
Exploring Determinants of COVID-19 Vaccine Acceptance, Uptake, and Hesitancy in the Pediatric Population: A Study of Parents and Caregivers in Saudi Arabia during the Initial Vaccination Phase

 , , ,
, , ,  , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Methods
2.1. Sample Size
2.2. Statistical Analyses
3. Results
3.1. Participants’ Sociodemographic Characteristics
3.2. Participants’ COVID-19 Perceptions and Vaccine Uptake
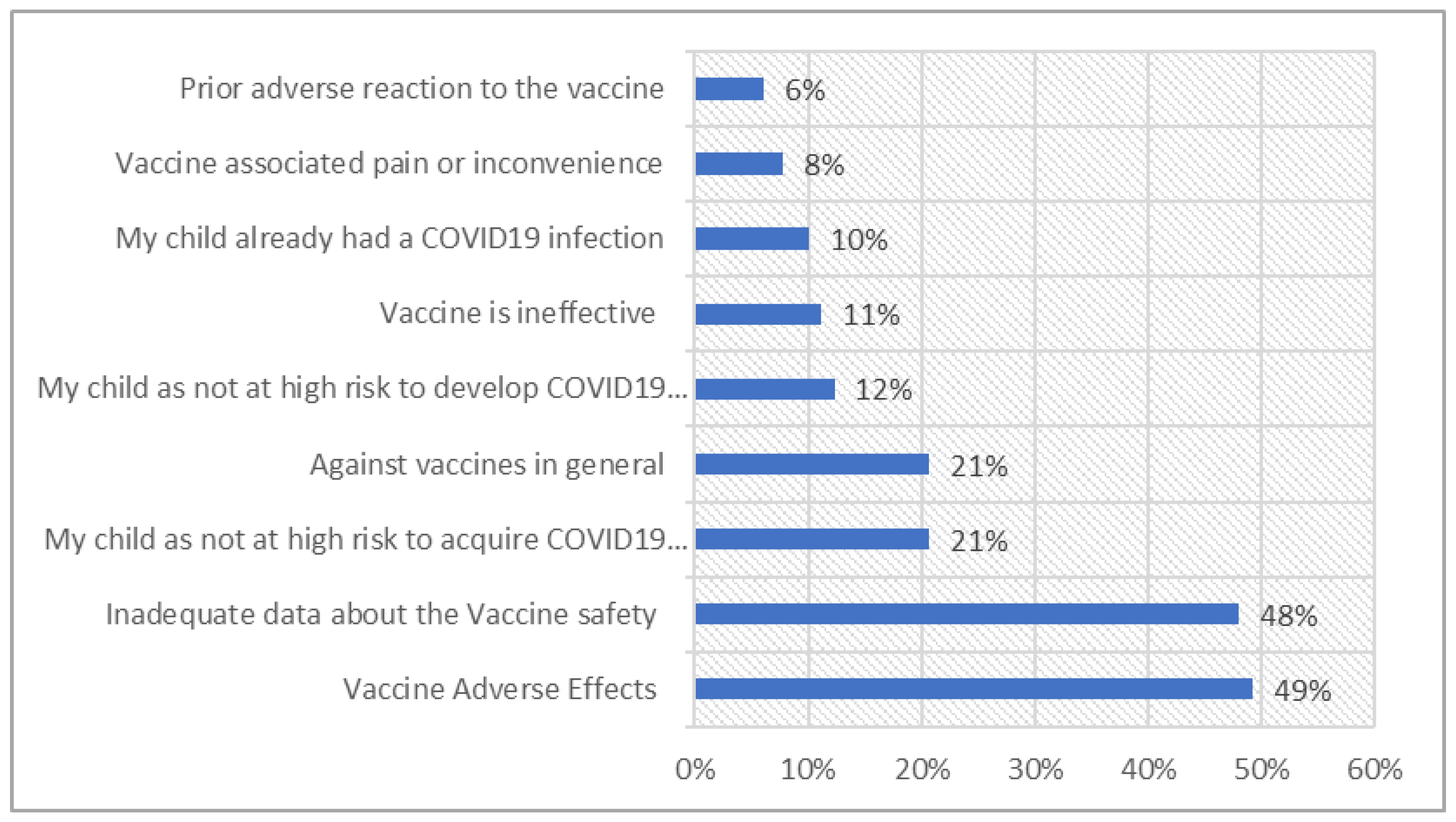
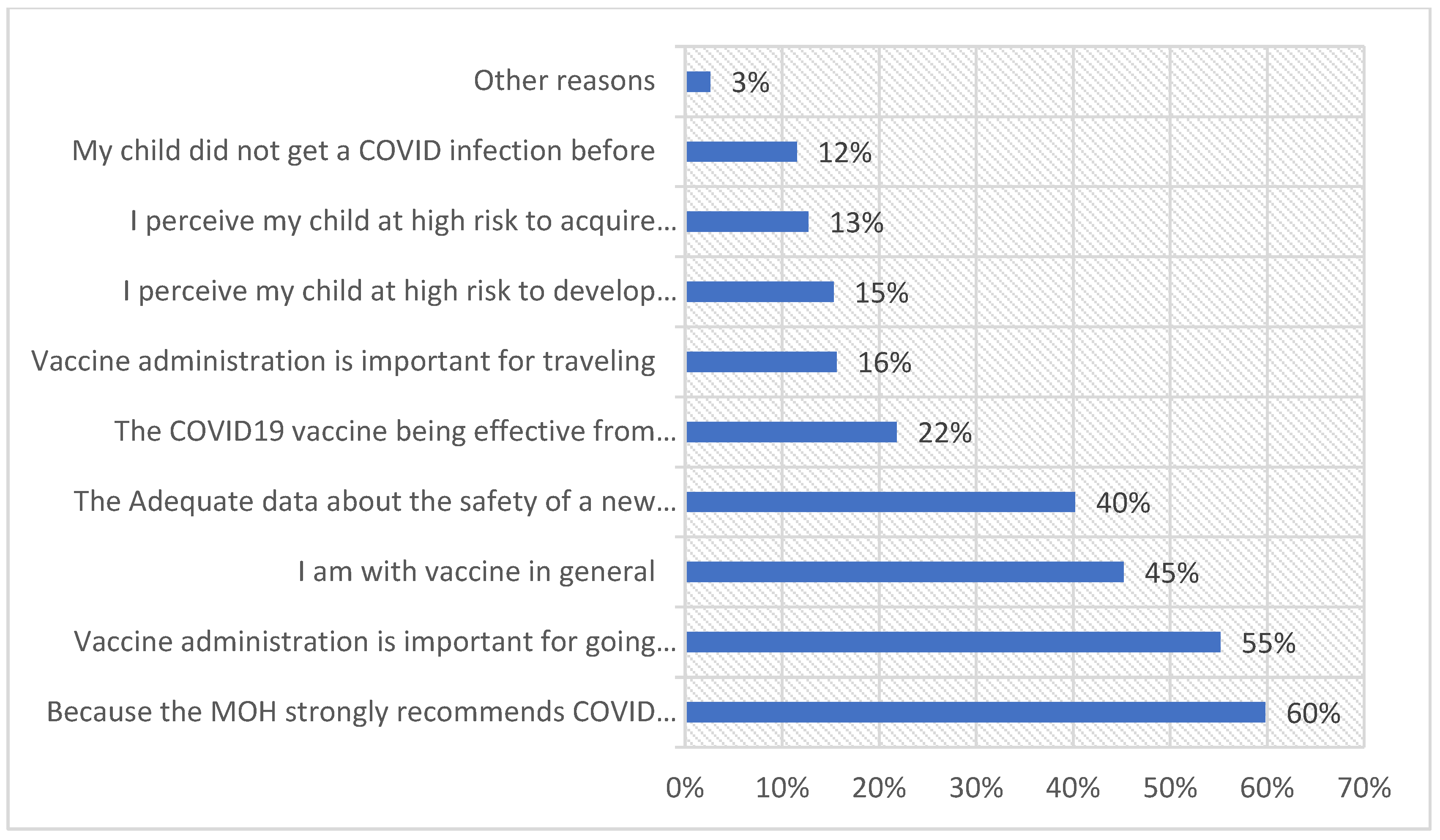
3.3. Reasons Affecting the Acceptance or Rejection of COVID-19 Vaccine in Children
3.4. Vaccine Hesitancy Scale (VHS) for COVID-19 Vaccine vs. Childhood Vaccines
3.5. Multivariate Analysis of Actual Uptake of COVID-19 Vaccine in Children
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.B.; Talaat, K.R.; Sabharwal, C.; Gurtman, A.; Lockhart, S.; Paulsen, G.C.; Barnett, E.D.; Muñoz, F.M.; Maldonado, Y.; Pahud, B.A.; et al. Evaluation of the BNT162b2 Covid-19 Vaccine in Children 5 to 11 Years of Age. N. Engl. J. Med. 2022, 386, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Capalbo, C.; Aceti, A.; Simmaco, M.; Bonfini, R.; Rocco, M.; Ricci, A.; Napoli, C.; Alfonsi, V.; Teggi, A.; Orsi, G.B.; et al. The Exponential Phase of the Covid-19 Pandemic in Central Italy: An Integrated Care Pathway. Int. J. Environ. Res. Public Health 2020, 17, 3792. [Google Scholar] [CrossRef] [PubMed]
- Sahin, U.; Muik, A.; Vogler, I.; Derhovanessian, E.; Kranz, L.M.; Vormehr, M.; Quandt, J.; Bidmon, N.; Ulges, A.; Baum, A.; et al. BNT162b2 vaccine induces neutralizing antibodies and poly-specific T cells in humans. Nature 2021, 595, 572–577. [Google Scholar] [CrossRef]
- Rumain, B.; Schneiderman, M.; Geliebter, A. Prevalence of COVID-19 in adolescents and youth compared with older adults in states experiencing surges. PLoS ONE 2021, 16, e0242587. [Google Scholar] [CrossRef] [PubMed]
- Szablewski, C.M.; Chang, K.T.; Brown, M.M.; Chu, V.T.; Yousaf, A.R.; Anyalechi, N.; Aryee, P.A.; Kirking, H.L.; Lumsden, M.; Mayweather, E.; et al. SARS-CoV-2 Transmission and Infection Among Attendees of an Overnight Camp—Georgia, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1023–1025. [Google Scholar] [CrossRef]
- Burki, T.K. COVID-19 vaccination in young children. Lancet Respir. Med. 2022, 10, e41. [Google Scholar] [CrossRef]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Comirnaty and Pfizer-BioNTech COVID-19 Vaccine. 2022. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccines (accessed on 12 February 2023).
- Glatman-Freedman, A.; Hershkovitz, Y.; Kaufman, Z.; Dichtiar, R.; Keinan-Boker, L.; Bromberg, M. Effectiveness of BNT162b2 Vaccine in Adolescents during Outbreak of SARS-CoV-2 Delta Variant Infection, Israel, 2021. Emerg. Infect. Dis. 2021, 27, 2919–2922. [Google Scholar] [CrossRef]
- Lau, J.J.; Cheng, S.M.S.; Leung, K.; Lee, C.K.; Hachim, A.; Tsang, L.C.H.; Yam, K.W.H.; Chaothai, S.; Kwan, K.K.H.; Chai, Z.Y.H.; et al. Real-world COVID-19 vaccine effectiveness against the Omicron BA.2 variant in a SARS-CoV-2 infection-naive population. Nat. Med. 2023, 29, 348–357. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Parsons Leigh, J.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 13, 3801. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of COVID-19 Vaccine Acceptance in Saudi Arabia: A Web-Based National Survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Temsah, M.H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef]
- Aljamaan, F.; Alhaboob, A.; Saddik, B.; Bassrawi, R.; Assiri, R.; Saeed, E.; Alhasan, K.; Alenezi, S.; Alarabi, M.; Alrabiaah, A.; et al. In-Person Schooling Amidst Children’s COVID-19 Vaccination: Exploring Parental Perceptions Just after Omicron Variant Announcement. Vaccines 2022, 10, 768. [Google Scholar] [CrossRef]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammed, O.A. Parents’ Hesitancy to Vaccinate Their 5–11-Year-Old Children Against COVID-19 in Saudi Arabia: Predictors From the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef] [PubMed]
- MOH. COVID-19 Vaccine Booking Service. Available online: https://www.moh.gov.sa/en/eServices/Pages/Vaccine-date.aspx (accessed on 31 January 2023).
- WHO. Report of the Sage Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 29 June 2021).
- Kempe, A.; Saville, A.W.; Albertin, C.; Zimet, G.; Breck, A.; Helmkamp, L.; Vangala, S.; Dickinson, L.M.; Rand, C.; Humiston, S.; et al. Parental Hesitancy About Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics 2020, 146, e20193852. [Google Scholar] [CrossRef]
- Temsah, M.H.; Barry, M.; Aljamaan, F.; Alhuzaimi, A.; Al-Eyadhy, A.; Saddik, B.; Alrabiaah, A.; Alsohime, F.; Alhaboob, A.; Alhasan, K.; et al. Adenovirus and RNA-based COVID-19 vaccines’ perceptions and acceptance among healthcare workers in Saudi Arabia: A national survey. BMJ Open 2021, 11, e048586. [Google Scholar] [CrossRef]
- Temsah, M.H.; Barry, M.; Aljamaan, F.; Alhuzaimi, A.N.; Al-Eyadhy, A.; Saddik, B.; Alsohime, F.; Alhaboob, A.; Alhasan, K.; Alaraj, A.; et al. SARS-CoV-2 B.1.1.7 UK Variant of Concern Lineage-Related Perceptions, COVID-19 Vaccine Acceptance and Travel Worry Among Healthcare Workers. Front. Public Health 2021, 9, 686958. [Google Scholar] [CrossRef]
- Tiirikainen, K.; Haravuori, H.; Ranta, K.; Kaltiala-Heino, R.; Marttunen, M. Psychometric properties of the 7-item Generalized Anxiety Disorder Scale (GAD-7) in a large representative sample of Finnish adolescents. Psychiatry Res. 2019, 272, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; Schuster, M.; MacDonald, N.E.; Wilson, R. Measuring vaccine hesitancy: The development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [Green Version]
- Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines 2022, 10, 110. [Google Scholar] [CrossRef]
- Mengistu, D.A.; Demmu, Y.M.; Asefa, Y.A. Global COVID-19 vaccine acceptance rate: Systematic review and meta-analysis. Front. Public Health 2022, 10, 1044193. [Google Scholar] [CrossRef] [PubMed]
- Khan, Y.H.; Rasheed, M.; Mallhi, T.H.; Salman, M.; Alzarea, A.I.; Alanazi, A.S.; Alotaibi, N.H.; Khan, S.U.; Alatawi, A.D.; Butt, M.H.; et al. Barriers and facilitators of childhood COVID-19 vaccination among parents: A systematic review. Front. Pediatr. 2022, 10, 950406. [Google Scholar] [CrossRef] [PubMed]
- Assiri, A.; Al-Tawfiq, J.A.; Alkhalifa, M.; Al Duhailan, H.; Al Qahtani, S.; Dawas, R.A.; El Seoudi, A.A.; Alomran, N.; Omar, O.A.; Alotaibi, N.; et al. Launching COVID-19 vaccination in Saudi Arabia: Lessons learned, and the way forward. Travel Med. Infect. Dis. 2021, 43, 102119. [Google Scholar] [CrossRef] [PubMed]
- Kitro, A.; Sirikul, W.; Dilokkhamaruk, E.; Sumitmoh, G.; Pasirayut, S.; Wongcharoen, A.; Panumasvivat, J.; Ongprasert, K.; Sapbamrer, R. COVID-19 vaccine hesitancy and influential factors among Thai parents and guardians to vaccinate their children. Vaccine X 2022, 11, 100182. [Google Scholar] [CrossRef]
- Skeens, M.A.; Hill, K.; Olsavsky, A.; Buff, K.; Stevens, J.; Akard, T.F.; Shah, N.; Gerhardt, C.A. Factors affecting COVID-19 vaccine hesitancy in parents of children with cancer. Pediatr. Blood Cancer 2022, 69, e29707. [Google Scholar] [CrossRef] [PubMed]
- Byrne, A.; Thompson, L.A.; Filipp, S.L.; Ryan, K. COVID-19 vaccine perceptions and hesitancy amongst parents of school-aged children during the pediatric vaccine rollout. Vaccine 2022, 40, 6680–6687. [Google Scholar] [CrossRef]
- Padhi, B.K.; Satapathy, P.; Rajagopal, V.; Rustagi, N.; Vij, J.; Jain, L.; Chakrapani, V.; Patro, B.K.; Kar, S.S.; Singh, R.; et al. Parents’ Perceptions and Intention to Vaccinate Their Children Against COVID-19: Results From a Cross-Sectional National Survey in India. Front. Med. 2022, 9, 806702. [Google Scholar] [CrossRef]
- Aedh, A.I. Parents’ Attitudes, Their Acceptance of the COVID-19 Vaccines for Children and the Contributing Factors in Najran, Saudi Arabia: A Cross-Sectional Survey. Vaccines 2022, 10, 1264. [Google Scholar] [CrossRef]
- Opel, D.J.; Taylor, J.A.; Mangione-Smith, R.; Solomon, C.; Zhao, C.; Catz, S.; Martin, D. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine 2011, 29, 6598–6605. [Google Scholar] [CrossRef]
- Al Naam, Y.A.; Elsafi, S.H.; Alkharraz, Z.S.; Almaqati, T.N.; Alomar, A.M.; Al Balawi, I.A.; Jebakumar, A.Z.; Ghazwani, A.A.; Almusabi, S.S.; Albusaili, S.; et al. Factors related to COVID-19 vaccine hesitancy in Saudi Arabia. Public Health Pract. 2022, 3, 100258. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, N.L.; Kusma, J.D.; Heard-Garris, N.; Davis, M.M.; Golbeck, E.; Barrera, L.; Macy, M.L. Parental COVID-19 vaccine hesitancy for children: Vulnerability in an urban hotspot. BMC Public Health 2021, 21, 1662. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Alrasheed, A.; Altulahi, N.; Temsah, M.H.; Almasri, Z.; Alghadeer, S.; Mubarak, A.M.; Alzamil, H.; Bashatah, A.S.; Asiri, Y.; AlRuthia, Y. Interprofessional Education Competition During the COVID-19 Pandemic at King Saud University: Benefits and Challenges. J. Multidiscip. Healthc. 2021, 14, 673–679. [Google Scholar] [CrossRef]
- Temsah, M.H.; Aljamaan, F.; Alhaboob, A.; Almosned, B.; Alsebail, R.; Temsah, R.; Senjab, A.; Alarfaj, A.; Aljudi, T.; Jamal, A.; et al. Enhancing parental knowledge of childhood and adolescence safety: An interventional educational campaign. Medicine 2022, 101, e28649. [Google Scholar] [CrossRef]
- Temsah, M.H.; Jamal, A.; Al-Tawfiq, J.A. Reflection with ChatGPT about the excess death after the COVID-19 pandemic. New Microbes New Infect. 2023, 52, 101103. [Google Scholar] [CrossRef] [PubMed]
- Huh, S. Issues in the 3rd year of the COVID-19 pandemic, including computer-based testing, study design, ChatGPT, journal metrics, and appreciation to reviewers. J. Educ. Eval. Health Prof. 2023, 20, 5. [Google Scholar] [CrossRef]
- Weeks, R.; Sangha, P.; Cooper, L.; Sedoc, J.; White, S.; Gretz, S.; Toledo, A.; Lahav, D.; Hartner, A.M.; Martin, N.M.; et al. Usability and Credibility of a COVID-19 Vaccine Chatbot for Young Adults and Health Workers in the United States: Formative Mixed Methods Study. JMIR Hum. Factors 2023, 10, e40533. [Google Scholar] [CrossRef]
- Latkin, C.A.; Dayton, L.; Yi, G.; Konstantopoulos, A.; Boodram, B. Trust in a COVID-19 vaccine in the U.S.: A social-ecological perspective. Soc. Sci. Med. 2021, 270, 113684. [Google Scholar] [CrossRef]
- Alenezi, S.; Alarabi, M.; Al-Eyadhy, A.; Aljamaan, F.; Elbarazi, I.; Saddik, B.; Alhasan, K.; Assiri, R.; Bassrawi, R.; Alshahrani, F.; et al. Parental perceptions and the 5C psychological antecedents of COVID-19 vaccination during the first month of omicron variant surge: A large-scale cross-sectional survey in Saudi Arabia. Front. Pediatr. 2022, 10, 944165. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, S.J. Data Sampling Strategies for Disaster and Emergency Health Research. Prehosp. Disaster Med. 2019, 34, 227–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Relationship to the Child | Frequency | Percentage |
|---|---|---|
| Mother | 352 | 40.3 |
| Father | 185 | 21.2 |
| Other relative | 336 | 38.5 |
| Age group | ||
| 18–24 years | 334 | 38.3 |
| 25–34 years | 145 | 16.6 |
| 35–44 years | 200 | 22.9 |
| 45–54 years | 151 | 17.3 |
| 55 years or higher | 43 | 4.9 |
| Marital status | ||
| Married, divorced, or widowed | 537 | 61.5 |
| Single | 336 | 38.5 |
| Household size (members), mean (SD) | 5.85 (2.42) | |
| Do you have a child/sibling whose age is 12–18 years | ||
| No | 327 | 37.5 |
| Yes | 546 | 62.5 |
| Was this child (aged 12–18 years) ever diagnosed with an physical or psychological illness? | ||
| No | 847 | 97 |
| Yes | 26 | 3 |
| Educational level | ||
| Middle school or less | 26 | 3 |
| High school | 214 | 24.5 |
| University | 633 | 72.5 |
| Households’ monthly income | ||
| Prefer not to answer | 213 | 24.4 |
| Less than SR 5000 (USD 1333) | 70 | 8 |
| SR 5000–10,000 (USD 1333–2666) | 162 | 18.6 |
| More than SR 10,000 (USD 2666) | 428 | 49 |
| Employment | ||
| Unemployed | 319 | 36.5 |
| Freelance job | 102 | 11.7 |
| Healthcare worker | 100 | 11.5 |
| Employed | 352 | 40.3 |
| Frequency | Percentage | |
|---|---|---|
| Did you take the COVID-19 vaccine? | ||
| Yes | 846 | 96.9 |
| No | 27 | 3.1 |
| Did any of your children/siblings (aged ≥ 12 years) receive the COVID-19 vaccine? | ||
| Yes: my child already received the COVID-19 vaccine | 421 | 48.2 |
| I plan to vaccinate my child | 273 | 31.3 |
| No | 100 | 11.5 |
| Not sure | 79 | 9 |
| Have any direct family members been affected by COVID-19? | ||
| No | 549 | 62.9 |
| Yes | 324 | 37.1 |
| Describe your family’s commitment to the precautionary measures against the COVID-19 virus, mean (SD) * | 4.10 (1.20) | |
| Describe your family’s commitment to the precautionary measures against the COVID-19 virus | ||
| Low commitment | 65 | 7.4 |
| Moderate commitment | 266 | 30.5 |
| High commitment | 542 | 62.1 |
| Parents’ generalized anxiety (GAD7) score, mean (SD) | 5.01 (5.04) | |
| Parents’ generalized anxiety (GAD7) classification | ||
| Very low: <5 points | 475 | 54.4 |
| Mild: 5–10 points | 273 | 31.3 |
| Moderate: 11–14 points | 71 | 8.1 |
| High: >15 points | 54 | 6.2 |
| Attitudes Toward Routine Childhood Vaccines | Mean * | SD |
|---|---|---|
| 3.39 | 0.7 |
| 3.3 | 0.65 |
| 3.23 | 0.73 |
| 3.06 | 0.66 |
| 3.25 | 0.66 |
| 3.3 | 0.59 |
| 2.54 | 0.85 |
| 2.29 | 0.86 |
| Attitudes Toward COVID-19 Vaccines | ||
| 3.05 | 0.086 |
| 3.05 | 0.78 |
| 3.13 | 0.8 |
| 2.52 | 0.84 |
| 3.04 | 0.69 |
| 3.08 | 0.78 |
| 3.19 | 0.69 |
| 2.82 | 0.87 |
| Multivariate Adjusted Odds Ratio | 95% CI for OR | p-Value | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Parent = Yes | 0.325 | 0.195 | 0.540 | <0.001 |
| Age group | 1.186 | 0.999 | 1.408 | 0.052 |
| COVID-19-vaccinated persons | 2.124 | 0.884 | 5.102 | 0.092 |
| Family level of COVID-19 precautionary commitment mean score | 1.233 | 0.985 | 1.544 | 0.068 |
| Household socioeconomic status index (SES-I) score | 1.771 | 1.417 | 2.212 | <0.001 |
| Educational level = High school | 0.211 | 0.074 | 0.608 | 0.004 |
| Educational level = University degree | 0.162 | 0.058 | 0.454 | 0.001 |
| Having a child/sibling who is mentally/physically disabled or diseased | 0.439 | 0.185 | 1.041 | 0.062 |
| Positive attitude toward COVID-19 vaccine | 1.301 | 0.914 | 1.851 | 0.144 |
| Positive attitude toward routine children’s vaccines | 1.150 | 0.803 | 1.646 | 0.446 |
| Generalized anxiety (GAD7) score | 1.007 | 0.979 | 1.036 | 0.612 |
| Constant | 1.545 | 0.569 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhuzaimi, A.N.; Alrasheed, A.A.; Al-Eyadhy, A.; Aljamaan, F.; Alhasan, K.; Batais, M.A.; Jamal, A.; Alshahrani, F.S.; Alenezi, S.; Alhaboob, A.; et al. Exploring Determinants of COVID-19 Vaccine Acceptance, Uptake, and Hesitancy in the Pediatric Population: A Study of Parents and Caregivers in Saudi Arabia during the Initial Vaccination Phase. Healthcare 2023, 11, 972. https://doi.org/10.3390/healthcare11070972
Alhuzaimi AN, Alrasheed AA, Al-Eyadhy A, Aljamaan F, Alhasan K, Batais MA, Jamal A, Alshahrani FS, Alenezi S, Alhaboob A, et al. Exploring Determinants of COVID-19 Vaccine Acceptance, Uptake, and Hesitancy in the Pediatric Population: A Study of Parents and Caregivers in Saudi Arabia during the Initial Vaccination Phase. Healthcare. 2023; 11(7):972. https://doi.org/10.3390/healthcare11070972
Chicago/Turabian StyleAlhuzaimi, Abdullah N., Abdullah A. Alrasheed, Ayman Al-Eyadhy, Fadi Aljamaan, Khalid Alhasan, Mohammed A. Batais, Amr Jamal, Fatimah S. Alshahrani, Shuliweeh Alenezi, Ali Alhaboob, and et al. 2023. "Exploring Determinants of COVID-19 Vaccine Acceptance, Uptake, and Hesitancy in the Pediatric Population: A Study of Parents and Caregivers in Saudi Arabia during the Initial Vaccination Phase" Healthcare 11, no. 7: 972. https://doi.org/10.3390/healthcare11070972