
Addressing Health Disparities through Community Participation: A Scoping Review of Co-Creation in Public Health
 , , , and
, , , and
Abstract
:1. Introduction
1.1. Citizen and Community Engagement in Public Health
1.2. Community-Based Participatory Research
1.3. Cocreation and Public Health
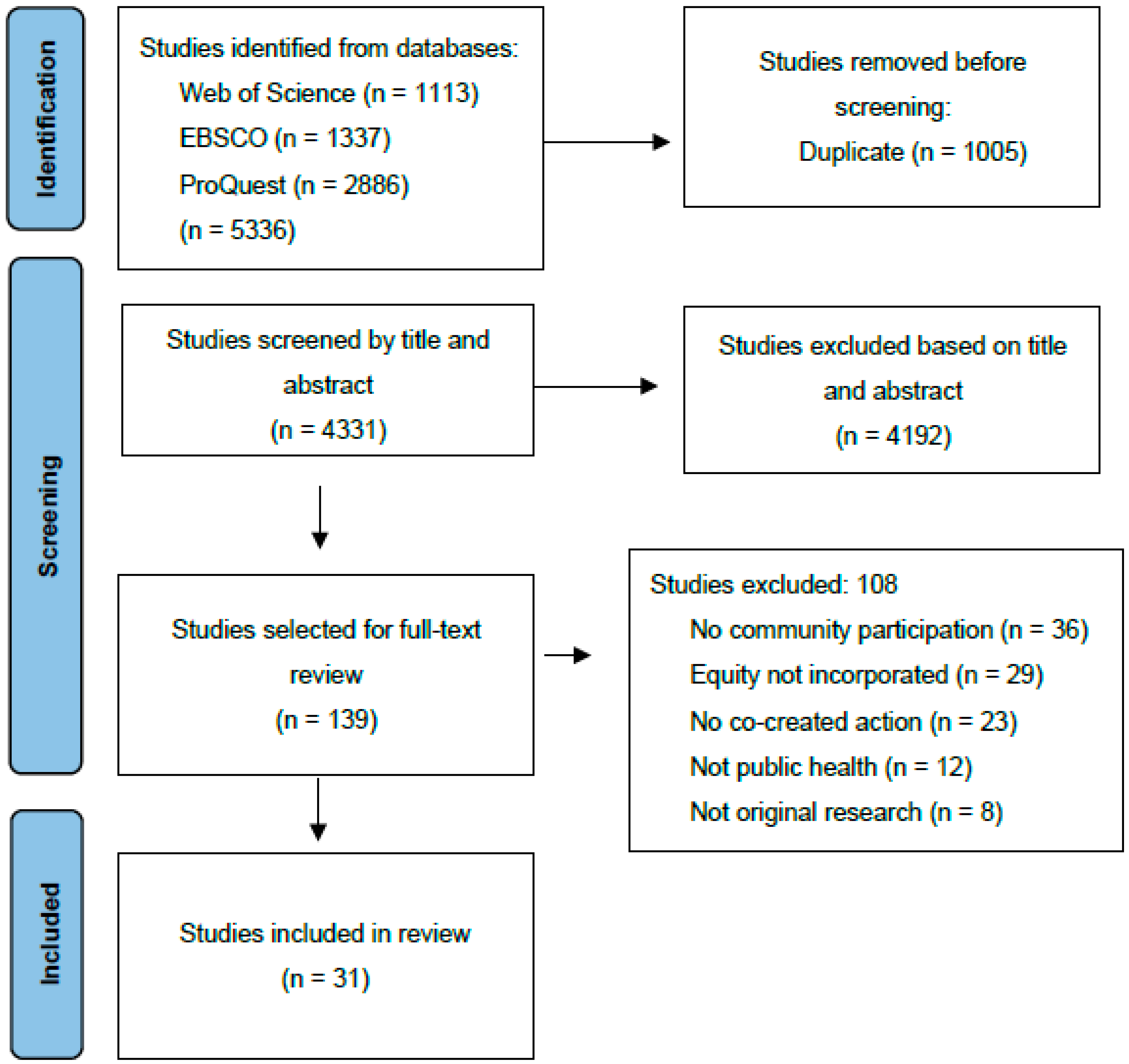
2. Materials and Methods
2.1. Search Strategy
2.2. Identifying Relevant Studies
2.3. Study Selection
2.4. Data Extraction and Synthesis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Web of Science (N = 1113) | TS = (“CO-CREATION” OR “OPEN SCIENCE” OR “COMMUNITY NETWORKS” OR “COPARTICIPACION” OR “INTEGRATED GOVERNANCE” OR “COLLABORATIVE LEADERSHIP” OR “PARTICIPATORY ACTION RESEARCH” OR “COPRODUCCION” OR “CO-DESIGN” OR “CITIZEN SCIENCE” OR “CITIZEN ENGAGMENT” OR “CO-OPERATION” OR “HUMAN CENTERED DESIGN”) AND TS = (“PUBLIC HEALTH” OR “PUBLIC POLICIES” OR “HEALTH POLICIES” OR “POLICY-MAKING PROCESS” OR “HEALTHCARE POLICIES” OR “HEALTH PROGRAMS” OR “HEALTH PROGRAMME”) AND TS = (“EQUITY” OR “HEALTH PROMOTION” OR “INEQUALITIES” OR “INEQUITIES” OR “INEQUALITY” OR “INEQUITY” OR “DISPARITY” OR “DISPARITIES”). |
| ProQuest (N = 2886) | ((“CO-CREATION” OR “OPEN SCIENCE” OR “COMMUNITY NETWORKS” OR “COPARTICIPACION” OR “INTEGRATED GOVERNANCE” OR “COLLABORATIVE LEADERSHIP” OR “PARTICIPATORY ACTION RESEARCH” OR “COPRODUCCION” OR “CO-DESIGN” OR “CITIZEN SCIENCE” OR “CITIZEN ENGAGMENT” OR “CO-OPERATION” OR “HUMAN CENTERED DESIGN”) AND (“PUBLIC HEALTH” OR “PUBLIC POLICIES” OR “HEALTH POLICIES” OR “POLICY-MAKING PROCESS” OR “HEALTHCARE POLICIES” OR “HEALTH PROGRAMS” OR “HEALTH PROGRAMME”) AND (“EQUITY” OR “HEALTH PROMOTION” OR “INEQUALITIES” OR “INEQUITIES” OR “INEQUALITY” OR “INEQUITY” OR “DISPARITY” OR “DISPARITIES”)) AND (at.exact(“Feature”) AND subt.exact(“public health”) AND stype.exact(“Scholarly Journals”)) |
| EBSCO (N = 1337) | (“CO-CREATION” OR “OPEN SCIENCE” OR “COMMUNITY NETWORKS” OR “COPARTICIPACION” OR “INTEGRATED GOVERNANCE” OR “COLLABORATIVE LEADERSHIP” OR “PARTICIPATORY ACTION RESEARCH” OR “COPRODUCCION” OR “CO-DESIGN” OR “CITIZEN SCIENCE” OR “CITIZEN ENGAGMENT” OR “CO-OPERATION” OR “HUMAN CENTERED DESIGN”) AND (“PUBLIC HEALTH” OR “PUBLIC POLICIES” OR “HEALTH POLICIES” OR “POLICY-MAKING PROCESS” OR “HEALTHCARE POLICIES” OR “HEALTH PROGRAMS” OR “HEALTH PROGRAMME”) AND (“EQUITY” OR “HEALTH PROMOTION” OR “INEQUALITIES” OR “INEQUITIES” OR “INEQUALITY” OR “INEQUITY” OR “DISPARITY” OR “DISPARITIES”) |
References
- World Health Organization. Community Engagement: A Health Promotion Guide for Universal Health Coverage in the Hands of the People; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization. Community Engagement Framework for Quality, People-Centred and Resilient Health Services; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- McCloskey, D.J.; Akintobi, T.H.; Bonham, A.; Cook, J.; Coyne-Beasley, T. Principles of Community Engagement, 2nd ed.; NIH Publication: Bethesda, MD, USA, 2011.
- Centers for Disease. CDC—10 Essential Public Health Services—CSTLTS. Available online: https://www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html (accessed on 25 January 2023).
- World Health Organization. Ottawa Charter for Health Promotion; World Health Organization: Geneva, Switzerland, 1986. [Google Scholar]
- Rootman, I.; Goodstadt, M.; Hyndman, B.; McQueen, D.V.; Potvin, L.; Springett, J.; Ziglio, E. Evaluation in Health Promotion: Principles and Perspectives; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2001. [Google Scholar]
- Public Health: Ethical Issues; Hepple, B.; Nuffield Council on Bioethics (Eds.) Nuffield Council on Bioethics: London, UK, 2007. [Google Scholar]
- American Public Health Association. Principles of the Ethical Practice of Public Health; American Public Health Association: Washington, DC, USA, 2002. [Google Scholar]
- O’Mara-Eves, A.; Brunton, G.; Oliver, S.; Kavanagh, J.; Jamal, F.; Thomas, J. The Effectiveness of Community Engagement in Public Health Interventions for Disadvantaged Groups: A Meta-Analysis. BMC Public Health 2015, 15, 129. [Google Scholar] [CrossRef] [Green Version]
- Von Heimburg, D.; Ness, O. Relational Welfare: A Socially Just Response to Co-Creating Health and Wellbeing for All. Scand. J Public Health 2021, 49, 639–652. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. Community Engagement: Improving Health and Wellbeing and Reducing Health Inequalities; National Institute for Health and Clinical Excellence: London, UK, 2016. [Google Scholar]
- South, J.; Phillips, G. Evaluating Community Engagement as Part of the Public Health System. J. Epidemiol. Commun. Health 2014, 68, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Chiu, L.F.; West, R.M. Health Intervention in Social Context: Understanding Social Networks and Neighbourhood. Soc. Sci. Med. 2007, 65, 1915–1927. [Google Scholar] [CrossRef]
- Holmes, B. Citizens’ Engagement in Policymaking and the Design of Public Services; Parliamentary Library: Canberra, Australia, 2011. [Google Scholar]
- Wallerstein, N. Empowerment to Reduce Health Disparities. Scand. J. Public Health 2002, 30 (Suppl. 59), 72–77. [Google Scholar] [CrossRef]
- Nascimento, F. Citizen Engagement in Science and Policy-Making; JRC Publications Repository: Luxembourg, 2016. [Google Scholar]
- Den Broeder, L.; Devilee, J.; Van Oers, H.; Schuit, A.J.; Wagemakers, A. Citizen Science for Public Health. Health Promot. Int. 2018, 33, 505–514. [Google Scholar] [CrossRef] [Green Version]
- MacQueen, K.M.; McLellan, E.; Metzger, D.S.; Kegeles, S.; Strauss, R.P.; Scotti, R.; Blanchard, L.; Trotter, R.T. What Is Community? An Evidence-Based Definition for Participatory Public Health. Am. J. Public Health 2001, 91, 1929–1938. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Community Power in Population Health Improvement: Proceedings of a Workshop; Nicholson, A., Haag, T., Eds.; National Academies Press: Washington, DC, USA, 2022. [Google Scholar] [CrossRef]
- Cyril, S.; Smith, B.J.; Possamai-Inesedy, A.; Renzaho, A.M.N. Exploring the Role of Community Engagement in Improving the Health of Disadvantaged Populations: A Systematic Review. Glob. Health Action 2015, 8, 29842. [Google Scholar] [CrossRef] [Green Version]
- Carlisle, S. Tackling Health Inequalities and Social Exclusion through Partnership and Community Engagement? A Reality Check for Policy and Practice Aspirations from a Social Inclusion Partnership in Scotland. Crit. Public Health 2010, 20, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.; Duran, B. Community-Based Participatory Research Contributions to Intervention Research: The Intersection of Science and Practice to Improve Health Equity. Am. J. Public Health 2010, 100 (Suppl. 1), S40–S46. [Google Scholar] [CrossRef]
- De Las Nueces, D.; Hacker, K.; DiGirolamo, A.; Hicks, L.S. A Systematic Review of Community-Based Participatory Research to Enhance Clinical Trials in Racial and Ethnic Minority Groups. Health Serv. Res. 2012, 47, 1363–1386. [Google Scholar] [CrossRef] [Green Version]
- Israel, B.A.; Schulz, A.J.; Parker, E.A.; Becker, A.B. Review of Community-Based Research: Assessing Partnership Approaches to Improve Public Health. Annu. Rev. Public Health 1998, 19, 173–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallerstein, N.B.; Duran, B. Using Community-Based Participatory Research to Address Health Disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Von Heimburg, D.; Cluley, V. Advancing Complexity-Informed Health Promotion: A Scoping Review to Link Health Promotion and Co-Creation. Health Promot. Int. 2021, 36, 581–600. [Google Scholar] [CrossRef] [PubMed]
- Leask, C.F.; Sandlund, M.; Skelton, D.A.; Altenburg, T.M.; Cardon, G.; Chinapaw, M.J.M.; De Bourdeaudhuij, I.; Verloigne, M.; Chastin, S.F.M.; on behalf of the GrandStand, Safe Step and Teenage Girls on the Move Research Groups. Framework, Principles and Recommendations for Utilising Participatory Methodologies in the Co-Creation and Evaluation of Public Health Interventions. Res. Involv. Engagem. 2019, 5, 2. [Google Scholar] [CrossRef]
- Voorberg, W.H.; Bekkers, V.J.J.M.; Tummers, L.G. A Systematic Review of Co-Creation and Co-Production: Embarking on the Social Innovation Journey. Public Manag. Rev. 2015, 17, 1333–1357. [Google Scholar] [CrossRef] [Green Version]
- Brandsen, T.; Verschuere, B.; Steen, T. Engaging Citizens in Public Services; Routledge: New York, NY, USA, 2020. [Google Scholar] [CrossRef] [Green Version]
- Research Glossary. Research Connections. Available online: https://www.researchconnections.org/research-tools/research-glossary (accessed on 25 January 2023).
- Rains, J.W.; Ray, D.W. Participatory Action Research for Community Health Promotion. Public Health Nurs. 1995, 12, 256–261. [Google Scholar] [CrossRef]
- Giachello, A.L.; Arrom, J.O.; Davis, M.; Sayad, J.V.; Ramirez, D.; Nandi, C.; Ramos, C. Reducing Diabetes Health Disparities through Community-Based Participatory Action Research: The Chicago Southeast Diabetes Community Action Coalition. Public Health Rep 2003, 118, 309–323. [Google Scholar] [CrossRef]
- Sullivan, M.; Bhuyan, R.; Senturia, K.; Shiu-Thornton, S.; Ciske, S. Participatory Action Research in Practice: A Case Study in Addressing Domestic Violence in Nine Cultural Communities. J. Interpers. Violence 2005, 20, 977–995. [Google Scholar] [CrossRef]
- Ferré, C.D.; Jones, L.; Norris, K.C.; Rowley, D.L. The Healthy African American Families (HAAF) Project: From Community-Based Participatory Research to Community-Partnered Participatory Research. Ethn. Dis. 2010, 20, S2-1–8. [Google Scholar]
- Schulz, A.J.; Israel, B.A.; Coombe, C.M.; Gaines, C.; Reyes, A.G.; Rowe, Z.; Sand, S.L.; Strong, L.L.; Weir, S. A Community-Based Participatory Planning Process and Multilevel Intervention Design: Toward Eliminating Cardiovascular Health Inequities. Health Promot. Pract. 2011, 12, 900–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kreuter, M.W. The impact of implementing selected CBPR strategies to address disparities in urban Atlanta: A retrospective case. Health Educ. Res. 2012, 27, 729–741. [Google Scholar] [CrossRef] [Green Version]
- Montgomery, M.; Manuelito, B.; Nass, C.; Chock, T.; Buchwald, D. The Native Comic Book Project: Native Youth Making Comics and Healthy Decisions. J. Cancer Educ. 2012, 27, S41–S46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abara, W.; Wilson, S.; Vena, J.; Sanders, L.; Bevington, T.; Culley, J.M.; Annang, L.; Dalemarre, L.; Svendsen, E. Engaging a Chemical Disaster Community: Lessons from Graniteville. Int. J. Environ. Res. Public Health 2014, 11, 5684–5697. [Google Scholar] [CrossRef] [Green Version]
- Noone, J.; Sullivan, M.; McKinnis, N.C.; Allen, T.L.; Regalado, C.; Esqueda, T. Latino Youth Participation in Community-Based Participatory Research to Reduce Teen Pregnancy Disparities. Child. Youth Serv. Rev. 2016, 63, 36–39. [Google Scholar] [CrossRef]
- Andress, L.; Hallie, S.S. Co-Constructing Food Access Issues: Older Adults in a Rural Food Environment in West Virginia Develop a Photonarrative. Cogent Medicine 2017, 4, 1309804. [Google Scholar] [CrossRef]
- Cuervo, I.; Leopold, L.; Baron, S. Promoting Community Preparedness and Resilience: A Latino Immigrant Community–Driven Project Following Hurricane Sandy. Am. J. Public Health 2017, 107, S161–S164. [Google Scholar] [CrossRef] [PubMed]
- Peréa, F.C.; Sayles, N.R.; Reich, A.J.; Koomas, A.; McMann, H.; Sprague Martinez, L.S. “Mejorando Nuestras Oportunidades”: Engaging Urban Youth in Environmental Health Assessment and Advocacy to Improve Health and Outdoor Play Spaces. Int. J. Environ. Res. Public Health 2019, 16, 571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, G.; Shi, T.; Yao, Z.; Li, D.; Sansom, G.; Kirsch, K.; Casillas, G.; Horney, J. Citizen Science-Informed Community Master Planning: Land Use and Built Environment Changes to Increase Flood Resilience and Decrease Contaminant Exposure. Int. J. Environ. Res. Public Health 2020, 17, 486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frerichs, L.; Smith, N.; Kuhlberg, J.A.; Mason, G.; Jackson-Diop, D.; Stith, D.; Corbie-Smith, G.; Lich, K.H. Novel Participatory Methods for Co-Building an Agent-Based Model of Physical Activity with Youth. PLoS ONE 2020, 15, e0241108. [Google Scholar] [CrossRef]
- Symanski, E.; An Han, H.; Hopkins, L.; Smith, M.A.; McCurdy, S.; Han, I.; Jimenez, M.; Markham, C.; Richner, D.; James, D.; et al. Metal Air Pollution Partnership Solutions: Building an Academic-Government-Community-Industry Collaboration to Improve Air Quality and Health in Environmental Justice Communities in Houston. Environ. Health 2020, 19, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, S.L.; Edge, V.L.; Cunsolo Willox, A.; Rigolet Inuit Community Government. “Changing Climate, Changing Health, Changing Stories” Profile: Using an EcoHealth Approach to Explore Impacts of Climate Change on Inuit Health. Ecohealth 2012, 9, 89–101. [Google Scholar] [CrossRef]
- Thompson, H.A.; Mason, C.W.; Robidoux, M.A. Hoop House Gardening in the Wapekeka First Nation as an Extension of Land-Based Food Practices. Arctic 2018, 71, 407–421. [Google Scholar] [CrossRef]
- Ríos-Cortázar, V.; Gasca-García, A.; Franco-Martínez, M.; Tolentino-Mayo, L. Narrativa infantil en entornos escolares. Una estrategia de promoción de la salud. Salud Publica Mex. 2013, 56, 123. [Google Scholar] [CrossRef]
- Brännström, L.; Nyhlén, S.; Gådin, K.G. Girls’ Perspectives on Gendered Violence in Rural Sweden: Photovoice as a Method for Increased Knowledge and Social Change. Int. J. Qual. Methods 2020, 19, 1609406920962904. [Google Scholar] [CrossRef]
- Ali, P.A.; Salway, S.; Such, E.; Dearden, A.; Willox, M. Enhancing Health Literacy through Co-Design: Development of Culturally Appropriate Materials on Genetic Risk and Customary Consanguineous Marriage. Prim. Health Care Res. Dev. 2018, 20, e2. [Google Scholar] [CrossRef] [Green Version]
- Prevo, L.; Kremers, S.; Jansen, M. The Power of Trading: Exploring the Value of a Trading Shop as a Health-Promoting Community Engagement Approach. Int. J. Environ. Res. Public Health 2020, 17, 4678. [Google Scholar] [CrossRef] [PubMed]
- Miranda, D.E.; Garcia-Ramirez, M.; Balcazar, F.E.; Suarez-Balcazar, Y. A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain. Int. J. Environ. Res. Public Health 2019, 16, 3722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda, D.E.; Gutiérrez-Martínez, A.; Vizarraga Trigueros, E.; Albar-Marín, M.J. Training for Roma health advocacy: A case study of Torreblanca, Seville. Gac. Sanit. 2022, 36, 118–126. [Google Scholar] [CrossRef]
- Cox, A.; Dudgeon, P.; Holland, C.; Kelly, K.; Scrine, C.; Walker, R. Using Participatory Action Research to Prevent Suicide in Aboriginal and Torres Strait Islander Communities. Aust. J. Prim. Health 2014, 20, 345–349. [Google Scholar] [CrossRef]
- Gilbert, E.; Collins, R.; Webster, V.; Boyd, N.; Maple-Brown, L.; Boyle, J.; Smith-Vaughan, H. Using Co-Design to Develop a Culturally Responsive Reproductive Health Learning Resource for Aboriginal and Torres Strait Islander Youth. Health Promot. J. Aust. 2021, 32, 179–185. [Google Scholar] [CrossRef]
- Carr, J.J.; Lalara, J.; Lalara, G.; Lalara, G.; Daniels, B.; Clough, A.R.; Lowell, A.; Barker, R.N. Staying Strong Toolbox: Co-Design of a Physical Activity and Lifestyle Program for Aboriginal Families with Machado-Joseph Disease in the Top End of Australia. PLoS ONE 2021, 16, e0244311. [Google Scholar] [CrossRef]
- Gerritsen, S.; Renker-Darby, A.; Harré, S.; Rees, D.; Raroa, D.A.; Eickstaedt, M.; Sushil, Z.; Allan, K.; Bartos, A.E.; Waterlander, W.E.; et al. Improving Low Fruit and Vegetable Intake in Children: Findings from a System Dynamics, Community Group Model Building Study. PLoS ONE 2019, 14, e0221107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chukwudozie, O.; Feinstein, C.; Jensen, C.; O’Kane, C.; Pina, S.; Skovdal, M.; Smith, R. Applying Community-Based Participatory Research to Better Understand and Improve Kinship Care Practices: Insights From the Democratic Republic of Congo, Nigeria, and Sierra Leone. Fam Community Health 2015, 38, 108–119. [Google Scholar] [CrossRef] [Green Version]
- Chimberengwa, P.T.; Naidoo, M. A Description of Community-Based Participatory Research of Hypertension Awareness, Prevention and Treatment in a District of Matabeleland South Province, Zimbabwe. Afr. J. Prim. Health Care Fam. Med. 2019, 11, 1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oladeinde, O.; Mabetha, D.; Twine, R.; Hove, J.; Van Der Merwe, M.; Byass, P.; Witter, S.; Kahn, K.; D’Ambruoso, L. Building Cooperative Learning to Address Alcohol and Other Drug Abuse in Mpumalanga, South Africa: A Participatory Action Research Process. Glob. Health Action 2020, 13, 1726722. [Google Scholar] [CrossRef] [Green Version]
- Kabukye, J.K.; Ilozumba, O.; Broerse, J.E.W.; de Keizer, N.; Cornet, R. Implementation of an Interactive Voice Response System for Cancer Awareness in Uganda: Mixed Methods Study. JMIR mHealth uHealth 2021, 9, e22061. [Google Scholar] [CrossRef]
- Halvorsrud, K.; Kucharska, J.; Adlington, K.; Rüdell, K.; Brown Hajdukova, E.; Nazroo, J.; Haarmans, M.; Rhodes, J.; Bhui, K. Identifying Evidence of Effectiveness in the Co-Creation of Research: A Systematic Review and Meta-Analysis of the International Healthcare Literature. J. Public Health 2021, 43, 197–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargas, C.; Whelan, J.; Brimblecombe, J.; Brock, J.; Christian, M.; Allender, S. Co-Creation of Healthier Food Retail Environments: A Systematic Review to Explore the Type of Stakeholders and Their Motivations and Stage of Engagement. Obes. Rev. 2022, 23, e13482. [Google Scholar] [CrossRef]
- Jacques-Aviñó, C.; Roel, E.; Medina-Perucha, L.; McGhie, J.; Pons-Vigués, M.; Pujol-Ribera, E.; Turiel, I.; Berenguera, A. Are We Leaving Someone behind? A Critical Discourse Analysis on the Understanding of Public Participation among People with Experiences of Participatory Research. PLoS ONE 2022, 17, e0273727. [Google Scholar] [CrossRef]
- Cowdell, F.; Dyson, J.; Sykes, M.; Dam, R.; Pendleton, R. How and How Well Have Older People Been Engaged in Healthcare Intervention Design, Development or Delivery Using Co-Methodologies: A Scoping Review with Narrative Summary. Health Soc. Care Commun. 2022, 30, 776–798. [Google Scholar] [CrossRef] [PubMed]
- Marsilio, M.; Fusco, F.; Gheduzzi, E.; Guglielmetti, C. Co-Production Performance Evaluation in Healthcare. A Systematic Review of Methods, Tools and Metrics. Int. J. Environ. Res. Public Health 2021, 18, 3336. [Google Scholar] [CrossRef] [PubMed]

| Promotors | Other Stakeholders | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Reference | Country | Objective | Academic lInstitutions | Healthcare Institutions | Governmental Institutions | Private Orgs. | Public Institutions | Social Orgs. | Private Orgs. |
| Rains & Ray, 1995 [31] | United States | To work with the community to address higher-than-average national heart disease and cancer-related mortality in a rural Indiana town. | ✓ | ✓ | |||||
| Giachello, 2003 [32] | United States | To reduce diabetes mortality, hospitalizations, complications, and related disabilities among African Americans and Latinos in Chicago’s Southeast Side communities. | ✓ | ✓ | ✓ | ||||
| Sullivan, 2005 [33] | United States | To improve understanding of the cultural context of domestic violence in King County, Washington; examine access to and satisfaction with the range of services for women who experience domestic violence; and identify women’s ideas for addressing domestic violence in their communities. | ✓ | ✓ | ✓ | ||||
| Ferré, 2010 [34] | United States | To improve the health outcomes in African American communities in LA County by enhancing the quality of care and by advancing social progress through education, training, and collaborative partnering | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Schulz, 2011 [35] | United States | To develop a multilevel intervention to address inequalities in cardiovascular disease in Detroit, Michigan | ✓ | ✓ | ✓ | ||||
| Kreuter, 2012 [36] | United States | To engage community organizations in an urban Atlanta neighbourhood to identify priority health and social or environmental problems and undertake actions to mitigate those problems. | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Montgomer, 2012 [37] | United States | To develop a curriculum that trains Native youth leaders to plan, write, and design original comic books to enhance healthy decision making. | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Abara, 2014 [38] | United States | To address community-identified health and environmental concerns in the aftermath of a chemical disaster. | ✓ | ✓ | ✓ | ✓ | |||
| Noone, 2016 [39] | United States | To engage Latino youth to address health disparities in unintended teen pregnancy rates. | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Andress & Hallie, 2017 [40] | United States | To construct a shared narrative about the food environment with older adults, specifically regarding their access to food. | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Cuervo, 2017 [41] | United States | To improve the capacity to provide ongoing disaster preparedness and occupational safety and health training for Latino immigrant labourers. | ✓ | ✓ | ✓ | ||||
| Peréa, 2019 [42] | United States | To engage urban youth in the development of local health promotion and advocacy efforts to increase physical activity. | ✓ | ✓ | ✓ | ||||
| Newman, 2020 [43] | United States | To use community engaged research and citizen science methods to derive data-driven community master plans to reduce toxic exposure and enhance resilience. | ✓ | ✓ | |||||
| Frerichs, 2020 [44] | United States | To engage adolescent youth in co-building an agent-based model of physical activity. | ✓ | ✓ | |||||
| Symanski, 2020 [45] | United States | To improve air quality and environmental health in neighbourhoods located adjacent to metal recycling facilities in Houston. | ✓ | ✓ | ✓ | ||||
| Harper, 2012 [46] | Canada | To develop a multimedia participatory, community-run methodological strategy to gather locally appropriate and meaningful data to explore climate–health relationships. | ✓ | ✓ | ✓ | ✓ | |||
| Thompson, 2018 [47] | Canada | To assess the general viability of the hoop house gardening initiative in the community and consider what role it might play in improving local food security. | ✓ | ✓ | |||||
| Ríos-Cortázar, 2014 [48] | Mexico | To promote a healthy diets, physical activity, and obesity preventive measures in an elementary school in Mexico City. | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Brännström L, 2020 [49] | Sweden | To gain increased knowledge about gendered violence against girls and young women in rural Sweden. | ✓ | ✓ | ✓ | ||||
| Ali, 2019 [50] | United Kingdom | To develop and produce culturally appropriate information resources that reflected the needs of the community. | ✓ | ✓ | |||||
| Prevo, 2020 [51] | Netherlands | To enhance community participation and improve the general wellbeing and positive health of low socioeconomic status families | ✓ | ✓ | ✓ | ✓ | |||
| Miranda, 2019 [52] | Spain | To empower the Roma community through sociopolitical awareness, promote alliances between Roma and community resources/institutions, and build a common agenda for promoting Roma health justice. | ✓ | ✓ | ✓ | ||||
| Miranda, 2022 [53] | Spain | To build capacity for health advocacy among a group of Roma neighbours living in contexts of risk of social exclusion. | ✓ | ✓ | ✓ | ||||
| Cox, 2014 [54] | Australia | To promote positive social and emotional wellbeing to increase resilience and reduce the high reported rates of psychological distress and suicide among Aboriginal and Torres Strait Islander people | ✓ | ✓ | |||||
| Gilbert, 2019 [55] | Australia | To improve health literacy among Aboriginal and Torres Strait Islander youth in preconception health, in terms of raising awareness of the determinants of health and encouraging collective actions to modify behavioural determinants. | ✓ | ✓ | ✓ | ||||
| Carr, 2021 [56] | Australia | To co-design a meaningful physical activity and lifestyle program tailored to the priorities of Aboriginal families with Machado-Joseph Disease in the Top End of Australia. | ✓ | ✓ | ✓ | ||||
| Gerritsen, 2019 [57] | New Zealand | To identify systemic barriers to children meeting fruit and vegetable (FV) guidelines and generate sustainable actions within a local community to improve children’s FV intake. | ✓ | ✓ | ✓ | ||||
| Chukwudozie, 2015 [58] | Nigeria, D.R. Congo, Sierra Leone | To enhance the understanding of kinship care arrangements, positive and negative experiences of kinship care, and influencing factors from different perspectives. | ✓ | ✓ | ✓ | ||||
| Chimberengwa & Naidoo, 2019 [59] | Zimbabwe | To improve the community’s knowledge about hypertension by positively influencing beliefs and behaviours emphasizing primary prevention. | ✓ | ✓ | ✓ | ✓ | |||
| Oladeinde, 2020 [60] | South Africa | To engage communities to nominate health concerns and generate new knowledge for action in the area of alcohol and drug use in marginalised communities in Mpumalanga, South Africa. | ✓ | ✓ | |||||
| Kabukye, 2021 [61] | Uganda | To understand the cancer awareness situation in Uganda and develop, implement, and evaluate cancer awareness messages. | ✓ | ✓ | |||||
| Methodology | Equity Focus | Community Participation * | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Health Issue Addressed | Workshops | Group Discussion | Interviews | Observation | Surveys | Economic Vulnerability | Racial Discrimination | Social Discrimination | Gender Discrimination | Agenda Setting | Design | Implementation | Evaluation |
| Rains & R. | Cardiovascular disease & Cancer | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Giachello | Diabetes | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Sullivan | Gender Violence | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Ferré | Racial health Disparities | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Schulz | Cardiovascular disease | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Kreuter | Health Disparities | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Montgomery | Tobacco control | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Abara | Environmental disaster | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Noone | Teen pregnancy | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Andress & H. | Food Security | ✓ | ✓ | ✓ | ✓ | |||||||||
| Cuervo | Disaster preparedness | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Peréa | Physical Activity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Newman | Environmental health | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Freriche | Physical Activity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Symanski | Air pollution | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Harper | Climate change | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Thompson | Food Security | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Ríos-Cortázar | Childhood obesity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Brännström | Gender Violence | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Ali | Health literacy | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
| Prevo | Health Disparities | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Miranda | Health Disparities | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Miranda | Health Disparities | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Cox | Suicide prevention | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||
| Gilbert | Reproductive health | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Carr | Physical Activity | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Gerritsen | Nutrition | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Chukwudozie | Childcare | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Chimberengwa & N. | Hypertension | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Oladeinde | Alcohol and other drug abuse | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Kabukye | Cancer | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Garzón, S.; Parker, L.A.; Hernández-Aguado, I.; González-Moro Tolosana, M.; Pastor-Valero, M.; Chilet-Rosell, E. Addressing Health Disparities through Community Participation: A Scoping Review of Co-Creation in Public Health. Healthcare 2023, 11, 1034. https://doi.org/10.3390/healthcare11071034
Morales-Garzón S, Parker LA, Hernández-Aguado I, González-Moro Tolosana M, Pastor-Valero M, Chilet-Rosell E. Addressing Health Disparities through Community Participation: A Scoping Review of Co-Creation in Public Health. Healthcare. 2023; 11(7):1034. https://doi.org/10.3390/healthcare11071034
Chicago/Turabian StyleMorales-Garzón, Sergio, Lucy Anne Parker, Ildefonso Hernández-Aguado, Manuel González-Moro Tolosana, María Pastor-Valero, and Elisa Chilet-Rosell. 2023. "Addressing Health Disparities through Community Participation: A Scoping Review of Co-Creation in Public Health" Healthcare 11, no. 7: 1034. https://doi.org/10.3390/healthcare11071034