
Cross-Cultural Validity of a Dietary Questionnaire for Studying Dental Caries in Japanese Children


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures and Procedures
2.3. Food Frequency Questionnaire (FFQ)
2.4. Dental Caries
2.5. Plaque Mutans Streptococci Levels
2.6. Data Analysis
3. Results
3.1. Construct Validity and Internal Consistency Reliability
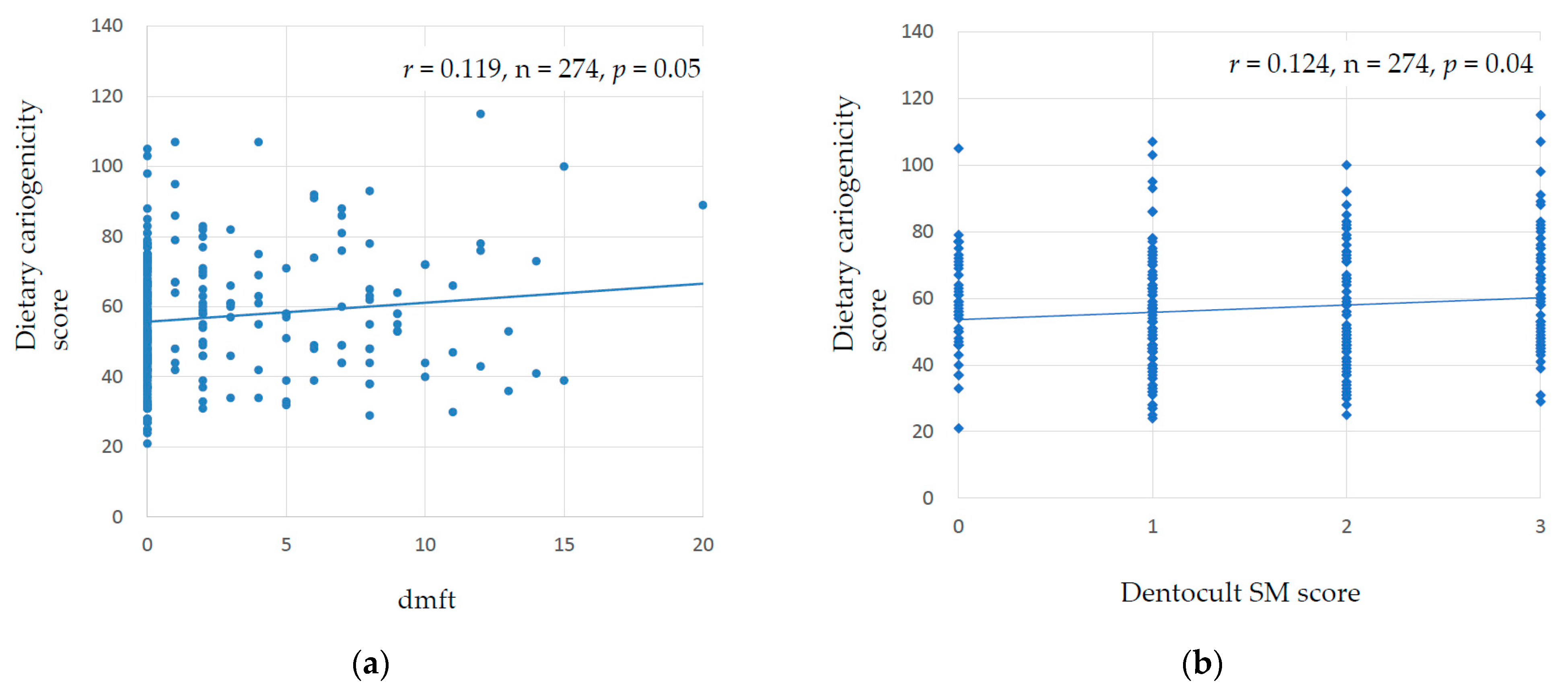
3.2. Criterion Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FDI & IADR. WHA72―FDI and IADR Statement on Item 11.8 Follow-Up to the High-Level Meeting on NCDs (A72/19). 2019. Available online: https://www.fdiworldental.org/sites/default/files/2021-02/fdi-wha72-11_8_followup_hlm_ncds.pdf (accessed on 3 February 2023).
- American Academy of Pediatric Dentistry. The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2022; pp. 90–93. [Google Scholar]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Trombini, J.; Scribante, A. Evaluation of children caries risk factors: A narrative review of nutritional aspects, oral hygiene habits, and bacterial alterations. Children 2022, 9, 262. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Barbieri, S.; Bruni, A.; Sinesi, A.; Ricci, M.; Trombini, J.; et al. Assessment of genetical, pre, peri and post natal risk factors of deciduous molar hypomineralization (DMH), hypomineralized second primary molar (HSPM) and molar incisor hypomineralization (MIH): A narrative review. Children 2021, 8, 432. [Google Scholar] [CrossRef] [PubMed]
- Marsh, P.D. Dental plaque as a biofilm and a microbial community—Implications for health and disease. BMC Oral Health 2006, 6 (Suppl. S1), S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.L.J. Global burden of oral conditions in 1990–2012: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. 2000, 28, 399–406. [Google Scholar] [CrossRef]
- Karjalainen, S.; Tolvanen, M.; Pienihäkkinen, K.; Söderling, E.; Lagström, H.; Simell, O.; Niinikoski, H. High sucrose intake at 3 years of age is associated with increased salivary counts of mutans streptococci and lactobacilli, and with increased caries rate from 3 to 16 years of age. Caries Res. 2015, 49, 125–132. [Google Scholar] [CrossRef]
- Peres, M.A.; Sheiham, A.; Liu, P.; Demarco, F.F.; Silva, A.E.; Assunção, M.C.; Menezes, A.M.; Barros, F.C.; Peres, K.G. Sugar consumption and changes in dental caries from childhood to adolescence. J. Dent. Res. 2016, 95, 388–394. [Google Scholar] [CrossRef]
- Ventura, A.K.; Worobey, J. Early influences on the development of food preferences. Curr. Biol. 2013, 23, R401–R408. [Google Scholar] [CrossRef] [Green Version]
- Darnton-Hill, I.; Nishida, C.; James, W. A life course approach to diet, nutrition and the prevention of chronic diseases. Public Health Nutr. 2004, 7, 101–121. [Google Scholar] [CrossRef] [Green Version]
- Evens, C.C. Snacking Patterns as a Risk Factor for Early Childhood Caries. Ph.D. Thesis, University of Washington, Seattle, WA, USA, 1997. [Google Scholar]
- Shinga-Ishihara, C.; Nakai, Y.; Milgrom, P.; Murakami, K.; Matsumoto-Nakano, M. Cross-cultural validity of a dietary questionnaire for studies of dental caries risk in Japanese. BMC Oral Health 2014, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Amezdroz, E.; Carpenter, L.; Johnson, S.; Flood, V.; Dashper, S.G.; Calache, H.; Gussy, M.; Waters, E. Feasibility and development of a cariogenic diet scale for epidemiological research. Int. J. Paediatr. Dent. 2019, 29, 310–324. [Google Scholar] [CrossRef]
- Kiwanuka, S.N.; Astrøm, A.N.; Trovik, T.A. Sugar snack consumption in Ugandan schoolchildren: Validity and reliability of a food frequency questionnaire. Community Dent. Oral Epidemiol. 2006, 34, 372–380. [Google Scholar] [CrossRef]
- Devenish, G.; Mukhtar, A.; Begley, A.; Do, L.; Scott, J. Development and relative validity of a food frequency questionnaire to assess intakes of total and free sugars in Australian toddlers. Int. J. Environ. Res. Public Health 2017, 14, 1361. [Google Scholar] [CrossRef] [Green Version]
- Thornley, S.; Bach, K.; Bird, A.; Farrar, R.; Bronte, S.; Turton, B.; Atatoa Carr, P.; Fa’alili-Fidow, J.; Morton, S.; Grant, C. What factors are associated with early childhood dental caries? A longitudinal study of the Growing Up in New Zealand cohort. Int. J. Paediatr. Dent. 2020, 31, 351–360. [Google Scholar] [CrossRef]
- Nakai, Y.; Mori-Suzuki, Y. Impact of dietary patterns on plaque acidogenicity and dental caries in early childhood: A retrospective analysis in Japan. Int. J. Environ. Res. Public Health 2022, 19, 7245. [Google Scholar] [CrossRef]
- Livingstone, M.B.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [Green Version]
- Papas, A.S.; Palmer, C.A.; Rounds, M.C.; Herman, J.; McGandy, R.B.; Hartz, S.C.; Russell, R.M.; DePaola, P. Longitudinal relationships between nutrition and oral health. Ann. N. Y. Acad. Sci. 1989, 561, 124–142. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013.
- Karjalainen, S.; Söderling, E.; Pienihäkkinen, K. Validation and inter-examiner agreement of mutans streptococci levels in plaque and saliva of 10-year-old children using simple chair-side tests. Acta. Odontol. Scand. 2004, 62, 153–157. [Google Scholar] [CrossRef]
- Dabawala, S.; Suprabha, B.S.; Shenoy, R.; Rao, A.; Shah, N. Parenting style and oral health practices in early childhood caries: A case-control study. Int. J. Paediatr. Dent. 2017, 27, 135–144. [Google Scholar] [CrossRef]
- Shackleton, N.; Broadbent, J.M.; Thornley, S.; Milne, B.J.; Crengle, S.; Exeter, D.J. Inequalities in dental caries experience among 4-year-old New Zealand children. Community Dent. Oral Epidemiol. 2018, 46, 288–296. [Google Scholar] [CrossRef]
- Singh, A.; Peres, M.A.; Watt, R.G. The relationship between income and oral health: A critical review. J. Dent. Res. 2019, 98, 853–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, C.; Cunha-Cruz, J.; Hugo, F.N. Is dietary pattern a mediator of the relationship between socioeconomic status and dental caries? Clin. Oral Investig. 2021, 25, 5441–5447. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, C.C.C.; Silva, M.C.B.D.; Nunes, A.M.M.; Thomaz, E.B.A.F.; Carmo, C.D.S.; Ribeiro, M.R.C.; Silva, A.A.M.D. Overweight, obese, underweight, and frequency of sugar consumption as risk indicators for early childhood caries in Brazilian preschool children. Int. J. Paediatr. Dent. 2017, 27, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Karki, S.; Päkkilä, J.; Ryhänen, T.; Laitala, M.L.; Humagain, M.; Ojaniemi, M.; Anttonen, V. Body mass index and dental caries experience in Nepalese schoolchildren. Community Dent. Oral Epidemiol. 2019, 47, 346–357. [Google Scholar] [CrossRef]
- Piovesan, É.T.A.; Leal, S.C.; Bernabé, E. The relationship between obesity and childhood dental caries in the United States. Int. J. Environ. Res. Public Health 2022, 19, 16160. [Google Scholar] [CrossRef]
- Kolodziejczyk, J.K.; Merchant, G.; Norman, G.J. Reliability and validity of child/adolescent food frequency questionnaires that assess foods and/or food groups. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 4–13. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 274) | With Caries (n = 109; 39.8%) | Without Caries (n = 165; 60.2%) | |||||
|---|---|---|---|---|---|---|---|
| Column | Row | Row | |||||
| n | % | n | % | n | % | p-Value | |
| Sex | |||||||
| Female | 137 | 50.0 | 56 | 40.9 | 81 | 59.1 | 0.805 a |
| Male | 137 | 50.0 | 53 | 38.7 | 84 | 61.3 | |
| Plaque SM scores | |||||||
| 0 | 40 | 14.6 | 12 | 30.0 | 28 | 70.0 | <0.001 b |
| 1 | 108 | 39.4 | 26 | 24.1 | 82 | 75.9 | |
| 2 | 67 | 24.5 | 30 | 44.8 | 37 | 55.2 | |
| 3 | 59 | 21.5 | 41 | 69.5 | 18 | 30.5 | |
| Toothbrushing/day | |||||||
| 0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0.119 b |
| 1 | 56 | 20.4 | 19 | 33.9 | 37 | 66.1 | |
| 2 | 115 | 42.0 | 49 | 42.6 | 66 | 57.4 | |
| 3 | 100 | 36.5 | 38 | 38.0 | 62 | 62.0 | |
| ≥4 | 3 | 1.1 | 3 | 100.0 | 0 | 0.0 | |
| Parental supervision for toothbrushing | |||||||
| Always | 240 | 87.6 | 92 | 38.3 | 148 | 61.7 | 0.197 a |
| Sometimes | 34 | 12.4 | 17 | 50.0 | 17 | 50.0 | |
| Never | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Type of health insurance | |||||||
| Employee | 249 | 90.9 | 95 | 87.2 | 154 | 93.3 | 0.09 a |
| National | 25 | 9.1 | 14 | 12.8 | 11 | 6.7 | |
| Public assistance | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | |
| Mean | SD | Mean | SD | Mean | SD | p-value | |
| Age (years) | 4.4 | 1.1 | 4.9 | 1.0 | 4.2 | 1.0 | <0.001 c |
| Birth weight (g) | 3017.4 | 407.9 | 3035.9 | 359.9 | 3005.1 | 437.3 | 0.542 c |
| Dietary cariogenicity score | 57.0 | 17.3 | 60.1 | 18.7 | 54.9 | 16.0 | 0.013 c |
| Distribution Percentage of Frequency Scores | |||||||
|---|---|---|---|---|---|---|---|
| Food Item | 0 (Never) | 1 (Rarely) | 2 (1/wk) | 3 (2–3/wk) | 4 (1/dy) | 5 (2–3/dy) | 6 (4+/dy) |
| Solid sugars | |||||||
| Cookies | 20.8 | 52.6 | 15.3 | 10.6 | 0.7 | 0 | 0 |
| Donuts or muffins | 25.2 | 60.6 | 11.3 | 2.9 | 0 | 0 | 0 |
| Cakes or pies | 27.0 | 67.9 | 3.6 | 1.5 | 0 | 0 | 0 |
| Solid and slowly dissolving sugars | |||||||
| Hard candy | 29.2 | 37.2 | 12.8 | 16.8 | 2.9 | 1.1 | 0 |
| Chips | 35.8 | 46.0 | 13.1 | 5.1 | 0 | 0 | 0 |
| Sticky candy (caramel) | 73.0 | 16.4 | 4.7 | 4.7 | 0.7 | 0.4 | 0 |
| Sticky sugars | |||||||
| Jam, jelly, or syrup | 55.5 | 21.5 | 5.8 | 10.6 | 5.8 | 0 | 0.7 |
| Bread filled with bean or fruit jam | 59.5 | 29.6 | 5.8 | 4.7 | 0 | 0 | 0.4 |
| Semisolid and sticky sugars | |||||||
| Plain yogurt | 73.0 | 12.0 | 4.0 | 6.9 | 4.0 | 0 | 0 |
| Banana | 16.8 | 35.8 | 19.7 | 20.1 | 6.6 | 0.7 | 0.4 |
| Slowly dissolving sugars | |||||||
| Breath mints | 96.4 | 2.9 | 0 | 0 | 0.7 | 0 | 0 |
| Gum (not sugar-free) | 79.2 | 13.1 | 4.4 | 2.2 | 0.7 | 0 | 0.4 |
| Starchy and slowly dissolving sugars | |||||||
| Plain cereal | 95.6 | 2.9 | 0.7 | 0 | 0.7 | 0 | 0 |
| Cough drops | 96.4 | 2.9 | 0 | 0 | 0 | 0.7 | 0 |
| Others | |||||||
| Cheese | 12.4 | 42.0 | 17.5 | 20.4 | 5.5 | 2.2 | 0 |
| Sugared yogurt | 24.5 | 31.8 | 8.4 | 21.2 | 12.4 | 1.5 | 0.4 |
| Bread | 4.0 | 17.2 | 17.9 | 31.8 | 27.4 | 0.4 | 1.5 |
| Rice | 0 | 0 | 0 | 1.1 | 8.8 | 83.9 | 6.2 |
| Sugar added to Cereal | 71.2 | 18.2 | 4.4 | 4.4 | 1.5 | 0.4 | 0 |
| Lactic acid-containing drink | 24.8 | 38.7 | 10.9 | 14.6 | 8.4 | 1.5 | 1.1 |
| Canned fruit | 72.6 | 23.7 | 1.8 | 1.5 | 0 | 0 | 0.4 |
| Dried fruit | 71.9 | 21.2 | 4.0 | 2.2 | 0.7 | 0 | 0 |
| Milk | 4.7 | 10.6 | 5.5 | 15.3 | 28.1 | 24.5 | 11.3 |
| Fruit juice | 63.9 | 26.6 | 3.6 | 5.5 | 0.4 | 0 | 0 |
| Soda (not diet) | 71.9 | 17.9 | 5.1 | 3.3 | 1.1 | 0.7 | 0 |
| Cold drinks | 16.1 | 40.1 | 12.8 | 22.3 | 6.2 | 2.2 | 0.4 |
| Cocoa | 75.9 | 13.5 | 3.6 | 4.4 | 2.6 | 0 | 0 |
| Sugar or Honey in Coffee or Tea | 82.8 | 8.8 | 1.5 | 3.6 | 2.6 | 0.7 | 0 |
| Sugared cereal | 99.6 | 0.4 | 0 | 0 | 0 | 0 | 0 |
| Ice cream or sorbet | 6.9 | 40.1 | 17.9 | 24.8 | 9.5 | 0.7 | 0 |
| Pudding or custard | 41.6 | 47.8 | 6.9 | 3.3 | 0.4 | 0 | 0 |
| Jell-O (not sugar-free) | 25.5 | 47.1 | 9.1 | 15.0 | 2.6 | 0.7 | 0 |
| Chocolate | 15.7 | 36.1 | 16.1 | 26.6 | 5.5 | 0 | 0 |
| Popcorn | 67.2 | 29.9 | 1.8 | 1.1 | 0.0 | 0 | 0 |
| Rice cracker | 21.5 | 43.4 | 17.2 | 16.1 | 1.8 | 0 | 0 |
| Bun with bean jam filling | 54.4 | 36.1 | 7.3 | 2.2 | 0 | 0 | 0 |
| Rice cake | 59.5 | 29.2 | 6.9 | 4.4 | 0 | 0 | 0 |
| Bar of sweet jellied adzuki bean paste | 90.9 | 9.1 | 0 | 0 | 0 | 0 | 0 |
| Food Item | Factor Loading Component | |||||
|---|---|---|---|---|---|---|
| I a | II b | III c | IV d | V e | VI f | |
| Cookies | 0.572 | −0.010 | 0.175 | 0.031 | −0.035 | −0.010 |
| Donuts or muffins | 0.531 | 0.239 | 0.044 | −0.035 | −0.048 | 0.004 |
| Cakes or pies | 0.418 | 0.052 | 0.022 | −0.073 | 0.150 | 0.057 |
| Hard candy | 0.049 | 0.662 | 0.050 | −0.061 | 0.039 | 0.024 |
| Chips | 0.118 | 0.413 | −0.082 | −0.110 | 0.024 | −0.041 |
| Sticky candy (caramel) | 0.073 | 0.405 | 0.248 | −0.003 | 0.204 | 0.007 |
| Jam, jelly, or syrup | 0.002 | −0.027 | 0.682 | −0.036 | −0.019 | 0.103 |
| Bread filled with bean or fruit jam | 0.316 | 0.052 | 0.556 | 0.103 | 0.103 | −0.067 |
| Plain yogurt | 0.012 | −0.171 | −0.009 | 0.621 | −0.007 | 0.089 |
| Banana | 0.088 | 0.001 | 0.084 | 0.404 | −0.127 | 0.017 |
| Breath mints | −0.021 | 0.029 | 0.014 | 0.026 | 0.859 | −0.024 |
| Gum (not sugar-free) | −0.008 | 0.253 | 0.069 | −0.071 | 0.407 | 0.006 |
| Plain cereal | 0.051 | 0.024 | −0.025 | 0.129 | −0.016 | 0.710 |
| Cough drops | −0.021 | −0.054 | 0.041 | −0.053 | −0.017 | 0.554 |
| Cheese | −0.020 | −0.147 | −0.046 | 0.131 | −0.082 | 0.074 |
| Sugared yogurt | 0.144 | 0.007 | 0.108 | −0.159 | −0.029 | −0.061 |
| Bread | 0.144 | 0.069 | 0.237 | 0.019 | 0.057 | 0.082 |
| Rice | −0.030 | −0.081 | 0.081 | 0.047 | −0.063 | 0.042 |
| Sugar added to Cereal | 0.080 | 0.095 | −0.028 | 0.035 | −0.106 | −0.067 |
| Lactic acid-containing drink | 0.143 | 0.172 | −0.016 | −0.267 | −0.012 | −0.073 |
| Canned fruit | 0.000 | 0.073 | 0.144 | 0.047 | −0.006 | −0.052 |
| Dried fruit | −0.059 | −0.017 | 0.223 | 0.118 | 0.025 | 0.387 |
| Milk | 0.065 | −0.048 | 0.086 | 0.111 | 0.035 | 0.007 |
| Fruit juice | 0.084 | 0.131 | −0.040 | 0.025 | 0.011 | −0.089 |
| Soda (not diet) | −0.043 | 0.247 | 0.046 | −0.039 | 0.304 | −0.078 |
| Cold drinks | 0.330 | 0.365 | 0.095 | −0.198 | −0.046 | −0.085 |
| Cocoa | 0.034 | 0.059 | 0.043 | −0.135 | 0.002 | −0.016 |
| Sugar or Honey in Coffee or Tea | −0.029 | −0.036 | 0.107 | 0.117 | 0.088 | 0.228 |
| Sugared cereal | −0.023 | −0.005 | 0.010 | 0.003 | 0.009 | −0.013 |
| Ice cream or sorbet | −0.006 | 0.227 | 0.054 | −0.079 | 0.075 | 0.051 |
| Pudding or custard | 0.367 | 0.099 | −0.080 | 0.016 | −0.018 | −0.049 |
| Jell-O (not sugar-free) | 0.079 | 0.111 | 0.032 | 0.024 | −0.040 | 0.012 |
| Chocolate | 0.276 | 0.191 | −0.050 | −0.447 | −0.015 | 0.156 |
| Popcorn | 0.080 | 0.370 | −0.047 | −0.060 | 0.051 | −0.022 |
| Rice cracker | 0.264 | 0.176 | 0.292 | 0.287 | 0.024 | 0.030 |
| Bun with bean jam filling | 0.345 | 0.178 | 0.268 | 0.298 | 0.060 | −0.019 |
| Rice cake | 0.175 | 0.074 | −0.082 | 0.078 | −0.009 | −0.062 |
| Bar of sweet jellied adzuki bean paste | 0.016 | 0.077 | 0.032 | 0.055 | 0.070 | 0.057 |
| Eigenvalue | 1.566 | 1.551 | 1.252 | 1.219 | 1.150 | 1.131 |
| Variance percentage | 4.120 | 4.081 | 3.296 | 3.207 | 3.027 | 2.977 |
| Chronbach’s alpha | 0.52 | 0.48 | 0.54 | 0.48 | 0.39 | 0.53 |
| Dentocult SM Score | ||||
|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |
| Mean ± SD | 58.2 ± 15.5 | 54.0 ± 16.8 | 55.6 ± 17.7 | 63.0 ± 17.6 |
| n | 40 | 108 | 67 | 59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakai, Y.; Mori-Suzuki, Y. Cross-Cultural Validity of a Dietary Questionnaire for Studying Dental Caries in Japanese Children. Healthcare 2023, 11, 1036. https://doi.org/10.3390/healthcare11071036
Nakai Y, Mori-Suzuki Y. Cross-Cultural Validity of a Dietary Questionnaire for Studying Dental Caries in Japanese Children. Healthcare. 2023; 11(7):1036. https://doi.org/10.3390/healthcare11071036
Chicago/Turabian StyleNakai, Yukie, and Yukako Mori-Suzuki. 2023. "Cross-Cultural Validity of a Dietary Questionnaire for Studying Dental Caries in Japanese Children" Healthcare 11, no. 7: 1036. https://doi.org/10.3390/healthcare11071036