
Effectiveness of Acupuncture on Health-Related Quality of Life in Patients Receiving Maintenance Hemodialysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
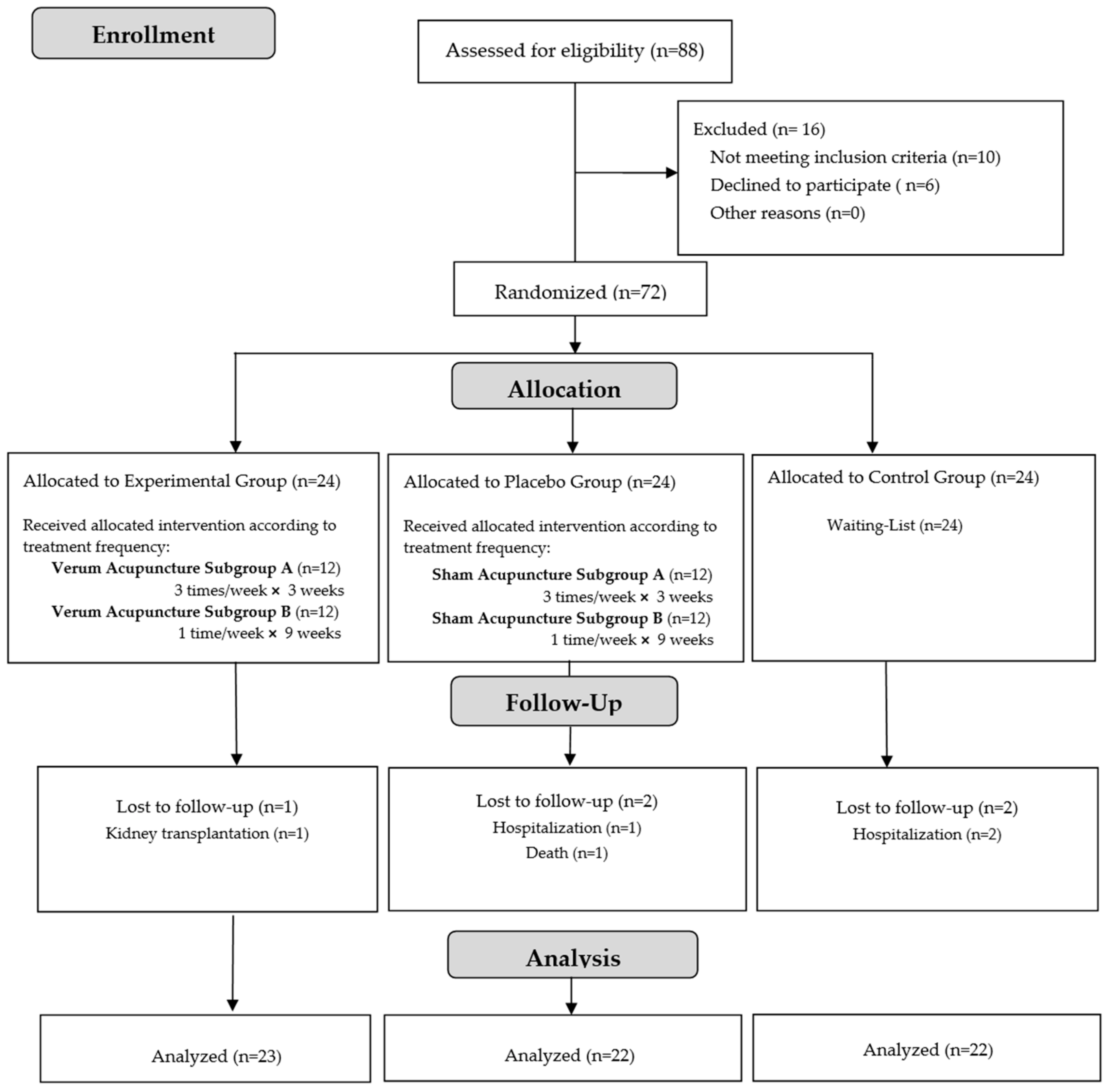
2.1. Study Design and Participants
2.2. Random Assignment and Masking
2.3. Intervention
2.3.1. Verum Acupuncture Group
2.3.2. Sham Acupuncture Group
2.3.3. Waiting List Group
2.4. Outcome Measurement
2.4.1. Kidney Disease Quality of Life—Short Form, Version 1.3 (KDQOL-SFTM 1.3)
2.4.2. Sociodemographic and Clinical Data Collection Form
2.5. Statistical Analysis and Sample Size
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, V.; Vilme, H.; Maciejewski, M.L.; Boulware, L.E. The Economic Burden of Chronic Kidney Disease and End-Stage Renal Disease. Semin. Nephrol. 2016, 36, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Sundström, J.; Bodegard, J.; Bollmann, A.; Vervloet, M.G.; Mark, P.B.; Karasik, A.; Taveira-Gomes, T.; Botana, M.; Birkeland, K.I.; Thuresson, M.; et al. Prevalence, outcomes, and cost of chronic kidney disease in a contemporary population of 2·4 million patients from 11 countries: The CaReMe CKD study. Lancet Reg. Health Eur. 2022, 20, 100438. [Google Scholar] [CrossRef] [PubMed]
- Vinhas, J.; Aires, I.; Batista, C.; Branco, P.; Brandão, J.; Nogueira, R.; Raposo, J.F.; Rodrigues, E. RENA Study: Cross-Sectional Study to Evaluate CKD Prevalence in Portugal. Nephron 2020, 144, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Kittiskulnam, P.; Sheshadri, A.; Johansen, K.L. Consequences of CKD on Functioning. Semin. Nephrol. 2016, 36, 305–318. [Google Scholar] [CrossRef]
- Golshayan, D.; Pascual, M. Burden of end-stage renal disease and evolving challenges in kidney transplantation. Transpl. Int. 2019, 32, 889–891. [Google Scholar] [CrossRef]
- Goh, Z.S.; Griva, K. Anxiety and depression in patients with end-stage renal disease: Impact and management challenges—A narrative review. Int. J. Nephrol. Renov. Dis. 2018, 11, 93–102. [Google Scholar] [CrossRef]
- Liew, A. Perspectives in renal replacement therapy: Haemodialysis. Nephrology 2018, 23 (Suppl. S4), 95–99. [Google Scholar] [CrossRef]
- Mapes, D.L.; Bragg-Gresham, J.L.; Bommer, J.; Fukuhara, S.; McKevitt, P.; Wikström, B.; Lopes, A.A. Health-related quality of life in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2004, 44, 54–60. [Google Scholar] [CrossRef]
- Fukuhara, S.; Lopes, A.A.; Bragg-Gresham, J.L.; Kurokawa, K.; Mapes, D.L.; Akizawa, T.; Bommer, J.; Canaud, B.J.; Port, F.K.; Held, P.J. Health-related quality of life among dialysis patients on three continents: The Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003, 64, 1903–1910. [Google Scholar] [CrossRef]
- Mapes, D.L.; Lopes, A.A.; Satayathum, S.; McCullough, K.P.; Goodkin, D.A.; Locatelli, F.; Fukuhara, S.; Young, E.W.; Kurokawa, K.; Saito, A.; et al. Health-related quality of life as a predictor of mortality and hospitalization: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Int. 2003, 64, 339–349. [Google Scholar] [CrossRef]
- Stengel, B.; Metzger, M.; Combe, C. Risk profile, quality of life and care of patients with moderate and advanced CKD: The French CKD-REIN Cohort Study. Nephrol. Dial. Transplant. 2019, 34, 277–286. [Google Scholar] [CrossRef]
- Legrand, K.; Speyer, E.; Stengel, B.; Frimat, L.; Ngueyon Sime, W.; Massy, Z.A.; Fouque, D.; Laville, M.; Combe, C.; Jacquelinet, C.; et al. Perceived Health and Quality of Life in Patients With CKD, Including Those With Kidney Failure: Findings From National Surveys in France. Am. J. Kidney Dis. 2020, 75, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Chuasuwan, A.; Pooripussarakul, S.; Thakkinstian, A.; Ingsathit, A.; Pattanaprateep, O. Comparisons of quality of life between patients underwent peritoneal dialysis and hemodialysis: A systematic review and meta-analysis. Health Qual. Life Outcomes 2020, 18, 191. [Google Scholar] [CrossRef]
- van Loon, I.N.; Bots, M.L.; Boereboom, F.T.J.; Grooteman, M.P.C.; Blankestijn, P.J.; van den Dorpel, M.A.; Nubé, M.J.; Ter Wee, P.M.; Verhaar, M.C.; Hamaker, M.E. Quality of life as indicator of poor outcome in hemodialysis: Relation with mortality in different age groups. BMC Nephrol. 2017, 18, 217. [Google Scholar] [CrossRef] [PubMed]
- Hall, R.K.; Luciano, A.; Pieper, C.; Colón-Emeric, C.S. Association of Kidney Disease Quality of Life (KDQOL-36) with mortality and hospitalization in older adults receiving hemodialysis. BMC Nephrol. 2018, 19, 11. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, Y.C.; Kwon, S.; Li, L.; Oh, S.; Kim, D.H.; An, J.N.; Cho, J.H.; Kim, D.K.; Kim, Y.L.; et al. Impact of health-related quality of life on survival after dialysis initiation: A prospective cohort study in Korea. Kidney Res. Clin. Pract. 2020, 39, 426–440. [Google Scholar] [CrossRef]
- Wirkner, J.; Scheuch, M.; Dabers, T.; Freiin von Rheinbaben, S.; Fiene, B.; Aymanns, S.; Endlich, K.; Endlich, N.; Lendeckel, U.; Rettig, R.; et al. Comorbid Depression and Diabetes Are Associated with Impaired Health-Related Quality of Life in Chronic Kidney Disease Patients. J. Clin. Med. 2022, 11, 4671. [Google Scholar] [CrossRef]
- Foundation, N.K. K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am. J. Kidney Dis. 2002, 39, S1–S266. [Google Scholar]
- Dyer, N.L.; Surdam, J.; Srinivasan, R.; Agarwal, A.; Dusek, J.A. The Impact of Individualized Complementary and Integrative Health Interventions Provided in Clinical Settings on Quality of Life: A Systematic Review of Practice-Based Research. J. Integr. Complement. Med. 2022, 28, 618–640. [Google Scholar] [CrossRef]
- Lin, W.F.; Zhong, M.F.; Zhou, Q.H.; Zhang, Y.R.; Wang, H.; Zhao, Z.H.; Cheng, B.B.; Ling, C.Q. Efficacy of complementary and integrative medicine on health-related quality of life in cancer patients: A systematic review and meta-analysis. Cancer Manag. Res. 2019, 11, 6663–6680. [Google Scholar] [CrossRef]
- Yang, J.; Wahner-Roedler, D.L.; Zhou, X.; Johnson, L.A.; Do, A.; Pachman, D.R.; Chon, T.Y.; Salinas, M.; Millstine, D.; Bauer, B.A. Acupuncture for palliative cancer pain management: Systematic review. BMJ Support. Palliat. Care 2021, 11, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Xu, L.; Lin, X.; Li, Q.; Ye, P.; Wu, L.; Wang, M.; Li, L.; Li, L.; Zhang, Y.; et al. Effectiveness and safety of acupuncture combined with traditional Chinese medicine in the treatment of chronic prostatitis: A systematic review and meta-analysis. Medicine 2021, 100, e28163. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Li, T.; Ma, C.; Liu, H.; Liang, F.; Yang, Y. Comparative efficacy of acupuncture-related therapy for migraine: A systematic review and network meta-analysis. Front. Neurol. 2022, 13, 1010410. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Duan, H.; Lian, A.; Zhuang, M.; Zhao, X.; Liu, X. Rehabilitation Effects of Acupuncture on the Diaphragm Dysfunction in Chronic Obstructive Pulmonary Disease: A Systematic Review. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 2023–2037. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.C.; Chen, H.; Xu, W.T.; Song, Y.Y.; Gu, Y.H.; Ni, G.X. Acupuncture therapy for fibromyalgia: A systematic review and meta-analysis of randomized controlled trials. J. Pain Res. 2019, 12, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.C.; Yang, M.C.; Wu, Y.K.; Chen, H.Y.; Tzeng, I.S.; Hsu, P.S.; Lee, C.T.; Chen, C.L.; Lan, C.C. Acupuncture therapy improves health-related quality of life in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2019, 35, 208–218. [Google Scholar] [CrossRef]
- Zhu, Y.J.; Wu, X.Y.; Wang, W.; Chang, X.S.; Zhan, D.D.; Diao, D.C.; Xiao, J.; Li, Y.; Ma, D.; Hu, M.; et al. Acupuncture for Quality of Life in Gastric Cancer Patients Undergoing Adjuvant Chemotherapy. J. Pain Symptom Manag. 2022, 63, 210–220. [Google Scholar] [CrossRef]
- Kim, K.H.; Kim, T.H.; Kang, J.W.; Sul, J.U.; Lee, M.S.; Kim, J.I.; Shin, M.S.; Jung, S.Y.; Kim, A.R.; Kang, K.W.; et al. Acupuncture for symptom management in hemodialysis patients: A prospective, observational pilot study. J. Altern. Complement. Med. 2011, 17, 741–748. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, M.S.; Kim, T.H.; Kang, J.W.; Choi, T.Y.; Lee, J.D. Acupuncture and related interventions for symptoms of chronic kidney disease. Cochrane Database Syst. Rev. 2016, 2016, Cd009440. [Google Scholar] [CrossRef]
- Bullen, A.; Awdishu, L.; Lester, W.; Moore, T.; Trzebinska, D. Effect of Acupuncture or Massage on Health-Related Quality of Life of Hemodialysis Patients. J. Altern. Complement. Med. 2018, 24, 1069–1075. [Google Scholar] [CrossRef]
- Jung, H.K.; Lai, T.H.; Lai, J.N.; Lin, J.G.; Kao, S.T. Preserving residual renal function: Is interdialytic acupuncture an add-on option? A case series report. Explore 2022, 18, 710–713. [Google Scholar] [CrossRef] [PubMed]
- Correia de Carvalho, M.; Nunes de Azevedo, J.; Azevedo, P.; Pires, C.; Laranjeira, M.; Machado, J.P. Effect of Acupuncture on Functional Capacity in Patients Undergoing Hemodialysis: A Patient-Assessor Blinded Randomized Controlled Trial. Healthcare 2022, 10, 1947. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, Y.; Xiao, X.; Shi, Y.; Xu, D.; Li, N.; Deng, Y. Acupuncture for Uremic Pruritus: A Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2023, 65, e51–e62. [Google Scholar] [CrossRef] [PubMed]
- Correia de Carvalho, M.; Pereira Machado, J.; Laranjeira, M.; Nunes de Azevedo, J.; Azevedo, P. Effect of Acupuncture on Functional Capacity and Health-Related Quality of Life of Hemodialysis Patients: Study Protocol for a Randomized Controlled Trial. Healthcare 2022, 10, 2050. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed]
- Maciocia, G. The Foundations of Chinese Medicine. A Comprehensive Text, 3rd ed.; Elsevier: Amsterdam, The Netherlands, 2015; pp. 1–1319. [Google Scholar]
- Li, W.; David, F. Clinical Nephrology in Chinese Medicine; Blue Poppy Press: Portland, OR, USA, 2003. [Google Scholar]
- Matos, L.C.; Machado, J.P.; Monteiro, F.J.; Greten, H.J. Understanding Traditional Chinese Medicine Therapeutics: An Overview of the Basics and Clinical Applications. Healthcare 2021, 9, 257. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.; Anes, E. Medição da qualidade de vida de insuficientes renais crónicos: Criação da versão portuguesa do KDQOL-SF. Rev. Port. Saúde Pública 2009, 28, 31–39. [Google Scholar]
- Hays, R.D.; Kallich, J.D.; Mapes, D.L.; Coons, S.J.; Carter, W.B. Development of the kidney disease quality of life (KDQOL) instrument. Qual. Life Res. 1994, 3, 329–338. [Google Scholar] [CrossRef]
- Hays, R.D.; Kallich, J.; Mapes, D.; Coons, S.; Amin, N.; Carter, W.B.; Kamberg, C. Kidney Disease Quality of Life Short Form (KDQOL-SF & Trade;), Version 1.3: A Manual for Use and Scoring; RAND Corporation: Santa Monica, CA, USA, 1997. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; Released 2020; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Cabrera, V.J.; Hansson, J.; Kliger, A.S.; Finkelstein, F.O. Symptom Management of the Patient with CKD: The Role of Dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 687–693. [Google Scholar] [CrossRef]
- Li, Y.N.; Shapiro, B.; Kim, J.C.; Zhang, M.; Porszasz, J.; Bross, R.; Feroze, U.; Upreti, R.; Martin, D.; Kalantar-Zadeh, K.; et al. Association between quality of life and anxiety, depression, physical activity and physical performance in maintenance hemodialysis patients. Chronic Dis. Transl. Med. 2016, 2, 110–119. [Google Scholar] [CrossRef]
- Lin, L.L.; Tu, J.F.; Wang, L.Q.; Yang, J.W.; Shi, G.X.; Li, J.L.; Zhang, N.; Shao, J.K.; Zou, X.; Liu, C.Z. Acupuncture of different treatment frequencies in knee osteoarthritis: A pilot randomised controlled trial. Pain 2020, 161, 2532–2538. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.W.; Wang, L.Q.; Zou, X.; Yan, S.Y.; Wang, Y.; Zhao, J.J.; Tu, J.F.; Wang, J.; Shi, G.X.; Hu, H.; et al. Effect of Acupuncture for Postprandial Distress Syndrome: A Randomized Clinical Trial. Ann. Intern. Med. 2020, 172, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Zhong, R.F.; Yin, X.H.; Cao, Y.H.; Zhang, X.F.; Zhang, Y.N.; Guo, B.; Xiao, X.L. Efficacy comparision of lumbar disc herniation treated with acupuncture at different time intervals. Zhongguo Zhen Jiu 2019, 39, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Yu, L.; Luo, X.; Wang, M.; Chen, G.; Zhang, Q.; Liu, W.; Zhou, Z.; Song, J.; Jing, H.; et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: Multicentre, randomised clinical trial. BMJ 2020, 368, m697. [Google Scholar] [CrossRef] [PubMed]
- Hershman, D.L.; Unger, J.M.; Greenlee, H.; Capodice, J.L.; Lew, D.L.; Darke, A.K.; Kengla, A.T.; Melnik, M.K.; Jorgensen, C.W.; Kreisle, W.H.; et al. Effect of Acupuncture vs Sham Acupuncture or Waitlist Control on Joint Pain Related to Aromatase Inhibitors Among Women With Early-Stage Breast Cancer: A Randomized Clinical Trial. JAMA 2018, 320, 167–176. [Google Scholar] [CrossRef]
- Rehman, I.U.; Ahmed, R.; Rahman, A.U.; Wu, D.B.C.; Munib, S.; Shah, Y.; Khan, N.A.; Rehman, A.U.; Lee, L.H.; Chan, K.G.; et al. Effectiveness and safety profiling of zolpidem and acupressure in CKD associated pruritus: An interventional study. Medicine 2021, 100, e25995. [Google Scholar] [CrossRef]
- Yıldırım Keskin, A.; Taşci, S. The Effect of Acupressure Applied to Individuals Receiving Hemodialysis Treatment on Severity of Thirst and Quality of Life. Altern. Ther. Health Med. 2021, 27, 20–30. [Google Scholar]
- Bao, T.; Baser, R.; Chen, C.; Weitzman, M.; Zhang, Y.L.; Seluzicki, C.; Li, Q.S.; Piulson, L.; Zhi, W.I. Health-Related Quality of Life in Cancer Survivors with Chemotherapy-Induced Peripheral Neuropathy: A Randomized Clinical Trial. Oncologist 2021, 26, e2070–e2078. [Google Scholar] [CrossRef]
- Pei, M.; Aguiar, R.; Pagels, A.A.; Heimbürger, O.; Stenvinkel, P.; Bárány, P.; Medin, C.; Jacobson, S.H.; Hylander, B.; Lindholm, B.; et al. Health-related quality of life as predictor of mortality in end-stage renal disease patients: An observational study. BMC Nephrol. 2019, 20, 144. [Google Scholar] [CrossRef]
- Evans, M.; Lewis, R.D.; Morgan, A.R.; Whyte, M.B.; Hanif, W.; Bain, S.C.; Davies, S.; Dashora, U.; Yousef, Z.; Patel, D.C.; et al. A Narrative Review of Chronic Kidney Disease in Clinical Practice: Current Challenges and Future Perspectives. Adv. Ther. 2022, 39, 33–43. [Google Scholar] [CrossRef]
- Hall, R.K.; Cary, M.P., Jr.; Washington, T.R.; Colón-Emeric, C.S. Quality of life in older adults receiving hemodialysis: A qualitative study. Qual. Life Res. 2020, 29, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.J.; Wang, W.J.; Tang, M.; Chen, H.; Ding, F. Mental health status and quality of life in patients with end-stage renal disease undergoing maintenance hemodialysis. Ann. Palliat. Med. 2021, 10, 6112–6121. [Google Scholar] [CrossRef] [PubMed]
- Cepeda Marte, J.L.; Javier, A.; Ruiz-Matuk, C.; Paulino-Ramirez, R. Quality of Life and Nutritional Status in diabetic patients on hemodialysis. Diabetes Metab. Syndr. 2019, 13, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, B.R.; Damery, S.; Aiyegbusi, O.L.; Anderson, N.; Calvert, M.; Cockwell, P.; Ferguson, J.; Horton, M.; Paap, M.C.S.; Sidey-Gibbons, C.; et al. Symptom burden and health-related quality of life in chronic kidney disease: A global systematic review and meta-analysis. PLoS Med. 2022, 19, e1003954. [Google Scholar] [CrossRef] [PubMed]
- Rao, Q.; Zeng, J.; Wang, S.; Hao, J.; Jiang, M. Chronic Pain and Quality of Life in Maintenance Hemodialysis Patients in China: A Multicenter, Cross-Sectional Study. J. Pain Res. 2022, 15, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.D.; Cukor, D.; Kimmel, P.L. Anxiety in Patients Treated with Hemodialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 2250–2255. [Google Scholar] [CrossRef]
- Pretto, C.R.; Winkelmann, E.R.; Hildebrandt, L.M.; Barbosa, D.A.; Colet, C.F.; Stumm, E.M.F. Quality of life of chronic kidney patients on hemodialysis and related factors. Rev. Lat. Am. Enferm. 2020, 28, e3327. [Google Scholar] [CrossRef]
- Brown, E.A.; Zhao, J.; McCullough, K.; Fuller, D.S.; Figueiredo, A.E.; Bieber, B.; Finkelstein, F.O.; Shen, J.; Kanjanabuch, T.; Kawanishi, H.; et al. Burden of Kidney Disease, Health-Related Quality of Life, and Employment Among Patients Receiving Peritoneal Dialysis and In-Center Hemodialysis: Findings From the DOPPS Program. Am. J. Kidney Dis. 2021, 78, 489–500.e481. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Screening | Baseline | Treatment | Follow-Up after Treatment | ||||
|---|---|---|---|---|---|---|---|
| 0-Week | 1-Week | 3-Week | 9-Week | 12-Week | |||
| Patient | Eligibility | X | |||||
| Informed Consent | X | ||||||
| Demographics and clinical data | X | ||||||
| Physical examination | X | ||||||
| Randomization | X | ||||||
| Laboratorial data | X | X | |||||
| Intervention | Verum Acupuncture Subgoup A (VA SgA) | 9 Acupuncture treatments (3 sessions per week for 3 weeks) | X | ||||
| Verum Acupuncture Subgroup B (VA SgB) | 9 Acupuncture treatments (1 session per week for 9 weeks) | ||||||
| Comparison | Sham Acupuncture Subgroup A (SA SgA) | 9 Acupuncture treatments in non-acupuncture points (3 sessions per week for 3 weeks) | X | ||||
| Sham Acupuncture Subgroup B (SA SgB) | 9 Acupuncture treatments in non-acupuncture points (1 session per week for 9 weeks) | X | |||||
| Waiting-List Group (WL) | Non-Acupuncture Treatment | X | |||||
| Outcomes | Health-related Quality of Life (Kidney Disease Quality of Life-Short Form, Version 1.3–KDQOL–SFTM 1.3) | X | X | X | X | ||
| Assessment of blinding success | X | X | |||||
| Participant Safety | Adverse effects | X | X | X | X | ||
| Variables | Total (n = 67) | Verum Acupuncture (VA) Group (n = 23) | Sham Acupuncture (SA) Group (n = 22) | Waiting-List (WL) Group (n = 22) | p |
|---|---|---|---|---|---|
| Sociodemographic | |||||
| Gender | |||||
| Female | 26 (38.8%) | 9 (39.1%) | 8 (36.4%) | 9 (40.9%) | 1.000 (1) |
| Male | 41 (61.2%) | 14 (60.9%) | 14 (63.6%) | 13 (59.1%) | |
| Age | |||||
| Minimum–Maximum | 56–91 | 60–84 | 57–91 | 56–87 | |
| Mean (SD) | 71.6 (7.7) | 71.2 (5.1) | 72.6 (8.3) | 71.0 (9.4) | 0.764 (2) |
| Level of education | |||||
| No literacy | 5 (7.5%) | 0 (0.0%) | 2 (9.1%) | 3 (13.6%) | 0.279 (1) |
| 1° Cycle (4 years) | 49 (73.1%) | 20 (87.0%) | 17 (77.3%) | 12 (54.5%) | |
| 2° Cycle (6 years) | 7 (10.4%) | 2 (8.7%) | 1 (4.5%) | 4 (18.2%) | |
| 3° Cycle (9 years) | 1 (1.5%) | 0 (0.0%) | 0 (0.0%) | 1 (4.5%) | |
| High school (12 years) | 5 (7.5%) | 1 (4.3%) | 2 (9.1%) | 2 (9.1%) | |
| Employment status | |||||
| Employed | 4 (6.0%) | 0 (0.0%) | 2 (9.1%) | 2 (9.1%) | 0.481 (1) |
| Self-employed | 4 (6.0%) | 2 (8.7%) | 0 (0.0%) | 2 (9.1%) | |
| Unemployed | 2 (3.0%) | 1 (4.3%) | 1 (4.5%) | 0 (0.0%) | |
| Retired | 57 (85.1%) | 20 (87.0%) | 19 (86.4%) | 18 (81.8%) | |
| Clinical | |||||
| Hemodialysis time | |||||
| <12 months | 2 (3.0%) | 2 (8.7%) | 0 (0.0%) | 0 (0.0%) | 0.240 (1) |
| 12 to 120 months | 56 (83.6%) | 19 (82.6%) | 20 (90.9%) | 17 (77.3%) | |
| >120 months | 9 (13.4%) | 2 (8.7%) | 2 (9.1%) | 5 (22.7%) | |
| Vascular access | |||||
| Arteriovenous fistula (AVF) | 61 (91.0%) | 22 (95.7%) | 18 (81.8%) | 21 (95.5%) | 0.306 (1) |
| Central venous catheter (CVC) | 6 (9.0%) | 1 (4.3%) | 4 (18.2%) | 1 (4.5%) | |
| Laboratorial | Mean (SD) | ||||
| Hemoglobin (g/dL) | 10.93 (1.03) | 10.88 (0.94) | 10.86 (1.05) | 11.05 (1.12) | 0.797 (2) |
| Potassium (mEq/L) | 5.44 (0.81) | 5.52 (0.89) | 5.35 (0.81) | 5.45 (0.74) | 0.799 (2) |
| Calcium (mg/dL) | 9.11 (0.51) | 9.13 (0.55) | 9.10 (0.49) | 9.10 (0.51) | 0.970 (2) |
| Phosphorus (mg/dL) | 4.74 (1.13) | 4.71 (1.17) | 4.70 (1.25) | 4.80 (1.00) | 0.944 (2) |
| Sodium (mg/dL) | 138.1 (3.0) | 138.5 (2.9) | 138.6 (3.8) | 137.3 (2.0) | 0.296 (2) |
| Albumin (g/dL) | 3.91 (0.28) | 3.98 (0.27) | 3.81 (0.27) | 3.95 (0.29) | 0.101 (2) |
| Urea (before HD) (mg/dL) | 152.6 (37.5) | 161.0 (37.9) | 145.3 (36.2) | 151.0 (38.3) | 0.369 (2) |
| Creatinine (mg/dL) | 9.94 (2.12) | 10.15 (2.26) | 9.51 (1.94) | 10.16 (2.16) | 0.514 (2) |
| Parathyroid hormone (pg/mL) | 418.0 (243.2) | 454.2 (256.9) | 358.2 (193.3) | 439.9 (271.5) | 0.370 (2) |
| Cholesterol (mg/dL) | 162.8 (37.1) | 166.0 (47.2) | 155.5 (35.8) | 166.6 (25.0) | 0.536 (2) |
| Verum Acupuncture (VA) Group | Sham Acupuncture (SA) Group | |||||
|---|---|---|---|---|---|---|
| HRQOL Domains | Treatment Frequency 3 × 3 (n = 12) | Treatment Frequency 1 × 9 (n = 11) | p | Treatment Frequency 3 × 3 (n = 12) | Treatment Frequency 1 × 9 (n = 10) | p |
| Kidney disease targeted areas Symptom/problem list | 78.0 ± 15.6 | 81.6 ± 10.1 | 81.6 ± 10.6 | 89.6 ± 8.4 | ||
| Baseline–after treatment | 10.9 ± 8.4 | 9.3 ± 4.8 | 0.709 | 0.6 ± 3.3 | −0.7 ± 1.9 | 0.214 |
| Baseline–12-week follow-up | 0.5 ± 4.5 | −1.1 ± 3.3 | 0.281 | −2.5 ± 2.5 | −1.1 ± 2.9 | 0.768 |
| Effects of kidney disease | 65.6 ± 15.9 | 62.5 ± 20.1 | 71.0 ± 24.0 | 79.8 ± 11.9 | ||
| Baseline–after treatment | 4.4 ± 4.3 | 3.1 ± 3.4 | 0.352 | −0.5 ± 5.0 | −3.1 ± 4.4 | 0.146 |
| Baseline–12-week follow-up | 1.0 ± 4.3 | −0.3 ± 5.5 | 0.296 | −2.3 ± 2.7 | −1.6 ± 2.2 | 0.833 |
| Burden of kidney disease | 34.4 ± 17.4 | 36.9 ± 16.2 | 38.0 ± 31.8 | 30.6 ± 21.3 | ||
| Baseline–after treatment | 2.1 ± 6.2 | 0.6 ± 3.4 | 0.445 | −0.6 ± 6.0 | 2.1 ± 7.9 | 0.335 |
| Baseline–12-week follow-up | −1.0 ± 3.6 | −3.4 ± 7.6 | 0.594 | −1.6 ± 1.8 | −0.3 ± 3.5 | 0.883 |
| Cognitive function | 83.9 ± 19.2 | 81.2 ± 14.2 | 91.1 ± 11.1 | 88.7 ± 7.7 | ||
| Baseline–after treatment | 3.3 ± 6.7 | 6.7 ± 8.4 | 0.315 | −1.7 ± 5.8 | −0.7 ± 3.8 | 0.766 |
| Baseline–12-week follow-up | −1.4 ± 2.8 | −0.4± 3.1 | 0.158 | −1.1 ± 2.6 | 0.0 ± 0.0 | 0.298 |
| Quality of social interaction | 83.9 ± 18.1 | 78.8 ± 20.6 | 79.4 ± 17.2 | 84.0 ± 6.4 | ||
| Baseline–after treatment | 0.6 ± 9.6 | 3.2 ± 9.6 | 0.746 | −2.8 ± 4.5 | −0.7 ± 3.8 | 0.179 |
| Baseline–12-week follow-up | −9.7 ± 8.7 | −11.8 ± 19.0 | 0.924 | −7.9 ± 14.9 | −5.7 ± 3.2 | 0.800 |
| Sleep | 65.0 ± 20.5 | 63.0 ± 21.2 | 57.9 ± 18.1 | 68.3 ± 12.8 | ||
| Baseline–after treatment | 4.0 ± 15.0 | 6.1 ± 8.4 | 0.615 | −5.2 ± 10.1 | −5.8 ± 9.7 | 0.840 |
| Baseline–12-week follow-up | −7.5 ± 5.8 | −10.5 ± 11.7 | 0.283 | 0.6 ± 5.4 | −4.0 ± 18.7 | 0.642 |
| Overall Health | 63.3 ± 17.8 | 56.4 ± 10.3 | 58.3 ± 18.5 | 49.0 ± 5.7 | ||
| Baseline–after treatment | 2.5 ± 7.5 | 4.5 ± 9.3 | 0.598 | −1.7 ± 11.1 | 1.0 ± 5.7 | 0.393 |
| Baseline–12-week follow-up | −1.7 ± 7.2 | 0.0 ± 6.3 | 0.677 | −4.2 ± 13.8 | 2.0 ± 6.3 | 0.245 |
| 36-item health survey (SF-36) SF12-Physical composite | 37.8 ± 10.9 | 36.1 ± 7.8 | 37.3 ± 10.4 | 38.9 ± 12.4 | ||
| Baseline–after treatment | 3.1 ± 5.3 | 3.6 ± 4.4 | 0.518 | −0.7 ± 3.1 | −1.4 ± 3.2 | 0.509 |
| Baseline–12-week follow-up | −0.9 ± 5.1 | −1.7 ± 4.5 | 0.782 | −2.3 ± 4.5 | −4.2 ± 5.1 | 0.176 |
| SF12-Mental composite | 50.8 ± 10.6 | 43.4 ± 10.3 | 44.3 ± 8.7 | 44.0 ± 7.3 | ||
| Baseline–after treatment | 3.9 ± 7.5 | 2.8 ± 6.9 | 0.601 | −0.5 ± 3.0 | 0.2 ± 1.7 | 0.741 |
| Baseline–12-week follow-up | −2.4 ± 3.8 | −1.5 ± 6.5 | 0.406 | −0.7 ± 3.2 | 1.4 ± 3.9 | 0.373 |
| HRQOL Domains/ KDQOL-SFTM 1.3 Scores | Verum Acupuncture (VA) Group (n = 23) | Sham Acupuncture (SA) Group (n = 22) | Waiting-List (WL) Group (n = 22) | p |
|---|---|---|---|---|
| Primary Outcome | ||||
| 36-item health survey (SF-36) scale | ||||
| Physical composite summary (PCS) | 37.0 ± 9.4 | 38.1 ± 11.1 | 38.2 ± 8.5 | 0.953 |
| Baseline–after treatment | 3.34 ± 4.77 ** | −1.02 ± 3.11 A | −2.27 ± 5.61 *A | <0.001 |
| Baseline–follow-up | −1.29 ± 4.72 | −3.18 ± 4.73 * | −3.50 ± 5.03 * | 0.283 |
| Secondary Outcomes | ||||
| Kidney disease targeted areas | ||||
| Symptom/problem list | 79.7 ± 13.1 | 85.2 ± 10.3 | 83.0 ± 8.8 | 0.320 |
| Baseline–after treatment | 10.14 ± 6.83 ** | 0.09 ± 3.18 A | −1.04 ± 2.47 A | <0.001 |
| Baseline–12–week follow–up | −0.27 ± 3.99 | −1.80 ± 2.67 * | −1.14 ± 3.20 | 0.409 |
| Effects of kidney disease | 64.1 ± 17.6 | 74.7 ± 20.5 | 70.0 ± 19.4 | 0.151 |
| Baseline–after treatment | 3.80 ± 3.88 ** | −1.70 ± 4.80 A | −1.85 ± 2.67 *A | <0.001 |
| Baseline–12-week follow-up | 0.41 ± 4.83 | −1.99 ± 2.47 * | −0.57 ± 1.57 | 0.244 |
| Burden of kidney disease | 35.6 ± 16.5 | 34.7 ± 27.2 | 43.5 ± 23.9 | 0.337 |
| Baseline–after treatment | 1.36 ± 4.97 | 0.57 ± 7.19 | −3.69 ± 9.18 | 0.084 |
| Baseline–12-week follow-up | −2.17 ± 5.84 | −0.57 ± 2.67 | −4.26 ± 12.56 | 0.586 |
| Cognitive function | 82.6 ± 16.7 | 90.0 ± 9.6 | 87.6 ± 12.6 | 0.431 |
| Baseline–after treatment | 4.93 ± 7.58 ** | −1.21 ± 4.88 A | −3.94 ± 8.40 *A | 0.001 |
| Baseline–12-week follow-up | −0.87 ± 3.05 | −0.61 ± 1.96 | −2.12 ± 8.82 | 0.944 |
| Quality of social interaction | 81.4 ± 19.1 | 81.5 ± 13.3 | 80.3 ± 15.2 | 0.789 |
| Baseline–after treatment | 1.74 ± 9.69 | −1.82 ± 4.21 | −2.42 ± 13.58 | 0.096 |
| Baseline–12-week follow-up | −10.72 ± 14.32 ** | −6.97 ± 11.17 ** | −5.76 ± 13.22 * | 0.199 |
| Sleep | 64.0 ± 20.4 | 62.6 ± 16.4 | 59.7 ± 16.4 | 0.488 |
| Baseline–after treatment | 4.89 ± 12.69 * | −5.45 ± 9.69 *A | −4.55 ± 13.84 *A | 0.001 |
| Baseline–12-week follow-up | −8.80 ± 9.62 ** | −1.48 ± 13.06 A | −2.61 ± 13.53 A | 0.026 |
| Overall Health | 60.0 ± 14.8 | 54.1 ± 14.7 | 60.5 ± 17.0 | 0.270 |
| Baseline–after treatment | 3.48 ± 8.32 *A | −0.45 ± 8.99 AB | −3.18 ± 7.16 *B | 0.048 |
| Baseline–12-week follow-up | −0.87 ± 6.68 | −1.36 ± 11.25 | −5.45 ± 9.12 * | 0.084 |
| 36-item health survey (SF-36) scale | ||||
| Mental composite summary (MCS) | 47.2 ± 10.9 | 44.1 ± 7.9 | 40.2 ± 6.5 | 0.078 |
| Baseline–after treatment | 3.35 ± 5.06 * | −0.18 ± 2.49 | 0.61 ± 2.48 | 0.415 |
| Baseline–12-week follow-up | −1.98 ± 5.18 | 0.27 ± 3.64 | −0.46 ± 2.40 | 0.228 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia de Carvalho, M.; Nunes de Azevedo, J.; Azevedo, P.; Pires, C.; Machado, J.P.; Laranjeira, M. Effectiveness of Acupuncture on Health-Related Quality of Life in Patients Receiving Maintenance Hemodialysis. Healthcare 2023, 11, 1355. https://doi.org/10.3390/healthcare11091355
Correia de Carvalho M, Nunes de Azevedo J, Azevedo P, Pires C, Machado JP, Laranjeira M. Effectiveness of Acupuncture on Health-Related Quality of Life in Patients Receiving Maintenance Hemodialysis. Healthcare. 2023; 11(9):1355. https://doi.org/10.3390/healthcare11091355
Chicago/Turabian StyleCorreia de Carvalho, Marta, José Nunes de Azevedo, Pedro Azevedo, Carlos Pires, Jorge Pereira Machado, and Manuel Laranjeira. 2023. "Effectiveness of Acupuncture on Health-Related Quality of Life in Patients Receiving Maintenance Hemodialysis" Healthcare 11, no. 9: 1355. https://doi.org/10.3390/healthcare11091355