relates to lower level of safety climate) 17.1% PPR Highest safety climate hospitals vs. lowest safety climate hospitals (mean PPR, p = 0.000) 11.5 vs. 24.6 Relationship of organizational characteristics with patient safety climate [overall average PPR (SD) p < 0.05] group culture vs. entrepreneurial culture vs. hierarchical culture vs. production-oriented culture −0.241 (0.011) vs.−0.279 (0.0022) vs. 0.300 (0.011) vs. 0.0666 (0.017) Organizational culture and safety climate [mean (SD] high vs. low safety climate group culture: 40.1 (6.7) vs. 26.9 (7.8) entrepreneurial: 15.3 (2.31) vs. 13.9 (0.9) production-oriented: 20.20 (2.1) vs. 22.4 (2.1) hierarchical: 24.6 (2.8) vs. 36.7 (6.2) | |
| Alahmadi (2010) [22] | Saudi Arabia, 13 general hospitals 223 health professions (nurses, technicians, managers, medical staff) | To assess whether organisation culture supports patient safety. | Patient safety culture (Hospital Survey on Patient Safety Culture questionnaire) | Patient safety Excellent or very good vs. acceptable vs. failing or poor (%) 60% vs. 33% vs. 7% Determinants of overall patient safety score(Standardised coefficient B) Organisational learning/continuous improvement: 0.128 Management role: 0.216 Communication and feedback about errors: 0.215 Teamwork: 0.160 | |
| Armellino et al. (2010) [23] | US descriptive correlation study Adult Critical Care Unit (ACCU) tertiary hospital 102 Registered Nurses | To explore the association between structural empowerment and patient safety culture among nurses. | Structural empowerment, SE (Conditions of Workplace Effectiveness Questionnaire) Patient safety climate (Hospital Survey on Patient Safety Culture) | Total structural empowerment, SE (CWEQ-II, mean score) 20.55 (moderate), Cronbach’s α = 0.89 Moderate SE vs. low level of SE vs. high level of SE (%) 79.2% vs. 1.98% vs. 18.91% Structural empowerment and patient safety climate (PSC)
| |
| Cummings et al. (2010) [24] | Canada, 1998–1999 Secondary analysis of data 90 hospitals 21,570 patients 5228 nurses | To explore the association of the role of hospital nursing leadership styles with 30-day mortality. | Five categories of hospitals’ leadership style:
| 30-day mortality | Hospital Nursing leadership styles and 30-day mortality High dissonant vs. moderately dissonant vs. mixed type vs. moderately resonant vs. high resonant (%) 4.3 vs. 8.8 vs. 8.1 vs. 7.4 vs. 5.2 High dissonant vs. moderately dissonant vs. mixed type vs. moderately resonant vs. high resonant Beta (SE) Ref vs.−0.64 (0.24) * vs. 0.05 (0.11) vs.−0.08 (0.10) vs.−0.40 (0.19) * High dissonant vs. moderately dissonant vs. mixed type vs. moderately resonant vs. high resonant aOR 95% CI Ref vs. 0.86 (0.56–1.31) vs. 1.10 (0.96–1.27) vs. 0.90 (0.77–1.04) vs. 0.77 (0.59–1.01) |
| Ginsburg et al. (2010) [25] | Canada, 2006 Two cross-sectional surveys 49 general acute care hospitals 54 patient safety officers (PSOs) 282 patient care managers (PCMs) PSOs and PCMs questionnaires | To explore organizational leadership towards patient safety and its relationship with five types of learning from patient safety events. | Two categories of organizational leadership style:
| Leadership style (PCM questionnaire) Learning from PSEs (four types of PSE-minor/moderate/major events/major near-miss) | Learning from PSEs [Mean (SD)] major event analysis 3.63 (0.56) major event dissemination/communication 2.86 (0.80) moderate event learning 3.03 (0.76) minor events learning 2.53 (0.67) major near-miss events learning 3.03 (0.75)formal organizational leadership 3.90 (0.44) informal organizational leadership 2.34 (1.28) Learning from Near-miss Events (β, p-value) hospital size −0.339 p < 0.10 formal leadership style 0.467 p < 0.05 Learning from Major events dissemination/communication (β, p-value) hospital size and formal leadership style −1.106, p < 0.001 |
| Purdy et al. (2010) [26] | Canada, Cross-sectional study 21 hospitals (61 medical and surgery units) 697 nurses 1005 patients | To assess the relationship of nurses' perceptions on their work environment and quality outcomes. | Work environment (Conditions of Workplace Effectiveness Questionnaire, and Work Group Characteristics Measure) Patient care quality/patient satisfaction (Nursing Care Quality Questionnaire and The Therapeutic Self-care Questionnaire-Acute Care Version) | Work environment and patient outcomes [χ2 = 21.074 df = 10] Work unit (β, p-value) structure empowerment and group processes 0.64 p < 0.001 group processes and nurse-assessed quality 0.61 p < 0.001 group processes and falls −0.19 p < 0.05 group processes and nurse-assessed risk −0.17 p < 0.05 Individual (β, p-value) psychological empowerment and empowerment behavior 0.47 p < 0.001 psychological empowerment and job satisfaction 0.39 p < 0.001 psychological empowerment and nurse assessed quality of care 0.22 p < 0.001 | |
| Squires et al. (2010) [27] | Ontario, Canada, 2008 cross-sectiona l267 nurses | To test a model of examining relationships among leadership, interactional justice, work environment, safety climate quality of the nursing and patient and nurse safety. | Nurse managers leadership:
| Leadership (measured by Resonant leadership Scale) Nursing work environment (by using Perceived nursing work environment) Safety climate (measured by Safety Climate Survey) | Final model χ2 = 217.6(138) p < 0.001 -resonant leadership and leader-nurse relationship (standardized coefficient) 0.52 nurse leader-nurse relationship and safety climate (standardized coefficient) 0.53 work environment and emotional exhaustion (standardized coefficient) −0.51 safety climate and medication errors (standardized coefficient) −0.22 |
| Castle, Decker (2011) [28] | US, 2008 3867 NHAs (Nursing Home Administrator) 3867 DONs (Director of Nursing) | To assess the relationship of leadership style and quality of care. | Four groups of leaders:
| Leadership style (Bonoma-Slevin leadership model) Quality of care (Nursing Home Compare Quality Measures and 5-Star Rating Scores) | Leadership style Consensus manager vs. consultative vs. shareholder manager vs. autocrat: NHA: 33% vs. 22% vs.19% vs. 26% DON: 30% vs. 20% vs.25% vs. 25% Leadership and quality of care [Incident-rate ratio (SE), p-value] NHA/DON both Consensus Managers: Percent physical restraint use: 0.97 (0.43), p < 0.05 Percent with moderate to severe pain: 0.51 (0.21), p < 0.01 Percent high-risk residents with pressure ulcers: 0.62 (0.24), p < 0.05 Percent had a catheter inserted and left in bladder: 0.79 (0.19), p < 0.001 NHA/DON both Consensus Managers: (Five-star quality measure score, squares regression) 4.02 p < 0.01 |
| Havig et al. (2011) [9] | Norway, Cross-sectional study 40 wards of nursing homes 414 employees 13 nursing home directors40 wards managers 444 staff questionnaires 378 relatives 900 h of field observation | To assess the relationship between ward leaders’ task—and leadership styles, on measures of quality of care. | 2 categories of hospitals’ leadership style:
| Quality of care (The national regulation for quality of care in nursing homes and home care) Staffing Care level | Leadership style and quality of care [coefficient (p-value) Task-oriented leadership style Relatives vs. staff vs. field observations 0.36 (0.02) vs. 0.63 (>0.01) vs. 0.28 (0.12) Relationship-oriented leadership style 0.12 (0.19) vs. 0.01 (0.91) vs. 0.10 (0.37) Staffing and quality of care [coefficient (p-value)Total staffing level Relatives vs. staff vs. field observations −0.95 (0.31) vs. 0.10 (0.90) vs. 1.17 (0.30) Ratio of RNs 0.32 (0.66) vs. 0.52 (0.42) vs. 0.20 (0.83) Ratio of unlicensed staff −2.05 (>0.01 vs. −0.80 (0.22) vs. −2.59 (>0.01) Care level [coefficient (p-value) Relatives vs. staff vs. field observations −0.20 (>0.01) vs. −0.11 (>0.01) vs. −0.11 (0.02) |
| Kvist et al. (2013) [29] | Finland, 2008–2009 Cross-sectional, descriptive quantitative design Four hospitals 2566 patients Nursing staff | To examine nurses’ and patients’ perceptions of the Magnet model components of transformational leadership and quality outcomes. | One category of hospitals’ leadership style:
| Transformational Leadership style (transformational leadership scale) Job satisfaction (The Kuopio University Hospital Job Satisfaction) Patient Safety Culture (The Hospital Survey on Patient Safety Culture) Patient Satisfaction (Revised Humane Caring Scale) | Transformational Leadership style Support for professional development by nurse managers (mean, SD) 3.66, 0.96 Patient Safety Culture (mean, SD)Teamwork within units 3.64, 0.69 Supervision 3.60, 0.80 Communication openness 3.57, 0.68 Patient Satisfaction (mean, SD, p-value) Professional practice 4.49, 0.67 Human resources 3.80, 1.13 PS average score (mean, SD) 4.18, 0.69 Total JS (mean, SD) 3.59, 0.62 Transformational leadership (mean, SD) 3.47, 0.81 Patient Safety Culture (mean, SD) 3.3, 0.47 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfantou, D.F.; Laliotis, A.; Patelarou, A.E.; Sifaki- Pistolla, D.; Matalliotakis, M.; Patelarou, E. Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review. Healthcare 2017, 5, 73. https://doi.org/10.3390/healthcare5040073
Sfantou DF, Laliotis A, Patelarou AE, Sifaki- Pistolla D, Matalliotakis M, Patelarou E. Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review. Healthcare. 2017; 5(4):73. https://doi.org/10.3390/healthcare5040073
Chicago/Turabian StyleSfantou, Danae F., Aggelos Laliotis, Athina E. Patelarou, Dimitra Sifaki- Pistolla, Michail Matalliotakis, and Evridiki Patelarou. 2017. "Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review" Healthcare 5, no. 4: 73. https://doi.org/10.3390/healthcare5040073