


Spanish Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire in Handball Players
 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Ethical Considerations
The Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire
2.4. Translation and Cross-Cultural Adaptation
2.5. Questionnaires Used for Construct Validity
2.5.1. Disability of the Arm, Shoulder and Hand (DASH)
2.5.2. Knee Injury and Osteoarthritis Outcome Score (KOOS)
2.5.3. Upper Limb Functional Index (ULFI), Lower Limb Functional Index (LLFI), Spine Functional Index (SFI)
2.5.4. Roland–Morris Disability Questionnaire (RMDQ)
2.5.5. EuroQol_5D-5L/EuroQol_VAS
2.6. Data Analysis
3. Results
4. Discussion
4.1. Translation and Cross-Cultural Adaptation of the OSTRC-Sp
4.2. Reliability and Measurement Error
4.3. Construct Validity
4.4. Criterion Validity
4.5. Implications for Future Research and Clinical Use
4.6. Strengths and Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rafnsson, E.T.; Valdimarsson, Ö.; Sveinsson, T.; Árnason, Á. Injury Pattern in Icelandic Elite Male Handball Players. Clin. J. Sport Med. 2019, 29, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Karcher, C.; Buchheit, M. On-Court demands of elite handball, with special reference to playing positions. Sport. Med. 2014, 44, 797–814. [Google Scholar] [CrossRef] [PubMed]
- Ghobadi, H.; Rajabi, H.; Farzad, B.; Bayati, M.; Jeffreys, I. Anthropometry of world-class elite handball players according to the playing position: Reports from men’s handball world championship 2013. J. Hum. Kinet. 2013, 39, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bere, T.; Alonso, J.M.; Wangensteen, A.; Bakken, A.; Eirale, C.; Paul Dijkstra, H.; Ahmed, H.; Bahr, R.; Popovic, N. Injury and illness surveillance during the 24th Men’s Handball World Championship 2015 in Qatar. Br. J. Sports Med. 2015, 49, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Forget, N.J.; Higgins, J. Comparison of generic patient-reported outcome measures used with upper extremity musculoskeletal disorders: Linking process using the International Classification of Functioning, Disability, and Health (ICF). J. Rehabil. Med. 2014, 46, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bunster, J.; Mauri-Stecca, M.V.; Leppe, J.; Besomi, M. Psychometric properties of physical functional questionnaires sports population with musculoskeletal conditions of the lower limb: A systematic review. Fisioterapia 2020, 42, 185–202. [Google Scholar] [CrossRef]
- Vicente-Herrero, M.; Delgado-Bueno, S.; Ramirez-Iñiguez, T. Trauma functional assessment questionnaires. Rev. Cuba. Ortop. Traumatol. 2019, 33, 1–15. [Google Scholar]
- Clarsen, B.; Myklebust, G.; Bahr, R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire. Br. J. Sports Med. 2013, 47, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Nagano, Y.; Kobayashi-Yamakawa, K.; Higashihara, A.; Yako-Suketomo, H. Japanese translation and modification of the Oslo Sports Trauma Research Centre overuse injury questionnaire to evaluate overuse injuries in female college swimmers. PLoS ONE 2019, 14, e0215352. [Google Scholar] [CrossRef]
- Jorgensen, J.E.; Rathleff, C.R.; Rathleff, M.S.; Andreasen, J. Danish translation and validation of the Oslo Sports Trauma Research Centre questionnaires on overuse injuries and health problems. Scand. J. Med. Sci. Sports 2016, 26, 1391–1397. [Google Scholar] [CrossRef]
- Hirschmüller, A.; Steffen, K.; Fassbender, K.; Clarsen, B.; Leonhard, R.; Konstantinidis, L.; Südkamp, N.P.; Kubosch, E.J. German translation and content validation of the OSTRC Questionnaire on overuse injuries and health problems. Br. J. Sports Med. 2017, 51, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Ekman, E.; Frohm, A.; Ek, P.; Hagberg, J.; Wirén, C.; Heijne, A. Swedish translation and validation of a web-based questionnaire for registration of overuse problems. Scand. J. Med. Sci. Sports 2015, 25, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Bonet, J.M.; Rodríguez-Ponga, R.; Salamanca; María Martínez, J.A.; Bueno, R.H.; López-Vega, M.; Fernández, D.V. EL Español: Una Lengua Viva; Informe 2018; Instituto Cervantes: Madrid, Spain, 2018; Volume 72, Available online: https://cvc.cervantes.es/lengua/espanol_lengua_viva/pdf/espanol_lengua_viva_2018.pdf (accessed on 8 October 2021).
- Ruiz-Zambrana, J. La Situación Actual de la Lengua Española en el Mundo. Contribuciones a las Ciencias Sociales. Available online: https://www.eumed.net/rev/cccss/05/jrz.htm (accessed on 8 October 2021).
- Bailón-Cerezo, J.; Clarsen, B.; Sánchez-Sánchez, B.; Torres-Lacomba, M. Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Center Questionnaires on Overuse Injury and Health Problems (2nd Version) in Spanish Youth Sports. Orthop. J. Sports Med. 2020, 8, 2325967120968552. [Google Scholar] [CrossRef]
- Muñiz, J.; Elosua, P.; Hambleton, R.K. Directrices para la traducción y adaptación de los tests: Segunda edición. Psicothema 2013, 25, 151–157. [Google Scholar] [PubMed] [Green Version]
- Hernández, A.; Hidalgo, M.D.; Hambleton, R.K.; Gómez-Benito, J. International Test Commission guidelines for test adaptation: A criterion checklist. Psicothema 2020, 32, 390–398. [Google Scholar] [PubMed]
- Hervás, M.T.; Navarro Collado, M.J.; Peiró, S.; Rodrigo Pérez, J.L.; López Matéu, P.; Martínez Tello, I. Versión Española del cuestionario DASH. Adaptación transcultural, fiabilidad, validez y sensibilidad a los cambios. Med. Clin. 2006, 127, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Lizaur-Utilla, A.; Miralles-Muñoz, F.A.; Gonzalez-Parreño, S.; Lopez-Prats, F.A. Validation of the Spanish Version of the Knee Injury and Osteoarthritis Outcome Score (KOOS) for Elderly Patients With Total Knee Replacement. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2019, 37, 2157–2162. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.I.; Gabel, P.C. Cross-cultural adaptation, reliability and validity of the Spanish version of the Upper Limb Functional Index. Health Qual. Life Outcomes 2013, 11, 126. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Vargas, A.I.; Gabel, C.P.; Bennett, P. Cross cultural adaptation and validation of a Spanish version of the Lower Limb Functional Index. Health Qual. Life Outcomes 2014, 12, 75. [Google Scholar] [CrossRef] [Green Version]
- Cuesta-Vargas, A.I.; Gabel, C.P. Validation of a Spanish version of the Spine Functional Index. Health Qual. Life Outcomes 2014, 12, 96. [Google Scholar] [CrossRef] [Green Version]
- Roland, M.; Fairbank, J. The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacs, F.M.; Llobera, J.; Gil Del Real, M.T.; Abraira, V.; Gestoso, M.; Fernandez, C.; Primaria Group, K.-A. Validation of the spanish version of the Roland-Morris questionnaire. Spine 2002, 27, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López Alonso, S.R.; Navarro Casado, F.; González Rojo, J.; Martínez Sánchez, C.M.; Romero Cañadillas, A.B. Validez, fiabilidad y convergencia de COOP/WONCA y EUROQoL, administrados telefónicamente, en población con osteoartrosis de cadera y rodilla. Index Enferm. 2009, 18, 195–200. [Google Scholar] [CrossRef]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Costello, A.B.; Osborne, J.W. Best Practices in Exploratory Factor Analysis: Four Recommendations for Getting the Most From Your Analysis. Pract. Assess. Res. Eval. 2005, 10, 7. [Google Scholar]
- Stratford, P.; Gill, C.; Westaway, M.; Binkley, J. Assessing disability and change on individual patients: A report of a patient sprecific measure. Physiother. Canada 1995, 47, 258–263. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS; SAGE Publications: New York, NY, USA, 2009; ISBN 9781847879066. [Google Scholar]
- Pimenta, R.M.; Hespanhol, L.; Lopes, A.D. Brazilian version of the OSTRC Questionnaire on health problems (OSTRC-BR): Translation, cross-cultural adaptation and measurement properties. Braz. J. Phys. Ther. 2021, 25, 785–793. [Google Scholar] [CrossRef]
- Mashimo, S.; Yoshida, N.; Hogan, T.; Takegami, A.; Nishida, S.; Nagano, Y. An update of the Japanese Oslo Sports Trauma Research Center questionnaires on overuse injuries and health problems. PLoS ONE 2021, 16, e0249685. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Frequency | Percentage | Accumulated Percentage | ||
|---|---|---|---|---|
| Gender | Man | 146 | 34.2 | 34.2 |
| Woman | 281 | 65.8 | 100 | |
| Study level | Basic Education | 12 | 2.8 | 2.8 |
| Highschool | 156 | 36.5 | 39.3 | |
| University studies | 211 | 49.4 | 88.8 | |
| Postgraduate | 48 | 11.2 | 100 | |
| Civil Status | Single | 325 | 75.9 | 75.9 |
| With partner | 21 | 4.9 | 81.0 | |
| Domestic Partner | 21 | 4.9 | 85.9 | |
| Married | 60 | 14.1 | 100 | |
| Laterality | Right | 369 | 86.4 | 86.2 |
| Left | 49 | 11.5 | 97.9 | |
| Bilaterality | 9 | 2.1 | 100 | |
| Previous Injuries | No Yes | 82 345 | 19.2 80.8 | 19.2 100 |
| Region | Shoulder | 61 | 17.9 | 17.9 |
| Hand | 17 | 5.0 | 22.9 | |
| Back | 9 | 2.6 | 25.5 | |
| Hip | 4 | 1.2 | 26.7 | |
| Thigh | 54 | 15.8 | 42.5 | |
| Knee | 124 | 36.4 | 78.9 | |
| Ankle | 58 | 17.0 | 95.9 | |
| Foot | 14 | 4.1 | 100 |
| Mean ± SD (Min–Max) | ||
|---|---|---|
| Age | 25.50 ± 8.456 (18–46) | |
| Years since last injury | 4.62 ± 4.384 (0–20) | |
| OSTRC | Knee | 5.14 ± 1.987 (4–12) |
| Low Back | 5.80 ± 3.361 (4–18) | |
| Shoulder | 4.87 ± 8.818 (4–13) | |
| Total | 15.81 ± 4.706 (4–33) | |
| DASH | Disability | 51.29 ± 29.686 (12–100) |
| Sport | 49.14 ± 30.819 (0–100) | |
| Upper Limb Functional Index | 48.19 ± 30.469 (0–100) | |
| KOOS | Pain | 17.66 ± 10.234 (0–35) |
| Symptoms | 13.67 ± 8.093 (0–27) | |
| ADL_Function | 33.40 ± 20.238 (0–67) | |
| Sport | 9.65 ± 5.787 (0–19) | |
| Quality of Life | 7.20 ± 4.772 (0–15) | |
| Total | 81.58 ± 49.078 (0–163) | |
| Lower Limb Functional Index | 51.59 ± 29.306 (0–100) | |
| Spine Functional Index | 48.19 ± 30.402 (0–100) | |
| Roland Morris Questionnaire | 11.43 ± 6.839 (0–24) | |
| EuroQol_5D | 0.641 ± 0.242 (0.24–1.00) | |
| EuroQol_VAS | 47.35 ± 31.158 (0–100) | |
| N | 427 | |
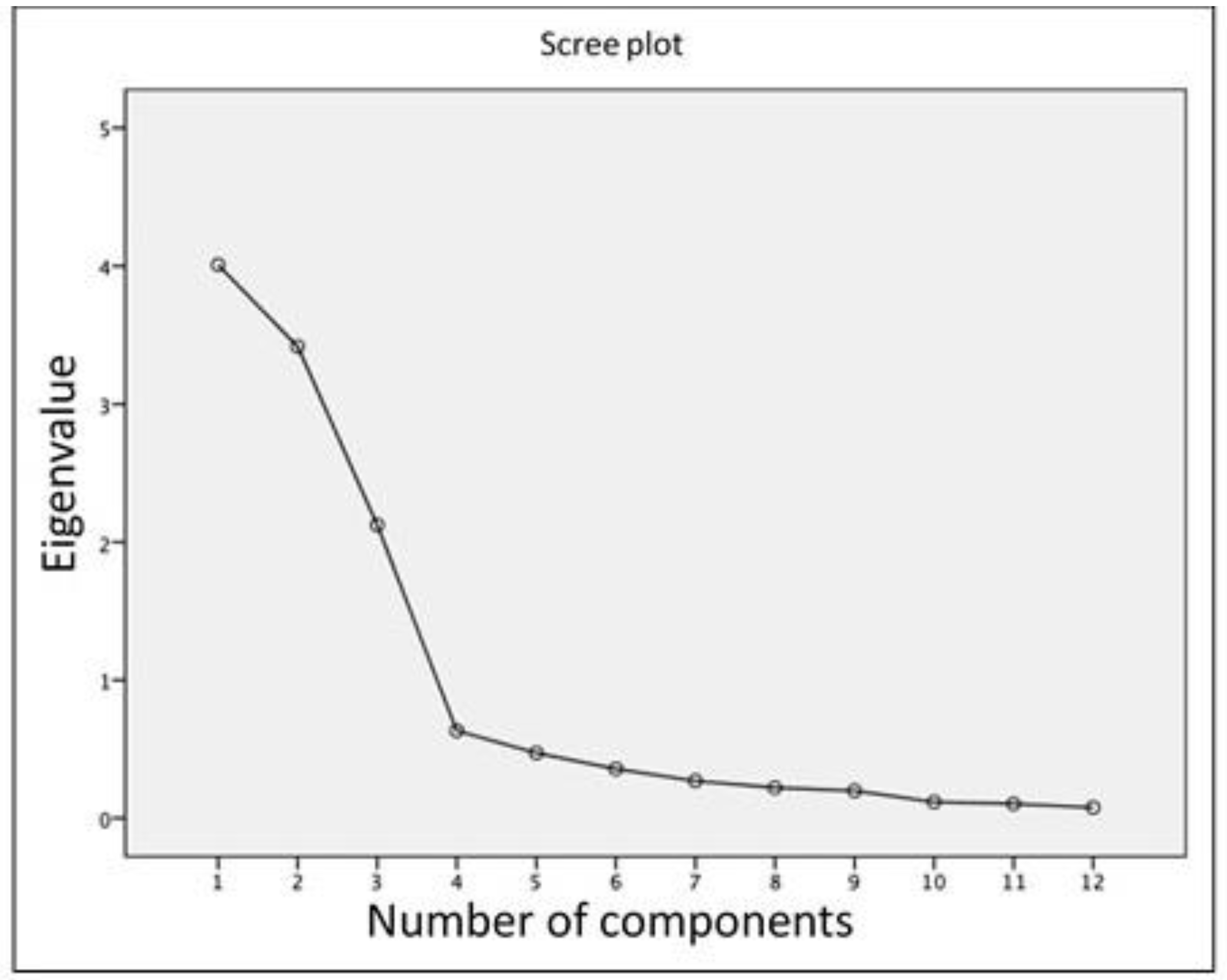
| Component | Initial Eigenvalues | Sums of Extraction of Charges Squared | ||||
|---|---|---|---|---|---|---|
| Total | % de Variance | % Accumulated | Total | % de Variance | % Accumulated | |
| 1 | 4.009 | 33.404 | 33.404 | 4.009 | 33.404 | 33.404 |
| 2 | 3.417 | 28.474 | 61.878 | 3.417 | 28.474 | 61.878 |
| 3 | 2.124 | 17.703 | 79.582 | 2.124 | 17.703 | 79.582 |
| 4 | 0.634 | 5.280 | 84.862 | |||
| 5 | 0.472 | 3.936 | 88.799 | |||
| 6 | 0.357 | 2.971 | 91.770 | |||
| 7 | 0.270 | 2.249 | 94.019 | |||
| 8 | 0.221 | 1.843 | 95.862 | |||
| 9 | 0.198 | 1.651 | 97.513 | |||
| 10 | 0.117 | 0.977 | 98.490 | |||
| 11 | 0.104 | 0.868 | 99.358 | |||
| 12 | 0.077 | 0.642 | 100.000 | |||
| Component | ||||
|---|---|---|---|---|
| 1 | 2 | 3 | ||
| OSTRC_1. Knee | Have you had any difficulties participating in normal training and competition due to knee problems during the past week? | 0.527 | 0.731 | 0.153 |
| OSTRC_2. Knee | To what extent have you reduced you training volume due to knee problems during the past week? | 0.479 | 0.792 | 0.174 |
| OSTRC_3. Knee | To what extent have knee problems affected your performance during the past week? | 0.554 | 0.759 | 0.169 |
| OSTRC_4. Knee | To what extent have you experienced knee pain related to your sport during the past week? | 0.411 | 0.810 | 0.138 |
| OSTRC_1. Lower Back | Have you had any difficulties participating in normal training and competition due to lower back problems during the past week? | 0.624 | −0.231 | −0.576 |
| OSTRC_2. Lower Back | To what extent have you reduced you training volume due to lower back problems during the past week? | 0.668 | −0.271 | −0.428 |
| OSTRC_3. Lower Back | To what extent have lower back problems affected your performance during the past week? | 0.674 | −0.201 | −0.556 |
| OSTRC_4. Lower Back | To what extent have you experienced lower back pain related to your sport during the past week? | 0.709 | −0.050 | −0.490 |
| OSTRC_1. Shoulder | Have you had any difficulties participating in normal training and competition due to shoulder problems during the past week? | 0.566 | −0.412 | 0.457 |
| OSTRC_2. Shoulder | To what extent have you reduced you training volume due to shoulder problems during the past week? | 0.577 | −0.497 | 0.315 |
| OSTRC_3. Shoulder | To what extent have shoulder problems affected your performance during the past week? | 0.565 | −0.496 | 0.551 |
| OSTRC_4. Shoulder | To what extent have you experienced shoulder pain related to your sport during the past week? | 0.510 | −0.435 | 0.589 |
| OSTRC | |||||
|---|---|---|---|---|---|
| Knee | Back | Shoulder | Total | ||
| OSTRC | Knee_Total | 1 | 0.016 | 0.222 ** | 0.405 ** |
| Back_Total | 0.016 | 1 | 0.223 ** | 0.784 ** | |
| Shoulder_Total | 0.222 ** | 0.223 ** | 1 | 0.599 ** | |
| Total | 0.405 ** | 0.784 ** | 0.599 ** | 1 | |
| Lower Limb Functional Index | 0.581 ** | 0.398 ** | 0.490 ** | 0.866 ** | |
| KOOS | Pain | 0.595 ** | 0.397 ** | 0.504 ** | 0.881 ** |
| Symptoms | 0.584 ** | 0.401 ** | 0.493 ** | 0.870 ** | |
| ADL_Function | 0.585 ** | 0.399 ** | 0.496 ** | 0.872 ** | |
| Sport | 0.585 ** | 0.398 ** | 0.491 ** | 0.868 ** | |
| QoL | 0.593 ** | 0.400 ** | 0.497 ** | 0.875 ** | |
| Total | 0.588 ** | 0.400 ** | 0.497 ** | 0.874 ** | |
| Spine Functional Index | 0.405 ** | 0.595 ** | 0.495 ** | 0.877 ** | |
| Roland-Morris Questionnaire | −0.281 ** | −0.565 ** | −0.363 ** | −0.665 ** | |
| Upper Limb Functional Index | 0.401 ** | 0.491 ** | 0.584 ** | 0.867 ** | |
| DASH | Disability | 0.403 ** | 0.493 ** | 0.592 ** | 0.870 ** |
| DASH_Sport | 0.396 ** | 0.482 ** | 0.604 ** | 0.870 ** | |
| EuroQoL | EuroQoL_5D | −0.337 ** | −0.525 ** | −0.401 ** | −0.699 ** |
| EuroQoL_VAS | 0.361 ** | 0.543 ** | 0.424 ** | 0.787 ** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Cal, J.; Molina-Torres, G.; Carrasco-Vega, E.; Barni, L.; Ventura-Miranda, M.I.; Gonzalez-Sanchez, M. Spanish Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire in Handball Players. Healthcare 2023, 11, 912. https://doi.org/10.3390/healthcare11060912
Martínez-Cal J, Molina-Torres G, Carrasco-Vega E, Barni L, Ventura-Miranda MI, Gonzalez-Sanchez M. Spanish Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire in Handball Players. Healthcare. 2023; 11(6):912. https://doi.org/10.3390/healthcare11060912
Chicago/Turabian StyleMartínez-Cal, Jesús, Guadalupe Molina-Torres, Elio Carrasco-Vega, Luca Barni, María Isabel Ventura-Miranda, and Manuel Gonzalez-Sanchez. 2023. "Spanish Cross-Cultural Adaptation and Validation of the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire in Handball Players" Healthcare 11, no. 6: 912. https://doi.org/10.3390/healthcare11060912