
Effects of Brain Wave Vibration Training on the Pain and Fatigue Disturbance Symptom Cluster in Persons with Cancer: A Randomized Controlled Trial
Abstract
:1. Introduction
2. Materials and Methods
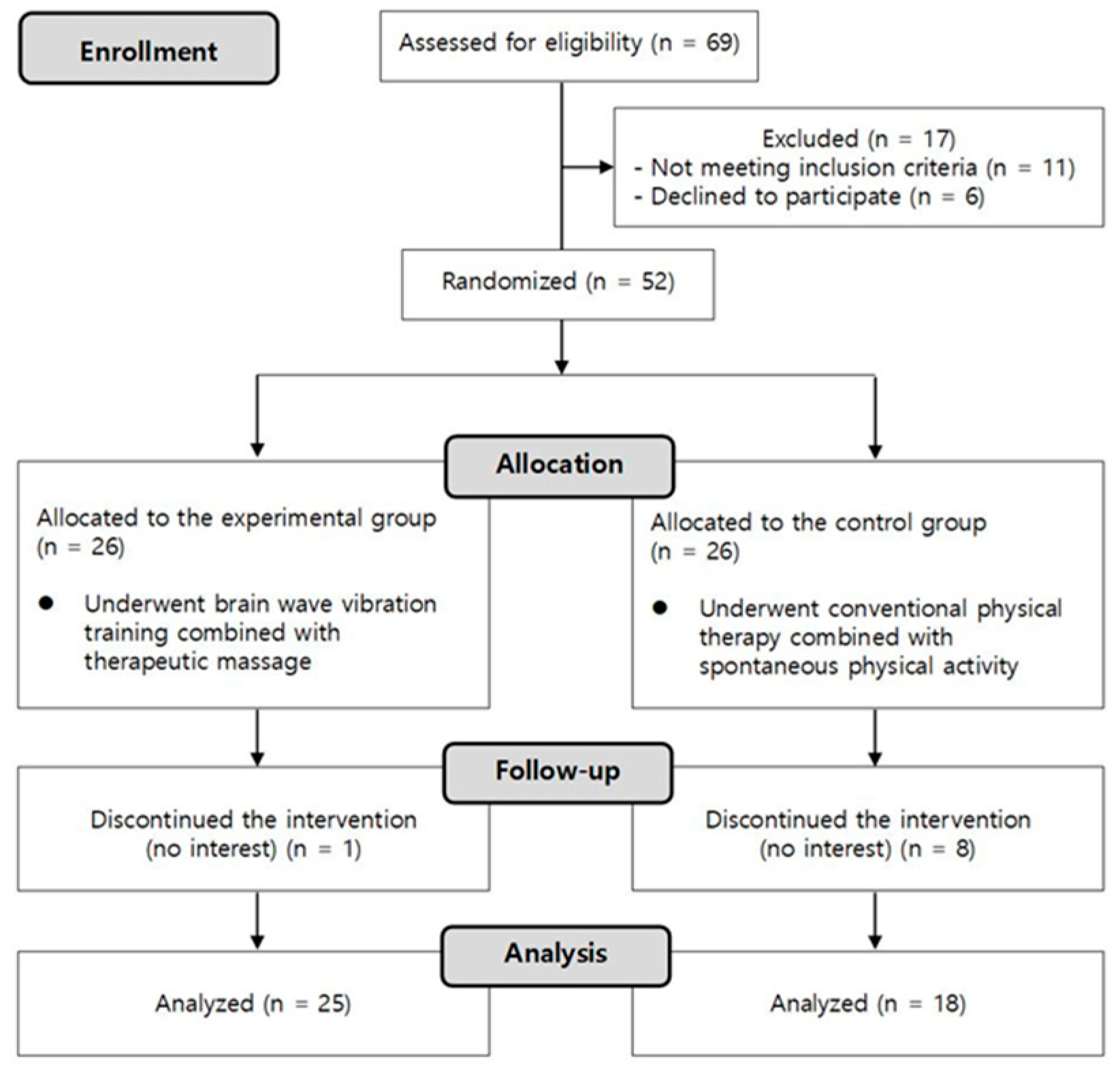
2.1. Participants
2.2. Intervention
2.3. Measurements
2.3.1. Breakthrough Pain Assessment Tool (BAT)
2.3.2. Brief Fatigue Inventory (BFI)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoffman, A.J.; Given, B.A.; von Eye, A.; Gift, A.G.; Given, C.W. Relationships Among Pain, Fatigue, Insomnia, and Gender in Persons With Lung Cancer. Oncol. Nurs. Forum 2007, 34, 785–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshields, T.L.; Potter, P.; Olsen, S.; Liu, J. The persistence of symptom burden: Symptom experience and quality of life of cancer patients across one year. Support. Care Cancer 2014, 22, 1089–1096. [Google Scholar] [CrossRef] [Green Version]
- Merskey, H. Logic, truth and language in concepts of pain. Qual. Life Res. 1994, 3, S69–S76. [Google Scholar] [CrossRef]
- Patrick, D.L.; Ferketich, S.L.; Frame, P.S.; Harris, J.J.; Hendricks, C.B.; Levin, B.; Link, M.P.; Lustig, C.; McLaughlin, J.; Ried, L.D. National Institutes of Health State-of-the-Science Conference Statement: Symptom management in cancer: Pain, depression, and fatigue, July 15-17, 2002. J. Natl. Cancer Inst. 2003, 95, 1110–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syrjala, K.L.; Jensen, M.P.; Mendoza, M.E.; Yi, J.C.; Fisher, H.M.; Keefe, F.J. Psychological and Behavioral Approaches to Cancer Pain Management. J. Clin. Oncol. 2014, 32, 1703–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maindet, C.; Burnod, A.; Minello, C.; George, B.; Allano, G.; Lemaire, A. Strategies of complementary and integrative therapies in cancer-related pain—Attaining exhaustive cancer pain management. Support. Care Cancer 2019, 27, 3119–3132. [Google Scholar] [CrossRef]
- Harrington, C.B.; Hansen, J.A.; Moskowitz, M.; Todd, B.L.; Feuerstein, M. It’s not over when it’s over: Long-term symptoms in cancer survivors—A systematic review. Int. J. Psychiatry Med. 2010, 40, 163–181. [Google Scholar] [CrossRef]
- Mock, V.; Atkinson, A.; Barsevick, A.; Cella, D.; Cimprich, B.; Cleeland, C.; Donnelly, J.; Eisenberger, M.A.; Escalante, C.; Hinds, P.; et al. NCCN Practice Guidelines for Cancer-Related Fatigue. Oncology 2000, 14, 151–161. [Google Scholar]
- Jacobsen, P.; Thors, C. Fatigue in the radiation therapy patient: Current management and investigations. Semin. Radiat. Oncol. 2003, 13, 372–380. [Google Scholar] [CrossRef]
- Everdingen, M.V.D.B.-V.; de Rijke, J.; Kessels, A.; Schouten, H.; van Kleef, M.; Patijn, J. Prevalence of pain in patients with cancer: A systematic review of the past 40 years. Ann. Oncol. 2007, 18, 1437–1449. [Google Scholar] [CrossRef]
- Kwekkeboom, K.L.; Cherwin, C.; Lee, J.W.; Wanta, B. Mind-Body Treatments for the Pain-Fatigue-Sleep Disturbance Symptom Cluster in Persons with Cancer. J. Pain Symptom Manag. 2010, 39, 126–138. [Google Scholar] [CrossRef]
- Lee, I. Brain Wave Vibration: Getting Back into the Rhythm of a Happy, Healthy Life; Best Life Media: Gilbert, AZ, USA, 2009. [Google Scholar]
- Bowden, D.E.; McLennan, D.; Gruzelier, J. A randomised controlled trial of the effects of Brain Wave Vibration training on mood and well-being. J. Complement. Integr. Med. 2014, 11, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Moruzzi, G.; Magoun, H. Brain stem reticular formation and activation of the EEG. Electroencephalogr. Clin. Neurophysiol. 1949, 1, 455–473. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-H.; Kang, D.-H.; Jang, J.H.; Park, H.Y.; Byun, M.S.; Kwon, S.J.; Jang, G.-E.; Lee, U.S.; An, S.C.; Kwon, J.S. The effects of mind–body training on stress reduction, positive affect, and plasma catecholamines. Neurosci. Lett. 2010, 479, 138–142. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, H.J.; Ahn, S.D.; Seo, Y.J.; Kim, S.H. Effects of meditation on anxiety, depression, fatigue, and quality of life of women undergoing radiation therapy for breast cancer. Complement. Ther. Med. 2013, 21, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Bowden, D.; Gaudry, C.; An, S.C.; Gruzelier, J. A Comparative Randomised Controlled Trial of the Effects of Brain Wave Vibration Training, Iyengar Yoga, and Mindfulness on Mood, Well-Being, and Salivary Cortisol. Evid. Based Complement. Altern. Med. 2011, 2012, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ma, J.; Cole, S.W.; Ganz, P.A. Mindfulness meditation for younger breast cancer survivors: A randomized controlled trial. Cancer 2014, 121, 1231–1240. [Google Scholar] [CrossRef] [Green Version]
- Metin, Z.G.; Karadas, C.; Izgu, N.; Ozdemir, L.; Demirci, U. Effects of progressive muscle relaxation and mindfulness meditation on fatigue, coping styles, and quality of life in early breast cancer patients: An assessor blinded, three-arm, randomized controlled trial. Eur. J. Oncol. Nurs. 2019, 42, 116–125. [Google Scholar] [CrossRef]
- Forsythe, L.P.; Alfano, C.M.; George, S.M.; McTiernan, A.; Baumgartner, K.B.; Bernstein, L.; Ballard-Barbash, R. Pain in long-term breast cancer survivors: The role of body mass index, physical activity, and sedentary behavior. Breast Cancer Res. Treat. 2012, 137, 617–630. [Google Scholar] [CrossRef] [Green Version]
- Post-White, J.; Kinney, M.E.; Savik, K.; Gau, J.B.; Wilcox, C.; Lerner, I. Therapeutic Massage and Healing Touch Improve Symptoms in Cancer. Integr. Cancer Ther. 2003, 2, 332–344. [Google Scholar] [CrossRef] [PubMed]
- Bangash, A.A.; Durrani, Z. Effectiveness of acetaminophen in control of breakthrough pain: Randomized controlled trial. J. Pak. Med. Assoc. 2018, 68, 994–1001. [Google Scholar]
- Shin, J.; Cho, S.J.; Lee, J.; Choi, Y.S. Validation of the Korean Version of the Breakthrough Pain Assessment Tool in Cancer Patients. J. Pain Symptom Manag. 2017, 54, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Webber, K.; Davies, A.N.; Zeppetella, G.; Cowie, M.R. Development and Validation of the Breakthrough Pain Assessment Tool (BAT) in Cancer Patients. J. Pain Symptom Manag. 2014, 48, 619–631. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The rapid assessment of fatigue severity in cancer patients: Use of the Brief Fatigue Inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Yun, Y.H.; Wang, X.S.; Lee, J.S.; Roh, J.W.; Lee, C.G.; Lee, W.S.; Lee, K.S.; Bang, S.-M.; Mendoza, T.R.; Cleeland, C.S. Validation Study of the Korean Version of the Brief Fatigue Inventory. J. Pain Symptom Manag. 2005, 29, 165–172. [Google Scholar] [CrossRef]
- Gebremariam, G.T.; Anshabo, A.T.; Tigeneh, W.; Engidawork, E. Validation of the Amharic Version of the Brief Fatigue Inventory for Assessment of Cancer-Related Fatigue in Ethiopian Cancer Patients. J. Pain Symptom Manag. 2018, 56, 264–272. [Google Scholar] [CrossRef] [PubMed]
- De Groef, A.; Penen, F.; Dams, L.; Van der Gucht, E.; Nijs, J.; Meeus, M. Best-Evidence Rehabilitation for Chronic Pain Part 2: Pain during and after Cancer Treatment. J. Clin. Med. 2019, 8, 979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alpozgen, A.Z.; Ozdincler, A.R.; Karanlik, H.; Agaoglu, F.Y.; Narin, A. Effectiveness of Pilates-based exercises on upper extremity disorders related with breast cancer treatment. Eur. J. Cancer Care 2016, 26, e12532. [Google Scholar] [CrossRef] [PubMed]
- Danhauer, S.C.; Addington, E.L.; Cohen, L.; Sohl, S.J.; Van Puymbroeck, M.; Albinati, N.K.; Culos-Reed, S.N. Yoga for symptom management in oncology: A review of the evidence base and future directions for research. Cancer 2019, 125, 1979–1989. [Google Scholar] [CrossRef]
- Eyigor, S.; Karapolat, H.; Yesil, H.; Uslu, R.; Durmaz, B. Effects of pilates exercises on functional capacity, flexibility, fatigue, depression and quality of life in female breast cancer patients: A randomized controlled study. Eur. J. Phys, Rehabil. Med. 2010, 46, 481–487. [Google Scholar]
- Husebø, A.M.L.; Husebø, T.L. Quality of Life and Breast Cancer: How Can Mind–Body Exercise Therapies Help? An Overview Study. Sports 2017, 5, 79. [Google Scholar] [CrossRef] [Green Version]
- Boyd, C.; Crawford, C.; Paat, C.F.; Price, A.; Xenakis, L.; Zhang, W.; Evidence for Massage Therapy (EMT) Working Group; Buckenmaier, C. The Impact of Massage Therapy on Function in Pain Populations-A Systematic Review and Meta-Analysis of Randomized Controlled Trials: Part III, Surgical Pain Populations. Pain Med. 2016, 17, 1757–1772. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.-J.; Kleckner, I.R.; Loh, K.P.; Inglis, J.E.; Peppone, L.J.; Janelsins, M.C.; Kamen, C.S.; Heckler, C.E.; Culakova, E.; Pigeon, W.R.; et al. Influence of Yoga on Cancer-Related Fatigue and on Mediational Relationships Between Changes in Sleep and Cancer-Related Fatigue: A Nationwide, Multicenter Randomized Controlled Trial of Yoga in Cancer Survivors. Integr. Cancer Ther. 2019, 18, 1534735419855134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zetzl, T.; Renner, A.; Pittig, A.; Jentschke, E.; Roch, C.; van Oorschot, B. Yoga effectively reduces fatigue and symptoms of depression in patients with different types of cancer. Support. Care Cancer 2020, 29, 2973–2982. [Google Scholar] [CrossRef] [PubMed]
- Larkey, L.K.; Roe, D.J.; Weihs, K.L.; Jahnke, R.; Lopez, A.M.; Rogers, C.E.; Oh, B.; Guillen-Rodriguez, J. Randomized Controlled Trial of Qigong/Tai Chi Easy on Cancer-Related Fatigue in Breast Cancer Survivors. Ann. Behav. Med. 2014, 49, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Fraser, L.-A.; Morrison, D.; Morley-Forster, P.; Paul, T.; Tokmakejian, S.; Nicholson, R.L.; Bureau, Y.; Friedman, T.; Van Uum, S.H.M. Oral Opioids for Chronic Non-cancer Pain: Higher Prevalence of Hypogonadism in Men than in Women. Exp. Clin. Endocrinol. Diabetes 2008, 117, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Rajagopal, A.; Vassilopoulou-Sellin, R.; Palmer, J.L.; Kaur, G.; Bruera, E. Symptomatic hypogonadism in male survivors of cancer with chronic exposure to opioids. Cancer 2004, 100, 851–858. [Google Scholar] [CrossRef]
- Greenfield, D.M.; Walters, S.J.; Coleman, R.E.; Hancock, B.W.; Snowden, J.A.; Shalet, S.M.; DeRogatis, L.R.; Ross, R.J. Quality of life, self-esteem, fatigue, and sexual function in young men after cancer: A controlled cross-sectional study. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2010, 116, 1592–1601. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Categories | Experimental Group (n = 25) | Control Group (n = 18) |
|---|---|---|---|
| Age (years) | 58.1 ± 5.6 a | 56.6 ± 9.9 | |
| Height (cm) | 160.2 ± 8.2 | 161.3 ± 8.5 | |
| Weight (kg) | 59.6 ± 7.5 | 58.6 ± 9.2 | |
| Gender | Male | 6 (24.0) b | 4 (22.2) |
| Female | 19 (76.0) | 14 (77.8) | |
| Cancer type c | Breast cancer | 10 (40.0) | 4 (22.2) |
| Gynecologic cancer | 5 (20.0) | 3 (16.7) | |
| Colorectal cancer | 4 (16.0) | 4 (22.2) | |
| Lung cancer | 5 (20.0) | 3 (16.7) | |
| Gastric cancer | 1 (4.0) | 1 (5.6) | |
| Other cancers | 3 (12.0) | 3 (16.7) | |
| Treatment d | Surgery | 22 (88.0) | 12 (66.7) |
| Chemotherapy | 20 (80.0) | 13 (72.2) | |
| Radiation therapy | 9 (36.0) | 4 (22.2) |
| Locations | Experimental Group (n = 25) | Control Group (n = 18) | ||
|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | |
| Waist | 8 (32.0) a | 7 (28.0) | 3 (16.7) | 4 (22.2) |
| Back | 1 (4.0) | 0 (0) | 3 (16.7) | 0 (0) |
| Neck | 6 (24.0) | 3 (12.0) | 0 (0) | 2 (11.1) |
| Pelvis | 2 (8.0) | 1 (4.0) | 0 (0) | 0 (0) |
| Lower extremities | 12 (48.0) | 12 (48.0) | 8 (44.4) | 7 (38.9) |
| Shoulder | 8 (32.0) | 5 (20.0) | 1 (5.6) | 3 (16.7) |
| Upper extremities | 7 (28.0) | 4 (16.0) | 5 (27.8) | 2 (11.1) |
| Abdomen | 3 (12.0) | 1 (4.0) | 2 (11.1) | 3 (16.7) |
| Elsewhere (e.g., chest, anus, surgical site) | 4 (16.0) | 5 (20.0) | 5 (27.8) | 5 (27.8) |
| Variables | Categories | Experimental Group (n = 25) | Control Group (n = 18) | ||
|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | ||
| Pain frequency | Less than once a day | 4 (16.0) a | 6 (24.0) | 3 (16.7) | 7 (38.9) |
| 1–2 times a day | 3 (12.0) | 8 (32.0) | 5 (27.8) | 3 (16.7) | |
| 3–4 times a day | 9 (36.0) | 4 (16.0) | 4 (22.2) | 2 (11.1) | |
| More than 4 times a day | 9 (36.0) | 5 (20.0) | 6 (33.3) | 6 (33.3) | |
| Do not know | 0 (0) | 2 (8.0) | 0 (0) | 0 (0) | |
| Trigger factors | Nonexistent | 9 (36.0) | 9 (36.0) | 9 (50.0) | 11 (61.1) |
| Existent | 16 (64.0) | 16 (64.0) | 9 (50.0) | 7 (38.9) | |
| Pain-relief factors | Nonexistent | 11 (44.0) | 8 (32.0) | 5 (27.8) | 8 (44.4) |
| Existent | 14 (56.0) | 17 (68.0) | 13 (72.2) | 10 (55.6) | |
| Variables | Categories | Experimental Group (n = 25) | Control Group (n = 18) | ||
|---|---|---|---|---|---|
| Pre-Test | Post-Test | Pre-Test | Post-Test | ||
| Use of painkillers | Non-use | 19 (76.0) a | 19 (76.0) | 8 (44.4) | 11 (61.1) |
| Use | 6 (24.0) | 6 (24.0) | 10 (55.6) | 7 (38.9) | |
| Meaningful effects | No effect | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| <10 min | 1 (4.0) | 0 (0) | 0 (0) | 0 (0) | |
| 10–20 min | 0 (0) | 1 (4.0) | 1 (5.6) | 0 (0) | |
| 20–30 min | 2 (8.0) | 0 (0) | 1 (5.6) | 2 (11.1) | |
| >30 min | 3 (12.0) | 5 (20.0) | 8 (44.4) | 5 (27.8) | |
| Side effects | Existent | 1 (4.0) | 1 (4.0) | 1 (5.6) | 1 (5.6) |
| Variables | Experimental Group (n = 25) | Within Group | Control Group (n = 18) | Within Group | Between Groups | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | z | p | Pre-Test | Post-Test | z | p | z | p | |
| Lasting time b | 3.0 (1.5–4.0) a | 2.0 (1.0–2.5) | −2.931 | 0.003 * | 2.5 (1.0–4.0) | 1.5 (1.0–4.0) | −0.358 | 0.720 | −0.357 | 0.721 |
| Worst episode | 8.0 (7.0–8.0) | 3.0 (1.5–5.0) | −3.981 | 0.000 * | 3.5 (2.8–6.0) | 5.0 (1.8–6.5) | −1.135 | 0.256 | −2.500 | 0.012 † |
| Typical episode | 7.0 (5.0–8.0) | 2.0 (1.0–3.5) | −4.241 | 0.000 * | 3.0 (2.0–4.3) | 3.0 (2.0–4.3) | −0.178 | 0.859 | −3.709 | 0.000 † |
| Pain distress | 8.0 (5.0–9.0) | 2.0 (1.0–5.0) | −4.025 | 0.000 * | 3.0 (1.8–5.0) | 3.0 (1.0–5.3) | −0.963 | 0.336 | −2.732 | 0.006 † |
| Interference with normal living | 8.0 (6.0–9.0) | 3.0 (1.0–5.0) | −3.744 | 0.000 * | 3.0 (0.0–6.3) | 2.0 (0.8–6.0) | −0.826 | 0.409 | −2.351 | 0.019 † |
| Variable | Experimental Group (n = 25) | Within Group | Control Group (n = 18) | Within Group | Between Groups | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Test | Post-Test | t | p | Pre-Test | Post-Test | t | p | t | p | |
| Fatigue | 49.1 ± 23.0 a | 29.2 ± 18.4 | 4.557 | 0.000 * | 30.9 ± 19.1 | 33.9 ± 22.9 | −0.753 | 0.462 | 2.368 | 0.070 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, N.-G.; Kim, B.-K. Effects of Brain Wave Vibration Training on the Pain and Fatigue Disturbance Symptom Cluster in Persons with Cancer: A Randomized Controlled Trial. Healthcare 2023, 11, 956. https://doi.org/10.3390/healthcare11070956
Lee N-G, Kim B-K. Effects of Brain Wave Vibration Training on the Pain and Fatigue Disturbance Symptom Cluster in Persons with Cancer: A Randomized Controlled Trial. Healthcare. 2023; 11(7):956. https://doi.org/10.3390/healthcare11070956
Chicago/Turabian StyleLee, Nam-Gi, and Byeong-Kwan Kim. 2023. "Effects of Brain Wave Vibration Training on the Pain and Fatigue Disturbance Symptom Cluster in Persons with Cancer: A Randomized Controlled Trial" Healthcare 11, no. 7: 956. https://doi.org/10.3390/healthcare11070956