
Correction of Thoracic Hypokyphosis in Adolescent Scoliosis Using Patient-Specific Rod Templating

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Coronal Plane Correction
3.2. Sagittal Plane Correction Parameters
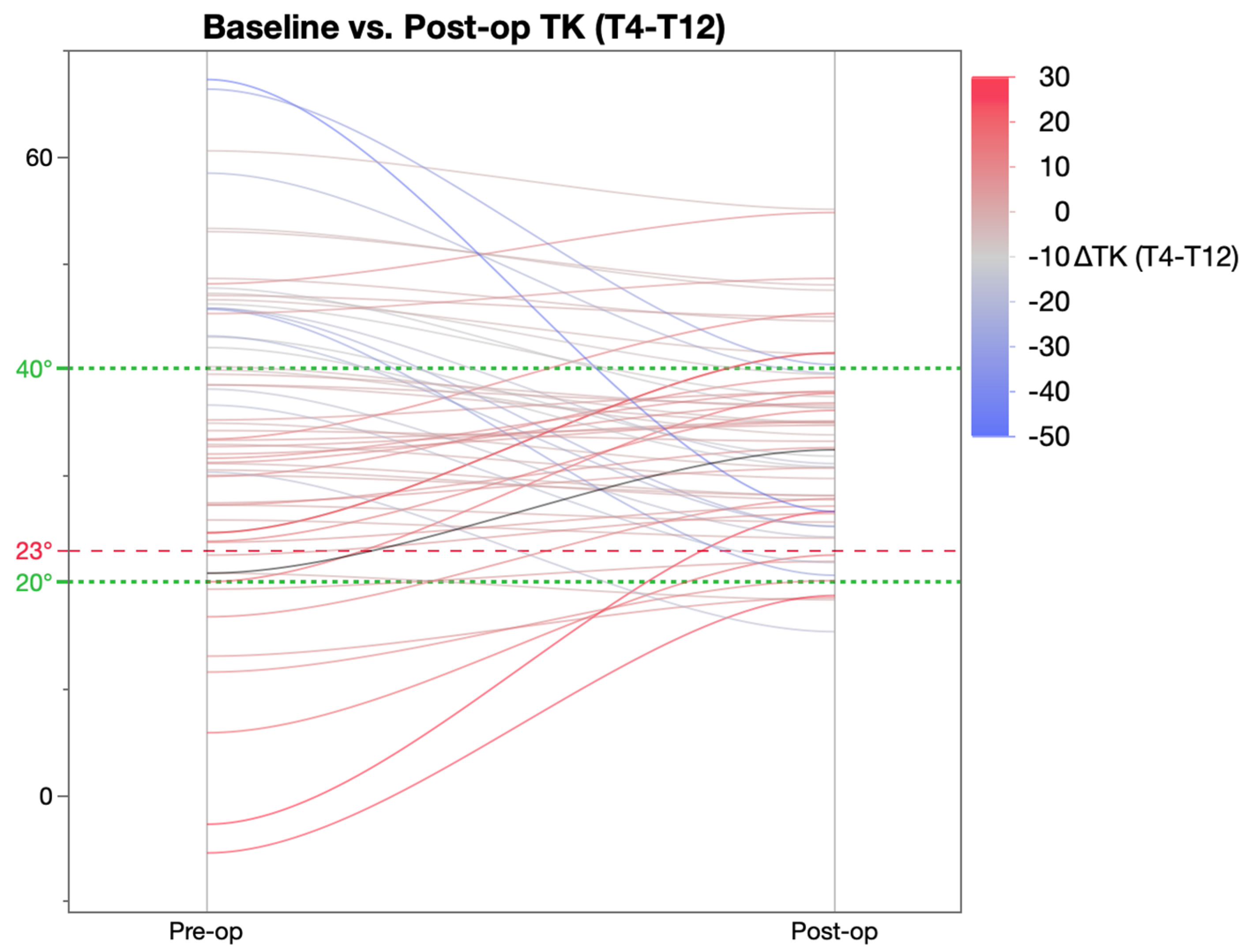
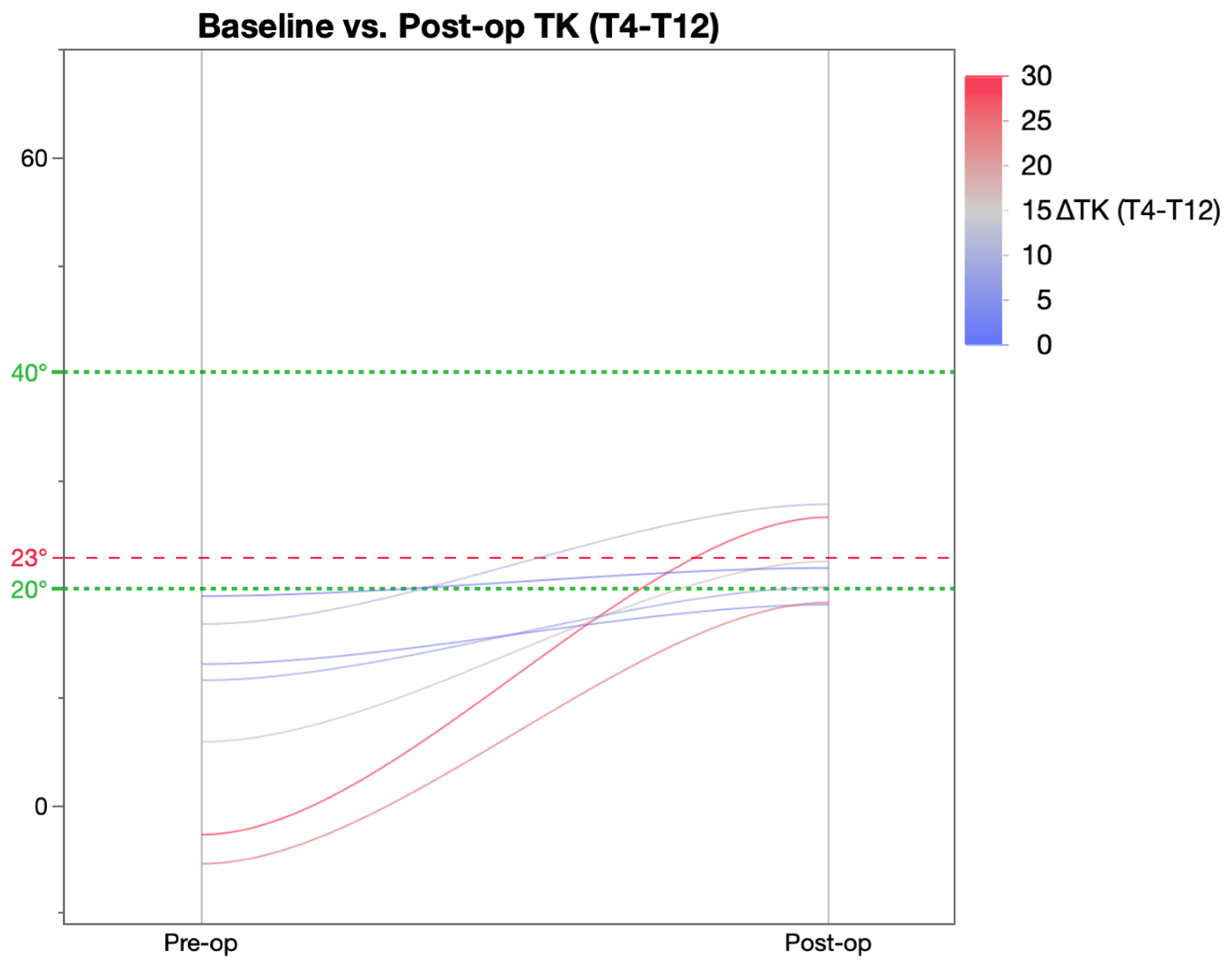
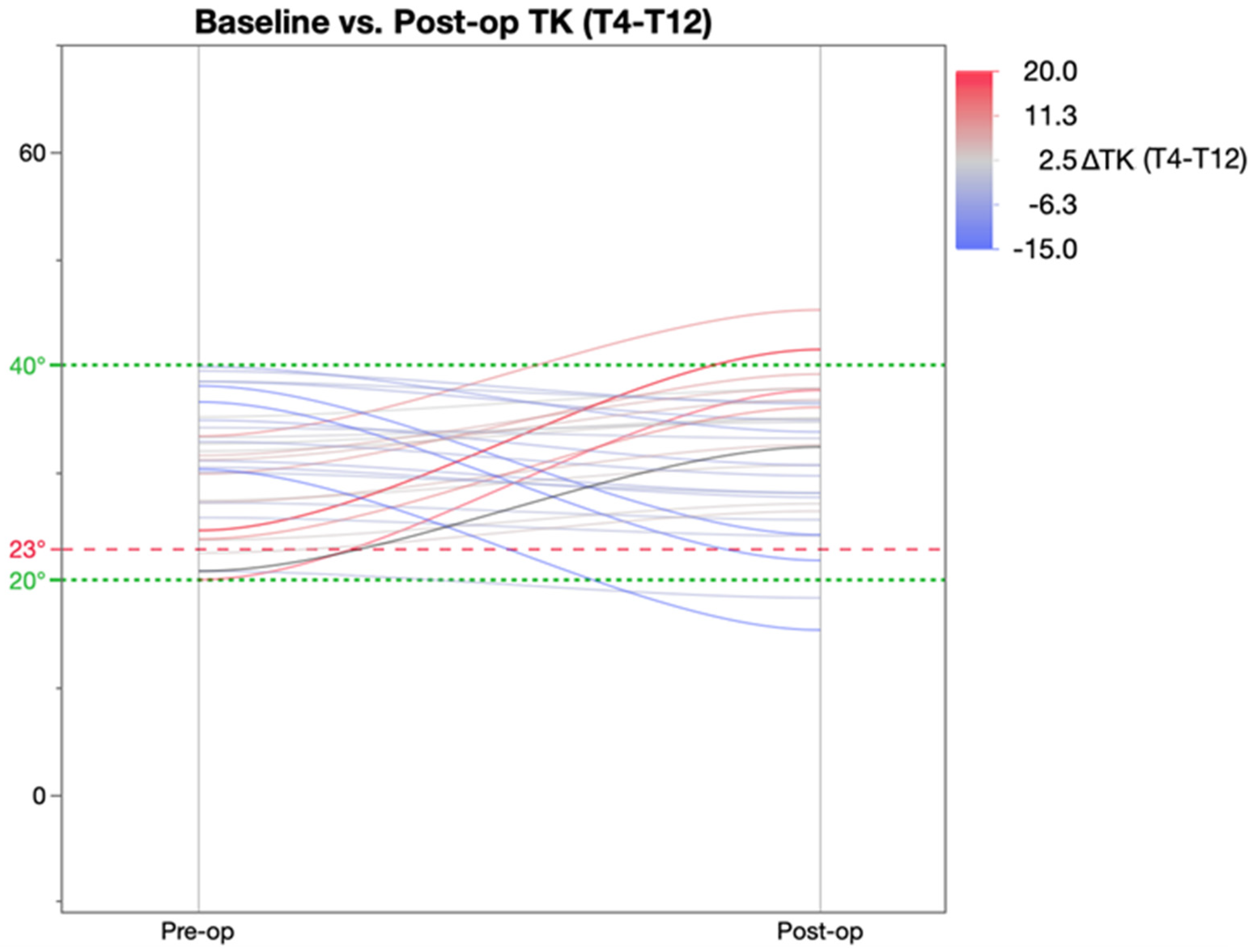
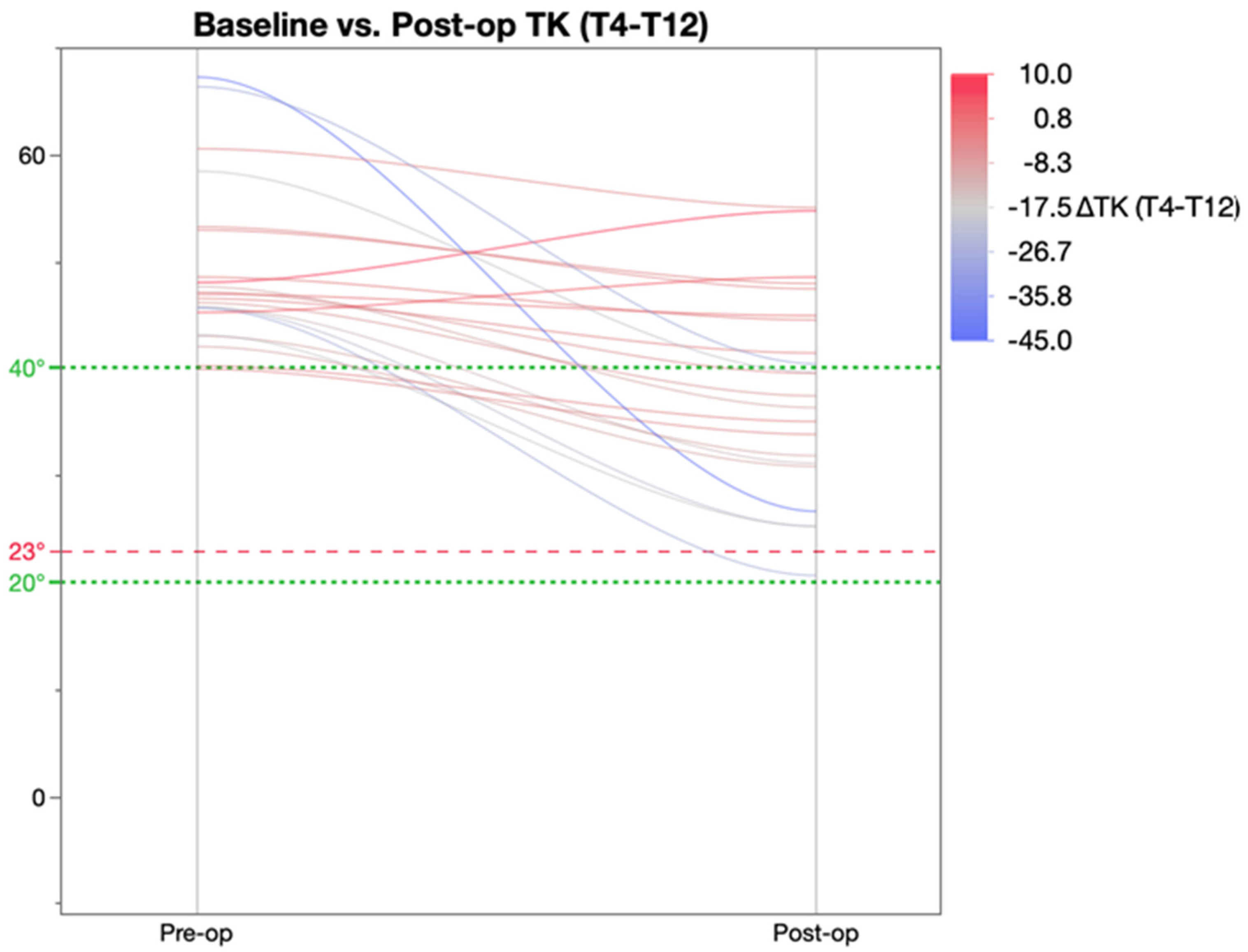
3.3. Comparison of TK Achieved with Templating
4. Discussion
- Implant density and implant choice: Higher screw density on the concave side with thicker and cobalt chrome rods have been associated with restoration of kyphosis to greater than 20 degrees [31]. Reduction in the implant density, however, also means the load exerted on each anchor is increased. One simulation study showed that the pull-out force exerted on the screw in the apical vertebra increased 2.5-fold when screw density decreased from 2.0 to 1.0 [32].
- Surgical correction technique: Dual differential rod contouring has been shown to achieve the best vertebral rotation [11,18]. Thoracic kyphosis is best restored through the dual rod posteromedial correction technique [33,34]. Manoeuvres such as simple rod roll and direct vertebral de-rotation have been found to worsen hypokyphosis as they are inherently lordogenic in nature [35,36].
- Restoring TK to a value of 20–40° regardless of pre-operative TK value.
- Post-operative TK achieved was within 5.5° of the value predicted using templating.
- Excellent coronal plane correction in addition to the correction of TK.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weinstein, S.L.; Dolan, L.A.; Cheng, J.C.Y.; Danielsson, A.; Morcuende, J.A. Adolescent Idiopathic Scoliosis. Lancet 2008, 371, 1527–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illés, T.; Tunyogi-Csapó, M.; Somoskeöy, S. Breakthrough in Three-Dimensional Scoliosis Diagnosis: Significance of Horizontal Plane View and Vertebra Vectors. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2011, 20, 135–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, P.O.; Yaszay, B.; Upasani, V.V.; Pawelek, J.B.; Bastrom, T.P.; Lenke, L.G.; Lowe, T.; Crawford, A.; Betz, R.; Lonner, B. Preservation of Thoracic Kyphosis Is Critical to Maintain Lumbar Lordosis in the Surgical Treatment of Adolescent Idiopathic Scoliosis. Spine 2010, 35, 1365–1370. [Google Scholar] [CrossRef] [PubMed]
- Majdouline, Y.; Aubin, C.-E.; Robitaille, M.; Sarwark, J.F.; Labelle, H. Scoliosis Correction Objectives in Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop. 2007, 27, 775–781. [Google Scholar] [CrossRef]
- Takayama, K.; Nakamura, H.; Matsuda, H. Low Back Pain in Patients Treated Surgically for Scoliosis: Longer than Sixteen-Year Follow-Up. Spine 2009, 34, 2198–2204. [Google Scholar] [CrossRef]
- Matsumoto, H.; Colacchio, N.D.; Schwab, F.J.; Lafage, V.; Roye, D.P.; Vitale, M.G. Flatback Revisited: Reciprocal Loss of Lumbar Lordosis Following Selective Thoracic Fusion in the Setting of Adolescent Idiopathic Scoliosis. Spine Deform. 2015, 3, 345–351. [Google Scholar] [CrossRef]
- Lonner, B.S.; Ren, Y.; Newton, P.O.; Shah, S.A.; Samdani, A.F.; Shufflebarger, H.L.; Asghar, J.; Sponseller, P.; Betz, R.R.; Yaszay, B. Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis—The Pelvis and Other Considerations. Spine Deform. 2017, 5, 181–188. [Google Scholar] [CrossRef]
- Ilharreborde, B. Sagittal Balance and Idiopathic Scoliosis: Does Final Sagittal Alignment Influence Outcomes, Degeneration Rate or Failure Rate? Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2018, 27, 48–58. [Google Scholar] [CrossRef]
- Winter, R.B.; Lovell, W.W.; Moe, J.H. Excessive Thoracic Lordosis and Loss of Pulmonary Function in Patients with Idiopathic Scoliosis. J. Bone Joint Surg. Am. 1975, 57, 972–977. [Google Scholar] [CrossRef]
- Hwang, S.W.; Samdani, A.F.; Tantorski, M.; Cahill, P.; Nydick, J.; Fine, A.; Betz, R.R.; Antonacci, M.D. Cervical Sagittal Plane Decompensation after Surgery for Adolescent Idiopathic Scoliosis: An Effect Imparted by Postoperative Thoracic Hypokyphosis. J. Neurosurg. Spine 2011, 15, 491–496. [Google Scholar] [CrossRef]
- Seki, S.; Newton, P.O.; Yahara, Y.; Makino, H.; Nakano, M.; Hirano, N.; Kawaguchi, Y.; Kimura, T. Differential Rod Contouring Is Essential for Improving Vertebral Rotation in Patients with Adolescent Idiopathic Scoliosis: Thoracic Curves Assessed with Intraoperative CT. Spine 2018, 43, E585–E591. [Google Scholar] [CrossRef]
- Le Navéaux, F.; Larson, A.N.; Labelle, H.; Aubin, C.-E. Significant Variability in Surgeons’ Preferred Correction Maneuvers and Instrumentation Strategies When Planning Adolescent Idiopathic Scoliosis Surgery. Scoliosis Spinal Disord. 2018, 13, 21. [Google Scholar] [CrossRef]
- Lenke, L.G.; Betz, R.R.; Harms, J.; Bridwell, K.H.; Clements, D.H.; Lowe, T.G.; Blanke, K. Adolescent Idiopathic Scoliosis: A New Classification to Determine Extent of Spinal Arthrodesis. J. Bone Joint Surg. Am. 2001, 83, 1169–1181. [Google Scholar] [CrossRef]
- Navéaux, F.L.; Aubin, C.E.; Parent, S.; Newton, P.O.; Labelle, H. 3D Rod Shape Changes in Adolescent Idiopathic Scoliosis Instrumentation: How Much Does It Impact Correction? Eur. Spine J. 2017, 26, 1676–1683. [Google Scholar] [CrossRef]
- Legaye, J.; Duval-Beaupère, G.; Hecquet, J.; Marty, C. Pelvic Incidence: A Fundamental Pelvic Parameter for Three-Dimensional Regulation of Spinal Sagittal Curves. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 1998, 7, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Samdani, A.F.; Bennett, J.T.; Singla, A.R.; Marks, M.C.; Pahys, J.M.; Lonner, B.S.; Miyanji, F.; Shah, S.A.; Shufflebarger, H.L.; Newton, P.O.; et al. Do Ponte Osteotomies Enhance Correction in Adolescent Idiopathic Scoliosis? An Analysis of 191 Lenke 1A and 1B Curves. Spine Deform. 2015, 3, 483–488. [Google Scholar] [CrossRef]
- Harfouch, E.B.; Bunyan, R.F.; Al Faraidy, M.; Dajim, N.B.; Al Mulhim, F.A.; Alnemari, H.H.; Bashir, S. The Effect of Ponte Osteotomies on the Sagittal Shape of Rods and Spine Derotation in Adolescent Idiopathic Scoliosis: A Single-Center, Retrospective Cohort Study. World Neurosurg. X 2022, 15, 100125. [Google Scholar] [CrossRef]
- Wang, X.; Boyer, L.; Naveaux, F.L.; Schwend, R.M.; Aubin, C.E. How Does Differential Rod Contouring Contribute to 3-Dimensional Correction and Affect the Bone-Screw Forces in Adolescent Idiopathic Scoliosis Instrumentation? Clin. Biomech. 2016, 39, 115–121. [Google Scholar] [CrossRef]
- Clément, J.-L.; Geoffray, A.; Yagoubi, F.; Chau, E.; Solla, F.; Oborocianu, I.; Rampal, V. Relationship between Thoracic Hypokyphosis, Lumbar Lordosis and Sagittal Pelvic Parameters in Adolescent Idiopathic Scoliosis. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2013, 22, 2414–2420. [Google Scholar] [CrossRef] [Green Version]
- Abelin-Genevois, K.; Sassi, D.; Verdun, S.; Roussouly, P. Sagittal Classification in Adolescent Idiopathic Scoliosis: Original Description and Therapeutic Implications. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2018, 27, 2192–2202. [Google Scholar] [CrossRef]
- Abelin-Genevois, K.; Estivalezes, E.; Briot, J.; Sévely, A.; Sales de Gauzy, J.; Swider, P. Spino-Pelvic Alignment Influences Disc Hydration Properties after AIS Surgery: A Prospective MRI-Based Study. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2015, 24, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.-L.; Solla, F.; Amorese, V.; Oborocianu, I.; Rosello, O.; Rampal, V. Lumbopelvic Parameters Can Be Used to Predict Thoracic Kyphosis in Adolescents. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2020, 29, 2281–2286. [Google Scholar] [CrossRef] [PubMed]
- Solla, F.; Ilharreborde, B.; Blondel, B.; Prost, S.; Bauduin, E.; Laouissat, F.; Riouallon, G.; Wolff, S.; Challier, V.; Obeid, I.; et al. Can Lumbopelvic Parameters Be Used to Predict Thoracic Kyphosis at All Ages? A National Cross-Sectional Study. Glob. Spine J. 2022, 21925682221134040. [Google Scholar] [CrossRef] [PubMed]
- Rothenfluh, D.A.; Stratton, A.; Nnadi, C.; Beresford-Cleary, N. A Critical Thoracic Kyphosis Is Required to Prevent Sagittal Plane Deterioration in Selective Thoracic Fusions in Lenke I and II AIS. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2019, 28, 3066–3075. [Google Scholar] [CrossRef] [PubMed]
- Monazzam, S.; Newton, P.O.; Bastrom, T.P.; Yaszay, B. Multicenter Comparison of the Factors Important in Restoring Thoracic Kyphosis during Posterior Instrumentation for Adolescent Idiopathic Scoliosis. Spine Deform. 2013, 1, 359–364. [Google Scholar] [CrossRef]
- Trobisch, P.D.; Samdani, A.F.; Betz, R.R.; Bastrom, T.; Pahys, J.M.; Cahill, P.J. Analysis of Risk Factors for Loss of Lumbar Lordosis in Patients Who Had Surgical Treatment with Segmental Instrumentation for Adolescent Idiopathic Scoliosis. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2013, 22, 1312–1316. [Google Scholar] [CrossRef] [Green Version]
- Lonner, B.S.; Lazar-Antman, M.A.; Sponseller, P.D.; Shah, S.A.; Newton, P.O.; Betz, R.; Shufflebarger, H.S. Multivariate Analysis of Factors Associated with Kyphosis Maintenance in Adolescent Idiopathic Scoliosis. Spine 2012, 37, 1297–1302. [Google Scholar] [CrossRef]
- Fletcher, N.D.; Hopkins, J.; McClung, A.; Browne, R.; Sucato, D.J. Residual Thoracic Hypokyphosis after Posterior Spinal Fusion and Instrumentation in Adolescent Idiopathic Scoliosis: Risk Factors and Clinical Ramifications. Spine 2012, 37, 200–206. [Google Scholar] [CrossRef]
- Sardi, J.P.; Ames, C.P.; Coffey, S.; Good, C.; Dahl, B.; Kraemer, P.; Gum, J.; Devito, D.; Brayda-Bruno, M.; Lee, R.; et al. Accuracy of Rod Contouring to Desired Angles with and Without a Template: Implications for Achieving Desired Spinal Alignment and Outcomes. Glob. Spine J. 2023, 13, 2192568221998371. [Google Scholar] [CrossRef]
- Andrew Pawelek, P.O.; Jeff, P. Newton Poster 7: The Variation in How Surgeons Contour Rods for Scoliosis Correction Is Substantial. In Proceedings of the IMAST 2007 Annual Meeting, Paradise Island, Bahamas, 11–14 July 2007; p. 44. [Google Scholar]
- Luo, M.; Jiang, H.; Wang, W.; Li, N.; Shen, M.; Li, P.; Xu, G.; Xia, L. Influence of Screw Density on Thoracic Kyphosis Restoration in Hypokyphotic Adolescent Idiopathic Scoliosis. BMC Musculoskelet. Disord. 2017, 18, 526. [Google Scholar] [CrossRef] [Green Version]
- Abe, Y.; Ito, M.; Abumi, K.; Sudo, H.; Salmingo, R.; Tadano, S. Scoliosis Corrective Force Estimation from the Implanted Rod Deformation Using 3D-FEM Analysis. Scoliosis 2015, 10, S2. [Google Scholar] [CrossRef] [Green Version]
- Pesenti, S.; Clément, J.-L.; Ilharreborde, B.; Morin, C.; Charles, Y.P.; Parent, H.F.; Violas, P.; Szadkowski, M.; Boissière, L.; Jouve, J.-L.; et al. Comparison of Four Correction Techniques for Posterior Spinal Fusion in Adolescent Idiopathic Scoliosis. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2022, 31, 1028–1035. [Google Scholar] [CrossRef]
- Pesenti, S.; Lafage, R.; Henry, B.; Kim, H.J.; Bolzinger, M.; Elysée, J.; Cunningham, M.; Choufani, E.; Lafage, V.; Blanco, J.; et al. Deformity Correction in Thoracic Adolescent Idiopathic Scoliosis: A Comparison of Posteromedial Translation Using Sublaminar Bands and Cantilever with Pedicle Screws. Bone Jt. J. 2020, 102-B, 376–382. [Google Scholar] [CrossRef]
- Mladenov, K.V.; Vaeterlein, C.; Stuecker, R. Selective Posterior Thoracic Fusion by Means of Direct Vertebral Derotation in Adolescent Idiopathic Scoliosis: Effects on the Sagittal Alignment. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2011, 20, 1114–1117. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Nakamura, T.; Iwanami, A.; Hosogane, N.; Tsuji, T.; Ishii, K.; Nakamura, M.; Toyama, Y.; Chiba, K.; Matsumoto, M. Vertebral Derotation in Adolescent Idiopathic Scoliosis Causes Hypokyphosis of the Thoracic Spine. BMC Musculoskelet. Disord. 2012, 13, 99. [Google Scholar] [CrossRef] [Green Version]
- Bodendorfer, B.M.; Shah, S.A.; Bastrom, T.P.; Lonner, B.S.; Yaszay, B.; Samdani, A.F.; Miyanji, F.; Cahill, P.J.; Sponseller, P.D.; Betz, R.R.; et al. Restoration of Thoracic Kyphosis in Adolescent Idiopathic Scoliosis Over a Twenty-Year Period: Are We Getting Better? Spine 2020, 45, 1625–1633. [Google Scholar] [CrossRef]
- Vallespir, G.P.; Flores, J.B.; Trigueros, I.S.; Sierra, E.H.; Fernández, P.D.; Olaverri, J.C.R.; Alonso, M.G.; Galea, R.R.; Francisco, A.P.; Rodríguez de Paz, B.; et al. Vertebral Coplanar Alignment: A Standardized Technique for Three Dimensional Correction in Scoliosis Surgery: Technical Description and Preliminary Results in Lenke Type 1 Curves. Spine 2008, 33, 1588–1597. [Google Scholar] [CrossRef]
- Quan, G.M.Y.; Gibson, M.J. Correction of Main Thoracic Adolescent Idiopathic Scoliosis Using Pedicle Screw Instrumentation: Does Higher Implant Density Improve Correction? Spine 2010, 35, 562–567. [Google Scholar] [CrossRef]
- Tsirikos, A.I.; Mataliotakis, G.; Bounakis, N. Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis Using a Convex Pedicle Screw Technique: A Novel Concept of Deformity Correction. Bone Jt. J. 2017, 99-B, 1080–1087. [Google Scholar] [CrossRef]
- Anekstein, Y.; Mirovsky, Y.; Arnabitsky, V.; Gelfer, Y.; Zaltz, I.; Smorgick, Y. Reversing the Concept: Correction of Adolescent Idiopathic Scoliosis Using the Convex Rod de-Rotation Maneuver. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2012, 21, 1942–1949. [Google Scholar] [CrossRef] [Green Version]
- Solla, F.; Clément, J.-L.; Cunin, V.; Bertoncelli, C.M.; Fière, V.; Rampal, V. Patient-Specific Rods for Thoracic Kyphosis Correction in Adolescent Idiopathic Scoliosis Surgery: Preliminary Results. Orthop. Traumatol. Surg. Res. OTSR 2020, 106, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Cidambi, K.R.; Glaser, D.A.; Bastrom, T.P.; Nunn, T.N.; Ono, T.; Newton, P.O. Postoperative Changes in Spinal Rod Contour in Adolescent Idiopathic Scoliosis: An in Vivo Deformation Study. Spine 2012, 37, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Kluck, D.; Newton, P.O.; Sullivan, T.B.; Yaszay, B.; Jeffords, M.; Bastrom, T.P.; Bartley, C.E. A 3D Parameter Can Guide Concave Rod Contour for the Correction of Hypokyphosis in Adolescent Idiopathic Scoliosis. Spine 2020, 45, E1264–E1271. [Google Scholar] [CrossRef] [PubMed]
- Glassman, S.D.; Sucato, D.J.; Carreon, L.Y.; Sanders, J.O.; Vitale, M.G.; Lenke, L.G. Does Thoracic Hypokyphosis Matter in Lenke Type 1 Adolescent Idiopathic Scoliosis? Spine Deform. 2013, 1, 40–45. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Patients | 61 (53F) |
|---|---|
| Lenke 1 | 29 |
| Lenke 2 | 13 |
| Lenke 3 | 7 |
| Lenke 4 | 12 |
| Lumbar Modifier | |
| A | 31 |
| B | 8 |
| C | 22 |
| Thoracic Modifier | |
| − | 5 |
| N | 43 |
| + | 13 |
| Measurement | Pre-op Angle | Post-op Angle | Change in Angle | % Change | p Value |
|---|---|---|---|---|---|
| Proximal Thoracic | 30.5° ± 10.2 | 15.6° ± 7.1 | 14.9° ± 7.9 | 48.1% ± 22.5 | <0.001 |
| Main Thoracic | 68.5° ± 13.4 | 17.4° ± 9.0 | 51.2° ± 10.2 | 75.4% ± 11.3 | <0.001 |
| Thoraco–Lumbar | 43.4° ± 14.2 | 15.5° ± (9.1) | 28.6° ± 12.1 | 67.4% ± 28.0 | <0.001 |
| Clavicle Angle | |
|---|---|
| Pre-op | −2.5°± 3.2° |
| Post-op | 3.0° ± 2.7° |
| p Value | <0.001 |
| T1 Tilt | |
| Pre-op | −2.4(+/−8.81) |
| Post-op | 5.42(+/−5.2) |
| p Value | <0.001 |
| Pre-op | Post-op | Mean Difference | p Value | |
|---|---|---|---|---|
| Thoracic Kyphosis (all) | 34.6° ± 14.6° | 33.1° ± 9.0 | –1.4 ± 12.7 | |
| PI-LL | −10.7 | −6.5 | −4.3 | 0.0074 |
| PT | 7.8° ± 8.2° | 10.8° ± 9.3° | 2.6 | 0.0012 |
| SVA | –13.5 ± 36.7 | –6.9 ± 37.1 | 6.7 | 0.3087 |
| TPA | 3.0 ± 8.2 | 6.2 ± 9.6 | 2.8 | 0.0061 |
| N | Pre-op | Post-op | Mean Difference (∆TK) | p Value | |
|---|---|---|---|---|---|
| Thoracic Kyphosis (all) | 61 | 34.6° ± 14.6° | 33.1° ± 9.0 | –1.4° | |
| TK Hypokyhphosis group | 7 | 8.4° ± 9.5° | 22.4°± 3.7° | 14.0° | 0.0096 |
| TK Normo-kyhphosis group | 33 | 30.5° ± 5.7° | 32.1° ± 6.8° | 1.62° | 0.2731 |
| TK Hyperkyhphosis group | 21 | 49.2° ± 7.7° | 38.2° ± 9.5° | −11.0° | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marya, S.; Elmalky, M.; Schroeder, A.; Tambe, A. Correction of Thoracic Hypokyphosis in Adolescent Scoliosis Using Patient-Specific Rod Templating. Healthcare 2023, 11, 980. https://doi.org/10.3390/healthcare11070980
Marya S, Elmalky M, Schroeder A, Tambe A. Correction of Thoracic Hypokyphosis in Adolescent Scoliosis Using Patient-Specific Rod Templating. Healthcare. 2023; 11(7):980. https://doi.org/10.3390/healthcare11070980
Chicago/Turabian StyleMarya, Shivan, Mahmoud Elmalky, Alex Schroeder, and Anant Tambe. 2023. "Correction of Thoracic Hypokyphosis in Adolescent Scoliosis Using Patient-Specific Rod Templating" Healthcare 11, no. 7: 980. https://doi.org/10.3390/healthcare11070980