
Comparison of Frailty Criteria, Cognitive Function, Depressive and Insomnia Symptoms in Men with Localized and Advanced Prostate Cancer under Androgen Deprivation Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Frailty Syndrome Assessment
2.3. Geriatric Assessment
3. Results
3.1. Sociodemographic and Clinical Data
3.2. Evaluation of Frailty Syndrome
3.3. Relationship between Frailty Syndrome and Socio-Demographic and Clinical Variables
3.4. Relationship between Frailty Syndrome and Geriatric Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martinez-Amores Martinez, B.; Durán Poveda, M.; Sánchez Encinas, M.; Molina Villaverde, R. Actualización En Cáncer de Próstata. Medicine 2013, 11, 1578–1587. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Las Cifras del Cáncer en España 2022. Available online: https://seom.org/images/LAS_CIFRAS_DEL_CANCER_EN_ESPANA_2022.pdf (accessed on 25 April 2023).
- Teo, M.Y.; Rathkopf, D.E.; Kantoff, P. Treatment of Advanced Prostate Cancer. Annu. Rev. Med. 2019, 70, 479. [Google Scholar] [CrossRef] [PubMed]
- Desai, K.; McManus, J.M.; Sharifi, N. Hormonal Therapy for Prostate Cancer. Endocr. Rev. 2021, 42, 354. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Meng, X.; Chen, Y.; Leng, S.X.; Zhang, H. The Biology of Aging and Cancer: Frailty, Inflammation, and Immunity. Cancer J. 2017, 23, 201–205. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older AdultsEvidence for a Phenotype. J. Gerontol. Ser. A 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Robinson, T.N.; Walston, J.D.; Brummel, N.E.; Deiner, S.; Brown, C.H.; Kennedy, M.; Hurria, A. Frailty for Surgeons: Review of a National Institute on Aging Conference on Frailty for Specialists. J. Am. Coll. Surg. 2015, 221, 1083. [Google Scholar] [CrossRef] [Green Version]
- Mohile, S.G.; Xian, Y.; Dale, W.; Fisher, S.G.; Rodin, M.; Morrow, G.R.; Neugut, A.; Hall, W. Association of a Cancer Diagnosis With Vulnerability and Frailty in Older Medicare Beneficiaries. JNCI J. Natl. Cancer Inst. 2009, 101, 1206–1215. [Google Scholar] [CrossRef] [Green Version]
- Rescigno, P.; Maruzzo, M.; Rebuzzi, S.E.; Murianni, V.; Cinausero, M.; Lipari, H.; Fratino, L.; Gamba, T.; De Giorgi, U.; Caffo, O.; et al. Adherence to Oral Treatments in Older Patients with Advanced Prostate Cancer, the ADHERE Study: A Prospective Trial of the Meet-URO Network. Oncologist 2022, 27, e949. [Google Scholar] [CrossRef]
- Banna, G.L.; Urzia, V.; Benanti, C.; Pitrè, A.; Lipari, H.; Di Quattro, R.; De Giorgi, U.; Schepisi, G.; Basso, U.; Bimbatti, D.; et al. Adherence to Abiraterone or Enzalutamide in Elderly Metastatic Castration-Resistant Prostate Cancer. Support. Care Cancer 2020, 28, 4687–4695. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Stone, K.L.; Cauley, J.A.; Tracy, J.K.; Hochberg, M.C.; Rodondi, N.; Cawthon, P.M.; et al. Frailty and Risk of Falls, Fracture, and Mortality in Older Women: The Study of Osteoporotic Fractures. J. Gerontol. Ser. A 2007, 62, 744–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kojima, G. Frailty as a Predictor of Future Falls among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2015, 16, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G. Frailty as a Predictor of Disabilities among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2016, 39, 1897–1908. [Google Scholar] [CrossRef]
- Kojima, G.; Green, J. Frailty as a Predictor of Hospitalisation among Community-Dwelling Older People: A Systematic Review and Meta-Analysis. J. Epidemiol. Community Health 2016, 70, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Yan, C.H.; Coleman, C.; Nabulsi, N.A.; Chiu, B.C.H.; Ko, N.Y.; Hoskins, K.; Calip, G.S. Associations between Frailty and Cancer-Specific Mortality among Older Women with Breast Cancer. Breast Cancer Res. Treat. 2021, 189, 769–779. [Google Scholar] [CrossRef]
- Kamijo, Y.; Kanda, E.; Ishibashi, Y.; Yoshida, M. Sarcopenia and Frailty in PD: Impact on Mortality, Malnutrition, and Inflammation. Perit. Dial. Int. 2018, 38, 447–454. [Google Scholar] [CrossRef]
- He, D.; Li, J.; Li, Y.; Zhu, J.; Zhou, T.; Xu, Y.; Wu, Q.; Cheng, Z.; Chen, Q.; Liu, Z.; et al. Frailty Is Associated with the Progression of Prediabetes to Diabetes and Elevated Risks of Cardiovascular Disease and All-Cause Mortality in Individuals with Prediabetes and Diabetes: Evidence from Two Prospective Cohorts. Diabetes Res. Clin. Pract. 2022, 194, 110145. [Google Scholar] [CrossRef]
- Jespersen, E.; Winther, S.B.; Minet, L.R.; Möller, S.; Pfeiffer, P. Frailty Screening for Predicting Rapid Functional Decline, Rapid Progressive Disease, and Shorter Overall Survival in Older Patients with Gastrointestinal Cancer Receiving Palliative Chemotherapy—A Prospective, Clinical Study. J. Geriatr. Oncol. 2021, 12, 578–584. [Google Scholar] [CrossRef]
- Extermann, M.; Aapro, M.; Bernabei, R.; Cohen, H.J.; Droz, J.P.; Lichtman, S.; Mor, V.; Monfardini, S.; Repetto, L.; Sørbye, L.; et al. Use of Comprehensive Geriatric Assessment in Older Cancer Patients:: Recommendations from the Task Force on CGA of the International Society of Geriatric Oncology (SIOG). Crit. Rev. Oncol. Hematol. 2005, 55, 241–252. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.G.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595. [Google Scholar] [CrossRef] [Green Version]
- Hurria, A. We Need a Geriatric Assessment for Oncologists. Nat. Clin. Pract. Oncol. 2006, 3, 642–643. [Google Scholar] [CrossRef] [PubMed]
- Kenis, C.; Bron, D.; Libert, Y.; Decoster, L.; Van Puyvelde, K.; Scalliet, P.; Cornette, P.; Pepersack, T.; Luce, S.; Langenaeken, C.; et al. Relevance of a Systematic Geriatric Screening and Assessment in Older Patients with Cancer: Results of a Prospective Multicentric Study. Ann. Oncol. 2013, 24, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.D.L.; Tajar, A.; Roberts, S.A.; Wu, F.C.W. Do Androgens Play Any Role in the Physical Frailty of Ageing Men? Int. J. Androl. 2011, 34, 195–211. [Google Scholar] [CrossRef]
- Gooren, L. Frailty and Its Relationship to Late Onset Hypogonadism. J. Men’s Health Gend. 2007, 4, 466–473. [Google Scholar] [CrossRef]
- Saad, F.; Röhrig, G.; Von Haehling, S.; Traish, A. Testosterone Deficiency and Testosterone Treatment in Older Men. Gerontology 2017, 63, 144–156. [Google Scholar] [CrossRef]
- Mafla-España, M.A.; Torregrosa, M.D.; Cauli, O. Analysis of Frailty Syndrome in Men with Metastatic Prostate Cancer: A Scoping Review. J. Pers. Med. 2023, 13, 319. [Google Scholar] [CrossRef]
- Zitzmann, M. Testosterone, Mood, Behaviour and Quality of Life. Andrology 2020, 8, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Seidman, S.N. Normative Hypogonadism and Depression: Does “andropause” Exist? Int. J. Impot. Res. 2006, 18, 415–422. [Google Scholar] [CrossRef]
- Walia, A.S.; de Lomeli, L.J.M.; Jiang, P.; Benca, R.; Yafi, F.A. Patients Presenting to a Men’s Health Clinic Are at Higher Risk for Depression, Insomnia, and Sleep Apnea. Int. J. Impot. Res. 2019, 31, 39–45. [Google Scholar] [CrossRef]
- Seidman, S.N.; Weiser, M. Testosterone and Mood in Aging Men. Psychiatr. Clin. N. Am. 2013, 36, 177–182. [Google Scholar] [CrossRef]
- Nowakowska, M.K.; Lei, X.; Wehner, M.R.; Corn, P.G.; Giordano, S.H.; Nead, K.T. Association of Second-Generation Antiandrogens with Depression among Patients with Prostate Cancer. JAMA Netw. Open 2021, 4, e2140803. [Google Scholar] [CrossRef] [PubMed]
- Batra, A.; Marchioni, M.; Hashmi, A.Z.; Lonergan, P.E.; Morgans, A.K.; Nead, K.T.; Nguyen, P.L.; Winquist, E.; Chin, J.L. Cognition and Depression Effects of Androgen Receptor Axis-Targeted Drugs in Men with Prostate Cancer: A Systematic Review. J. Geriatr. Oncol. 2021, 12, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Mondal, S.; Edwards, S.; Wibowo, E.; Ahmed, H.; Wassersug, R.J.; Ellis, J.; Isaac, M.; Dimitriou, D.; Mangar, S. Evaluating Patterns and Factors Related to Sleep Disturbances in Prostate Cancer Patients. Healthcare 2022, 10, 832. [Google Scholar] [CrossRef]
- Revalidación, L.A. Normalizacion Del Mini-Examen Cognoscitivo (Primera Version En Castellano Del Mini-Mental Status Examination) En La Poblacion General Geriatrica. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an Instrument Based on ICD-10 Criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Gómez-Benito, J.; Ruiz, C.; Guilera, G. A Spanish Version of the Athens Insomnia Scale. Qual. Life Res. 2011, 20, 931–937. [Google Scholar] [CrossRef] [Green Version]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and Validation of a Geriatric Depression Screening Scale: A Preliminary Report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Martínez de la Iglesia, J.; Onís Vilches, M.; Aguado Taberné, C.; Dueñas Herrero, R.; Albert Colomer, C.; Luque Luque, R. Versión Española Del Cuestionario de Yesavage Abreviado (GDS) Para El Despistaje de Depresión En Mayores de 65 Años: Adaptación y Validación. Medifam 2002, 12, 620–630. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Hamaya, T.; Hatakeyama, S.; Momota, M.; Narita, T.; Iwamura, H.; Kojima, Y.; Hamano, I.; Fujita, N.; Okamoto, T.; Togashi, K.; et al. Association between the Baseline Frailty and Quality of Life in Patients with Prostate Cancer (FRAQ-PC Study). Int. J. Clin. Oncol. 2021, 26, 199–206. [Google Scholar] [CrossRef]
- Momota, M.; Hatakeyama, S.; Soma, O.; Tanaka, T.; Hamano, I.; Fujita, N.; Okamoto, T.; Yoneyama, T.; Yamamoto, H.; Imai, A.; et al. Geriatric 8 Screening of Frailty in Patients with Prostate Cancer. Int. J. Urol. 2020, 27, 642–648. [Google Scholar] [CrossRef]
- Handforth, C.; Burkinshaw, R.; Freeman, J.; Brown, J.E.; Snowden, J.A.; Coleman, R.E.; Greenfield, D.M. Comprehensive Geriatric Assessment and Decision-Making in Older Men with Incurable but Manageable (Chronic) Cancer. Support. Care Cancer 2019, 27, 1755–1763. [Google Scholar] [CrossRef] [PubMed]
- Della Pepa, C.; Cavaliere, C.; Rossetti, S.; Di Napoli, M.; Cecere, S.C.; Crispo, A.; De Sangro, C.; Rossi, E.; Turitto, D.; Germano, D.; et al. Predictive Comprehensive Geriatric Assessment in Elderly Prostate Cancer Patients: The Prospective Observational Scoop Trial Results. Anticancer Drugs 2017, 28, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, H.M.; Llaniguez, J.T.; Telemi, E.; Chuang, M.; Abouelleil, M.; Wilkinson, B.; Chandra, A.; Boyce-Fappiano, D.; Elibe, E.; Schultz, L.; et al. Sarcopenia Predicts Overall Survival in Patients with Lung, Breast, Prostate, or Myeloma Spine Metastases Undergoing Stereotactic Body Radiation Therapy (SBRT), Independent of Histology. Neurosurgery 2020, 86, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martínez, R.; Serrano-Carrascosa, M.; Buigues, C.; Fernández-Garrido, J.; Sánchez-Martínez, V.; Castelló-Domenech, A.B.; García-Villodre, L.; Wong-Gutiérrez, A.; Rubio-Briones, J.; Cauli, O. Frailty Syndrome Is Associated with Changes in Peripheral Inflammatory Markers in Prostate Cancer Patients Undergoing Androgen Deprivation Therapy. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Buigues, C.; Navarro-Martínez, R.; Sánchez-Martínez, V.; Serrano-Carrascosa, M.; Rubio-Briones, J.; Cauli, O. Interleukin-6 and Lymphocyte Count Associated and Predicted the Progression of Frailty Syndrome in Prostate Cancer Patients Undergoing Antiandrogen Therapy. Cancers 2020, 12, 1716. [Google Scholar] [CrossRef]
- Kaufman, J.M.; Vermeulen, A. The Decline of Androgen Levels in Elderly Men and Its Clinical and Therapeutic Implications. Endocr. Rev. 2005, 26, 833–876. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Ensrud, K.E.; Laughlin, G.A.; Cauley, J.A.; Dam, T.T.L.; Barrett-Connor, E.; Fink, H.A.; Hoffman, A.R.; Lau, E.; Lane, N.E.; et al. Sex Hormones and Frailty in Older Men: The Osteoporotic Fractures in Men (MrOS) Study. J. Clin. Endocrinol. Metab. 2009, 94, 3806–3815. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and Pre-Frailty in Middle-Aged and Older Adults and Its Association with Multimorbidity and Mortality: A Prospective Analysis of 493 737 UK Biobank Participants. Lancet Public Health 2018, 3, e323. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, C.S.; Kvale, E.; Fisch, M.J. Multimorbidity: An Issue of Growing Importance for Oncologists. J. Oncol. Pract. 2011, 7, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Kodama, H.; Hatakeyama, S.; Momota, M.; Togashi, K.; Hamaya, T.; Hamano, I.; Fujita, N.; Kojima, Y.; Okamoto, T.; Yoneyama, T.; et al. Effect of Frailty and Comorbidity on Surgical Contraindication in Patients with Localized Prostate Cancer (FRART-PC Study). Urol. Oncol. Semin. Orig. Investig. 2021, 39, 191.e1–191.e8. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.J.H.; Pahor, M.; Lauretani, F.; Corsi, A.M.; Williams, G.R.; Guralnik, J.M.; Ferrucci, L. Inflammatory Markers and Physical Performance in Older Persons: The InCHIANTI Study. J. Gerontol. Ser. A 2004, 59, M242–M248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, G.R.; Rier, H.N.; McDonald, A.; Shachar, S.S. Sarcopenia & Aging in Cancer. J. Geriatr. Oncol. 2019, 10, 374. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European Consensus on Definition and DiagnosisReport of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Williams, G.R.; Chen, Y.; Kenzik, K.M.; McDonald, A.; Shachar, S.S.; Klepin, H.D.; Kritchevsky, S.; Bhatia, S. Assessment of Sarcopenia Measures, Survival, and Disability in Older Adults before and after Diagnosis with Cancer. JAMA Netw. Open 2020, 3, e204783. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, K.; Tuffaha, H.; Galvão, D.A.; Scuffham, P.; Newton, R.U. Incidence of the Adverse Effects of Androgen Deprivation Therapy for Prostate Cancer: A Systematic Literature Review. Support. Care Cancer 2020, 28, 2079–2093. [Google Scholar] [CrossRef] [Green Version]
- Soyupek, F.; Soyupek, S.; Perk, H.; Özorak, A. Androgen Deprivation Therapy for Prostate Cancer: Effects on Hand Function. Urol. Oncol. Semin. Orig. Investig. 2008, 26, 141–146. [Google Scholar] [CrossRef]
- Basaria, S.; Lieb, J.; Tang, A.M.; DeWeese, T.; Carducci, M.; Eisenberger, M.; Dobs, A.S. Long-Term Effects of Androgen Deprivation Therapy in Prostate Cancer Patients. Clin. Endocrinol. 2002, 56, 779–786. [Google Scholar] [CrossRef]
- Hong, S.; Youk, T.; Lee, S.J.; Kim, K.M.; Vajdic, C.M. Bone Metastasis and Skeletal-Related Events in Patients with Solid Cancer: A Korean Nationwide Health Insurance Database Study. PLoS ONE 2020, 15, e0234927. [Google Scholar] [CrossRef]
- Pamoukdjian, F.; Paillaud, E.; Zelek, L.; Laurent, M.; Lévy, V.; Landre, T.; Sebbane, G. Measurement of Gait Speed in Older Adults to Identify Complications Associated with Frailty: A Systematic Review. J. Geriatr. Oncol. 2015, 6, 484–496. [Google Scholar] [CrossRef]
- Abellan Van Kan, G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait Speed at Usual Pace as a Predictor of Adverse Outcomes in Community-Dwelling Older People an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; et al. Sarcopenia: Prevalence, Associated Factors, and the Risk of Mortality and Disability in Japanese Older Adults. J. Cachexia Sarcopenia Muscle 2021, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Bylow, K.; Mohile, S.G.; Stadler, W.M.; Dale, W. Does Androgen-Deprivation Therapy Accelerate the Development of Frailty in Older Men with Prostate Cancer?: A Conceptual Review. Cancer 2007, 110, 2604–2613. [Google Scholar] [CrossRef]
- Villareal, D.T.; Banks, M.; Siener, C.; Sinacore, D.R.; Klein, S. Physical Frailty and Body Composition in Obese Elderly Men and Women. Obes. Res. 2004, 12, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Blaum, C.S.; Xue, Q.L.; Michelon, E.; Semba, R.D.; Fried, L.P. The Association between Obesity and the Frailty Syndrome in Older Women: The Women’s Health and Aging Studies. J. Am. Geriatr. Soc. 2005, 53, 927–934. [Google Scholar] [CrossRef]
- Bylow, K.; Hemmerich, J.; Mohile, S.G.; Stadler, W.M.; Sajid, S.; Dale, W. Obese Frailty, Physical Performance Deficits, and Falls in Older Men with Biochemical Recurrence of Prostate Cancer on Androgen Deprivation Therapy: A Case-Control Study. Urology 2011, 77, 934. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, B.D.; Small, B.J.; Cases, M.G.; Williams, N.L.; Fishman, M.N.; Jacobsen, P.B.; Jim, H.S.L. Sleep Disturbance in Men Receiving Androgen Deprivation Therapy for Prostate Cancer: The Role of Hot Flashes and Nocturia. Cancer 2018, 124, 499–506. [Google Scholar] [CrossRef]
- Savard, J.; Simard, S.; Hervouet, S.; Ivers, H.; Lacombe, L.; Fradet, Y. Insomnia in Men Treated with Radical Prostatectomy for Prostate Cancer. Psychooncology 2005, 14, 147–156. [Google Scholar] [CrossRef]
- Gillessen, S.; Attard, G.; Beer, T.M.; Beltran, H.; Bjartell, A.; Bossi, A.; Briganti, A.; Bristow, R.G.; Chi, K.N.; Clarke, N.; et al. Management of Patients with Advanced Prostate Cancer: Report of the Advanced Prostate Cancer Consensus Conference 2019. Eur. Urol. 2020, 77, 508–547. [Google Scholar] [CrossRef]
- Savard, J.; Morin, C.M. Insomnia in the Context of Cancer: A Review of a Neglected Problem. J. Clin. Oncol. 2001, 19, 895–908. [Google Scholar] [CrossRef]
- Galvão, D.A.; Taaffe, D.R.; Spry, N.; Cormie, P.; Joseph, D.; Chambers, S.K.; Chee, R.; Peddle-Mcintyre, C.J.; Hart, N.H.; Baumann, F.T.; et al. Exercise Preserves Physical Function in Prostate Cancer Patients with Bone Metastases. Med. Sci. Sport. Exerc. 2018, 50, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvão, D.A.; Spry, N.; Denham, J.; Taaffe, D.R.; Cormie, P.; Joseph, D.; Lamb, D.S.; Chambers, S.K.; Newton, R.U. A Multicentre Year-Long Randomised Controlled Trial of Exercise Training Targeting Physical Functioning in Men with Prostate Cancer Previously Treated with Androgen Suppression and Radiation from TROG 03.04 RADAR. Eur. Urol. 2014, 65, 856–864. [Google Scholar] [CrossRef] [PubMed]
- Sheill, G.; Guinan, E.; Neill, L.O.; Hevey, D.; Hussey, J. The Views of Patients with Metastatic Prostate Cancer towards Physical Activity: A Qualitative Exploration. Support. Care Cancer 2018, 26, 1747–1754. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency % (Categorical Variables) or Mean ± Standard Error of the Mean (Range Min–Max) (Discrete Variables) | mPCa Patients (N = 27) | PCa Localized (N = 36) | p Value |
|---|---|---|---|---|
| Previous prostatectomy | 0.36 | |||
| Yes | 38 (61.9%) | Yes (51.9%) | Yes (66.7%) | |
| No | 25 (38.1%) | No (48.1%) | No (33.3%) | |
| BMI (kg/m2) | 0.22 | |||
| Underweight (<18.5) | 0 | |||
| Normal (18.5–24.9) | 15 (23.8%) | 9 (32.1%) | 6 (16.6%) | |
| Overweight (25–29.9) | 34 (54%) | 14 (51.8%) | 20 (55.5%) | |
| Obese (>30) | 14 (22.2%) | 4 (14.8%) | 10 (27.6%) | |
| Abdominal perimeter | 0.65 | |||
| <102 cm | 26 (41.3%) | 12 (44.4%) | 14 (38.8%) | |
| ≥102 cm | 37 (58.7%) | 15 (55.5%) | 22 (61.1%) | |
| Age | 73.6 ± 1.18 (51–92) | 75 ± 1.6 | 72.9 ± 1.6 | 0.42 |
| Gleason Index | 7.30 ± 0.14 (5–10) | 7.5 ± 0.25 | 7.1 ± 0.17 | 0.21 |
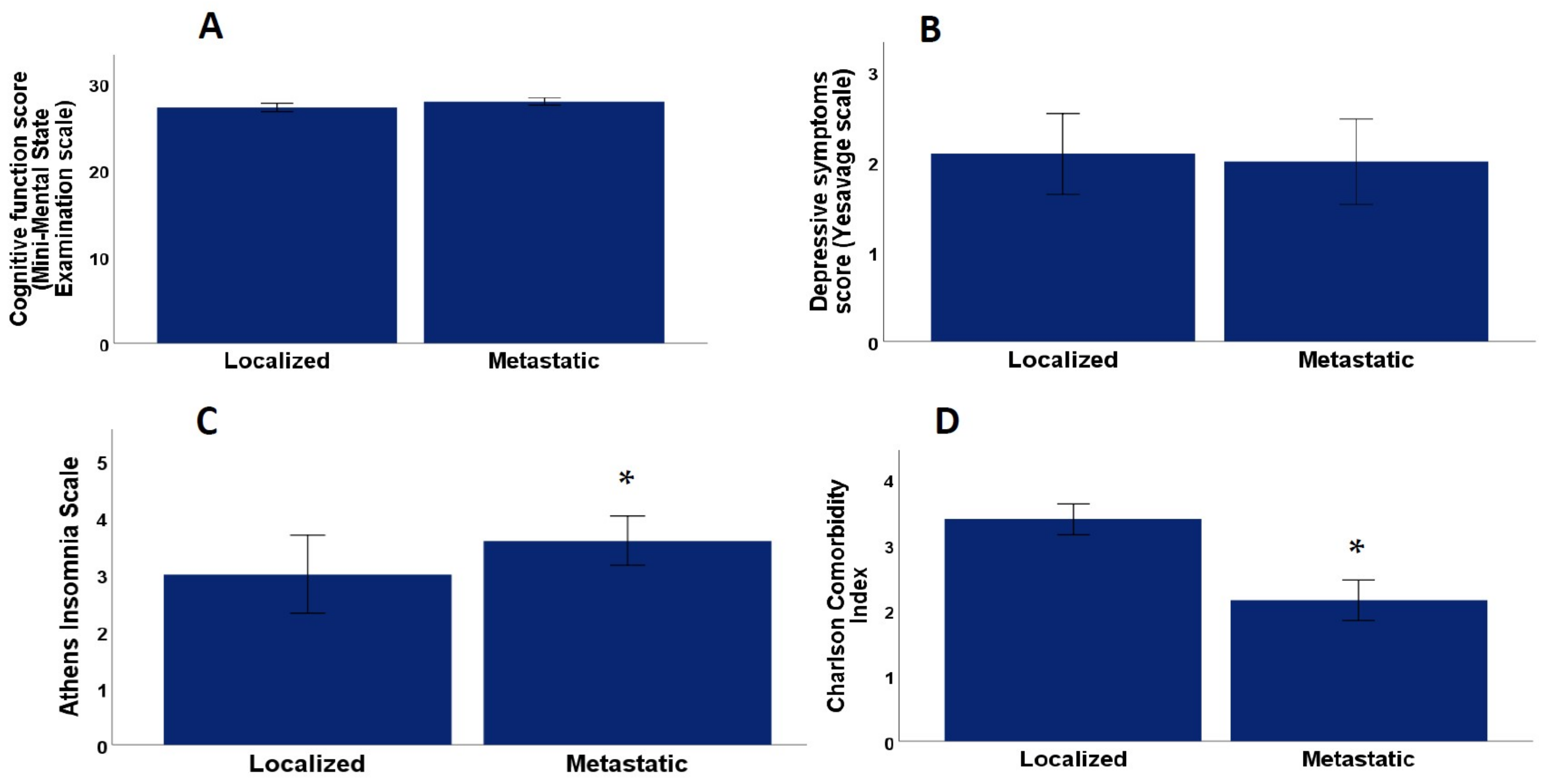
| Charlson Comorbidity Index | 2.87 ± 0.20 (0–7) | 2.6 ± 0.29 | 3.3 ± 0.23 | 0.02 |
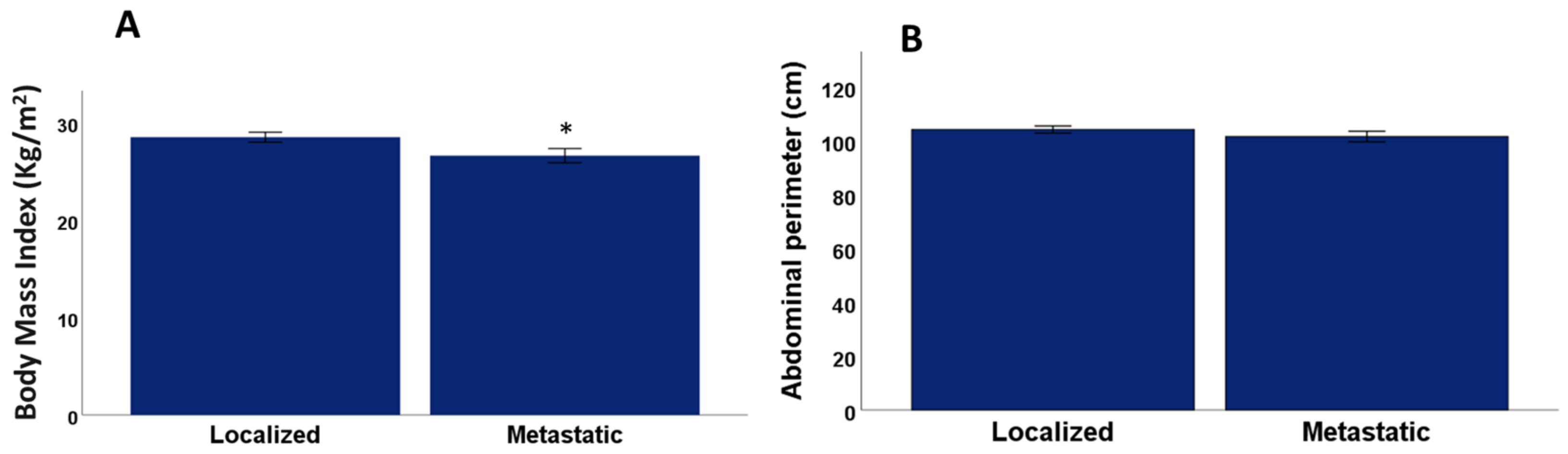
| Body mass index | 27.6 ± 0.42 (19.6–34.5) | 26.6 ± 0.73 | 28.5 ± 0.51 | 0.01 |
| Abdominal perimeter | 102.8 ± 1.08 (84–125) | 101.8 ± 2.0 | 104.3 ± 1.33 | 0.28 |
| Criteria of frailty syndrome | 0.57 | |||
| Robust (0 criteria) | 15 (23.8%) | 5 (18.5%) | 10 (27.7%) | |
| Pre-frail (1–2 criteria) | 38 (60.3%) | 17 (63%) | 22 (58.3%) | |
| Frail (>3 criteria) | 10 (15.9%) | 5 (18.5%) | 5 (13.8) | |
| Number of Fried criteria | 1.46 ± 0.13 (0–4) | 1.55 ± 0.20 (0–4) | 1.38 ± 0.18 (0–4) | 0.78 |
| Prevalence of prefrailty plus frailty | 76.20% | 81.50% | 72.30% | 0.76 |
| Athens Scale | 3.26 ± 0.43 (0–17) | 3.59 ± 0.43 | 3.0 ± 0.69 | 0.02 |
| MMSE Scale | 27.5 ± 0.34 (16–30) | 27.81 ± 0.43 | 27.2 ± 0.50 | 0.42 |
| Yesavage Scale | 2.05 ± 0.32 (0–14) | 2.0 ± 0.47 | 2.09 ± 0.44 | 0.67 |
| Health Perception Scale | 7.51 ± 0.20 (2–10) | 7.70 ± 0.32 | 7.37 ± 0.26 | 0.43 |
| Prevalence % | p Value for the Comparison between Metastatic and Localized PCa | |
|---|---|---|
| 1. Frailty criterion: involuntary weight loss | Yes 22 (34.9%) | 0.76 |
| No 41 (65.1%) | ||
| 2. Frailty criterion: weakness | Yes 17 (27%) | 0.11 |
| No 46 (73%) | ||
| 3. Frailty criterion: low physical activity | Yes 28 (44.4%) | 0.11 |
| No 35 (55.6%) | ||
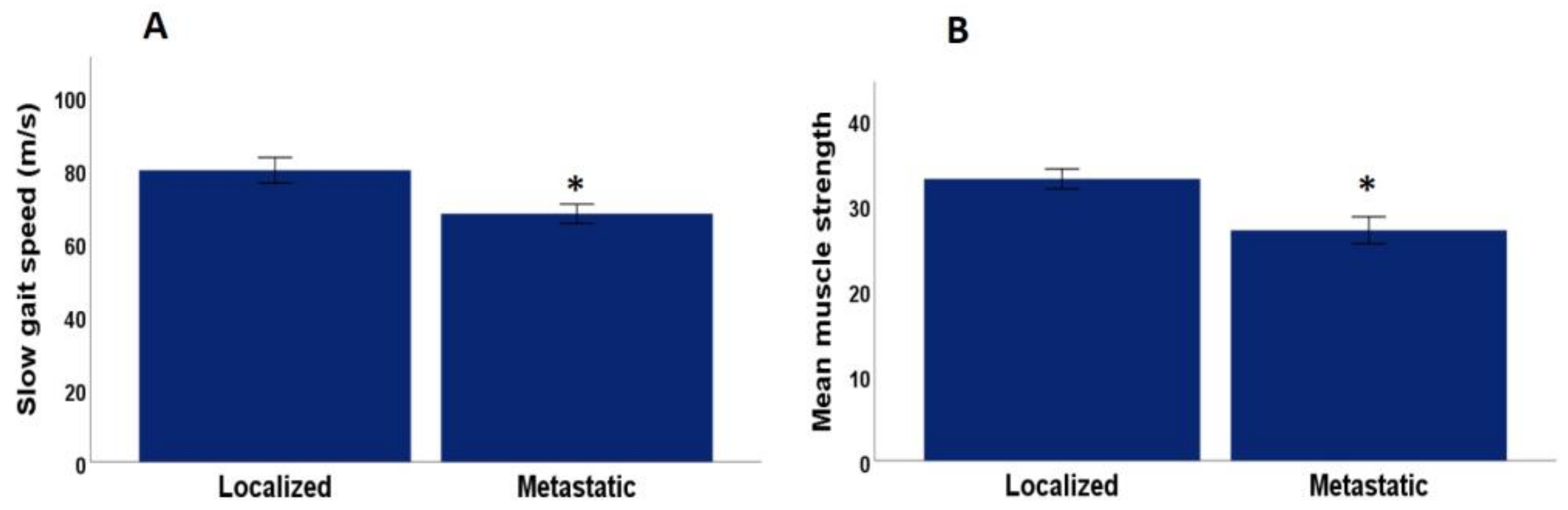
| 4. Frailty criterion: slow gait speed | Yes 19 (31.1%) | 0.001 |
| No 42 (68.9%) | ||
| 5. Frailty criterion: low muscle strength | Yes 5 (7.9%) | 0.04 |
| No 58 (92.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mafla-España, M.A.; Torregrosa, M.D.; Beamud-Cortés, M.; Bermell-Marco, L.; Rubio-Briones, J.; Cauli, O. Comparison of Frailty Criteria, Cognitive Function, Depressive and Insomnia Symptoms in Men with Localized and Advanced Prostate Cancer under Androgen Deprivation Therapy. Healthcare 2023, 11, 1266. https://doi.org/10.3390/healthcare11091266
Mafla-España MA, Torregrosa MD, Beamud-Cortés M, Bermell-Marco L, Rubio-Briones J, Cauli O. Comparison of Frailty Criteria, Cognitive Function, Depressive and Insomnia Symptoms in Men with Localized and Advanced Prostate Cancer under Androgen Deprivation Therapy. Healthcare. 2023; 11(9):1266. https://doi.org/10.3390/healthcare11091266
Chicago/Turabian StyleMafla-España, Mayra Alejandra, María Dolores Torregrosa, Manel Beamud-Cortés, Lorena Bermell-Marco, José Rubio-Briones, and Omar Cauli. 2023. "Comparison of Frailty Criteria, Cognitive Function, Depressive and Insomnia Symptoms in Men with Localized and Advanced Prostate Cancer under Androgen Deprivation Therapy" Healthcare 11, no. 9: 1266. https://doi.org/10.3390/healthcare11091266