
“Breastfeeding at Night Is Awesome” Mothers’ Intentions of Continuation of Breastfeeding Extreme and Very Preterm Babies upon Discharge from a Kangaroo Mother Care Unit of a Tertiary Hospital in South Africa

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and Population
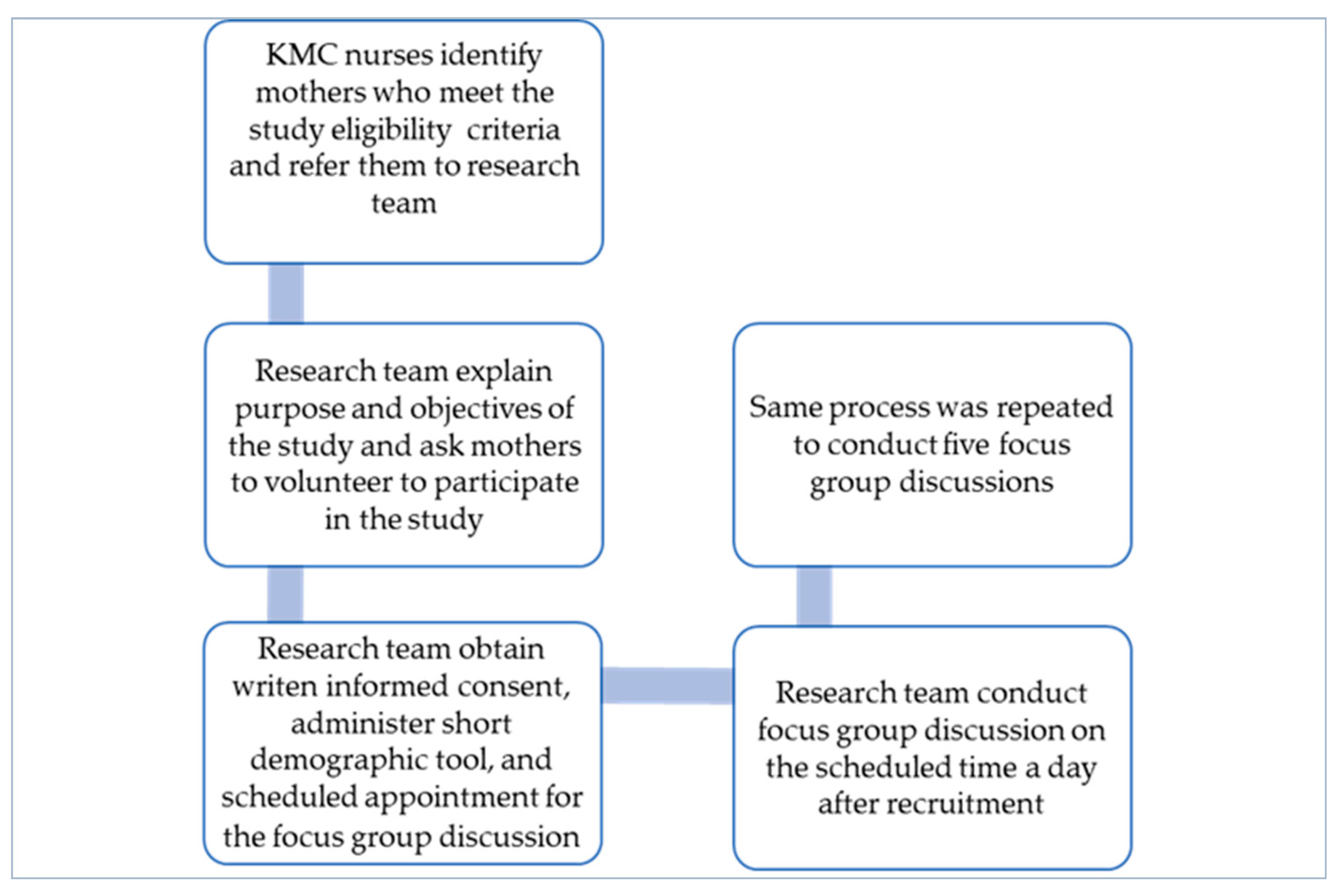
2.3. Data Collection, Tools, and Procedure
2.4. Ethical Considerations
2.5. Data Analysis
2.6. Rigour
3. Results
3.1. Sociodemographic Profile of Participants
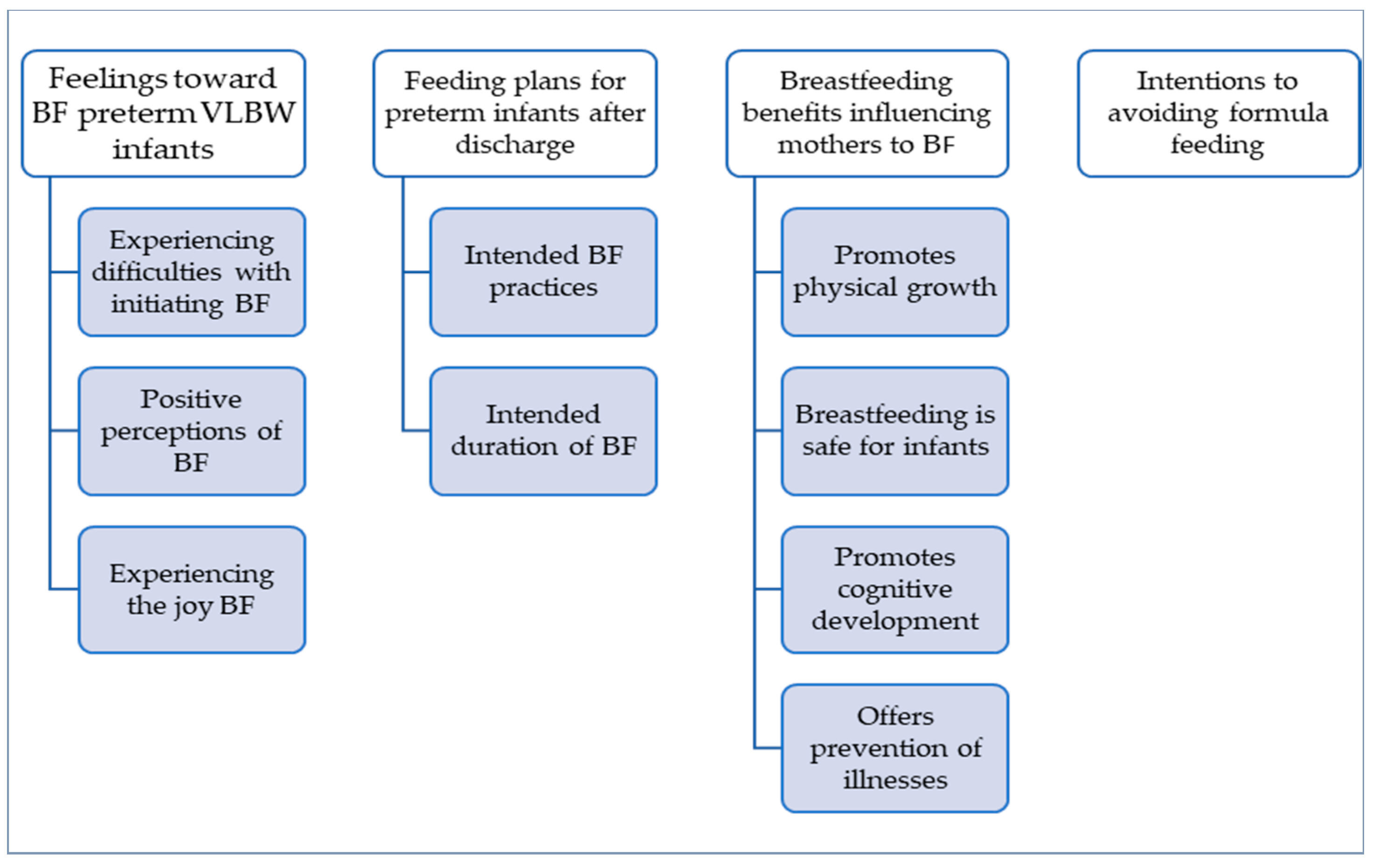
3.2. Themes
3.2.1. Feelings toward Breastfeeding VLBW Infants
3.2.2. Feeding Plans for Preterm Infants after Discharge
3.2.3. Breastfeeding Benefits Influencing Mothers to BF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bergh, A.M.; Arsalo, I.; Malan, A.F.; Patrick, M.; Pattinson, R.C.; Phillips, N. Measuring implementation progress in kangaroo mother care. Acta Paediatr. 2005, 94, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Souza, R.C.; Wolkers, P.C.B.; Pereira, L.A.; Romão, R.S.; Medeiros, E.S.; Ferreira, D.M.L.M.; Rinaldi, A.E.M.; Azevedo, V.M.G.O. The possible mediating relationship promoted by the self-efficacy of breastfeeding associated with the Kangaroo Method on indicators of exclusive breastfeeding. J. De Pediatr. 2022, 98, 540–544. [Google Scholar] [CrossRef] [PubMed]
- WHO. Protecting, Promoting and Supporting Breastfeeding: The Baby-Friendly Hospital Initiative for Small, Sick and Preterm Newborns; Report No.: 9240005641; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sharma, D.; Farahbakhsh, N.; Sharma, S.; Sharma, P.; Sharma, A. Role of kangaroo mother care in growth and breast-feeding rates in very low birth weight (VLBW) neonates: A systematic review. J. Matern. Neonatal Med. 2017, 32, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Flacking, R.; Tandberg, B.S.; Niela-Vilén, H.; Jónsdóttir, R.B.; Jonas, W.; Ewald, U.; Thomson, G. Positive breastfeeding experiences and facilitators in mothers of preterm and low birthweight infants: A meta-ethnographic review. Int. Breastfeed. J. 2021, 16, 1–17. [Google Scholar] [CrossRef]
- WHO. Guideline: Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Strobel, N.A.; Adams, C.; McAullay, D.R.; Edmond, K.M. Mother’s own milk compared with formula milk for feeding preterm or low birth weight infants: Systematic review and meta-analysis. Pediatrics 2022, 150, e2022057092D. [Google Scholar] [CrossRef] [PubMed]
- Boundy, E.O.; Dastjerdi, R.; Spiegelman, D.; Fawzi, W.W.; Missmer, S.A.; Lieberman, E.; Kajeepeta, S.; Wall, S.; Chan, G.J. Kangaroo mother care and neonatal outcomes: A meta-analysis. Pediatrics 2016, 137, e20152238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Underwood, M.A. Human Milk for the Premature Infant. Pediatr. Clin. N. Am. 2013, 60, 189–207. [Google Scholar] [CrossRef] [Green Version]
- Dritsakou, K.; Liosis, G.; Valsami, G.; Polychronopoulos, E.; Skouroliakou, M. Improved outcomes of feeding low birth weight infants with predominantly raw human milk versus donor banked milk and formula. J. Matern. Neonatal Med. 2016, 29, 1131–1138. [Google Scholar] [CrossRef]
- Corpeleijn, W.E.; Kouwenhoven, S.M.; Paap, M.C.; van Vliet, I.; Scheerder, I.; Muizer, Y.; Helder, O.K.; van Goudoever, J.B.; Vermeulen, M.J. Intake of Own Mother’s Milk during the First Days of Life Is Associated with Decreased Morbidity and Mortality in Very Low Birth Weight Infants during the First 60 Days of Life. Neonatology 2012, 102, 276–281. [Google Scholar] [CrossRef] [Green Version]
- Cleminson, J.S.; Zalewski, S.P.; Embleton, N.D. Nutrition in the preterm infant: What’s new? Curr. Opin. Clin. Nutr. Metab. Care 2016, 19, 220–225. [Google Scholar]
- Boucher, C.A.; Brazal, P.M.; Graham-Certosini, C.; Carnaghan-Sherrard, K.; Feeley, N. Mothers’ Breastfeeding Experiences in the NICU. Neonatal Netw. 2011, 30, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Giannì, M.L.; Bezze, E.; Sannino, P.; Stori, E.; Plevani, L.; Roggero, P.; Agosti, M.; Mosca, F. Facilitators and barriers of breastfeeding late preterm infants according to mothers’ experiences. BMC Pediatr. 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ross, E.S.; Browne, J.V. Feeding Outcomes in Preterm Infants After Discharge From the Neonatal Intensive Care Unit (NICU): A Systematic Review. Newborn Infant Nurs. Rev. 2013, 13, 87–93. [Google Scholar] [CrossRef]
- Aagaard, H.; Hall, E.C.; Audulv, Å.; Ludvigsen, M.S.; Westergren, T.; Fegran, L. Parents’ experiences of transitioning to home with a very-low-birthweight infant: A meta-ethnography. J. Neonatal Nurs. 2022; in press. [Google Scholar] [CrossRef]
- Lee, H.C.; Jegatheesan, P.; Gould, J.B.; A Dudley, R. Hospital-wide breastfeeding rates vs. breastmilk provision for very-low-birth-weight infants. Acta Paediatr. 2013, 102, 268–272. [Google Scholar] [CrossRef] [Green Version]
- Niela-Vilén, H.; Axelin, A.; Salanterä, S.; Melender, H.-L. A typology of breastfeeding mothers of preterm infants: A qualitative analysis. Adv. Neonatal Care 2019, 19, 42–50. [Google Scholar] [CrossRef]
- Brødsgaard, A.; Andersen, B.L.; Skaaning, D.; Petersen, M.; Dowling, D.; Newberry, D.M.; Parker, L. From Expressing Human Milk to Breastfeeding—An Essential Element in the Journey to Motherhood of Mothers of Prematurely Born Infants. Adv. Neonatal Care 2022, 22, 560–570. [Google Scholar] [CrossRef]
- Flacking, R.; Ewald, U.; Wallin, L. Positive Effect of Kangaroo Mother Care on Long-Term Breastfeeding in Very Preterm Infants. J. Obstet. Gynecol. Neonatal Nurs. 2011, 40, 190–197. [Google Scholar] [CrossRef]
- Briere, C.E.; McGrath, J.; Cong, X.; Cusson, R. An Integrative Review of Factors that Influence Breastfeeding Duration for Premature Infants after NICU Hospitalization. J. Obstet. Gynecol. Neonatal Nurs. 2014, 43, 272–281. [Google Scholar] [CrossRef]
- Green, J.; Fowler, C.; Petty, J.; Whiting, L. The transition home of extremely premature babies: An integrative review. J. Neonatal Nurs. 2021, 27, 26–32. [Google Scholar] [CrossRef]
- Boykova, M.; Kenner, C. Transition From Hospital to Home for Parents of Preterm Infants. J. Périnat. Neonatal Nurs. 2012, 26, 81–87. [Google Scholar] [CrossRef]
- Davim, R.M.B.; Enders, B.C.; Da Silva, R.A.R.D. Mothers’ feelings about breastfeeding their premature babies in a rooming-in facility. Rev. Esc. Enferm. USP 2010, 44, 713–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, R.H.; Zhang, Q.; Ni, Z.H.; Lv, H.T. Transitional care experiences of caregivers of preterm infants hospitalized in a neonatal intensive care unit: A qualitative descriptive study. Nurs. Open 2021, 8, 3484–3494. [Google Scholar] [CrossRef] [PubMed]
- Hariati, S.; Sutomo, R.; Lusmilasari, L.; Febriani, A.D.B.; Kadar, K. Discharge readiness of Indonesian mother with preterm infant in NICU. Enferm. Clin. 2020, 30, 234–237. [Google Scholar] [CrossRef]
- Rustina, Y.; Budi, I.; Hariyati, R.T.S. Mothers’ needs in discharge planning for low birth weight babies: A qualitative study. J. Neonatal Nurs. 2022, 28. [Google Scholar]
- Niela-Vilén, H.; Axelin, A.; Melender, H.-L.; Salanterä, S. Aiming to be a breastfeeding mother in a neonatal intensive care unit and at home: A thematic analysis of peer-support group discussion in social media. Matern. Child Nutr. 2015, 11, 712–726. [Google Scholar] [CrossRef]
- Alves, E.; Rodrigues, C.E.D.; Fraga, S.; Barros, H.; Silva, S. Parents’ views on factors that help or hinder breast milk supply in neonatal care units: Systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2013, 98, F511–F517. [Google Scholar] [CrossRef] [PubMed]
- Brockway, M.; Benzies, K.; Hayden, K.A. Interventions to Improve Breastfeeding Self-Efficacy and Resultant Breastfeeding Rates: A Systematic Review and Meta-Analysis. J. Hum. Lact. 2017, 33, 486–499. [Google Scholar] [CrossRef]
- Heidarzadeh, M.; Hosseini, M.B.; Ershadmanesh, M.; Tabari, M.G.; Khazaee, S. The Effect of Kangaroo Mother Care (KMC) on Breast Feeding at the Time of NICU Discharge. Iran. Red Crescent Med. J. 2013, 15, 302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almeida, H.D.; Venancio, S.I.; Sanches, M.T.C.; Onuki, D. The impact of kangaroo care on exclusive breastfeeding in low-birth-weight newborns. J. Pediatria 2010, 86, 250–253. [Google Scholar] [CrossRef] [Green Version]
- Yilmaz, F.; Küçükoglu, S.; Özdemir, A.A.; Ogul, T.; Aski, N. The effect of kangaroo mother care, provided in the early postpartum period, on the breastfeeding self-efficacy level of mothers and the perceived insufficient milk supply. J. Perinat. Neonatal Nurs. 2020, 34, 80–87. [Google Scholar] [CrossRef]
- Palmér, L.; Ericson, J. A qualitative study on the breastfeeding experience of mothers of preterm infants in the first 12 months after birth. Int. Breastfeed. J. 2019, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granero-Molina, J.; Medina, I.M.F.; Fernández-Sola, C.; Hernández-Padilla, J.M.; Lasserrotte, M.D.M.J.; Rodríguez, M.D.M.L. Experiences of Mothers of Extremely Preterm Infants after Hospital Discharge. J. Pediatr. Nurs. 2019, 45, e2–e8. [Google Scholar] [CrossRef]
- Madiba, S.; Sengane, M. Tube Feeding Practices and Transition to Breastfeeding Experiences of Mothers of Preterm Infants at a Kangaroo Mother Care Unit of a Tertiary Hospital in South Africa. Glob. Pediatr. Health. 2021, 8, 2333794X211037032. [Google Scholar] [CrossRef] [PubMed]
- Hurst, N.; Engebretson, J.; Mahoney, J.S. Providing mother’s own milk in the context of the NICU: A paradoxical experience. J. Hum. Lact. 2013, 29, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Fusch, P.I.; Ness, L.R. Are We There Yet? Data Saturation in Qualitative Research. Qual. Rep. 2015, 20, 1408–1416. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Shenton, A.K. Strategies for ensuring trustworthiness in qualitative research projects. Educ. Inf. 2004, 22, 63–75. [Google Scholar] [CrossRef] [Green Version]
- Mekonnen, A.G.; Yehualashet, S.S.; Bayleyegn, A.D. The effects of kangaroo mother care on the time to breastfeeding initiation among preterm and LBW infants: A meta-analysis of published studies. Int. Breastfeed. J. 2019, 14, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Briere, C.-E.; McGrath, J.M.; Cong, X.; Brownell, E.; Cusson, R. Direct-breastfeeding in the neonatal intensive care unit and breastfeeding duration for premature infants. Appl. Nurs. Res. 2016, 32, 47–51. [Google Scholar] [CrossRef] [Green Version]
- Pineda, R.G. Predictors of Breastfeeding and Breastmilk Feeding Among Very Low Birth Weight Infants. Breastfeed. Med. 2011, 6, 15–19. [Google Scholar] [CrossRef]
- Zukova, S.; Krumina, V.; Buceniece, J. Breastfeeding preterm born infant: Chance and challenge. Int. J. Pediatr. Adolesc. Med. 2021, 8, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Gianni, M.L.; Bezze, E.N.; Sannino, P.; Baro, M.; Roggero, P.; Muscolo, S.; Plevani, L.; Mosca, F. Maternal views on facilitators of and barriers to breastfeeding preterm infants. BMC Pediatr. 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madiba, S.; Modjadji, P.; Ntuli, B. “Breastfeeding at Night Is Awesome” Mothers’ Intentions of Continuation of Breastfeeding Extreme and Very Preterm Babies upon Discharge from a Kangaroo Mother Care Unit of a Tertiary Hospital in South Africa. Healthcare 2023, 11, 1048. https://doi.org/10.3390/healthcare11071048
Madiba S, Modjadji P, Ntuli B. “Breastfeeding at Night Is Awesome” Mothers’ Intentions of Continuation of Breastfeeding Extreme and Very Preterm Babies upon Discharge from a Kangaroo Mother Care Unit of a Tertiary Hospital in South Africa. Healthcare. 2023; 11(7):1048. https://doi.org/10.3390/healthcare11071048
Chicago/Turabian StyleMadiba, Sphiwe, Perpetua Modjadji, and Busisiwe Ntuli. 2023. "“Breastfeeding at Night Is Awesome” Mothers’ Intentions of Continuation of Breastfeeding Extreme and Very Preterm Babies upon Discharge from a Kangaroo Mother Care Unit of a Tertiary Hospital in South Africa" Healthcare 11, no. 7: 1048. https://doi.org/10.3390/healthcare11071048