Validation of the Opening Minds Scale for Health Care Providers (OMS-HC): Factor Structure and Psychometric Properties of the Brazilian Version

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Background
2.2. Participants
2.3. Measures
2.4. Statistical Analysis
2.5. Ethical Aspects
3. Results
3.1. Sociodemographic Characteristics
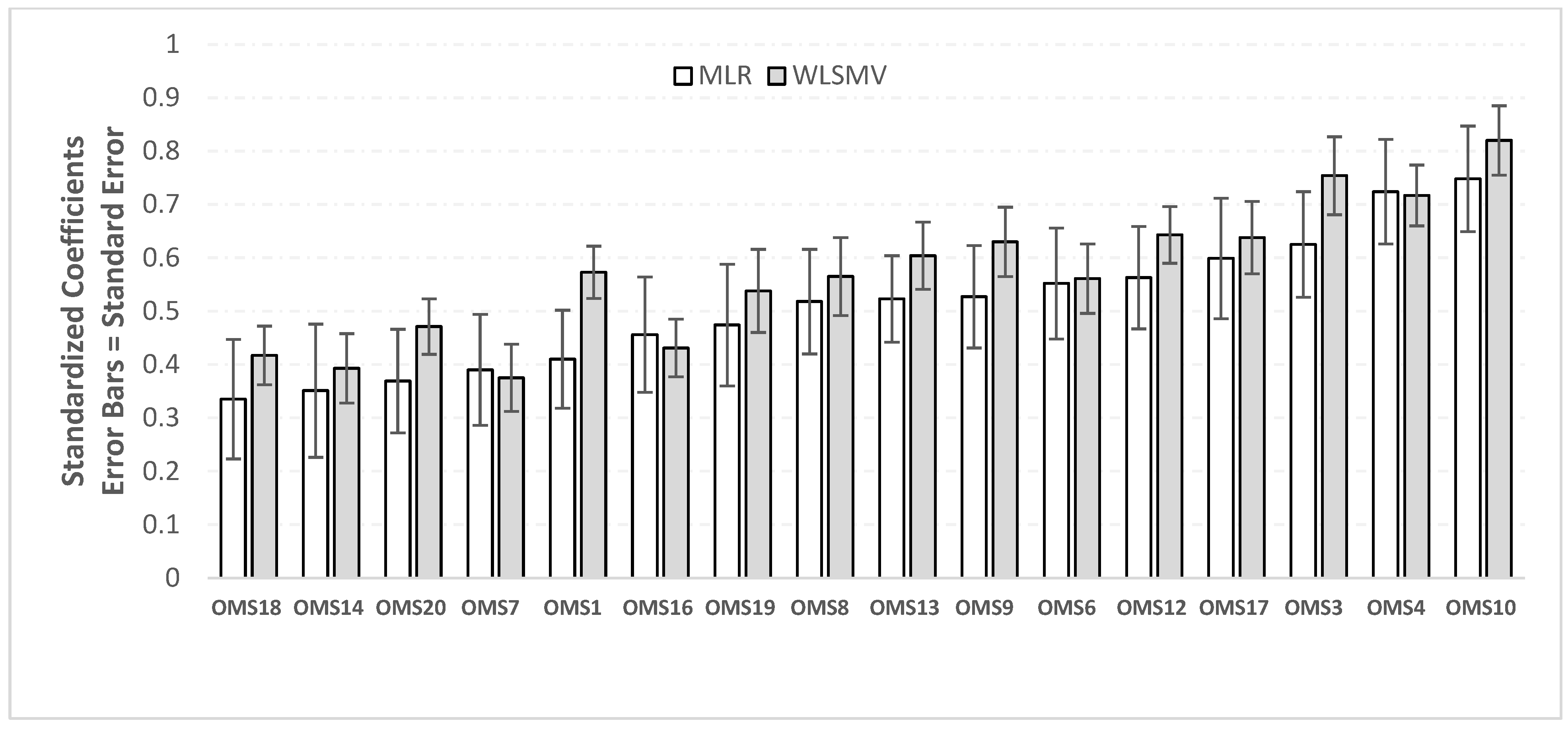
3.2. Validity
3.3. Individual Item Analysis
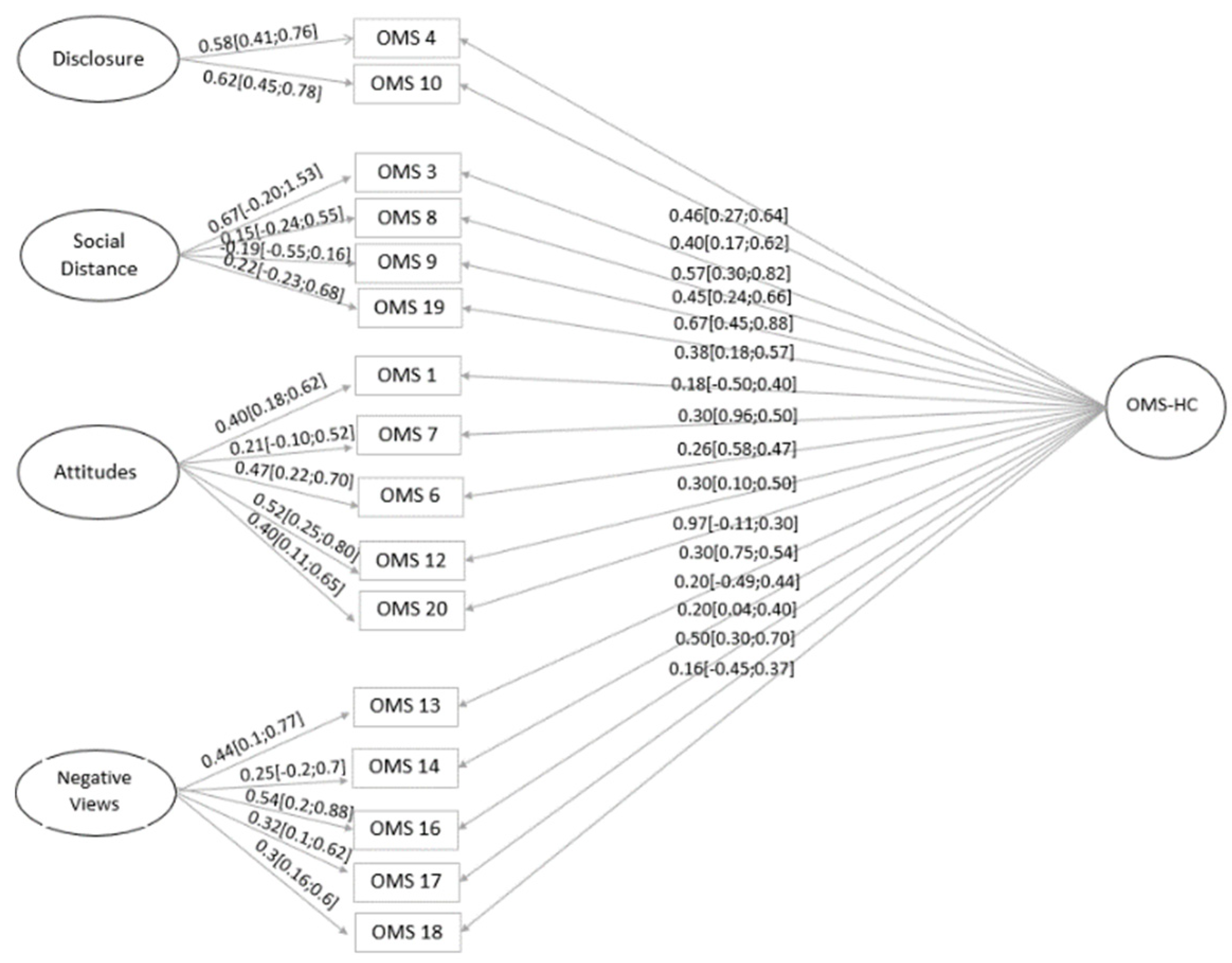
3.4. Dimensionality
3.5. The Bifactor Model

{kind=link}
{kind=link}
| 4 Factors | 4 Factors | 5 Factors | 1 Factor | 5 Factors | |
|---|---|---|---|---|---|
| CFA | CFA | Bifactor | CFA | Second-Order | |
| 20 Items | 16 Items | 16 Items | 16 Items | 16 Items | |
| Chi-square | 222.4 | 133.6 | 117.6 | 199.9 | 132.4 |
| df | 164 | 98 | 89 | 104 | 100 |
| p-value | 0.0016 | 0.0098 | 0.0229 | <0.0001 | 0.0166 |
| RMSEA | 0.043 | 0.043 | 0.041 | 0.069 | 0.041 |
| RMSEA CI | 0.027–0.056 | 0.022–0.061 | 0.016–0.059 | 0.054–0.083 | 0.018–0.059 |
| CFI | 0.837 | 0.878 | 0.902 | 0.671 | 0.889 |
| TLI | 0.811 | 0.85 | 0.868 | 0.62 | 0.866 |
| SRMR | 0.067 | 0.06 | 0.057 | 0.076 | 0.06 |
| AIC | 10,514.842 | 8356.547 | 8353.067 | 8435.081 | 8352.578 |
| BIC | 10,730.521 | 8533.012 | 8558.942 | 8591.938 | 8522.507 |
| SABIC | 10,521.446 | 8361.951 | 8359.371 | 8439.884 | 8357.781 |
3.6. Reliability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Item–Total Correlation | Cronbach’s Alpha | |
|---|---|---|
| 1. I am more comfortable helping a person who has a physical illness than I am helping a person who has a mental illness. | 0.254 | 0.721 |
| 2. If a person with a mental illness complains of physical symptoms (e.g., nausea, back pain or headache), I would likely attribute this to their mental ilness. | 0.164 | 0.726 |
| 3. If a colleague with whom I work told me they had a managed mental illness, I would be as willing to work with him/her. | 0.407 | 0.708 |
| 4. If I were under treatment for a mental illness I would not disclose this to any of my colleagues. | 0.407 | 0.707 |
| 5. I would be more inclined to seek help for a mental illness if my treating health care provider was not associated with my workplace. | 0.169 | 0.732 |
| 6. I would see myself as weak if I had a mental illness and could not fix it myself. | 0.332 | 0.713 |
| 7. I would be reluctant to seek help if I had a mental illness. | 0.329 | 0.714 |
| 8. Employers should hire a person with a managed mental illness if he/she is the best person for the job. | 0.382 | 0.712 |
| 9. I would still go to a physician if I knew that the physician had been treated for a mental illness. | 0.416 | 0.707 |
| 10. If I had a mental illness, I would tell my friends. | 0.422 | 0.706 |
| 11. It is the responsibility of health care providers to inspire hope in people with mental illnes | 0.164 | 0.727 |
| 12. Despite my professional beliefs, I have negative reactions towards people who have mental illness. | 0.362 | 0.711 |
| 13. There is little I can do to help people with mental illness. | 0.359 | 0.711 |
| 14. More than half of people with mental illness don’t try hard enough to get better. | 0.269 | 0.719 |
| 15. People with mental illness seldom pose a risk to the public. | 0.035 | 0.737 |
| 16. The best treatment for mental illness is medication. | 0.247 | 0.721 |
| 17. I would not want a person with a mental illness, even if it were appropriately managed, to work with children. | 0.430 | 0.705 |
| 18. Health care providers do not need to be advocates for people with mental illness. | 0.213 | 0.724 |
| 19. I would not mind if a person with a mental illness lived next door to me. | 0.340 | 0.713 |
| 20. I struggle to feel compassion for a person with a mental ilness. | 0.218 | 0.722 |


Appendix B. Short Explanation of Ancillary Indices That Are Calculated from the Bifactor Model
Appendix B.1. Measures Related to Dimensionality
Appendix B.2. Model-Based Reliability Measures
References
- World Health Organization. Cross-national comparisons of the prevalences and correlates of mental disorders. Bull. WHO 2000, 78, 413–426. [Google Scholar]
- Crisp, A.H.; Gelder, A.G.; Rix, S.; Meltzer, H.I.; Rowlands, O.J. Stigmatisation of people with mental illnesses. Br. J. Psychiatry 2000, 177, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Link, B.G.; Phelan, J.C.; Bresnahan, M.; Stueve, A.; Pescosolido, B.A. Public conceptions of mental illness: Labels, causes, dangerousness and social distance. Am. J. Public Health 1999, 89, 1328–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, J.C.; Link, B.G. The growing belief that people with mental illnesses are violent: The role of the dangerousness criterion for civil commitment. Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 7–12. [Google Scholar] [CrossRef]
- Stuart, H.; Arboleda-Florez, J.; Sartorius, N. Paradigms Lost: Fighting Stigma and the Lessons Learned; Oxford University Press Inc.: New York, NY, USA, 2012. [Google Scholar]
- Corrigan, P.; Watson, A. Understanding the impact of stigma on people with mental illness. World Psychiatry 2002, 1, 16–20. [Google Scholar]
- Sartorius, N. Stigma and mental health. Lancet 2007, 370, 810–811. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J. Contesting stigma and contested emotions: Personal experience and public perception of specific phobias. Soc. Sci. Med. 2005, 61, 2155–2164. [Google Scholar] [CrossRef] [PubMed]
- Fraser, K.; Gallop, R. Nurses’ confirming/disconfirming responses to patients diagnosed with borderline personality disorder. Arch. Psychiatr. Nurs. 1993, 7, 336–341. [Google Scholar] [CrossRef]
- Corrigan, P.W. How stigma interferes with mental health care. Am. Psychol. 2004, 59, 614–625. [Google Scholar] [CrossRef] [Green Version]
- Corrigan, P.; Markowitz, F.E.; Watson, A.; Rowan, D.; Kubiak, M.A. An attribution model of public discrimination towards persons with mental illness. J. Health Soc. Behav. 2003, 44, 162–179. [Google Scholar] [CrossRef] [Green Version]
- Rüsch, N.; Angermeyer, M.C.; Corrigan, P.W. Mental illness stigma: Concepts, consequences, and initiatives to reduce stigma. Eur. Psychiatry 2005, 20, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Andrade, L.H.; Wang, Y.P.; Andreoni, S.; Silveira, C.M.; Alexandrino-Silva, C. Mental disorders in megacities: Findings from the São Paulo megacity mental health survey, Brazil. PLoS ONE 2012, 7, e31879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Boekel, L.C.; Brouwers, E.P.; Wan Weeghel, J.; Garretsen, H.F. Stigma among health professionals towards patients with substance use disorders and its consequences for healthcare delivery: Systematic review. Drug Alcohol Depend. 2013, 13, 23–35. [Google Scholar] [CrossRef]
- Mestdagh, A.; Hansen, B. Stigma in patients with schizophrenia receiving community mental health care: A review of qualitative studies. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 79–87. [Google Scholar] [CrossRef]
- Abdullah, T.; Brown, T.L. Mental illness stigma and ethnocultural beliefs, values, and norms: An integrative review. Clin. Psychol. Rev. 2011, 31, 934–948. [Google Scholar] [CrossRef] [PubMed]
- Kawar, A. Mental Illness and Stigma: Has Psychiatry Done more Harm than Good? Indian J. Psychol. Med. 2015, 37, 181–183. [Google Scholar] [CrossRef] [Green Version]
- Paim, J.; Travassos, C.; Almeida, C.; Bahia, L.; Macinko, J. O sistema de saúde brasileiro: História, avanços e desafios. Lancet 2011, 6736, 60054–60058. [Google Scholar]
- Costa, G.D.; Cotta, R.M.; Ferreira, M.L.; Reis, J.R.; Franceschini, S.C. Saúde da família: Desafios no processo de reorientação do modelo assistencial. Rev. Bras. Enferm. 2009, 62, 113–128. [Google Scholar] [CrossRef] [Green Version]
- Soares, R.G.; Nery, F.C.; Silveira, P.S.; Noto, A.R.; Ronzani, T.M. A mensuração do estigma internalizado: Revisão sistemática da literatura. Psicol. Em Estud. 2011, 16, 635–645. [Google Scholar] [CrossRef] [Green Version]
- Semerau, M.; Evans-lacko, S.; Koschorke, M.; Ashenafi, L.; Thornicroft, G. Stigma and discrimination related to mental illness in low- and middle- income countries. Epidemiol. Psychiatr. Sci. 2015, 24, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Hanssom, L.; Jormfeldt, H.; Svedberg, P.; Svensson, B. Mental health professionals’ attitudes towards people with mental illness: Do they differ from attitudes held by people with mental illness? Int. J. Soc. Psychiatr. 2013, 59, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Modgill, G.; Patten, S.B.; Knaak, S.; Kassam, A.; Szeto, A.C. Opening minds stigma scale for health care providers (OMS-HC): Examination of psychometric properties and responsiveness. BMC Psychiatry 2014, 14, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patten, S.B.; Remillard, A.; Phillips, L.; Modgill, G.; Szeto, A.C.; Kassam, A.; Gardner, D.M. Effectiveness of contact-based education for reducing mental illness-related stigma in pharmacy students. BMC Med. Educ. 2012, 12, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassam, A.; Papish, A.; Modgill, G.; Patten, S. The development and psychometric properties of a new scale to measure mental illness related stigma by health care providers: The opening minds scale for Health Care Providers (OMS-HC). BMC Psychiatr. 2012, 12, 62. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.; Ong, H.L.; Seow, E.; Chua, B.Y.; Abdin, E.; Samari, E.; Teh, W.L.; Chong, S.A.; Subramaniam, M. Stigma towards mental illness among medical and nursing students in Singapore: A cross-sectional study. BMJ Open 2017, 7, e018099. [Google Scholar] [CrossRef] [Green Version]
- Destrebecq, A.; Ferrara, P.; Frattini, L.; Pittella, F.; Rossano, G.; Striano, G.; Terzoni, S.; Gambini, O. The Italian Version of the Opening Minds Stigma Scale for Healthcare Providers: Validation and Study on a Sample of Bachelor Students. Community Ment. Health J. 2018, 54, 66–72. [Google Scholar] [CrossRef]
- Sapag, J.C.; Klabunde, R.; Villarroel, L.; Velasco, P.R.; Álvarez, C.; Parra, C.; Bobbili, S.J.; Mascayano, F.; Bustamante, I.; Alvarado, R.; et al. Validation of the Opening Minds Scale and patterns of stigma in Chilean primary health care. PLoS ONE 2019, 14, e0221825. [Google Scholar] [CrossRef] [Green Version]
- Carrara, B.S.; Ventura, C.A.; Costa, S.G. Cultural adaptation of the opening minds scale for health care providers (OMS-HC) for Brazil. Acta Sci. Health Sci. 2022, 45, e54524. [Google Scholar] [CrossRef]
- Morais, J.F. Validade e confiabilidade de escalas multi itens. Estima 2004, 2, 42–45. [Google Scholar]
- Pasquali, L. Psicometria. Rev. Esc. Enferm. USP 2009, 43, 992–999. [Google Scholar] [CrossRef]
- Gabbidon, J.; Clement, S.; van Nieuwenhuizen, A.; Kassam, A.; Brohan, E.; Norman, I.; Thornicroft, G. Mental Illness: Clinicians’ Attitudes (MICA) Scale—Psychometric properties of a version for healthcare students and professionals. Psychiatry Res. 2013, 206, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Muthén, B.; du Toit, S.H.; Spisic, D. Robust inference using weighted least squares and quadratic estimating equations in latent variable modeling with categorical and continuous outcomes. Psychometrika 1997, 75, 1–27. [Google Scholar]
- Browne, M.W. An overview of analytic rotation in exploratory factor analysis. Multivar. Behav. Res. 2011, 36, 111–150. [Google Scholar] [CrossRef]
- Hayton, J.C.; Allen, D.G.; Scarpello, V. Factor retention decisions in exploratory factor analysis: A tutorial on parallel analysis. Organ. Res. Methods 2004, 7, 191–205. [Google Scholar] [CrossRef]
- Hu, L.; Peter, M.B. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Tofighi, D.; Enders, C.K. Identifying the correct number of classes in a growth mixture model. Adv. Latent Var. Mix. Model. 2007, 2007, 317–341. [Google Scholar]
- Rodriguez, A.; Steven, P.R.; Mark, G.H. Evaluating bifactor models: Calculating and interpreting statistical indices. Psychol. Methods 2016, 21, 137. [Google Scholar] [CrossRef]
- Arminger, G.; Ronald, J.S. Pseudo maximum likelihood estimation and a test for misspecification in mean and covariance structure models. Psychometrika 1989, 54, 409–425. [Google Scholar] [CrossRef]
- Reise, S.P. The rediscovery of bifactor measurement models. Multivar. Behav. Res. 2012, 47, 667–696. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Őri, D.; Rózsa, S.; Szocsics, P.; Simon, L.; Purebl, G.; Győrffy, Z. Factor structure of The Opening Minds Stigma Scale for Health Care Providers and psychometric properties of its Hungarian version. BMC Psychiatry 2020, 20, 504. [Google Scholar] [CrossRef] [PubMed]
- Hocking, B. Reducing mental illness stigma and discrimination—Everybody’s business. Med. J. 2003, 178, S47–S48. [Google Scholar] [CrossRef] [PubMed]
- Kassam, A.; Glozier, N.; Leese, M.; Henderson, C.; Thornicroft, G. Development and responsiveness of a scale to measure clinicians’ attitudes to people with mental illness (medical student version). Acta Psychiatr. Scand. 2010, 122, 153–161. [Google Scholar] [CrossRef] [PubMed]
| N | % | ||
|---|---|---|---|
| Total | 195 | 100.0% | |
| Gender | Female | 172 | 88.2% |
| Male | 23 | 11.8% | |
| Occupation/Function in the Unit (grouped) | Nurse | 15 | 7.7% |
| Nursing Assistant | 39 | 20.0% | |
| Nurse Technician | 11 | 5.6% | |
| Community Wealth Workers | 88 | 45.1% | |
| Other | 42 | 21.5% | |
| Postgraduate | Yes | 10 | 5.1% |
| No | 185 | 94.9% | |
| Know someone close to you with a mental disorder | Yes | 177 | 91.2% |
| No | 17 | 8.8% | |
| Have you ever cared for/treated someone with a mental disorder | Yes | 130 | 67.4% |
| No | 63 | 32.6% | |
| Age (Mean/SD) | 44.9 | 9.5 | |
| Questionnarie time in minutes (Mean/SD) | 10.4 | 10.9 | |
| Time working in years (Mean/SD) | 18.1 | 9.4 | |
| Time working in the health unit in months (Mean/SD) | 83.1 | 59.5 | |
| Disclosure | Social Distance | Attitude | Negative View | |
|---|---|---|---|---|
| 4. If I were under treatment for a mental illness I would not disclose this to any of my colleagues. | 0.678 * | 0.206 * | −0.118 * | −0.012 |
| 10. If I had a mental illness, I would tell my friends. | 0.847 * | −0.08 | 0.110 * | 0.085 |
| 3. If a colleague with whom I work told me they had a managed mental illness, I would be as willing to work with him/her. | 0.294 * | 0.510 * | 0.024 | 0.139 * |
| 8. Employers should hire a person with a managed mental illness if he/she is the best person for the job. | −0.02 | 0.645 * | 0.108 | 0.005 |
| 9. I would still go to a physician if I knew that the physician had been treated for a mental illness. | 0.157 * | 0.495 * | 0.004 | 0.169 * |
| 19. I would not mind if a person with a mental illness lived next door to me. | 0.013 | 0.462 * | 0.213 * | 0.057 |
| 7. I would be reluctant to seek help if I had a mental illness. | 0.135 | 0.220 * | 0.407 * | −0.033 |
| 1. I am more comfortable helping a person who has a physical illness than I am helping a person who has a mental illness. | 0.035 | 0.062 | 0.276 * | 0.089 |
| 6. I would see myself as weak if I had a mental illness and could not fix it myself. | 0.085 | 0.092 | 0.498 * | 0.04 |
| 12. Despite my professional beliefs, I have negative reactions towards people who have mental illness. | 0.159 * | 0.108 | 0.541 * | −0.001 |
| 20. I struggle to feel compassion for a person with a mental ilness. | −0.023 | −0.044 | 0.588 * | 0.074 |
| 13. There is little I can do to help people with mental illness. | 0.277 * | −0.163 * | 0.088 | 0.605 * |
| 14. More than half of people with mental illness don’t try hard enough to get better. | −0.148 | 0.041 | 0.248 * | 0.375 * |
| 16. The best treatment for mental illness is medication. | −0.03 | 0.004 | 0.016 | 0.523 * |
| 17. I would not want a person with a mental illness, even if it were appropriately managed, to work with children. | 0.014 | 0.337 * | −0.166 * | 0.585 * |
| 18. Health care providers do not need to be advocates for people with mental illness. | 0.103 | 0.004 | 0.197 * | 0.260 * |
| Factors | Item | Bifactor | CFA Loadings | 1-Dim. CFA Loadings | Second-Order Factor Loadings | Bias | IECV | |
|---|---|---|---|---|---|---|---|---|
| Gen. Factor Loadings | Spec. Factor Loadings | |||||||
| Disclosure | 4 | 0.456 | 0.584 | 0.724 | 0.506 | 0.723 | 11% | 84% |
| 10 | 0.399 | 0.616 | 0.748 | 0.495 | 0.749 | 24% | 58% | |
| Social Distance | 3 | 0.561 | 0.665 | 0.625 | 0.486 | 0.624 | 13% | 62% |
| 8 | 0.454 | 0.152 | 0.518 | 0.322 | 0.519 | 29% | 76% | |
| 9 | 0.669 | −0.191 | 0.527 | 0.495 | 0.527 | 26% | 33% | |
| 19 | 0.376 | 0.224 | 0.474 | 0.36 | 0.475 | 4% | 10% | |
| Attitudes | 1 | 0.176 | 0.400 | 0.410 | 0.304 | 0.409 | 73% | 8% |
| 7 | 0.299 | 0.210 | 0.390 | 0.399 | 0.391 | 33% | 70% | |
| 6 | 0.263 | 0.467 | 0.552 | 0.397 | 0.552 | 51% | 75% | |
| 12 | 0.304 | 0.521 | 0.563 | 0.354 | 0.563 | 16% | 67% | |
| 20 | 0.097 | 0.377 | 0.369 | 0.156 | 0.369 | 61% | 61% | |
| Negative Views | 13 | 0.306 | 0.438 | 0.523 | 0.423 | 0.525 | 38% | 88% |
| 14 | 0.197 | 0.249 | 0.351 | 0.256 | 0.350 | 30% | 30% | |
| 16 | 0.200 | 0.536 | 0.456 | 0.29 | 0.456 | 45% | 79% | |
| 17 | 0.494 | 0.319 | 0.599 | 0.474 | 0.598 | 4% | 26% | |
| 18 | 0.161 | 0.309 | 0.335 | 0.297 | 0.335 | 84% | 94% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrara, B.S.; Sanches, M.; Bobbili, S.J.; de Godoy Costa, S.; de Sousa, Á.F.L.; de Souza, J.; Ventura, C.A.A. Validation of the Opening Minds Scale for Health Care Providers (OMS-HC): Factor Structure and Psychometric Properties of the Brazilian Version. Healthcare 2023, 11, 1049. https://doi.org/10.3390/healthcare11071049
Carrara BS, Sanches M, Bobbili SJ, de Godoy Costa S, de Sousa ÁFL, de Souza J, Ventura CAA. Validation of the Opening Minds Scale for Health Care Providers (OMS-HC): Factor Structure and Psychometric Properties of the Brazilian Version. Healthcare. 2023; 11(7):1049. https://doi.org/10.3390/healthcare11071049
Chicago/Turabian StyleCarrara, Bruna Sordi, Marcos Sanches, Sireesha Jennifer Bobbili, Simone de Godoy Costa, Álvaro Francisco Lopes de Sousa, Jacqueline de Souza, and Carla Aparecida Arena Ventura. 2023. "Validation of the Opening Minds Scale for Health Care Providers (OMS-HC): Factor Structure and Psychometric Properties of the Brazilian Version" Healthcare 11, no. 7: 1049. https://doi.org/10.3390/healthcare11071049