

Developmental Strategy and Validation of the Midwifery Interventions Classification (MIC): A Delphi Study Protocol and Results from the Developmental Phase

 , ,
, ,
Abstract
:1. Introduction
Background
2. Materials and Methods
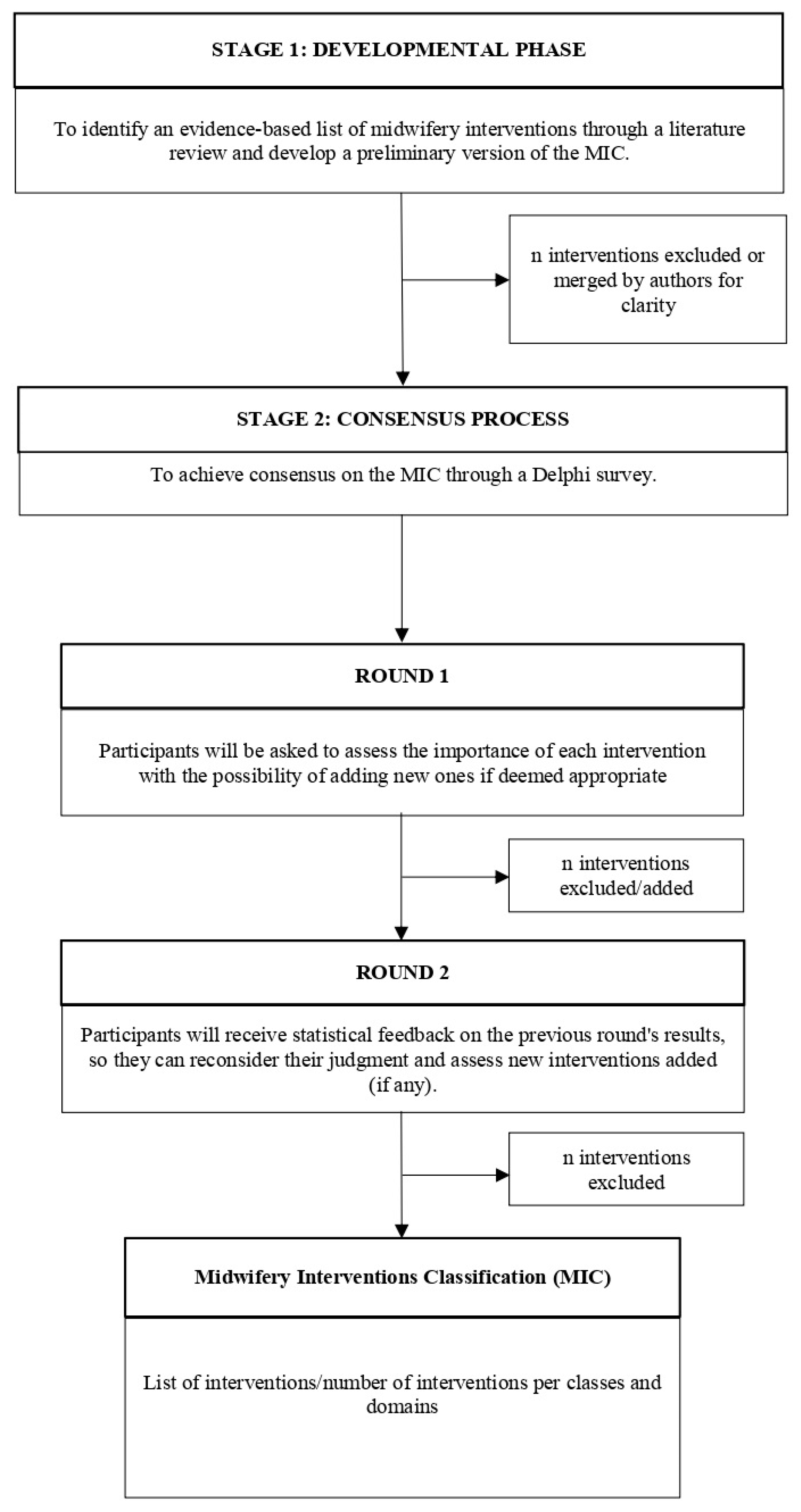
2.1. Design
2.1.1. Stage 1: Developmental Phase
2.1.2. Stage 2: Consensus Process
2.2. Participants: Panel Composition
Group Size
2.3. Data Collection and Analysis
2.3.1. Number of Rounds
2.3.2. Structure of the Questionnaire
2.3.3. Scoring System
2.3.4. Feedback between Rounds
2.3.5. Consensus Definition
2.4. Ethical Considerations
2.5. Validity and Reliability
3. Preliminary Results: Stage 1—Developmental Phase
4. Discussion of the Preliminary Results from the Stage 1—Developmental Phase
5. Expected Results from the Delphi Study
Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kennedy, H.P.; Cheyney, M.; Dahlen, H.G.; Downe, S.; Foureur, M.J.; Homer, C.S.E.; Jefford, E.; McFadden, A.; Michel-Schuldt, M.; Sandall, J.; et al. Asking Different Questions: A Call to Action for Research to Improve the Quality of Care for Every Woman, Every Child. Birth 2018, 45, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Lazzaretto, E.; Nespoli, A.; Fumagalli, S.; Colciago, E.; Perego, S.; Locatelli, A. Intrapartum Care Quality Indicators: A Literature Review. Minerva Ginecol. 2018, 70, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Maga, G.; Brigante, L.; Del Bo, E.; Cappadona, R.; Daniele, M.; Arrigoni, C.; Caruso, R.; Magon, A. The Italian Midwifery Core Outcome Set (M-COS) for Healthy Childbearing Women and Newborns: Development and Initial Validation Study. Midwifery 2022, 108, 103292. [Google Scholar] [CrossRef] [PubMed]
- Gu, C.; Lindgren, H.; Wang, X.; Zhang, Z.; Liang, S.; Ding, Y.; Qian, X. Developing a Midwifery Service Task List for Chinese Midwives in the Task-Shifting Context: A Delphi Study. BMJ Open 2021, 11, e044792. [Google Scholar] [CrossRef]
- Kazemi, A.; Beigi, M.; Najafabadi, H.E. Environmental Factors Influencing Women’s Childbirth Experiences in Labor-Delivery-Recovery-Postpartum Unit: A Qualitative Cross-Sectional Study. BMC Pregnancy Childbirth 2023, 23, 169. [Google Scholar] [CrossRef]
- Tunçalp, Ö.; Were, W.M.; MacLennan, C.; Oladapo, O.T.; Gülmezoglu, A.M.; Bahl, R.; Daelmans, B.; Mathai, M.; Say, L.; Kristensen, F.; et al. Quality of Care for Pregnant Women and Newborns-the WHO Vision. BJOG 2015, 122, 1045–1049. [Google Scholar] [CrossRef] [Green Version]
- Angelini, D.; Howard, E. Obstetric Triage: A Systematic Review of the Past Fifteen Years. MCN Am. J. Matern. Child Nurs. 2014, 39, 284–287. [Google Scholar] [CrossRef]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Meml. Fund Q. 1966, 44, 166–203. [Google Scholar] [CrossRef] [Green Version]
- Donabedian, A. The Quality of Care: How Can It Be Assessed? JAMA J. Am. Med. Assoc. 1988, 260, 1743–1748. [Google Scholar] [CrossRef]
- Arora, N.K.; Mohapatra, A.; Gopalan, H.S.; Wazny, K.; Thavaraj, V.; Rasaily, R.; Das, M.K.; Maheshwari, M.; Bahl, R.; Qazi, S.A.; et al. Setting Research Priorities for Maternal, Newborn, Child Health and Nutrition in India by Engaging Experts from 256 Indigenous Institutions Contributing over 4000 Research Ideas: A CHNRI Exercise by ICMR and INCLEN. J. Glob. Health 2017, 7, 011002. [Google Scholar] [CrossRef]
- Jamieson Gilmore, K.; Bonciani, M.; Vainieri, M. A Comparison of Census and Cohort Sampling Models for the Longitudinal Collection of User-Reported Data in the Maternity Care Pathway: Mixed Methods Study. JMIR Med. Inform. 2022, 10, e25477. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.; Kolip, P.; Schäfers, R. A Theory of the Aims and Objectives of Midwifery Practice: A Theory Synthesis. Midwifery 2020, 84, 102653. [Google Scholar] [CrossRef] [PubMed]
- Butcher, H.K.; Bulecheck, G.M.; Dochterman, J.M.; Wagner, C.M. Nursing Interventions Classification (NIC)-E-Book, 7th ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 2018; ISBN 978-0-323-49770-1. [Google Scholar]
- Renfrew, M.J.; McFadden, A.; Bastos, M.H.; Campbell, J.; Channon, A.A.; Cheung, N.F.; Silva, D.R.A.D.; Downe, S.; Kennedy, H.P.; Malata, A.; et al. Midwifery and Quality Care: Findings from a New Evidence-Informed Framework for Maternal and Newborn Care. Lancet 2014, 384, 1129–1145. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, F.; McCauley, M.; Smith, H.; van den Broek, N. Patient Reported Outcome Measures for Use in Pregnancy and Childbirth: A Systematic Review. BMC Pregnancy Childbirth 2019, 19, 155. [Google Scholar] [CrossRef]
- Tunçalp, Ö.; Were, W.; Bahl, R.; Gülmezoglu, A.M. Authors’ Reply Re: Quality of Care for Pregnant Women and Newborns-the WHO Vision. BJOG 2016, 123, 145. [Google Scholar] [CrossRef]
- Smith, V.; Daly, D.; Lundgren, I.; Eri, T.; Benstoem, C.; Devane, D. Salutogenically Focused Outcomes in Systematic Reviews of Intrapartum Interventions: A Systematic Review of Systematic Reviews. Midwifery 2014, 30, e151–e156. [Google Scholar] [CrossRef]
- Williamson, P.R.; Altman, D.G.; Bagley, H.; Barnes, K.L.; Blazeby, J.M.; Brookes, S.T.; Clarke, M.; Gargon, E.; Gorst, S.; Harman, N.; et al. The COMET Handbook: Version 1.0. Trials 2017, 18, 1–50. [Google Scholar] [CrossRef] [Green Version]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in Palliative Care: Recommendations Based on a Methodological Systematic Review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, 1–15. [Google Scholar] [CrossRef]
- Niederberger, M.; Köberich, S. Coming to Consensus: The Delphi Technique. Eur. J. Cardiovasc. Nurs. 2021, 20, 692–695. [Google Scholar] [CrossRef]
- Lee, S.I.; Eastwood, K.A.; Moss, N.; Azcoaga-Lorenzo, A.; Subramanian, A.; Anand, A.; Taylor, B.; Nelson-Piercy, C.; Yau, C.; McCowan, C.; et al. Protocol for the Development of a Core Outcome Set for Studies of Pregnant Women with Pre-Existing Multimorbidity. BMJ Open 2021, 11, e044919. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Atkins, D.; Brozek, J.; Vist, G.; Alderson, P.; Glasziou, P.; Falck-Ytter, Y.; Schünemann, H.J. GRADE Guidelines: 2. Framing the Question and Deciding on Important Outcomes. J. Clin. Epidemiol. 2011, 64, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Wylde, V.; Mackichan, F.; Bruce, J.; Gooberman-Hill, R. Assessment of Chronic Post-Surgical Pain after Knee Replacement: Development of a Core Outcome Set. Eur. J. Pain 2015, 19, 611–620. [Google Scholar] [CrossRef] [Green Version]
- Harman, N.L.; Bruce, I.A.; Kirkham, J.J.; Tierney, S.; Callery, P.; O’Brien, K.; Bennett, A.M.D.; Chorbachi, R.; Hall, P.N.; Harding-Bell, A.; et al. The Importance of Integration of Stakeholder Views in Core Outcome Set Development: Otitis Media with Effusion in Children with Cleft Palate. PLoS ONE 2015, 10, e0129514. [Google Scholar] [CrossRef] [PubMed]
- Saturno-Hernández, P.J.; Martínez-Nicolás, I.; Moreno-Zegbe, E.; Fernández-Elorriaga, M.; Poblano-Verástegui, O. Indicators for Monitoring Maternal and Neonatal Quality Care: A Systematic Review. BMC Pregnancy Childbirth 2019, 19, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pricilla, R.A.; Vasandhi David, K.; Rahman, S.P.M.F.; Angeline, N.; Siva, R.; Christal Vimala, T.J. Quality of Antenatal Care Provided by Nurse Midwives in an Urban Health Centre with Regard to Low-Risk Antenatal Mothers. Indian J. Community Med. 2017, 42, 37–42. [Google Scholar] [CrossRef]
- Obara, H.; Sobel, H. Quality Maternal and Newborn Care to Ensure a Healthy Start for Every Newborn in the World Health Organization Western Pacific Region. BJOG: Int. J. Obstet. Gynaecol. 2014, 121, 154–159. [Google Scholar] [CrossRef]
- Nababan, H.Y.; Islam, R.; Mostari, S.; Tariqujjaman, M.; Sarker, M.; Islam, M.T.; Moucheraud, C. Improving Quality of Care for Maternal and Newborn Health: A Pre-Post Evaluation of the Safe Childbirth Checklist at a Hospital in Bangladesh. BMC Pregnancy Childbirth 2017, 17, 402. [Google Scholar] [CrossRef]
- Flenady, V.; Wojcieszek, A.M.; Fjeldheim, I.; Friberg, I.K.; Nankabirwa, V.; Jani, J.V.; Myhre, S.; Middleton, P.; Crowther, C.; Ellwood, D.; et al. ERegistries: Indicators for the WHO Essential Interventions for Reproductive, Maternal, Newborn and Child Health. BMC Pregnancy Childbirth 2016, 16, 293. [Google Scholar] [CrossRef] [Green Version]
- Diamond-Smith, N.; Lin, S.; Peca, E.; Walker, D. A Landscaping Review of Interventions to Promote Respectful Maternal Care in Africa: Opportunities to Advance Innovation and Accountability. Midwifery 2022, 115, 103488. [Google Scholar] [CrossRef]
- Day, L.T.; Sadeq-ur Rahman, Q.; Ehsanur Rahman, A.; Salim, N.; Kc, A.; Ruysen, H.; Tahsina, T.; Masanja, H.; Basnet, O.; Gore-Langton, G.R.; et al. Assessment of the Validity of the Measurement of Newborn and Maternal Health-Care Coverage in Hospitals (EN-BIRTH): An Observational Study. Lancet Glob. Health 2021, 9, e267–e279. [Google Scholar] [CrossRef] [PubMed]
- Butcher, H.K.; Bulechek, G.M.; Dochterman, J.M.; Wagner, C.M. Classificazione NIC Degli Interventi Infermieristici [Nursing Interventions Classification (NIC)], 3rd ed.; Casa Editrice Ambrosiana: Rozzano, Italy, 2020; ISBN 976-88-08-78006-5. [Google Scholar]
- Ueda, K.; Kaso, M.; Ohtera, S.; Nakayama, T. Updating Quality Indicators for Low-Risk Labour Care in Japan Using Current Clinical Practice Guidelines: A Modified Delphi Method. BMJ Open 2019, 9, e023595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, K.R.; Lyndon, A.; Spetz, J.; Gay, C.L.; Landstrom, G.L. Adaptation of the MISSCARE Survey to the Maternity Care Setting. J. Obstet. Gynecol. Neonatal Nurs. 2019, 48, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Downe, S.; Finlayson, K.; Tunçalp, Ö.; Gülmezoglu, A.M. Provision and Uptake of Routine Antenatal Services: A Qualitative Evidence Synthesis. Cochrane Database Syst. Rev. 2019, 6, CD012392. [Google Scholar] [CrossRef] [PubMed]
- Lavender, D.T. Improving Quality of Care during Labour and Childbirth and in the Immediate Postnatal Period. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 36, 57–67. [Google Scholar] [CrossRef]
- Escuriet, R.; White, J.; Beeckman, K.; Frith, L.; Leon-Larios, F.; Loytved, C.; Luyben, A.; Sinclair, M.; van Teijlingen, E. Assessing the Performance of Maternity Care in Europe: A Critical Exploration of Tools and Indicators. BMC Health Serv. Res. 2015, 15, 491. [Google Scholar] [CrossRef] [Green Version]
- Devane, D.; Barrett, N.; Gallen, A.; O’Reilly, M.F.; Nadin, M.; Conway, G.; Biesty, L.; Smith, V. Identifying and Prioritising Midwifery Care Process Metrics and Indicators: A Delphi Survey and Stakeholder Consensus Process. BMC Pregnancy Childbirth 2019, 19, 198. [Google Scholar] [CrossRef]
- Blanc, A.K.; Warren, C.; McCarthy, K.J.; Kimani, J.; Ndwiga, C.; RamaRao, S. Assessing the Validity of Indicators of the Quality of Maternal and Newborn Health Care in Kenya. J. Glob. Health 2016, 6, 010405. [Google Scholar] [CrossRef]
- Alliman, J.; Stapleton, S.R.; Wright, J.; Bauer, K.; Slider, K.; Jolles, D. Strong Start in Birth Centers: Socio-demographic Characteristics, Care Processes, and Outcomes for Mothers and Newborns. Birth 2019, 46, 234–243. [Google Scholar] [CrossRef] [Green Version]
- de Carvalho, E.C.; Eduardo, A.H.A.; Romanzini, A.; Simão, T.P.; Zamarioli, C.M.; Garbuio, D.C.; Herdman, T.H. Correspondence Between NANDA International Nursing Diagnoses and Outcomes as Proposed by the Nursing Outcomes Classification. Int. J. Nurs Knowl. 2018, 29, 66–78. [Google Scholar] [CrossRef]
- Stievano, A.; Caruso, R.; Pittella, F.; Shaffer, F.A.; Rocco, G.; Fairman, J. Shaping Nursing Profession Regulation through History—A Systematic Review. Int. Nurs. Rev. 2019, 66, 17–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dell’Omodarme, C.; Bocci, G.; Troiano, G.; Rossi, S.; Kundisova, L.; Nante, N.; Alaimo, L. Midwives in England and in Italy: Two Realities Compared. Ann. Ig. 2018, 30, 14–20. [Google Scholar] [CrossRef]
- Fennelly, O.; Grogan, L.; Reed, A.; Hardiker, N.R. Use of Standardized Terminologies in Clinical Practice: A Scoping Review. Int. J. Med. Inf. 2021, 149, 104431. [Google Scholar] [CrossRef] [PubMed]
- Stothers, L.; Tsang, B.; Nigro, M.; Lazare, D.; Macnab, A. An Integrative Review of Standardized Clinical Evaluation Tool Utilization in Anticholinergic Drug Trials for Neurogenic Lower Urinary Tract Dysfunction. Spinal Cord 2016, 54, 1114–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkinson, L.; French, D.P.; Ménage, D.; Olander, E.K. Midwives’ Experiences of Referring Obese Women to Either a Community or Home-Based Antenatal Weight Management Service: Implications for Service Providers and Midwifery Practice. Midwifery 2017, 49, 102–109. [Google Scholar] [CrossRef]
- Irvine, J. Taxonomies in Education: Overview, Comparison, and Future Directions. J. Educ. Dev. 2021, 5, 1. [Google Scholar] [CrossRef]
- Caruso, R.; Arrigoni, C.; Conte, G.; Rocco, G.; Dellafiore, F.; Ambrogi, F.; Stievano, A. The Byzantine Role of Big Data Application in Nursing Science: A Systematic Review. Comput. Inform. Nurs. 2020, 39, 178–186. [Google Scholar] [CrossRef]
- Aceto, G.; Persico, V.; Pescapé, A. The Role of Information and Communication Technologies in Healthcare: Taxonomies, Perspectives, and Challenges. J. Netw. Comput. Appl. 2018, 107, 125–154. [Google Scholar] [CrossRef]
- Hasson, F.; Keeney, S.; McKenna, H. Research Guidelines for the Delphi Survey Technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar] [CrossRef] [Green Version]
- Gogovor, A.; Zomahoun, H.T.V.; Ben Charif, A.; McLean, R.K.D.; Moher, D.; Milat, A.; Wolfenden, L.; Prévost, K.; Aubin, E.; Rochon, P.; et al. Essential Items for Reporting of Scaling Studies of Health Interventions (SUCCEED): Protocol for a Systematic Review and Delphi Process. Syst. Rev. 2020, 9, 11. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
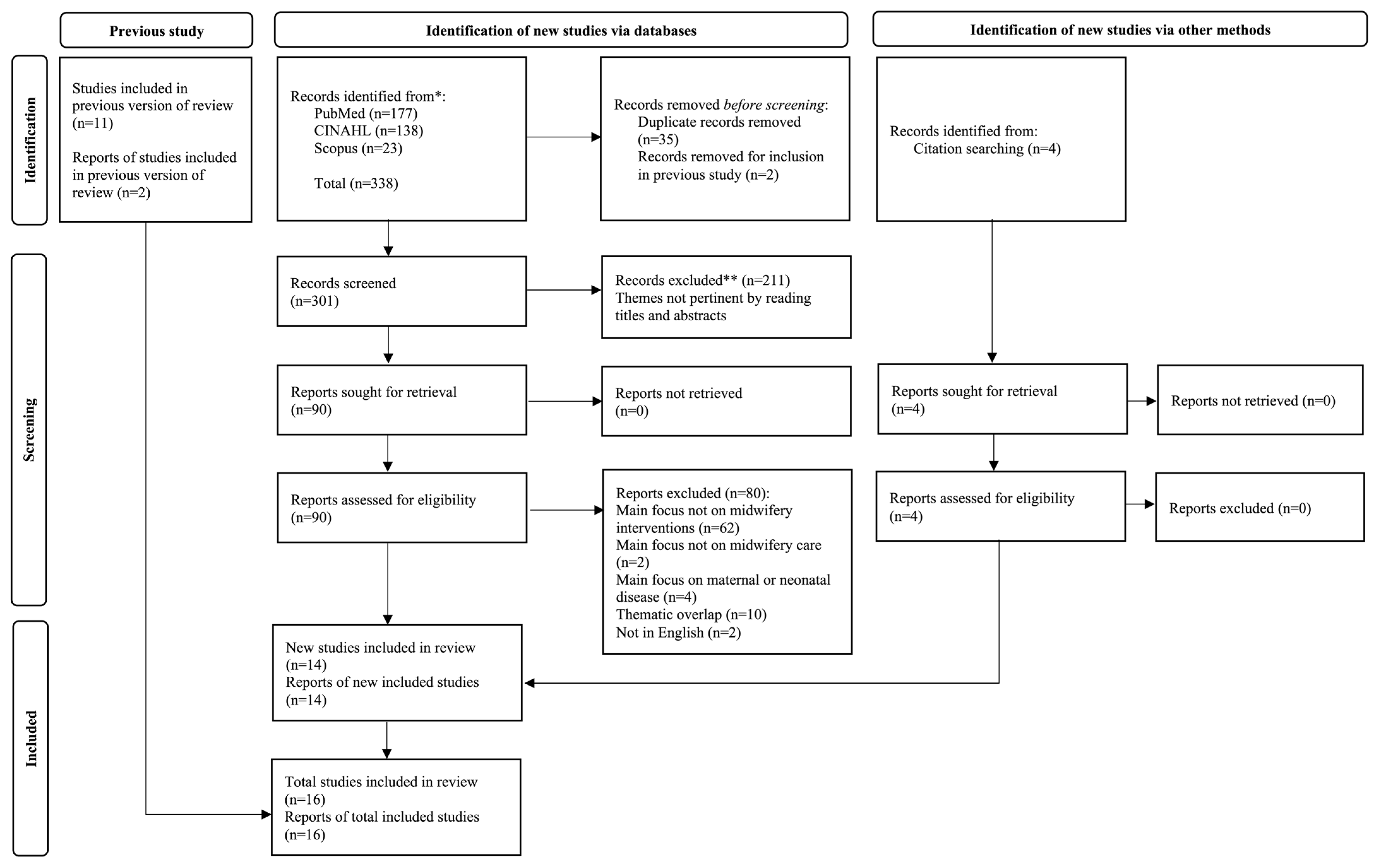
| Databases | Search Queries | Studies |
|---|---|---|
| (Last Updated on 15 February 2023) | (n) | |
| PubMed | Search (((“Maternal Health”[Mesh] or Health, Maternal)) AND (“Midwifery”[Mesh] or Midwives or midwife)) AND (“Quality Indicators, Health Care”[Mesh]OR Quality Indicators, Healthcare OR Healthcare Quality Indicator) Sort by: Best Match | 177 |
| CINAHL | AB (midwifery or midwives or midwife) AND AB maternal health AND AB (patient outcomes or quality of care) | 138 |
| Scopus | TITLE-ABS-KEY ((maternal AND health OR health, AND maternal) AND (midwifery OR midwives) AND (quality AND indicators, AND health AND care OR quality AND indicators, AND healthcare OR healthcare AND quality AND indicator)) | 23 |
| Midwifery Interventions | References | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alliman et al., 2019 [41] | Blanc et al., 2016 [40] | Butcher et al., 2020 [33] | Day et al., 2021 [32] | Devane et al., 2019 [39] | Diamond-Smith et al., 2022 [31] | Escuriet et al., 2015 [38] | Flenady et al., 2016 [30] | Lavender, 2016 [37] | Lazzaretto et al., 2018 [2] | Nababan et al., 2017 [29] | Obara et al., 2014 [28] | Pricilla et al., 2017 [27] | Saturno-Hernàndez et al., 2019 [26] | Simpson et al., 2019 [35] | Ueda et al., 2019 [34] | ||
| Italian Wording | English Wording | ||||||||||||||||
| Accoglienza in una struttura sanitaria o sociale | Reception in a healthcare or social facility | x | |||||||||||||||
| Alimentazione con biberon | Bottle feeding | x | |||||||||||||||
| Alimentazione con tazza: neonato | Cup feeding: newborn | x | |||||||||||||||
| Alimentazione del neonato | Infant feeding | x | x | x | |||||||||||||
| Alimentazione della donna | Maternal feeding | x | x | x | x | ||||||||||||
| Allattamento al seno: avvio | Breastfeeding initiation | x | x | x | x | x | x | x | x | ||||||||
| Allattamento al seno: mantenimento | Breastfeeding continuation | x | |||||||||||||||
| Ascolto attivo | Active listening | x | |||||||||||||||
| Assistenza al I stadio del travaglio | First stage of labor care attendance | x | x | ||||||||||||||
| Assistenza al II stadio del travaglio | Second stage of labor care attendance | x | x | ||||||||||||||
| Assistenza al III stadio del travaglio | Third stage of labor care attendance | x | x | x | |||||||||||||
| Assistenza al IV stadio del travaglio | Fourth stage of labor care attendance | x | x | x | |||||||||||||
| Assistenza al parto | Birth attendance | x | x | x | x | ||||||||||||
| Assistenza all’adattamento neonatale | Neonatal adaptation care | x | x | x | x | x | x | x | |||||||||
| Assistenza allo stadio prodromico del travaglio | Early labor (latent phase) care attendance | x | x | ||||||||||||||
| Assistenza domiciliare | Home care attendance | x | |||||||||||||||
| Assistenza ostetrica in gravidanza | Antenatal care (ANC) attendance | x | |||||||||||||||
| Assistenza ostetrica in puerperio | Postnatal care attendance | x | x | x | |||||||||||||
| Attuazione di meccanismi di responsabilità sociale su un’assistenza alla maternità rispettosa e dignitosa | Implementation of mechanisms for social responsibility in Respectful Maternity Care (RMC) | x | |||||||||||||||
| Cardiotocografia: gestione delle alterazioni | Cardiotocography: management of alterations | x | x | x | |||||||||||||
| Case management | Midwifery case management | x | |||||||||||||||
| Clampaggio del cordone | Cord clamping | x | x | ||||||||||||||
| Coinvolgimento del caregiver | Involvement of the caregiver | x | x | x | |||||||||||||
| Coinvolgimento di membri della comunità sull’assistenza alla maternità rispettosa e dignitosa | Involvement of community members in RMC | x | |||||||||||||||
| Collaborazione con l’équipe | Collaboration with the team | x | x | ||||||||||||||
| Condivisione di obiettivi | Sharing of objectives | x | |||||||||||||||
| Consegne ostetriche | Midwifery clinical handover | x | x | x | |||||||||||||
| Consulenza | Midwifery clinical consultation | x | |||||||||||||||
| Consulenza assistenziale multidisciplinare | Multi-disciplinary clinical consultation | x | |||||||||||||||
| Consulenza telefonica | Telephone counseling | x | |||||||||||||||
| Continuità assistenziale ostetrica (one to one) | Midwifery Led Care | x | |||||||||||||||
| Contratto con l’assistito | Contract with the assisted person | x | |||||||||||||||
| Controllo del carrello dell’emergenza | Emergency cart control | x | |||||||||||||||
| Controllo delle infezioni | Infection control | x | x | x | x | x | |||||||||||
| Counseling | Counseling | x | x | ||||||||||||||
| Counseling alle donne sulla consapevolezza di un’assistenza alla maternità rispettosa e dignitosa | Counseling on women’s awareness of RMC | x | |||||||||||||||
| Counseling sessuale | Sexual counseling | x | |||||||||||||||
| Counseling: accudimento del neonato | Counseling: infant care | x | |||||||||||||||
| Counseling: allattamento | Counseling: breastfeeding | x | x | ||||||||||||||
| Counseling: comportamenti di salute | Counseling: health behaviors | x | x | x | x | ||||||||||||
| Counseling: diagnosi prenatale | Counseling: prenatal diagnosis | x | |||||||||||||||
| Counseling: eliminazione intestinale del neonato | Counseling: infant bowel elimination | x | |||||||||||||||
| Counseling: eliminazione intestinale della donna | Counseling: maternal bowel elimination | x | |||||||||||||||
| Counseling: eliminazione urinaria del neonato | Counseling: infant urinary elimination | x | |||||||||||||||
| Counseling: eliminazione urinaria della donna | Counseling: maternal urinary elimination | x | |||||||||||||||
| Counseling: nutrizione del neonato | Counseling: infant nutrition | x | |||||||||||||||
| Counseling: nutrizione della donna | Counseling: maternal nutrition | x | x | ||||||||||||||
| Counseling: pianificazione familiare | Counseling: family planning | x | x | x | x | x | x | ||||||||||
| Counseling: segni e sintomi | Counseling: signs and symptoms | x | x | ||||||||||||||
| Counseling: sicurezza del neonato | Counseling: infant safety | x | |||||||||||||||
| Cura del cordone ombelicale | Umbilical cord care | x | x | ||||||||||||||
| Cura del perineo | Perineal care | x | x | ||||||||||||||
| Cura delle lacerazioni perineali | Perineal tears care | x | x | x | |||||||||||||
| Documentazione | Clinical documentation | x | x | x | x | x | x | x | |||||||||
| Documentazione del travaglio: partogramma | Labor clinical documentation: partograph | x | x | x | x | x | x | x | |||||||||
| Ecografia office | Obstetric Point-of-Care Ultra-sound (POCUS) | x | |||||||||||||||
| Educazione alla salute | Health education | x | x | ||||||||||||||
| Eliminazione intestinale del neonato | Infant bowel movements | x | |||||||||||||||
| Eliminazione intestinale della donna | Women’s bowel movements | x | |||||||||||||||
| Eliminazione urinaria del neonato | Infant urinary elimination | x | |||||||||||||||
| Eliminazione urinaria della donna | Women’s urinary elimination | x | x | ||||||||||||||
| Esame obiettivo del neonato | Neonatal physical examination | x | x | ||||||||||||||
| Esame obiettivo della donna | Women’s physical examination | x | x | x | |||||||||||||
| Facilitazione dell’apprendimento | Facilitation of learning | x | |||||||||||||||
| Facilitazione delle visite | Facilitation of visits | x | |||||||||||||||
| Follow-up telefonico | Telephone follow-up | x | |||||||||||||||
| Formazione del personale sanitario su un’assistenza alla maternità rispettosa e dignitosa | Training healthcare staff on RMC | x | |||||||||||||||
| Gestione degli approvvigionamenti | Management of supplies | x | |||||||||||||||
| Gestione dei campioni di laboratorio | Management of laboratory samples | x | |||||||||||||||
| Gestione dei codici di gravità | Management of severity codes | x | |||||||||||||||
| Gestione dei farmaci | Management of medications | x | |||||||||||||||
| Gestione del dolore | Pain management | x | x | x | x | x | x | ||||||||||
| Gestione dell’allergia | Allergy management | x | |||||||||||||||
| Gestione dell’ambiente | Environmental management | x | |||||||||||||||
| Gestione dell’ambiente: benessere | Environmental management: well-being | x | x | ||||||||||||||
| Gestione dell’ambiente: sicurezza | Environmental management: safety | x | |||||||||||||||
| Gestione della tecnologia | Technology management | x | |||||||||||||||
| Gestione delle profilassi del neonato | Management of neonatal prophylaxis | x | x | x | |||||||||||||
| Gestione delle risore economiche | Management of economic resources | x | |||||||||||||||
| Gestione delle vaccinazioni | Management of vaccinations | x | x | x | |||||||||||||
| Guida al sistema sanitario | Guide to the healthcare system | x | |||||||||||||||
| Guida preventiva alle situazioni critiche | Preventive guidance for critical situations | x | |||||||||||||||
| Identificazione dei rischi | Risk identification | x | |||||||||||||||
| Identificazione della persona assistita | Identification of the assisted person | x | |||||||||||||||
| Idroterapia | Hydrotherapy | x | |||||||||||||||
| Igiene del neonato | Neonatal hygiene | x | |||||||||||||||
| Igiene della donna | Women’s hygiene | x | x | ||||||||||||||
| Implementazione di programmi di miglioramento della qualità dell’assistenza | Implementation of quality improvement programs | x | |||||||||||||||
| Implementazione di regolamenti/raccomandazioni e linee guida a supporto di un’assistenza alla maternità rispettosa e dignitosa | Implementation of regulations/recommendations and guidelines to RMC | x | |||||||||||||||
| Incannulazione venosa | Venous cannulation | x | |||||||||||||||
| Interpretazione dei dati di laboratorio | Interpretation of laboratory data | x | |||||||||||||||
| Massaggio | Massage | x | |||||||||||||||
| Mediazione culturale | Cultural mediation | x | |||||||||||||||
| Miglioramento del coping | Coping improvement | x | |||||||||||||||
| Miglioramento dell’alfabetizzazione sulla salute | Health literacy improvement | x | |||||||||||||||
| Miglioramento dell’autoefficacia | Self-efficacy improvement | x | |||||||||||||||
| Miglioramento dell’autostima | Self-esteem improvement | x | |||||||||||||||
| Miglioramento della collaborazione | Collaboration improvement | x | x | x | |||||||||||||
| Miglioramento della disponibilità all’apprendimento | Improved learning availability | x | |||||||||||||||
| Miglioramento della socializzazione | Socialization improvement | x | |||||||||||||||
| Monitoraggio dei parametri vitali | Vital signs monitoring | x | x | x | x | ||||||||||||
| Monitoraggio della politica sanitaria | Health policy monitoring | x | |||||||||||||||
| Monitoraggio della qualità | Quality monitoring | x | |||||||||||||||
| Osservazione post-partum | Postpartum observation | x | x | x | x | ||||||||||||
| Personalizzazione dell’assistenza | Personalized care | x | |||||||||||||||
| Pianificazione dell’assistenza | Care planning | x | x | x | |||||||||||||
| Pianificazione della dimissione | Discharge planning | x | x | x | x | ||||||||||||
| Potenziamento del ruolo | Role empowerment | x | |||||||||||||||
| Potenziamento della consapevolezza di sé | Self-awareness empowerment | x | |||||||||||||||
| Precauzioni d’uso per il lattice | Precautions for latex use | x | |||||||||||||||
| Prelievo ematico capillare | Capillary blood sampling | x | |||||||||||||||
| Prelievo: campione di sangue venoso | Venous blood sample collection | x | |||||||||||||||
| Preparazione al parto | Antenatal class | x | x | x | |||||||||||||
| Prescrizione: test diagnostico | Prescription: diagnostic test | x | |||||||||||||||
| Prescrizione: trattamento non farmacologico | Prescription: non-pharmacological treatment | x | x | x | |||||||||||||
| Presenza | Presence | x | |||||||||||||||
| Prevenzione dell’emorragia post-partum | Prevention of postpartum hemorrhage | x | x | x | x | x | x | x | x | x | |||||||
| Prevenzione delle cadute | Fall prevention | x | |||||||||||||||
| Promozione del movimento in travaglio | Promotion of movement during labor | x | |||||||||||||||
| Promozione del ruolo genitoriale | Promotion of parental role | x | x | ||||||||||||||
| Promozione dell’attaccamento genitore-bambino | Promotion of parent–child attachment | x | x | ||||||||||||||
| Promozione dell’attività fisica | Promotion of physical activity | x | |||||||||||||||
| Promozione dell’empowerment | Empowerment promotion | x | x | x | |||||||||||||
| Promozione della cura di sé (self-care) | Self-care promotion | x | |||||||||||||||
| Promozione della normalità della nascita | Promotion of normal labor and birth | x | |||||||||||||||
| Promozione di posizioni materne libere al parto | Promotion of free maternal positions during childbirth | x | x | x | |||||||||||||
| Promozione di un’assistenza alla maternità rispettosa e dignitosa (advocacy) | Promotion of respectful maternity care (advocacy) | x | |||||||||||||||
| Promozione donazione sangue cordone ombelicale | Promotion of umbilical cord blood donation | x | |||||||||||||||
| Raccolta dati ai fine di ricerca | Data collection for research purposes | x | |||||||||||||||
| Regolazione della temperatura | Temperature regulation | x | x | x | x | x | x | x | |||||||||
| Relazione su un evento accidentale (incident reporting) | Reporting of accidental events (incident reporting) | x | |||||||||||||||
| Rooming in | Rooming in | x | |||||||||||||||
| Scambio di informazioni relative alla salute | Exchange of health information | x | |||||||||||||||
| Screening | Screening | x | x | x | x | x | |||||||||||
| Skin to skin | Skin-to-skin contact | x | x | x | x | x | x | x | |||||||||
| Somministrazione di analgesici | Administration of analgesics | x | |||||||||||||||
| Somministrazione di farmaci | Administration of medication | x | x | x | |||||||||||||
| Sorveglianza | Surveillance | x | |||||||||||||||
| Sorveglianza: gravidanza a termine | Surveillance: term pregnancy | x | |||||||||||||||
| Sorveglianza: teleassistenza | Surveillance: teleassistance | x | |||||||||||||||
| Sostegno al processo decisionale | Support for decision-making process | x | x | x | x | ||||||||||||
| Sostegno del caregiver | Support for caregiver | x | |||||||||||||||
| Sostegno emozionale | Emotional support | x | x | ||||||||||||||
| Sostegno nella gestione del comportamento | Support in behavior management | x | |||||||||||||||
| Sostegno nella modifica del comportamento | Support in behavior modification | x | |||||||||||||||
| Supervisione del personale | Personnel supervision | x | |||||||||||||||
| Supporto a chi fornisce un’assistenza alla maternità rispettosa e dignitosa | Support for those providing RMC | x | |||||||||||||||
| Sutura del perineo | Perineal suturing | x | x | x | |||||||||||||
| Sviluppo del personale | Staff development | x | |||||||||||||||
| Sviluppo della salute della comunità | Community health development | x | |||||||||||||||
| Sviluppo di programmi | Program development | x | |||||||||||||||
| Trasferimento all’interno della struttura | Transfer within the facility | x | |||||||||||||||
| Triage ostetrico | Obstetric triage | x | |||||||||||||||
| Triage telefonico | Telephone triage | x | |||||||||||||||
| Tutela dei diritti della persona assistita | Protection of the rights of the assisted person | x | |||||||||||||||
| Tutorato: personale dipendente | Staff tutoring | x | |||||||||||||||
| Tutorato: studenti | Student tutoring | x | |||||||||||||||
| Valutazione benessere fetale: battito cardiaco fetale (BCF) | Fetal well-being evaluation: fetal heart rate (FHR) | x | x | x | x | x | |||||||||||
| Valutazione benessere fetale: movimenti attivi fetali (MAF) | Fetal well-being evaluation: fetal movement (FM) | x | x | ||||||||||||||
| Valutazione dei presidi | Assessment of equipment | x | |||||||||||||||
| Valutazione del benessere emotivo | Emotional well-being assessment | x | x | x | |||||||||||||
| Valutazione del rischio ostetrico feto/neonatale | Obstetric risk assessment: fetal/neonatal | x | x | x | x | ||||||||||||
| Valutazione del rischio ostetrico materno | Obstetric risk assessment: maternal | x | x | x | x | ||||||||||||
| Valutazione dell’attività contrattile uterina (ACU) | Assessment of uterine contractions | x | x | ||||||||||||||
| Visualizzazione guidata | Guided visualization | x | |||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maga, G.; Arrigoni, C.; Brigante, L.; Cappadona, R.; Caruso, R.; Daniele, M.A.S.; Del Bo, E.; Ogliari, C.; Magon, A. Developmental Strategy and Validation of the Midwifery Interventions Classification (MIC): A Delphi Study Protocol and Results from the Developmental Phase. Healthcare 2023, 11, 919. https://doi.org/10.3390/healthcare11060919
Maga G, Arrigoni C, Brigante L, Cappadona R, Caruso R, Daniele MAS, Del Bo E, Ogliari C, Magon A. Developmental Strategy and Validation of the Midwifery Interventions Classification (MIC): A Delphi Study Protocol and Results from the Developmental Phase. Healthcare. 2023; 11(6):919. https://doi.org/10.3390/healthcare11060919
Chicago/Turabian StyleMaga, Giulia, Cristina Arrigoni, Lia Brigante, Rosaria Cappadona, Rosario Caruso, Marina Alice Sylvia Daniele, Elsa Del Bo, Chiara Ogliari, and Arianna Magon. 2023. "Developmental Strategy and Validation of the Midwifery Interventions Classification (MIC): A Delphi Study Protocol and Results from the Developmental Phase" Healthcare 11, no. 6: 919. https://doi.org/10.3390/healthcare11060919