
The Effectiveness and Safety of Acupuncture on Suicidal Behavior: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection Process
2.4. Data Extraction Process
2.5. Quality Assessment Process
2.6. Data Synthesis and Analysis Process
3. Results
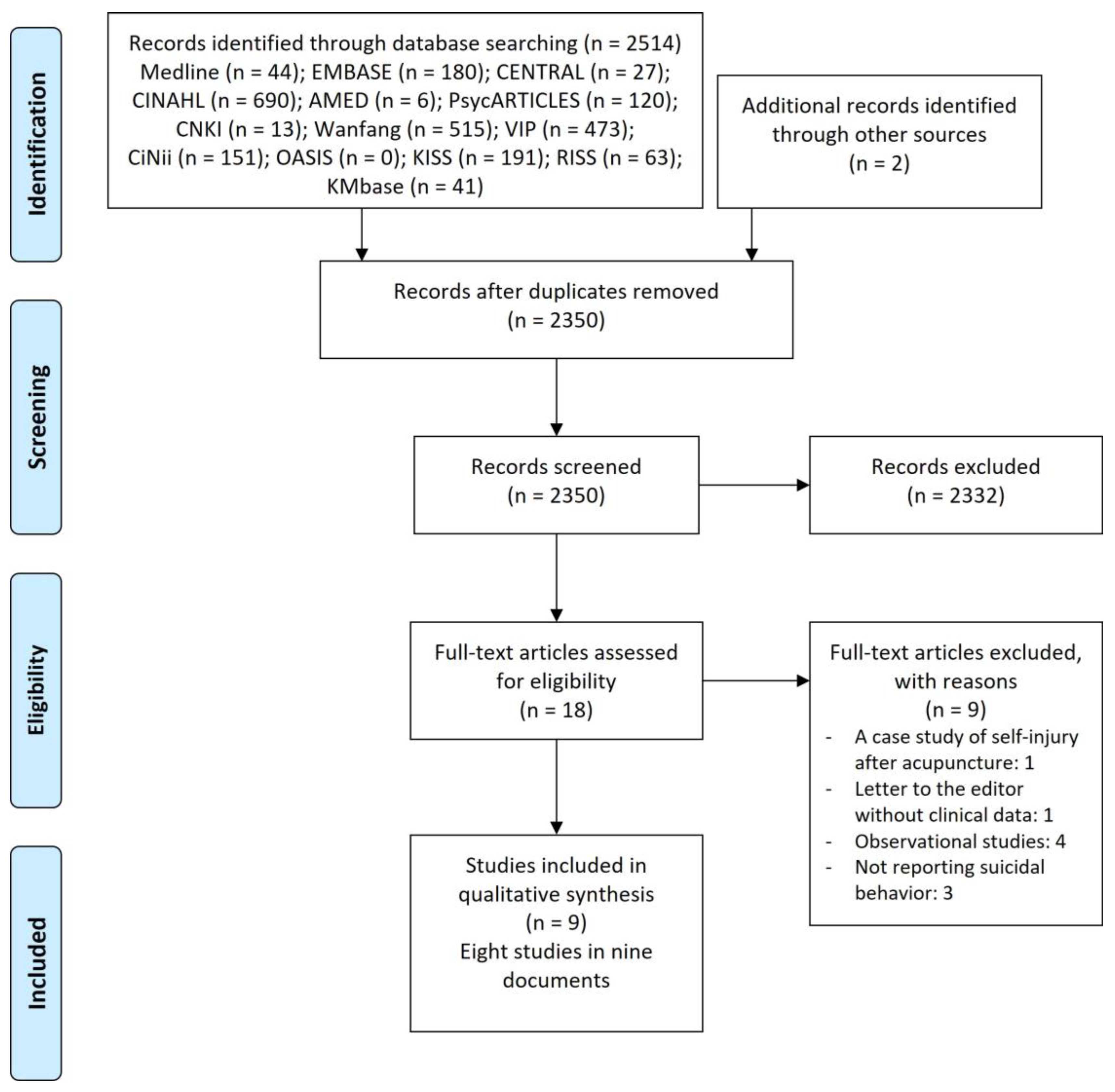
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. The Methodological Quality of Included Studies
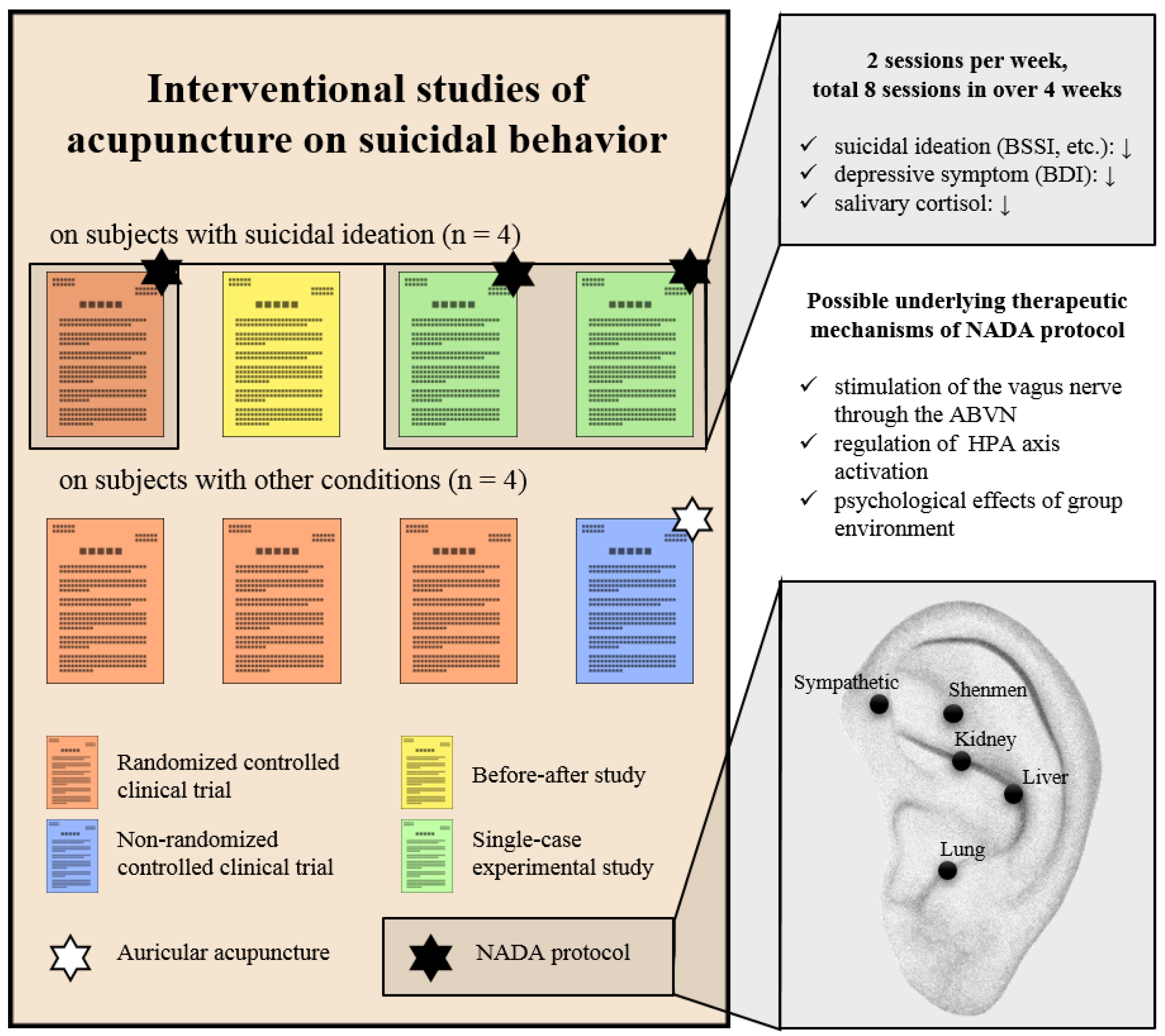
3.4. Details of Acupuncture Procedure
3.5. Impact of Acupuncture on Subjects with Suicidal Ideation
3.5.1. RCT (n = 1)
3.5.2. Before–After Study (n = 1)
3.5.3. Single-Case Experimental Study (n = 2)
3.6. Impact of Acupuncture on Participants with Other Conditions
3.6.1. RCT (n = 3)
3.6.2. CCT (n = 1)
3.7. Safety of Acupuncture
4. Discussion
4.1. Summary of Findings
4.2. Clinical Implication
4.3. Limitations
4.4. Suggestions for Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ilic, M.; Ilic, I. Worldwide suicide mortality trends (2000–2019): A joinpoint regression analysis. World J. Psychiatry 2022, 12, 1044–1060. [Google Scholar] [CrossRef]
- Borges, G.; Nock, M.K.; Haro Abad, J.M.; Hwang, I.; Sampson, N.A.; Alonso, J.; Andrade, L.H.; Angermeyer, M.C.; Beautrais, A.; Bromet, E.; et al. Twelve-month prevalence of and risk factors for suicide attempts in the World Health Organization World Mental Health Surveys. J. Clin. Psychiatry 2010, 71, 1617–1628. [Google Scholar] [CrossRef] [Green Version]
- Bachmann, S. Epidemiology of Suicide and the Psychiatric Perspective. Int. J. Environ. Res. Public Health 2018, 15, 1425. [Google Scholar] [CrossRef] [Green Version]
- Nock, M.K.; Hwang, I.; Sampson, N.; Kessler, R.C.; Angermeyer, M.; Beautrais, A.; Borges, G.; Bromet, E.; Bruffaerts, R.; de Girolamo, G.; et al. Cross-national analysis of the associations among mental disorders and suicidal behavior: Findings from the WHO World Mental Health Surveys. PLoS Med. 2009, 6, e1000123. [Google Scholar] [CrossRef] [Green Version]
- Ahmedani, B.K.; Peterson, E.L.; Hu, Y.; Rossom, R.C.; Lynch, F.; Lu, C.Y.; Waitzfelder, B.E.; Owen-Smith, A.A.; Hubley, S.; Prabhakar, D.; et al. Major Physical Health Conditions and Risk of Suicide. Am. J. Prev. Med. 2017, 53, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Hochhauser, S.; Rao, S.; England-Kennedy, E.; Roy, S. Why social justice matters: A context for suicide prevention efforts. Int J. Equity Health 2020, 19, 76. [Google Scholar] [CrossRef]
- D’Anci, K.E.; Uhl, S.; Giradi, G.; Martin, C. Treatments for the Prevention and Management of Suicide: A Systematic Review. Ann. Intern. Med. 2019, 171, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, K.E.A.; Hawton, K. The role of psychopharmacology in suicide prevention. Epidemiol. E Psichiatr. Soc. 2011, 18, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Iskander, J.K.; Crosby, A.E. Implementing the national suicide prevention strategy: Time for action to flatten the curve. Prev. Med. 2021, 152, 106734. [Google Scholar] [CrossRef]
- Stene-Larsen, K.; Reneflot, A. Contact with primary and mental health care prior to suicide: A systematic review of the literature from 2000 to 2017. Scand. J. Public Health 2019, 47, 9–17. [Google Scholar] [CrossRef]
- Raue, P.J.; Ghesquiere, A.R.; Bruce, M.L. Suicide risk in primary care: Identification and management in older adults. Curr. Psychiatry Rep. 2014, 16, 466. [Google Scholar] [CrossRef] [Green Version]
- Basri, N.F.; Ramli, A.S.; Mohamad, M.; Kamaruddin, K.N. Traditional and complementary medicine (TCM) usage and its association with Patient Assessment of Chronic Illness Care (PACIC) among individuals with metabolic syndrome in primary care. BMC Complement Med. Ther. 2022, 22, 14. [Google Scholar] [CrossRef]
- Ashraf, H.; Salehi, A.; Sousani, M.; Sharifi, M.H. Use of Complementary Alternative Medicine and the Associated Factors among Patients with Depression. Evid. Based Complement. Alternat. Med. 2021, 2021, 6626394. [Google Scholar] [CrossRef] [PubMed]
- Prady, S.L.; Burch, J.; Crouch, S.; MacPherson, H. Controlling practitioner-patient relationships in acupuncture trials: A systematic review and meta-regression. Acupunct. Med. 2013, 31, 162–171. [Google Scholar] [CrossRef]
- Armour, M.; Smith, C.A.; Wang, L.Q.; Naidoo, D.; Yang, G.Y.; MacPherson, H.; Lee, M.S.; Hay, P. Acupuncture for Depression: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, S.; Colaiaco, B.; Motala, A.; Shanman, R.; Sorbero, M.; Hempel, S. Acupuncture for the Treatment of Adults with Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. J. Trauma Dissociation 2018, 19, 39–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Skinner, M.; McDonough, S.; Mabire, L.; Baxter, G.D. Acupuncture for low back pain: An overview of systematic reviews. Evid. Based Complement. Alternat. Med. 2015, 2015, 328196. [Google Scholar] [CrossRef] [Green Version]
- Kwon, C.Y.; Lee, B. The efficacy of acupuncture on suicidal behavior: A protocol for systematic review and meta-analysis. AIMS Public Health 2022, 9, 651–660. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A. Manual for the Beck Scale for Suicide Ideation; Psychological Corporation: San Antonio, TX, USA, 1991; Volume 63. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.; Seo, H.; Lee, Y.; Park, J. Study design algorithm for medical literature of intervention (DAMI) and risk of bias for nonrandomized studies (robans) ver 2.0 by HIRA. In Seoul: Health Insurance Review & Assessment Service; Health Insurance Review & Assessment Service: Seoul, Republic of Korea, 2013. [Google Scholar]
- National Heart, Lung, and Blood Institute (NHLBI). Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 5 December 2022).
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donaldson, D.; Kroening, R. Self injury following acupuncture treatment. Am. J. Acupunct. 1979, 7, 339–342. [Google Scholar]
- Nateghi, S.; Effatpanah, H. Auricular acupuncture for suicidal ideation in methadone patients. Iran. J. Psychiatry Behav. Sci. 2019, 13, e98121. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Lin, X.; Brauera, F.J.; Scott, E.; Murray, A.; Brady, K.; Goldberg, B. A Preliminary Study on the Effect of Traditional Chinese Medicine and Acupuncture on Self-mutilation Behavior. Yunnan J. Tradit. Chin. Med. Mater. Med. 1995, 16, 4. [Google Scholar]
- Janssen, P.A.; Demorest, L.C.; Whynot, E.M. Acupuncture for substance abuse treatment in the Downtown Eastside of Vancouver. J. Urban Health 2005, 82, 285–295. [Google Scholar] [CrossRef] [Green Version]
- Meerwijk, E.L.; Larson, M.J.; Schmidt, E.M.; Adams, R.S.; Bauer, M.R.; Ritter, G.A.; Buckenmaier, C., 3rd; Harris, A.H.S. Nonpharmacological Treatment of Army Service Members with Chronic Pain Is Associated with Fewer Adverse Outcomes After Transition to the Veterans Health Administration. J. Gen. Intern. Med. 2020, 35, 775–783. [Google Scholar] [CrossRef]
- Vitale, A.; Byma, L.; Sun, S.; Podolak, E.; Wang, Z.; Alter, S.; Galfalvy, H.; Geraci, J.; Langhoff, E.; Klingbeil, H.; et al. Effectiveness of Complementary and Integrative Approaches in Promoting Engagement and Overall Wellness Toward Suicide Prevention in Veterans. J. Altern. Complement. Med. 2021, 27, S14–S27. [Google Scholar] [CrossRef]
- Nixon, M.K.; Cheng, M.; Cloutier, P. An open trial of auricular acupuncture for the treatment of repetitive self-injury in depressed adolescents. Can. Child Adolesc. Psychiatry Rev. 2003, 12, 10–12. [Google Scholar]
- Davies, S.; Bell, D.; Irvine, F.; Tranter, R. Self-administered acupuncture as an alternative to deliberate self-harm: A feasibility study. J. Pers. Disord. 2011, 25, 741–754. [Google Scholar] [CrossRef]
- Ting, C.H. The Study on the Clinical Effect of Lai’s Tong-Yuan Acupuncture in Depression caused by Liver qi Stagnation Syndrome. Ph.D. Thesis, Guangzhou University of Chinese Medicine, Guangzhou, China, 2020. [Google Scholar]
- Wang, S. Correlation Research on Antidepressant Clinical Effect of Electroacupuncture and TCM Symptoms Based on RWS Principle. Ph.D. Thesis, Beijing University of Chinese Medicine, Beijing, China, 2014. [Google Scholar]
- Yang, X. Correlation between the Clinical Effect of Electroacupuncture Treatment of Depression and the Quality of Life Based on RWS. Master’s Thesis, Beijing University of Chinese Medicine, Beijing, China, 2014. [Google Scholar]
- Li, Z.; Liu, F.; Luo, B.; Dai, Y. Clinical observation on auricular magnetotherapy for convalescent stroke patients with depression. Zhongguo Zhen Jiu 2018, 38, 942–947. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Wang, S.; Feng, J.; Guo, T. 21 Cases of Depression Accompanied by Suicidal Ideation Treated with Acupuncture of Soothing the Liver and Regulating Qi. TCM Res. 2019, 32, 2. [Google Scholar]
- Pirnia, B.; Bazargan, N.M.; Hamdieh, M.; Pirnia, K.; Malekanmehr, P.; Maleki, F.; Zahiroddin, A. The effectiveness of auricular acupuncture on the levels of cortisol in a depressed patient. Iran. J. Public Health 2019, 48, 1748–1750. [Google Scholar] [CrossRef] [PubMed]
- Pirnia, B.; Mohammadi, A.R.; Zahiroddin, A.; Bazargan, N.M.; Malekanmehr, P.; Pirnia, K. Evaluation of the effectiveness of auricular acupuncture in suicidal ideation and cortisol level in dysthymic patients with comorbid opiate use disorders enrolled in methadone maintenance treatment: A randomized, double-blind, sham-controlled trial. Iran. J. Psychiatry Behav. Sci. 2019, 13, 1–5. [Google Scholar] [CrossRef]
- Pirnia, B.; Pirnia, K.; Haghighat, S.; Malekanmehr, P.; Zahiroddin, A. The effectiveness of acupuncture on cortisol levels in a prostate-carcinoma patient under androgen deprivation therapy with dysthymic syndrome: A single-case experimental design. Middle East J. Cancer 2020, 11, 237–242. [Google Scholar] [CrossRef]
- Yang, X.; Gong, W.; Ma, X.; Wang, S.; Wang, X.; Guo, T.; Guo, Z.; Sun, Y.; Li, J.; Zhao, B.; et al. Factor analysis of electroacupuncture and selective serotonin reuptake inhibitors for major depressive disorder: An 8-week controlled clinical trial. Acupunct. Med. 2020, 38, 45–52. [Google Scholar] [CrossRef]
- Li, J.; Maimaitiaili, M. Influence of Electroacupuncture Therapy and Music Therapy on Patients with Mild and Moderate Depression. West. J. Tradit. Chin. Med. 2021, 34, 127–129. [Google Scholar] [CrossRef]
- Carter, K.; Olshan-Perlmutter, M.; Marx, J.; Martini, J.F.; Cairns, S.B. NADA Ear Acupuncture: An Adjunctive Therapy to Improve and Maintain Positive Outcomes in Substance Abuse Treatment. Behav. Sci. 2017, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Stuyt, E.B.; Voyles, C.A. The National Acupuncture Detoxification Association protocol, auricular acupuncture to support patients with substance abuse and behavioral health disorders: Current perspectives. Subst. Abuse Rehabil. 2016, 7, 169–180. [Google Scholar] [CrossRef] [Green Version]
- Geib, J.; Rieger, M.A.; Joos, S.; Eschweiler, G.W.; Metzger, F.G. Implementation of auricular acupuncture by the NADA protocol in geriatric patients suffering from major depression: A mixed methods feasibility study. Z. Gerontol. Geriatr. 2017, 50, 316–324. [Google Scholar] [CrossRef]
- Kwon, C.Y.; Lee, B.; Kim, S.H. Effectiveness and safety of ear acupuncture for trauma-related mental disorders after large-scale disasters: A PRISMA-compliant systematic review. Medicine 2020, 99, e19342. [Google Scholar] [CrossRef] [PubMed]
- Hou, P.W.; Hsu, H.C.; Lin, Y.W.; Tang, N.Y.; Cheng, C.Y.; Hsieh, C.L. The History, Mechanism, and Clinical Application of Auricular Therapy in Traditional Chinese Medicine. Evid. Based Complement. Alternat. Med. 2015, 2015, 495684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bremner, J.D.; Gurel, N.Z.; Wittbrodt, M.T.; Shandhi, M.H.; Rapaport, M.H.; Nye, J.A.; Pearce, B.D.; Vaccarino, V.; Shah, A.J.; Park, J.; et al. Application of Noninvasive Vagal Nerve Stimulation to Stress-Related Psychiatric Disorders. J. Pers. Med. 2020, 10, 119. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Ferguson, E.; Green, J.A.; O’Carroll, R.E.; O’Connor, R.C. Cortisol levels and suicidal behavior: A meta-analysis. Psychoneuroendocrinology 2016, 63, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Carter, K.; Olshan-Perlmutter, M. Impulsivity and Stillness: NADA, Pharmaceuticals, and Psychotherapy in Substance Use and Other DSM 5 Disorders. Behav. Sci. 2015, 5, 537–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.F.; Huang, Y.C.; Lee, M.C.; Wang, T.J.; Tung, H.H.; Wu, M.P. Self-efficacy, self-care behavior, anxiety, and depression in Taiwanese with type 2 diabetes: A cross-sectional survey. Nur.s Health Sci. 2013, 15, 213–219. [Google Scholar] [CrossRef]
- Li, S.Y. The relationships among self-efficacy, social support, and self-care behavior in the elderly patients with chronic pain (a STROBE-compliant article). Medicine 2021, 100, e24554. [Google Scholar] [CrossRef]
- Czyz, E.K.; Bohnert, A.S.; King, C.A.; Price, A.M.; Kleinberg, F.; Ilgen, M.A. Self-efficacy to avoid suicidal action: Factor structure and convergent validity among adults in substance use disorder treatment. Suicide Life Threat Behav. 2014, 44, 698–709. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Lu, Y.; Sun, J.; Huang, G.; Gong, Y.; Zhang, B.; Chen, Z.; Zhang, X.; Huang, Y.; Zeng, X. Comparison of Effects and Brain Imaging Mechanisms of Acupuncture and Paroxetine for Depressive Patients with Suicidal Ideation: Study Protocol of a 20-Week Clinical Trial; Research Square: Durham, NC, USA, 2023. [Google Scholar]
- Andover, M.S.; Schatten, H.T.; Morris, B.W.; Holman, C.S.; Miller, I.W. An intervention for nonsuicidal self-injury in young adults: A pilot randomized controlled trial. J. Consult. Clin. Psychol. 2017, 85, 620–631. [Google Scholar] [CrossRef]
- Horváth, L.O.; Győri, D.; Komáromy, D.; Mészáros, G.; Szentiványi, D.; Balázs, J. Nonsuicidal Self-Injury and Suicide: The Role of Life Events in Clinical and Non-Clinical Populations of Adolescents. Front. Psychiatry 2020, 11, 370. [Google Scholar] [CrossRef]
- Karnick, A.T.; Fergerson, A.K.; Caulfield, N.M.; Buerke, M.; Albanese, B.J.; Schmidt, N.B.; Capron, D.W. Toward an integrative model of transdiagnostic risk factors and suicide: A network comparison of psychiatric outpatients. J. Psychiatr. Res. 2022, 154, 252–260. [Google Scholar] [CrossRef]
- Bäumler, P.; Zhang, W.; Stübinger, T.; Irnich, D. Acupuncture-related adverse events: Systematic review and meta-analyses of prospective clinical studies. BMJ Open 2021, 11, e045961. [Google Scholar] [CrossRef]
- Joe, S.; Canetto, S.S.; Romer, D. Advancing prevention research on the role of culture in suicide prevention. Suicide Life Threat Behav. 2008, 38, 354–362. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Study/Country/Study Design | Sample Size (Included → Analyzed) | Clinical Condition (Diagnostic Criteria) | Intervention | Treatment Duration (f/u) | Results |
|---|---|---|---|---|---|
| Wang (2014)/China/RCT [35] | 61 (20:21:20) → 55 (19:16:20) | Depressive episode (ICD), 35 ≥ HAMD-24 > 8 | TG1: EA + placebo pill; TG2: EA + SSRI; CG1: sham EA + SSRI | 6 weeks (4-week post-treatment) | 1. CSRS |
| Yang (2014) and Yang et al. (2020)/China/CCT [36,42] | 60 (35:25) → 55 (32:23) | Depressive episode (ICD), HAMD-24 ≥ 20 | TG: EA; CG: SSRI | 8 weeks (4-week post-treatment) | 1. CSRS |
| Li et al. (2018)/China/RCT [37] | 93 (31:31:31) → 83 (29:27:27) | Post-stroke depression (CCMD-3) | TG1: ROC + AA (magnetotherapy); TG2: ROC + AA (vaccaria seed); CG: ROC for stroke | 4 weeks (4-week. post-treatment) | 1. Item 3 of HAMD-17 (suicide) |
| Jin et al. (2019)/China/Before–after study [38] | 21→21 | Depression with suicidal ideation (CPG of depression by CMA psychiatric branch in 2015) | Acupuncture | 3 months | 1. CER (reduction in HAMD score); 2. Number of patients with suicidal ideation; 3. BSSI |
| Pirnia et al. (2019)/Iran/single-case experimental study [39] | 1 | Major depression with suicidal ideation, heroin abuse, and three occurrences of suicide attempts (NR) | AA + methadone | 4 weeks | 1. Salivary cortisol (unclear unit and the timing of sampling); 2. Suicidal ideation (unclear assessment tool) |
| Pirnia et al. (2019)/Iran/RCT [40] | 24 (12:12) → 24 (12:12) | PDD (dysthymia) with suicidal ideation (DSM-5) | TG: AA + methadone; CG: Sham AA + methadone | 4 weeks | 1. Salivary cortisol sampled at random times among the three meals (unclear unit); 2. BSSI |
| Pirnia et al. (2020)/Iran/single-case experimental study [41] | 1 | Prostate carcinoma with dysthymic disorder and suicidal ideation (SCID) | AA + ROC | 4 weeks | 1. BDI; 2. BSSI; 3. Salivary cortisol in morning (unclear unit) |
| Li et al. (2021)/China/RCT [43] | 90 (45:45) → 90 (45:45) | Mild and moderate depression (ICD-10), HAMD > 7 | TG: EA + MT + ROC; CG: EA + ROC | 1 month | 1. NGASR |
| RCTs | Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Result | Overall Bias | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wang (2014) [35] | Low risk | Some concerns | Low risk | Low risk | Some concerns | Some concerns | ||||||||||
| Li et al. (2018) [37] | Low risk | Some concerns | Some concerns | High risk | Some concerns | High risk | ||||||||||
| Pirnia et al. (2019) [40] | Some concerns | Some concerns | Low risk | Low risk | Some concerns | Some concerns | ||||||||||
| Li et al. (2021) [43] | Some concerns | Some concerns | Low risk | High risk | Some concerns | High risk | ||||||||||
| CCTs | Selection bias due to the selection of inappropriate comparison target group | Selection bias due to inappropriate intervention or inappropriate selection of exposure group or patient group | Selection bias due to inappropriate confounder confirmation and consideration | Performance bias due to inappropriate intervention or inappropriate exposure measurement | Confirmation bias due to inappropriate blinding of assessors | Confirmation bias due to inappropriate outcome assessment methods | Attrition bias due to inappropriate handling of incomplete data | Reporting bias due to selective outcome reporting | ||||||||
| Yang (2014) and Yang et al. (2020) [36,42] | Low risk | High risk | High risk | Low risk | Low risk | Low risk | Unclear | Low risk | ||||||||
| Before–after studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | ||||
| Jin et al. (2019) [38] | Yes | Yes | Yes | CD | No | Yes | Yes | No | Yes | Yes | Yes | NA | ||||
| Study | Intervention | Acupoint | Depth of Insertion | Response Sought | Needle Stimulation | Needle Retention Time | Needle Type | Practitioner Background | Frequency (Treatment Duration)/Number of Sessions | Concurrent Treatment |
|---|---|---|---|---|---|---|---|---|---|---|
| Wang (2014) [35] | TG1: EA + placebo pill; TG2: EA + SSRI; CG1: placebo EA + SSRI | ST36, SP6, PC6, LR3, HT7 (additional 2–3 additional points based on clinical symptoms) | 0.5–0.8 cun | De qi | 1–50 Hz, disperse-dense waves, −10 mA depending on the participant’s comfort level | 30 min | 0.30 × 25 mm and 0.30 × 40 mm | NR | 3 sessions per week (6 weeks)/18 | SSRI (escitalopram) |
| Yang (2014) and Yang et al. (2020) [36,42] | TG: EA; CG: SSRI | GV20, EX-HN3 (additional 2–5 additional points based on TCM syndrome differentiation) | 0.5–0.8 cun | NR | 1–50 Hz, disperse-dense waves, 0.1–5 mA depending on the participant’s comfort level | 30 min | 0.32 mm | NR | 3 sessions per week (8 weeks)/24 | None |
| Li et al. (2018) [37] | TG1 and 2: ROC + AA; CG: ROC for stroke | (Unilateral) liver, heart, spleen, kidney, Shenmen, subcortex | NA | NA | Self-acupressure | 3 days | TG1: magnetotherapy TG2: vaccaria seed | NR | 3 sessions per week (4 weeks)/12 | ROC for stroke (e.g., blood pressure control, cerebral edema management, and rehabilitation training) |
| Jin et al. (2019) [38] | Acupuncture | (bilateral) SP4, PC6, BL62, SI3, GB41, TE5, LU7, KI6, BL15, BL18, BL23, CV12, ST25, CV6, CV4, KI3, HT7, LR3 | Back-su point: 1–1.2 cun; acupoints of the arms and legs: 0.5–1 cun (except for HT7: 0.3–0.5 cun); Abdominal acupoints: 1–1.2 cun | No De-qi | NR | 40 min | 0.25 × 40 mm | NR | 1st month: 5 sessions per week; 2nd and 3rd months: 3 sessions per week/44 | Infrared irradiation |
| Pirnia et al. (2019) [39] | AA + methadone | (Bilateral) sympathetic, Shenmen, kidney, liver, lung (NADA protocol) | 2–3 mm | NR | NR | NR | 0.25 × 13 mm | NR | 2 sessions per week (4 weeks)/8 | Methadone syrup 8 mg/d |
| Pirnia et al. (2019) [40] | TG: AA + methadone; CG: Sham AA + methadone | (Bilateral) sympathetic, Shenmen, kidney, liver, lung (NADA protocol) | 2–3 mm | NR | NR | NR | 0.25 × 13 mm | NR | 2 sessions per week (4 weeks)/8 | Methadone syrup 35 ± 0.3 cc/d |
| Pirnia et al. (2020) [41] | AA + ROC | (Bilateral) sympathetic, Shenmen, kidney, liver, lung (NADA protocol) | 2–3 mm | NR | NR | 30–45 min | 0.25 × 13 mm | a trained physician and an acupuncturist with a certification and five-year history of the treatment | 2 sessions per week (4 weeks)/8 | ROC (degarelix 40 mg/d, venlafaxine 225 mg/d, and methadone syrup 15 mg/d) |
| Li et al. (2021) [43] | TG: EA + MT + ROC; CG: EA + ROC | GV20, PC6, HT7, LI4, CV17, ST36, SP6 (optional: CV12, LR3, LR2, GB40) | NR | NR | 1.5 Hz, gradually increase the voltage until the skin next to the acupoints of the patient twitches slightly | 30 min | NR | NR | 1 session per day (1 month)/30 | MT + ROC (psychological support, health education, etc.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, C.-Y.; Lee, B. The Effectiveness and Safety of Acupuncture on Suicidal Behavior: A Systematic Review. Healthcare 2023, 11, 955. https://doi.org/10.3390/healthcare11070955
Kwon C-Y, Lee B. The Effectiveness and Safety of Acupuncture on Suicidal Behavior: A Systematic Review. Healthcare. 2023; 11(7):955. https://doi.org/10.3390/healthcare11070955
Chicago/Turabian StyleKwon, Chan-Young, and Boram Lee. 2023. "The Effectiveness and Safety of Acupuncture on Suicidal Behavior: A Systematic Review" Healthcare 11, no. 7: 955. https://doi.org/10.3390/healthcare11070955