
Sparing Is Caring: Hormonal Retreatment in Women with Recurrent Endometrial Cancer after Fertility Preservation Management—A Single Centre Retrospective Study

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
- GnRHa + LNG-IUD;
- MA 160 mg/day + LNG-IUD;
- MA 160 mg/day + LNG-IUD + MET 500 mg 3 times per day;
- Continuous oral progestin alone (MA 160 mg, Desogestrel 75 mcg).
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, S.; Gong, T.-T.; Liu, F.-H.; Jiang, Y.-T.; Sun, H.; Ma, X.-X.; Zhao, Y.-H.; Wu, Q.-J. Global, Regional, and National Burden of Endometrial Cancer, 1990–2017: Results from the Global Burden of Disease Study, 2017. Front. Oncol. 2019, 9, 1440. [Google Scholar] [CrossRef]
- Cancer Research UK. Uterine Cancer Incidence Statistics. 2019. Available online: https://www.cancerresearchuk.org/healthprofessional/cancer-statistics/statistics-by-cancer-type/uterine-cancer (accessed on 28 September 2021).
- Obermair, A.; Baxter, E.; Brennan, D.J.; McAlpine, J.N.; Muellerer, J.J.; Amant, F.; van Gent, M.D.J.M.; Coleman, R.L.; Westin, S.N.; Yates, M.S.; et al. Fertility-sparing treatment in early endometrial cancer: Current state and future strategies. Obstet. Gynecol. Sci. 2020, 63, 417–431. [Google Scholar] [CrossRef]
- Giuseppe, T.; Claudiana, O.; Raffaele, T.; Gianluca, R.D.; Antonio, P.; Ettore, C. Conservative treatment in early stage endometrial cancer: A review. Acta Biomed. 2019, 90, 405–410. [Google Scholar] [CrossRef]
- Soliman, P.T.; Oh, J.C.; Schmeler, K.M.; Sun, C.C.; Slomovitz, B.M.; Gershenson, D.M.; Burke, T.W.; Lu, K.H. Risk Factors for Young Premenopausal Women with Endometrial Cancer. Obstet. Gynecol. 2005, 105, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Okamura, Y.; Saito, F.; Takaishi, K.; Motohara, T.; Honda, R.; Ohba, T.; Katabuchi, H. Polycystic ovary syndrome: Early diagnosis and intervention are necessary for fertility preservation in young women with endometrial cancer under 35 years of age. Reprod. Med. Biol. 2016, 16, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, Y.; Taguchi, A.; Adachi, K.; Sato, M.; Kawata, A.; Tanikawa, M.; Sone, K.; Mori, M.; Nagasaka, K.; Matsumoto, Y.; et al. Polycystic Ovarian Morphology may be a Positive Prognostic Factor in Patients with Endometrial Cancer who Achieved Complete Remission after Fertility-Sparing Therapy with Progestin. Asian Pac. J. Cancer Prev. 2017, 18, 3111–3116. [Google Scholar] [CrossRef]
- Shao, Y.; Cheng, S.; Hou, J.; Zuo, Y.; Zheng, W.; Xia, M.; Mu, N. Insulin is an important risk factor of endometrial cancer among premenopausal women: A case-control study in China. Tumor Biol. 2016, 37, 4721–4726. [Google Scholar] [CrossRef]
- Rodolakis, A.; Scambia, G.; Planchamp, F.; Acien, M.; Sardo, A.D.S.; Farrugia, M.; Grynberg, M.; Pakiz, M.; Pavlakis, K.; Vermeulen, N.; et al. ESGO/ESHRE/ESGE Guidelines for the fertility-sparing treatment of patients with endometrial carcinoma. Hum. Reprod. Open 2023, 2023, hoac025. [Google Scholar] [CrossRef]
- Kyo, S.; Nakayama, K. Endometrial Cancer as a Metabolic Disease with Dysregulated PI3K Signaling: Shedding Light on Novel Therapeutic Strategies. Int. J. Mol. Sci. 2020, 21, 6073. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.Y.; Martinez-Outschoorn, U.; Schilder, R.J.; Kim, C.H.; Richard, S.D.; Rosenblum, N.G.; Johnson, J.M. Metformin as a Therapeutic Target in Endometrial Cancers. Front. Oncol. 2018, 8, 341. [Google Scholar] [CrossRef]
- Pino, I.; Iacobone, A.D.; Urbinati, A.M.V.; Di Giminiani, M.; Radice, D.; Guerrieri, M.E.; Preti, E.P.; Martella, S.; Franchi, D. Fertility-Sparing Treatment for Endometrial Cancer: Oncological and Obstetric Outcomes in Combined Therapies with Levonorgestrel Intrauterine Device. Cancers 2022, 14, 2170. [Google Scholar] [CrossRef]
- Mitsuhashi, A.; Habu, Y.; Kobayashi, T.; Kawarai, Y.; Ishikawa, H.; Usui, H.; Shozu, M. Long-term outcomes of progestin plus metformin as a fertility-sparing treatment for atypical endometrial hyperplasia and endometrial cancer patients. J. Gynecol. Oncol. 2019, 30, e90. [Google Scholar] [CrossRef] [PubMed]
- Gallos, I.D.; Yap, J.; Rajkhowa, M.; Luesley, D.M.; Coomarasamy, A.; Gupta, J.K. Regression, relapse, and live birth rates with fertility-sparing therapy for endometrial cancer and atypical complex endometrial hyperplasia: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2012, 207, 266.e1–266.e12. [Google Scholar] [CrossRef] [PubMed]
- Erkanli, S.; Ayhan, A. Fertility-Sparing Therapy in Young Women with Endometrial Cancer: 2010 Update. Int. J. Gynecol. Cancer 2010, 20, 1170–1187. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Bodurka, D.C.; Sun, C.C.; Levenback, C. Hormonal therapy for the management of grade 1 endometrial adenocarcinoma: A literature review. Gynecol. Oncol. 2004, 95, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Kesterson, J.P.; Fanning, J. Fertility-sparing treatment of endometrial cancer: Options, outcomes and pitfalls. J. Gynecol. Oncol. 2012, 23, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Westin, S.N.; Fellman, B.; Sun, C.C.; Broaddus, R.R.; Woodall, M.L.; Pal, N.; Urbauer, D.L.; Ramondetta, L.M.; Schmeler, K.M.; Soliman, P.T.; et al. Prospective phase II trial of levonorgestrel intrauterine device: Nonsurgical approach for complex atypical hyperplasia and early-stage endometrial cancer. Am. J. Obstet. Gynecol. 2021, 224, 191.e1–191.e15. [Google Scholar] [CrossRef]
- Janda, M.; Robledo, K.P.; Gebski, V.; Armes, J.E.; Alizart, M.; Cummings, M.; Chen, C.; Leung, Y.; Sykes, P.; McNally, O.; et al. Complete pathological response following levonorgestrel intrauterine device in clinically stage 1 endometrial adenocarcinoma: Results of a randomized clinical trial. Gynecol. Oncol. 2021, 161, 143–151. [Google Scholar] [CrossRef]
- Park, J.-Y.; Lee, S.-H.; Seong, S.J.; Kim, D.-Y.; Kim, T.-J.; Kim, J.W.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Bae, D.-S.; et al. Progestin re-treatment in patients with recurrent endometrial adenocarcinoma after successful fertility-sparing management using progestin. Gynecol. Oncol. 2013, 129, 7–11. [Google Scholar] [CrossRef]
- Wang, Y.; Yu, M.; Yang, J.X.; Cao, D.Y.; Yuan, Z.; Zhou, H.M.; Zhang, Y.; Li, L.; Shen, K.; Wu, H. Prolonged conservative treatment in patients with recurrent endometrial cancer after primary fertility-sparing therapy: 15-year experience. Int. J. Clin. Oncol. 2019, 24, 712–720. [Google Scholar] [CrossRef]
- Maggiore, U.L.R.; Martinelli, F.; Dondi, G.; Bogani, G.; Chiappa, V.; Evangelista, M.T.; Liberale, V.; Ditto, A.; Ferrero, S.; Raspagliesi, F. Efficacy and fertility outcomes of levonorgestrel-releasing intra-uterine system treatment for patients with atypical complex hyperplasia or endometrial cancer: A retrospective study. J. Gynecol. Oncol. 2019, 30, e57. [Google Scholar] [CrossRef]
- Yamagami, W.; Susumu, N.; Makabe, T.; Sakai, K.; Nomura, H.; Kataoka, F.; Hirasawa, A.; Banno, K.; Aoki, D. Is repeated high-dose medroxyprogesterone acetate (MPA) therapy permissible for patients with early stage endometrial cancer or atypical endometrial hyperplasia who desire preserving fertility? J. Gynecol. Oncol. 2018, 29, e21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-Y.; Kim, D.-Y.; Kim, J.-H.; Kim, Y.-M.; Kim, K.-R.; Kim, Y.-T.; Seong, S.J.; Kim, T.-J.; Kim, J.-W.; Kim, S.M.; et al. Long-term oncologic outcomes after fertility-sparing management using oral progestin for young women with endometrial cancer (KGOG 2002). Eur. J. Cancer 2013, 49, 868–874. [Google Scholar] [CrossRef]
- Tamauchi, S.; Kajiyama, H.; Utsumi, F.; Suzuki, S.; Niimi, K.; Sakata, J.; Mizuno, M.; Shibata, K.; Kikkawa, F. Efficacy of medroxyprogesterone acetate treatment and retreatment for atypical endometrial hyperplasia and endometrial cancer. J. Obstet. Gynaecol. Res. 2018, 44, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Legge, F.; Restaino, S.; Leone, L.; Carone, V.; Ronsini, C.; Di Fiore, G.L.M.; Pasciuto, T.; Pelligra, S.; Ciccarone, F.; Scambia, G.; et al. Clinical outcome of recurrent endometrial cancer: Analysis of post-relapse survival by pattern of recurrence and secondary treatment. Int. J. Gynecol. Cancer 2020, 30, 193–200. [Google Scholar] [CrossRef]
- Creasman, W.T.; Morrow, C.P.; Bundy, B.N.; Homesley, H.D.; Graham, J.E.; Heller, P.B. Surgical pathologic spread patterns of endometrial cancer. A gynecologic oncology group study. Cancer 1987, 60, 2035–2041. [Google Scholar] [CrossRef]
- Ronsini, C.; Mosca, L.; Iavarone, I.; Nicoletti, R.; Vinci, D.; Carotenuto, R.M.; Pasanisi, F.; Solazzo, M.C.; De Franciscis, P.; Torella, M.; et al. Oncological outcomes in fertility-sparing treatment in stage IA-G2 endometrial cancer. Front. Oncol. 2022, 12, 965029. [Google Scholar] [CrossRef]
- Thigpen, J.T.; Brady, M.F.; Alvarez, R.D.; Adelson, M.D.; Homesley, H.D.; Manetta, A.; Soper, J.T.; Given, F.T. Oral medroxyprogesterone acetate in the treatment of advanced or recurrent endometrial carcinoma: A dose-response study by the gynecologic oncology group. J. Clin. Oncol. 1999, 17, 1736–1744. [Google Scholar] [CrossRef]
- Falcone, F.; Maggiore, U.L.R.; Di Donato, V.; Perrone, A.M.; Frigerio, L.; Bifulco, G.; Polterauer, S.; Casadio, P.; Cormio, G.; Masciullo, V.; et al. Fertility-sparing treatment for intramucous, moderately differentiated, endometrioid endometrial cancer: A gynecologic cancer intergroup (GCIG) study. J. Gynecol. Oncol. 2020, 31, e74. [Google Scholar] [CrossRef]
- Casadio, P.; La Rosa, M.; Alletto, A.; Magnarelli, G.; Arena, A.; Fontana, E.; Fabbri, M.; Giovannico, K.; Virgilio, A.; Raimondo, D.; et al. Fertility Sparing Treatment of Endometrial Cancer with and without Initial Infiltration of Myometrium: A Single Center Experience. Cancers 2020, 12, 3571. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.; Azizia, M.M.; Hardiman, P.J. Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: A systematic review and meta-analysis. Hum. Reprod. Updat. 2014, 20, 748–758. [Google Scholar] [CrossRef]
- Franks, S. Polycystic Ovary Syndrome. New Engl. J. Med. 1995, 333, 853–861. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.P.; Cook, L.S.; Weiderpass, E.; Adami, H.-O.E.; Anderson, K.; Cai, H.; Cerhan, J.R.; Clendenen, T.V.; Felix, A.S.; Friedenreich, C.; et al. Infertility and incident endometrial cancer risk: A pooled analysis from the epidemiology of endometrial cancer consortium (E2C2). Br. J. Cancer 2015, 112, 925–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.-C.; Lin, C.-Y.; Chang, W.-C.; Shen, B.-J.; Chuang, C.-M. Increased Association Between Endometriosis and Endometrial Cancer. Int. J. Gynecol. Cancer 2015, 25, 447–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yates, M.S.; Coletta, A.M.; Zhang, Q.; Schmandt, R.E.; Medepalli, M.; Nebgen, D.; Soletsky, B.; Milbourne, A.; Levy, E.; Fellman, B.; et al. Prospective Randomized Biomarker Study of Metformin and Lifestyle Intervention for Prevention in Obese Women at Increased Risk for Endometrial Cancer. Cancer Prev. Res. 2018, 11, 477–490. [Google Scholar] [CrossRef] [Green Version]
- Bjørge, T.; Häggström, C.; Ghaderi, S.; Nagel, G.; Manjer, J.; Tretli, S.; Ulmer, H.; Harlid, S.; Rosendahl, A.H.; Lang, A.H.; et al. BMI and weight changes and risk of obesity-related cancers: A pooled European cohort study. Leuk. Res. 2019, 48, 1872–1885. [Google Scholar] [CrossRef]
- Onstad, M.A.; Schmandt, R.E.; Lu, K.H. Addressing the Role of Obesity in Endometrial Cancer Risk, Prevention, and Treatment. J. Clin. Oncol. 2016, 34, 4225–4230. [Google Scholar] [CrossRef]
- Pronin, S.M.; Novikova, O.V.; Andreeva, J.Y.; Novikova, E.G. Fertility-Sparing Treatment of Early Endometrial Cancer and Complex Atypical Hyperplasia in Young Women of Childbearing Potential. Int. J. Gynecol. Cancer 2015, 25, 1010–1014. [Google Scholar] [CrossRef] [PubMed]
- Pashov, A.I.; Tskhay, V.B.; Ionouchene, S.V. The combined GnRH-agonist and intrauterine levonorgestrel-releasing system treatment of complicated atypical hyperplasia and endometrial cancer: A pilot study. Gynecol. Endocrinol. 2012, 28, 559–561. [Google Scholar] [CrossRef] [PubMed]
- Dhar, K.K.; NeedhiRajan, T.; Koslowski, M.; Woolas, R.P. Is levonorgestrel intrauterine system effective for treatment of early endometrial cancer? Report of four cases and review of the literature. Gynecol. Oncol. 2005, 97, 924–927. [Google Scholar] [CrossRef]
- Gotlieb, W.H. Outcome of fertility-sparing treatment with progestins in young patients with endometrial cancer. Obstet. Gynecol. 2003, 102, 718–725. [Google Scholar] [CrossRef]
- Koskas, M.; Uzan, J.; Luton, D.; Rouzier, R.; Daraï, E. Prognostic factors of oncologic and reproductive outcomes in fertility-sparing management of endometrial atypical hyperplasia and adenocarcinoma: Systematic review and meta-analysis. Fertil. Steril. 2014, 101, 785–794.e3. [Google Scholar] [CrossRef] [PubMed]
- Piatek, S.; Michalski, W.; Sobiczewski, P.; Bidzinski, M.; Szewczyk, G. The results of different fertility-sparing treatment modalities and obstetric outcomes in patients with early endometrial cancer and atypical endometrial hyperplasia: Case series of 30 patients and systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Pal, N.; Broaddus, R.R.; Urbauer, D.L.; Balakrishnan, N.; Milbourne, A.; Schmeler, K.M.; Meyer, L.A.; Soliman, P.T.; Lu, K.H.; Ramirez, P.T.; et al. Treatment of Low-Risk Endometrial Cancer and Complex Atypical Hyperplasia with the Levonorgestrel-Releasing Intrauterine Device. Obstet. Gynecol. 2018, 131, 109–116. [Google Scholar] [CrossRef]
- Lago, V.; Marina, T.; Modrego, M.L.; Gil-Ibañez, B.; Rodriguez, J.R.; Domingo, J.; Minig, L.; Padilla-Iserte, P.; Sánchez, O.A.; Ferichola, M.S.; et al. Fertility sparing treatment in patients with endometrial cancer (FERT-ENC): A multicentric retrospective study from the Spanish Investigational Network Gynecologic Oncology Group (SPAIN-GOG). Arch. Gynecol. Obstet. 2022, 306, 821–828. [Google Scholar] [CrossRef]
- Kim, M.K.; Seong, S.J.; Kim, Y.S.; Song, T.; Yoon, B.S.; Jun, H.S.; Lee, Y.H. Combined medroxyprogesterone acetate/levonorgestrel–intrauterine system treatment in young women with early-stage endometrial cancer. Am. J. Obstet. Gynecol. 2013, 209, 358.e1–358.e4. [Google Scholar] [CrossRef]
- Kim, M.K.; Seong, S.J.; Kang, S.-B.; Bae, D.-S.; Kim, J.-W.; Nam, J.-H.; Lim, M.C.; Lee, T.S.; Kim, S.; Paek, J. Six months response rate of combined oral medroxyprogesterone/levonorgestrel-intrauterine system for early-stage endometrial cancer in young women: A Korean Gynecologic-Oncology Group Study. J. Gynecol. Oncol. 2019, 30, e47. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Wang, Y.-L.; Yu, L.; Hu, Q.; Ji, L.; Zhang, Y.; Liao, Q.-P. Metformin promotes progesterone receptor expression via inhibition of mammalian target of rapamycin (mTOR) in endometrial cancer cells. J. Steroid Biochem. Mol. Biol. 2011, 126, 113–120. [Google Scholar] [CrossRef]
- Park, J.-Y.; Seong, S.J.; Kim, T.-J.; Kim, J.W.; Bae, D.-S.; Nam, J.-H. Significance of body weight change during fertility-sparing progestin therapy in young women with early endometrial cancer. Gynecol. Oncol. 2017, 146, 39–43. [Google Scholar] [CrossRef]
- Mitsuhashi, A.; Kawasaki, Y.; Hori, M.; Fujiwara, T.; Hanaoka, H.; Shozu, M. Medroxyprogesterone acetate plus metformin for fertility-sparing treatment of atypical endometrial hyperplasia and endometrial carcinoma: Trial protocol for a prospective, randomised, open, blinded-endpoint design, dose-response trial (FELICIA trial). BMJ Open 2020, 10, e035416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Cao, D.; Yang, J.; Yu, M.; Zhou, H.; Cheng, N.; Wang, J.; Zhang, Y.; Peng, P.; Shen, K. Management of Recurrent Endometrial Cancer or Atypical Endometrial Hyperplasia Patients After Primary Fertility-Sparing Therapy. Front. Oncol. 2021, 11, 738370. [Google Scholar] [CrossRef]
- Vaugon, M.; Peigné, M.; Phelippeau, J.; Gonthier, C.; Koskas, M. IVF impact on the risk of recurrence of endometrial adenocarcinoma after fertility-sparing management. Reprod. Biomed. Online 2021, 43, 495–502. [Google Scholar] [CrossRef]
- Mutlu, L.; Manavella, D.D.; Gullo, G.; McNamara, B.; Santin, A.D.; Patrizio, P. Endometrial Cancer in Reproductive Age: Fertility-Sparing Approach and Reproductive Outcomes. Cancers 2022, 14, 5187. [Google Scholar] [CrossRef] [PubMed]
- Mosher, W.D.; Pratt, W.F. Fecundity and infertility in the United States: Incidence and trends. Fertil. Steril. 1991, 56, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L.; Simpson, J.L.; Driscoll, S.G.; Jovanovic-Peterson, L.; Van Allen, M.; Aarons, J.H.; Metzger, B.; Bieber, F.R.; Knopp, R.H.; Holmes, L.B.; et al. Incidence of Spontaneous Abortion among Normal Women and Insulin-Dependent Diabetic Women Whose Pregnancies Were Identified within 21 Days of Conception. New Engl. J. Med. 1988, 319, 1617–1623. [Google Scholar] [CrossRef]
- Stovall, T.G. Early Pregnancy Loss and Ectopic Pregnancy. In Berek and Novek’s Gynecology, 14th ed.; Berek, J.S., Ed.; Lip-Pincott Williams and Wilkins: Philadelphia, PA, USA, 2007; pp. 601–635. [Google Scholar]
- Chung, Y.S.; Woo, H.Y.; Lee, J.Y.; Park, E.; Nam, E.J.; Kim, S.; Kim, S.W.; Kim, Y.T. Mismatch repair status influences response to fertility-sparing treatment of endometrial cancer. Am. J. Obstet. Gynecol. 2021, 224, 370.e1–370.e13. [Google Scholar] [CrossRef]
- Puechl, A.; Spinosa, D.; Berchuck, A.; Secord, A.; Drury, K.; Broadwater, G.; Wong, J.; Whitaker, R.; Devos, N.; Corcoran, D.; et al. Molecular Classification to Prognosticate Response in Medically Managed Endometrial Cancers and Endometrial Intraepithelial Neoplasia. Cancers 2021, 13, 2847. [Google Scholar] [CrossRef] [PubMed]
- Cuccu, I.; D’Oria, O.; Sgamba, L.; De Angelis, E.; Golia D’Augè, T.; Turetta, C.; Di Dio, C.; Scudo, M.; Bogani, G.; Di Donato, V.; et al. Role of Genomic and Molecular Biology in the Modulation of the Treatment of Endometrial Cancer: Narrative Review and Perspectives. Healthcare 2023, 11, 571. [Google Scholar] [CrossRef]
- Cavaliere, A.F.; Perelli, F.; Zaami, S.; Piergentili, R.; Mattei, A.; Vizzielli, G.; Scambia, G.; Straface, G.; Restaino, S.; Signore, F. Towards Personalized Medicine: Non-Coding RNAs and Endometrial Cancer. Healthcare 2021, 9, 965. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | |||||
|---|---|---|---|---|---|
| Characteristic | All patients N = 61 | FS-Treatment N = 41 | FS-Retreatment N = 20 | p-Value b | |
| Age at diagnosis, years | 34.3 (5.6) | 34.7 (5.6) | 33.5 (5.2) | 0.36 | |
| Age at menarche, years, N = 54 c | 12.0 (1.6) | 12.4 (1.7) | 11.4 (1.1) | 0.02 | |
| Body Mass Index, N = 59 d | 24.6 (5.9) | 24.6 (6.1) | 24.4 (5.4) | 0.88 | |
| Follow-up, months | 54 | 45 | 72 | <0.01 | |
| PCOS | 10 (16.4) | 7 (17.1) | 3 (15.0) | 1.00 | |
| Hypertension | 3 (4.9) | 2 (4.9) | 1 (5.0) | 1.00 | |
| Diabetes | 1 (1.6) | 0 | 1 (5.0) | 0.33 | |
| Endometriosis | 11 (18.3) | 8 (20.0) | 3 (15.0) | 0.74 | |
| Infertility | 17 (27.9) | 11 (26.8) | 6 (30.0) | 1.00 | |
| Ovarian cancer | 10 (16.4) | 6 (14.6) | 4 (20.0) | 0.72 | |
| Smoke | Never | 42 (79.3) | 26 (76.5) | 16 (84.2) | |
| Former | 3 (5.7) | 3 (8.8) | 0 | ||
| Present | 8 (15.1) | 5 (14.7) | 3 (15.8) | 0.65 | |
| Group, N (%) a | |||||
|---|---|---|---|---|---|
| All Patients N = 26 | Hysterectomy N = 6 | FS-Retreatment N = 20 | p-Value b | ||
| Ongoing treatment at relapse | No Therapy | 7 (26.9) | 1 (16.7) | 6 (30.0) | |
| IUD | 7 (26.9) | 2 (33.3) | 5 (25.0) | ||
| IUD + Met | 3 (11.5) | 2 (33.3) | 1 (5.0) | ||
| Cyclic Progesterone | 8 (30.8) | 1 (16.7) | 7 (35.0) | ||
| Continuous Progestin | 1 (3.9) | 0 | 1 (5.0) | 0.46 | |
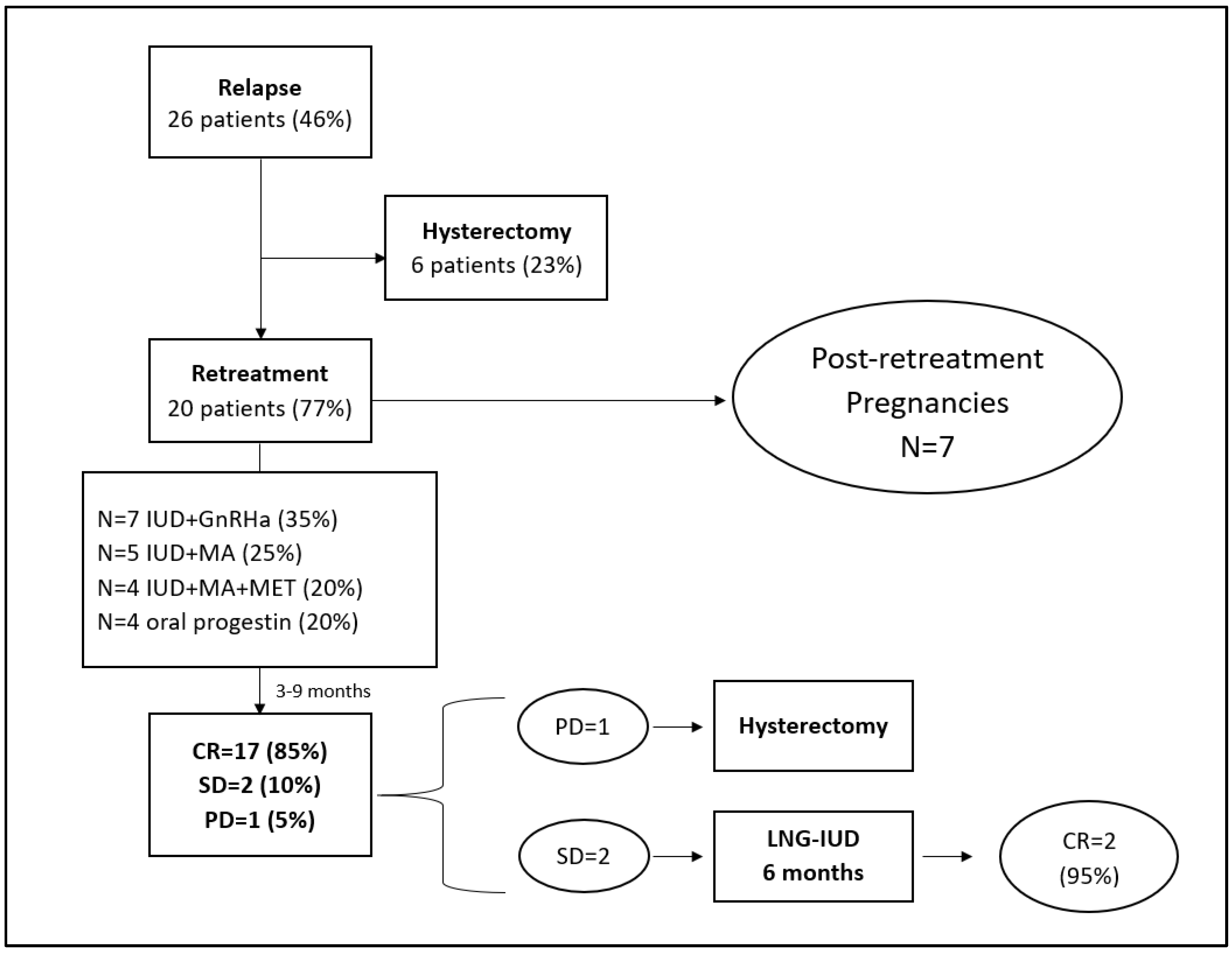
| Treatment of relapse | Hysterectomy | 6 (23.1) | 6 (100) | 0 | |
| IUD + GnRha | 7 (26.9) | 0 | 7 (35.0) | ||
| IUD + MA+Met | 5 (19.2) | 0 | 4 (20.0) | ||
| IUD + MA | 4 (15.4) | 0 | 5 (25.0) | ||
| Continuous Progestin | 4 (15.4) | 0 | 4 (20.0) | NA | |
| Ovarian stimulation before relapse | 7 (26.9) | 2 (33.3) | 5 (25.0) | 1.00 | |
| Group, N (%) a | ||||
|---|---|---|---|---|
| All Patients N = 61 | FS-Treatment N = 41 | FS-Retreatment N = 20 | p-Value b | |
| Try to conceive | 38 (62) | 24 (59) | 14 (70) | 0.83 |
| Infertility treatment | 21/38 (55) | 10/24 (42) | 11/14 (79) | 0.28 |
| Post-treatment pregnancy | 29/38 (76) | 22/24 (92) | 7/14 (50) | 0.30 |
| Live Birth | 19/38 (50) | 15/24 (63) | 4/14 (29) | 0.37 |
| Miscarriages | 10/29 (34) | 7/22 (32) | 3/7 (43) | 0.70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pino, I.; Di Giminiani, M.; Radice, D.; Vidal Urbinati, A.M.; Iacobone, A.D.; Guerrieri, M.E.; Preti, E.P.; Martella, S.; Franchi, D. Sparing Is Caring: Hormonal Retreatment in Women with Recurrent Endometrial Cancer after Fertility Preservation Management—A Single Centre Retrospective Study. Healthcare 2023, 11, 1058. https://doi.org/10.3390/healthcare11071058
Pino I, Di Giminiani M, Radice D, Vidal Urbinati AM, Iacobone AD, Guerrieri ME, Preti EP, Martella S, Franchi D. Sparing Is Caring: Hormonal Retreatment in Women with Recurrent Endometrial Cancer after Fertility Preservation Management—A Single Centre Retrospective Study. Healthcare. 2023; 11(7):1058. https://doi.org/10.3390/healthcare11071058
Chicago/Turabian StylePino, Ida, Maria Di Giminiani, Davide Radice, Ailyn Mariela Vidal Urbinati, Anna Daniela Iacobone, Maria Elena Guerrieri, Eleonora Petra Preti, Silvia Martella, and Dorella Franchi. 2023. "Sparing Is Caring: Hormonal Retreatment in Women with Recurrent Endometrial Cancer after Fertility Preservation Management—A Single Centre Retrospective Study" Healthcare 11, no. 7: 1058. https://doi.org/10.3390/healthcare11071058