

Medical Professional Liability in Obstetrics and Gynecology: A Pilot Study of Criminal Proceedings in the Public Prosecutor’s Office at the Court of Rome
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
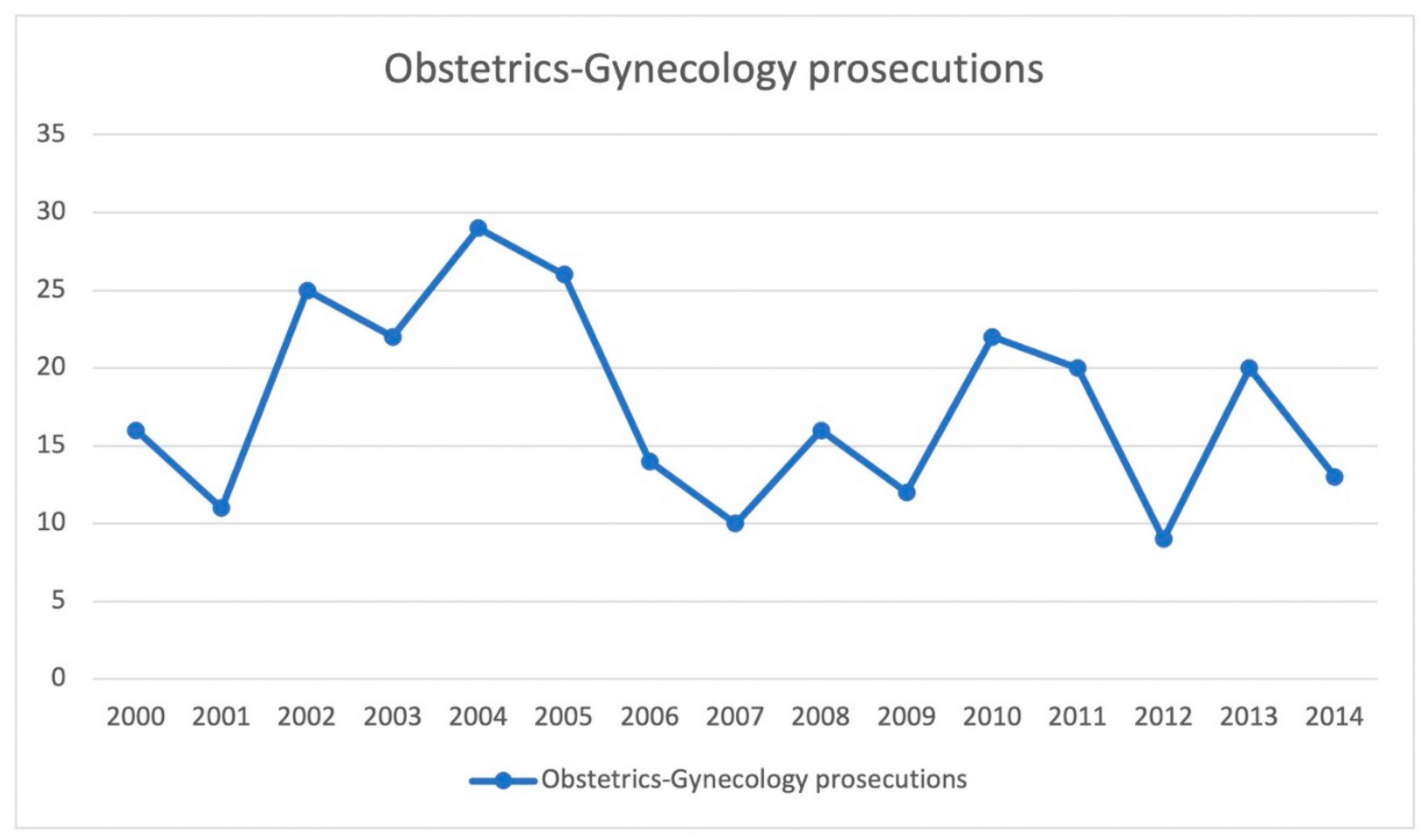
- The trend of medical professional liability prosecutions in the field of Ob-Gyn in Rome, from 2000 to 2014;
- The types of crimes that were prosecuted;
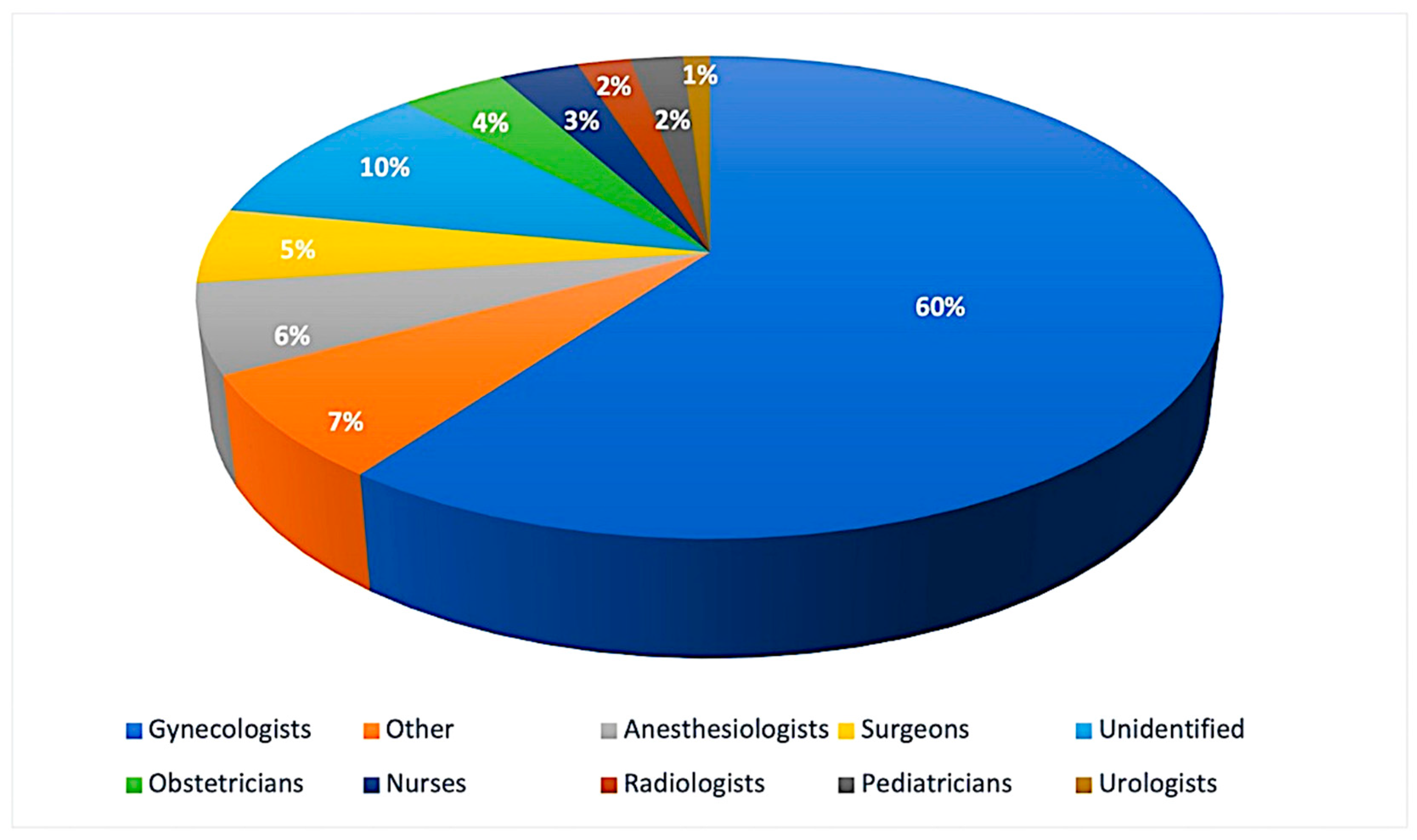
- The numbers, genders and categories of involved professionals;
- The number of professionals for whom dismissal was requested;
- The number of professionals for whom the motion to dismiss was opposed;
- The number of professionals for whom the motion to dismiss was granted;
- The number of professionals for whom an indictment or direct subpoena was requested (and granted);
- The number of proceedings that were resolved with a conviction verdict;
- The number of proceedings that were resolved with an acquittal verdict.
- The number of proceedings in which a court-appointed expert witness provided technical advice and the consultants’ credentials;
- The time elapsed between the assignment and the filing of the technical consultancy;
- The number of cases in which expert witnesses demonstrated that professional behavior was causally related to the event;
- The outcome of proceedings in which no culpable behavior was found;
- The outcome of proceedings in which culpable behavior was proven;
- The number of criminal proceedings in which court-appointed technical consultants were required to provide clarifications and/or additions;
- The outcome of clarifications and/or additions;
- The number of proceedings for which a technical consultant was appointed by the party, as well as the consultants’ credentials;
- The number of proceedings involving Obstetrics and associated topics;
- The number of proceedings involving Gynecology and associated topics;
- The nature of the convictions;
- The type of healthcare facility involved;
- The role of involved professionals (university or hospital employees, freelance workers).
3. Results
4. Discussion
- In Scandinavian countries, a system for managing the consequences of adverse events known as the “no-fault compensation system” has been promoted, which provides financial compensation for all those who demonstrate iatrogenic injury, regardless of the demonstration of censurable profiles of physicians’ behavior or structural deficiencies [29,30];
- The French judicial system is centered on Law 303 of 4 March 2002, which enshrines, in a nutshell, the obligation of compensation in connection to the risk associated with performance rather than the establishment of fault. The universality of the risk’s exposure and the ad hoc nature of the risk’s actual scope lead to a principle of solidarity that extends the obligation of compensation to the entire community. This is referred to as “socialization of risk”—if the liability of a professional, hospital, or healthcare institution cannot be demonstrated, the patient who is the victim of a medical accident may file a claim for damages as a form of national solidarity. However, the damage must be directly related to an act of prevention, diagnosis or treatment, and must exceed a minimum severity level determined by a specific decree;
- Furthermore, alternative out-of-court forms such as mediation, conciliation, and arbitration have been promoted in the international arena (United Nations, as well as some EU states: England, Austria, France, and Germany). In practice, it seeks to handle the conflict between doctor and patient using simple procedures that allow for a resolution in a short period of time and at a low cost, while avoiding the emotional and psychological stress associated with the process [31,32,33,34,35,36,37].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Knaak, J.P.; Parzeller, M. Court decisions on medical malpractice. Int. J. Leg. Med. 2014, 128, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, G.; Foti, F.; Grassi, V.M.; De-Giorgio, F.; Cambieri, A.; Ghisellini, R.; Clemente, F.; Marchese, L.; Sabatelli, G.; Delogu, G.; et al. Malpractice Claims and Incident Reporting: Two Faces of the Same Coin? Int. J. Environ. Res. Public Health 2022, 19, 16253. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, G.; De-Giorgio, F.; Foti, F. Everyone is affected, everyone a victim. BMJ 2019, 365, 12160. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, S.D. Errori, Percorso Unico Nell’UE. Available online: https://www.responsabilitasanitaria.it/pdf_articoli/Sole_24_Ore_Errori-PercorsoUnicoUe.pdf (accessed on 20 October 2022).
- Vetrugno, G.; Foti, F.; Spagnolo, A.; De-Giorgio, F. Reconciling patients’ need for compensation with doctors’ need for protection. BMJ 2019, 365, 11717. [Google Scholar] [CrossRef] [PubMed]
- ANIA. Available online: https://archivio.corriere.it/Archivio/interface/slider_pagine.html#!/11-12-2012/11-12-2012/NobwRAdghgtgpmAXGALnAziqWwBowCWAJkmAMIDyASgMoCiVAgnqnAB4qlkD2ATrwTi84AAiJwANhKgiaQqGAC+ucNHiki2BfgBmvbjFIBGIwHojAJlMWADJZYpuxs5et2LSlZFgJkAazgATwB3PhJ8NA5SJQBdIA (accessed on 20 October 2022).
- Becker, J.L.; Milad, M.P.; Klock, S.C. Burnout, depression, and career satisfaction: Cross-sectional study of obstetrics and gynecology residents. Am. J. Obstet. Gynecol. 2006, 195, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Kordel, P.; Kordel, K. Professional misconduct in obstetrics and gynecology in light of the Supreme Medical Court between 2002–2012. Ginekol. Pol. 2014, 85, 860–866. [Google Scholar] [CrossRef]
- Iverson, R.E., Jr.; Heffner, L.J. Patient safety series: Obstetric safety improvement and its reflection in reserved claims. Am. J. Obstet. Gynecol. 2011, 205, 398–401. [Google Scholar] [CrossRef]
- Chauhan, S.P.; Chauhan, V.B.; Cowan, B.D.; Hendrix, N.W.; Magann, E.F.; Morrison, J.C. Professional liability claims and Central Association of Obstetricians and Gynecologists members: Myth versus reality. Am. J. Obstet. Gynecol. 2005, 192, 1820–1826; discussion 1826–1828. [Google Scholar] [CrossRef]
- Wilson, N.; Strunk, A.L. District VI Liability Lowdown: Overview of the 2006 ACOG Survey on Professional Liability; Department of Professional Liability/Risk Management: Washington, DC, USA, 2006; Volume 1–3. [Google Scholar]
- Ferrara, S.D.; Baccino, E.; Bajanowski, T.; Boscolo-Berto, R.; Castellano, M.; De Angel, R.; Pauliukevičius, A.; Ricci, P.; Vanezis, P.; Vieira, D.N.; et al. Malpractice and medical liability. European Guidelines on Methods of Ascertainment and Criteria of Evaluation. Int. J. Leg. Med. 2013, 127, 545–557. [Google Scholar] [CrossRef]
- Cassano, G.; Cirillo, B. Casi di Responsabilità Medica; Maggioli Editore: Rimini, Italy, 2013. [Google Scholar]
- Blickstein, I. Litigation in multiple pregnancy and birth. Clin. Perinatol. 2007, 34, 319–327. [Google Scholar] [CrossRef]
- Boyaciyan, K.; Camano, L. Profile of denounced physicians that practice obstetrics and gynecology in the state of São Paulo. Rev. Assoc. Med. Bras. 2006, 52, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Shwayder, J.M. Liability in high-risk obstetrics. Obstet. Gynecol. Clin. N. Am. 2007, 34, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Smits, A.K.; Clark, E.C.; Nichols, M.; Saultz, J.W. Factors influencing cessation of pregnancy care in Oregon. Fam. Med. 2004, 36, 490–495. [Google Scholar] [PubMed]
- Clark, S.L.; Meyers, J.A.; Frye, D.R.; McManus, K.; Perlin, J.B. A systematic approach to the identification and classification of near-miss events on labor and delivery in a large, national health care system. Am. J. Obstet. Gynecol. 2012, 207, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Seubert, D.E.; Huang, W.M.; Wasserman-Hoff, R. Medical legal issues in the prevention of prematurity. Clin. Perinatol. 2007, 34, 309–318. [Google Scholar] [CrossRef]
- Cohen, W.R.; Schifrin, B.S. Medical negligence lawsuits relating to labor and delivery. Clin. Perinatol. 2007, 34, 345–360. [Google Scholar] [CrossRef]
- Johnson, S.L.; Blair, E.; Stanley, F.J. Obstetric malpractice litigation and cerebral palsy in term infants. J. Forensic Leg. Med. 2011, 18, 97–100. [Google Scholar] [CrossRef]
- Grimaldi, L.; De Giorgio, F.; Andreotta, P.; D’Alessio, M.C.; Piscicelli, C.; Pascali, V.L. Medicolegal aspects of an unusual uterine perforation with multiload-Cu 375R. Am. J. Forensic Med. Pathol. 2005, 26, 365–366. [Google Scholar] [CrossRef]
- Sanders, R.C. Changing patterns of ultrasound-related litigation: A historical survey. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2003, 22, 1009–1015. [Google Scholar] [CrossRef]
- Chervenak, F.A.; Chervenak, J.L. Medical legal issues in obstetric ultrasound. Clin. Perinatol. 2007, 34, 299–308. [Google Scholar] [CrossRef]
- Società Italiana di Ecografia Ostetrico Ginecologica. Ecografia di Screening in Ostetricia: Problematiche Medico-Legali; Editeam: Cento, Italy, 2009. [Google Scholar]
- Schifrin, B.S.; Cohen, W.R. Medical legal issues in fetal monitoring. Clin. Perinatol. 2007, 34, 329–343. [Google Scholar] [CrossRef] [PubMed]
- Asher, E.; Dvir, S.; Seidman, D.S.; Greenberg-Dotan, S.; Kedem, A.; Sheizaf, B.; Reuveni, H. Defensive medicine among obstetricians and gynecologists in tertiary hospitals. PLoS ONE 2013, 8, e57108. [Google Scholar] [CrossRef] [PubMed]
- Foti, F.; De-Giorgio, F.; Vetrugno, G. Let us learn from litigation claims: Actuarial tools can improve safety. BMJ 2021, 373, n1480. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, S.; Backe, B.; Jørstad, R.G.; Oian, P. A nationwide descriptive study of obstetric claims for compensation in Norway. Acta Obstet. Gynecol. Scand. 2012, 91, 1191–1195. [Google Scholar] [CrossRef] [PubMed]
- Milland, M.; Christoffersen, J.K.; Hedegaard, M. The size of the labor wards: Is bigger better when it comes to patient safety? Acta Obstet. Gynecol. Scand. 2013, 92, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Büken, E.; Ornek Büken, N.; Büken, B. Obstetric and gynecologic malpractice in Turkey: Incidence, impact, causes and prevention. J. Clin. Forensic Med. 2004, 11, 233–247. [Google Scholar] [CrossRef]
- Donlen, J.; Puro, J.S. The impact of the medical malpractice crisis on OB-GYNs and patients in southern New Jersey. N. J. Med. J. Med. Soc. N. J. 2003, 100, 12–19. [Google Scholar]
- Gómez-Durán, E.L.; Mulà-Rosías, J.A.; Lailla-Vicens, J.M.; Benet-Travé, J.; Arimany-Manso, J. Analysis of obstetrics and gynecology professional liability claims in Catalonia, Spain (1986–2010). J. Forensic Leg. Med. 2013, 20, 442–446. [Google Scholar] [CrossRef]
- Institute of Medicine Committee on Clinical Practice Guidelines. Guidelines for Clinical Practice: From Development to Use; Field, M.J., Lohr, K.N., Eds.; National Academies Press: Washington, DC, USA, 1992. [Google Scholar]
- Vetrugno, G.; Spagnolo, A.; De-Giorgio, F. Recession may decrease mortality trends. BMJ 2016, 354, i5165. [Google Scholar] [CrossRef]
- Xu, X.; Siefert, K.A.; Jacobson, P.D.; Lori, J.R.; Ransom, S.B. The effects of medical liability on obstetric care supply in Michigan. Am. J. Obstet. Gynecol. 2008, 198, 205.e1–205.e9. [Google Scholar] [CrossRef]
- Benedetti, T.J.; Baldwin, L.M.; Skillman, S.M.; Andrilla, C.H.; Bowditch, E.; Carr, K.C.; Myers, S.J. Professional liability issues and practice patterns of obstetric providers in Washington State. Obstet. Gynecol. 2006, 107, 1238–1246. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergamin, E.; Fiorillo, A.; Grassi, V.M.; Lodise, M.; Vetrugno, G.; De-Giorgio, F. Medical Professional Liability in Obstetrics and Gynecology: A Pilot Study of Criminal Proceedings in the Public Prosecutor’s Office at the Court of Rome. Healthcare 2023, 11, 1331. https://doi.org/10.3390/healthcare11091331
Bergamin E, Fiorillo A, Grassi VM, Lodise M, Vetrugno G, De-Giorgio F. Medical Professional Liability in Obstetrics and Gynecology: A Pilot Study of Criminal Proceedings in the Public Prosecutor’s Office at the Court of Rome. Healthcare. 2023; 11(9):1331. https://doi.org/10.3390/healthcare11091331
Chicago/Turabian StyleBergamin, Eva, Annamaria Fiorillo, Vincenzo M. Grassi, Maria Lodise, Giuseppe Vetrugno, and Fabio De-Giorgio. 2023. "Medical Professional Liability in Obstetrics and Gynecology: A Pilot Study of Criminal Proceedings in the Public Prosecutor’s Office at the Court of Rome" Healthcare 11, no. 9: 1331. https://doi.org/10.3390/healthcare11091331