
Explainable Machine Learning to Predict Successful Weaning of Mechanical Ventilation in Critically Ill Patients Requiring Hemodialysis


Abstract
:1. Introduction
2. Materials and Methods
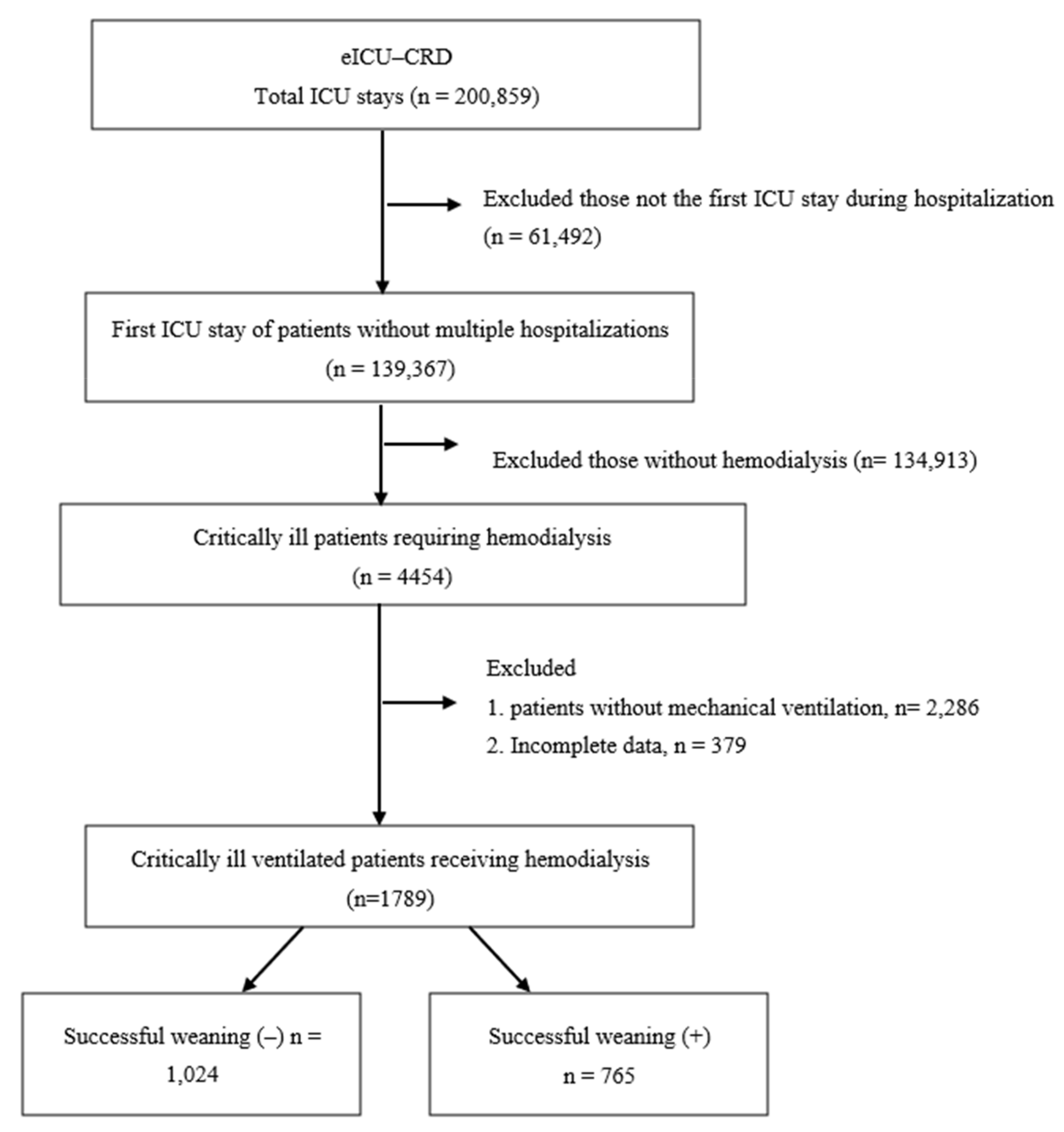
2.1. Source of Data
2.2. Machine Learning Models
2.3. Statistical Analysis
3. Results
3.1. Demographics and Basic Characteristics
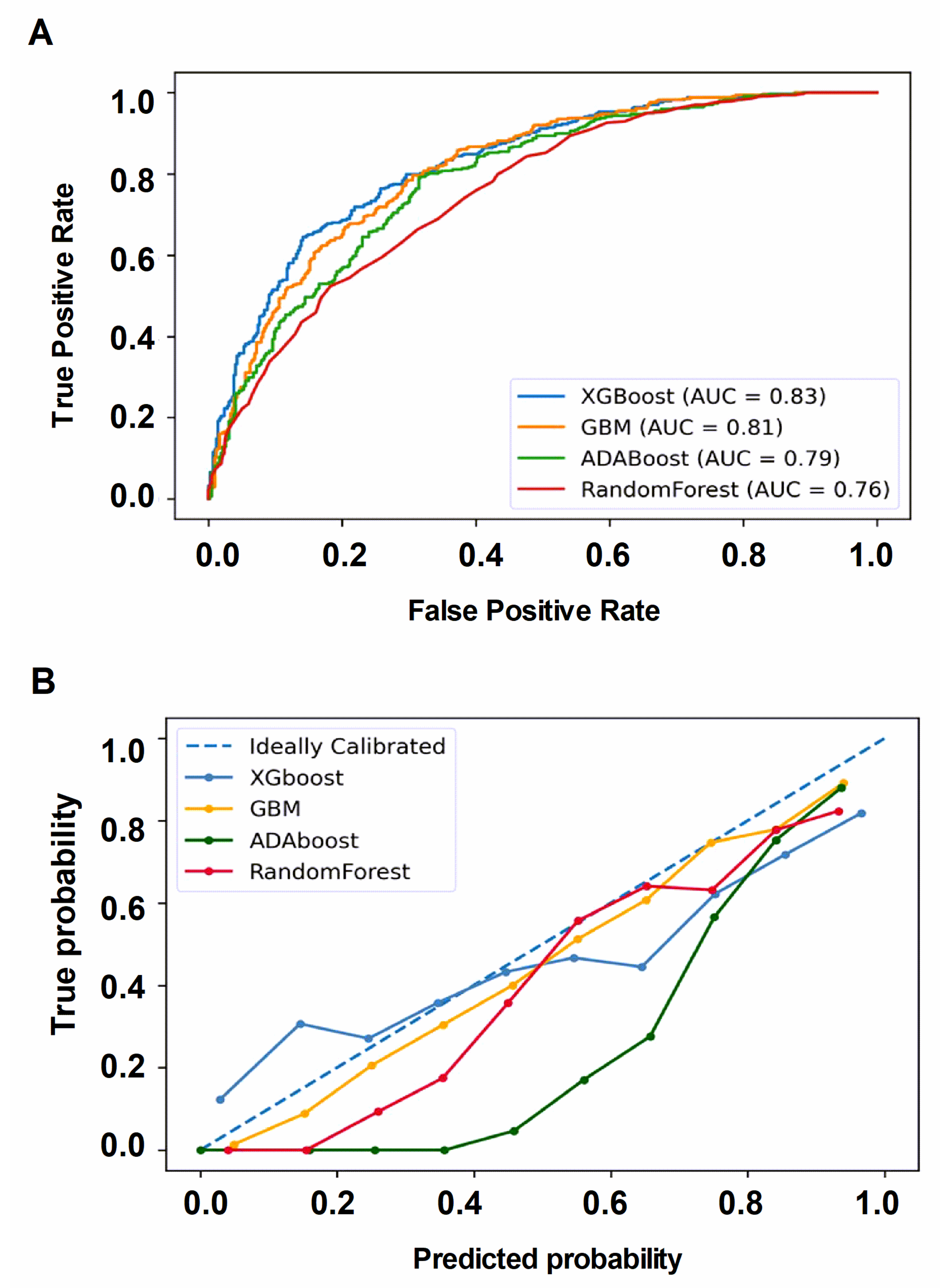
3.2. Performance of the Four Machine Learning Models
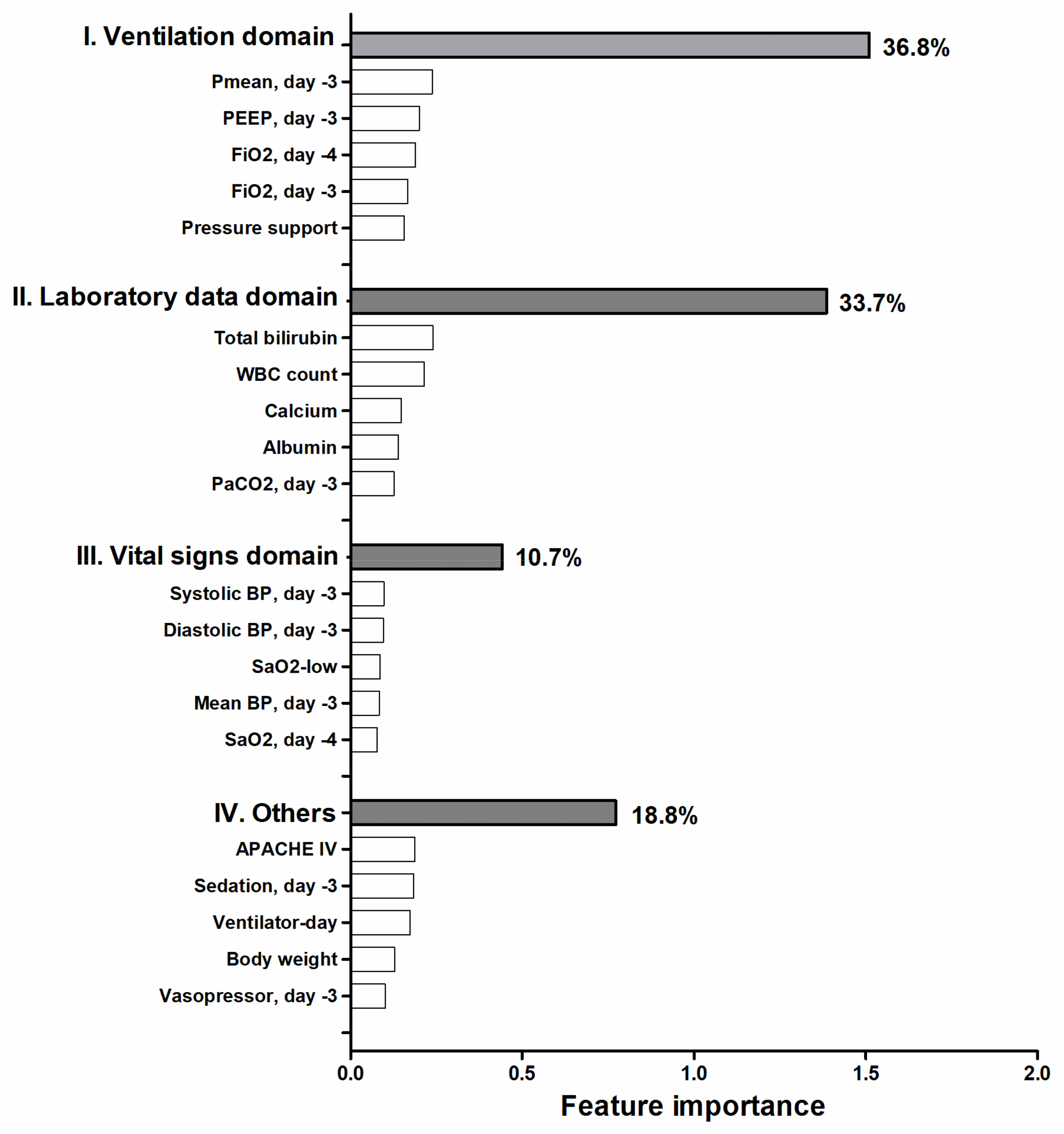
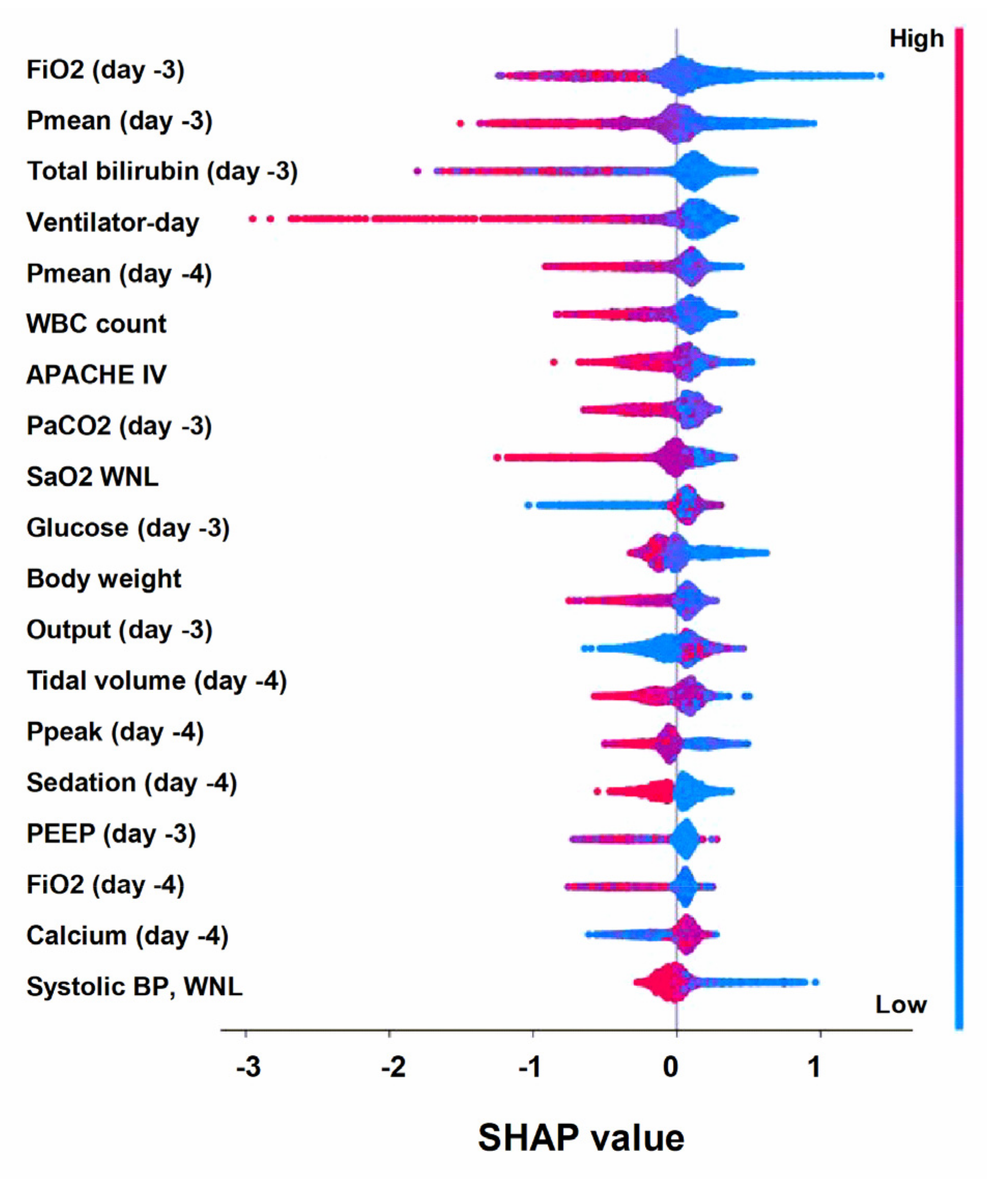
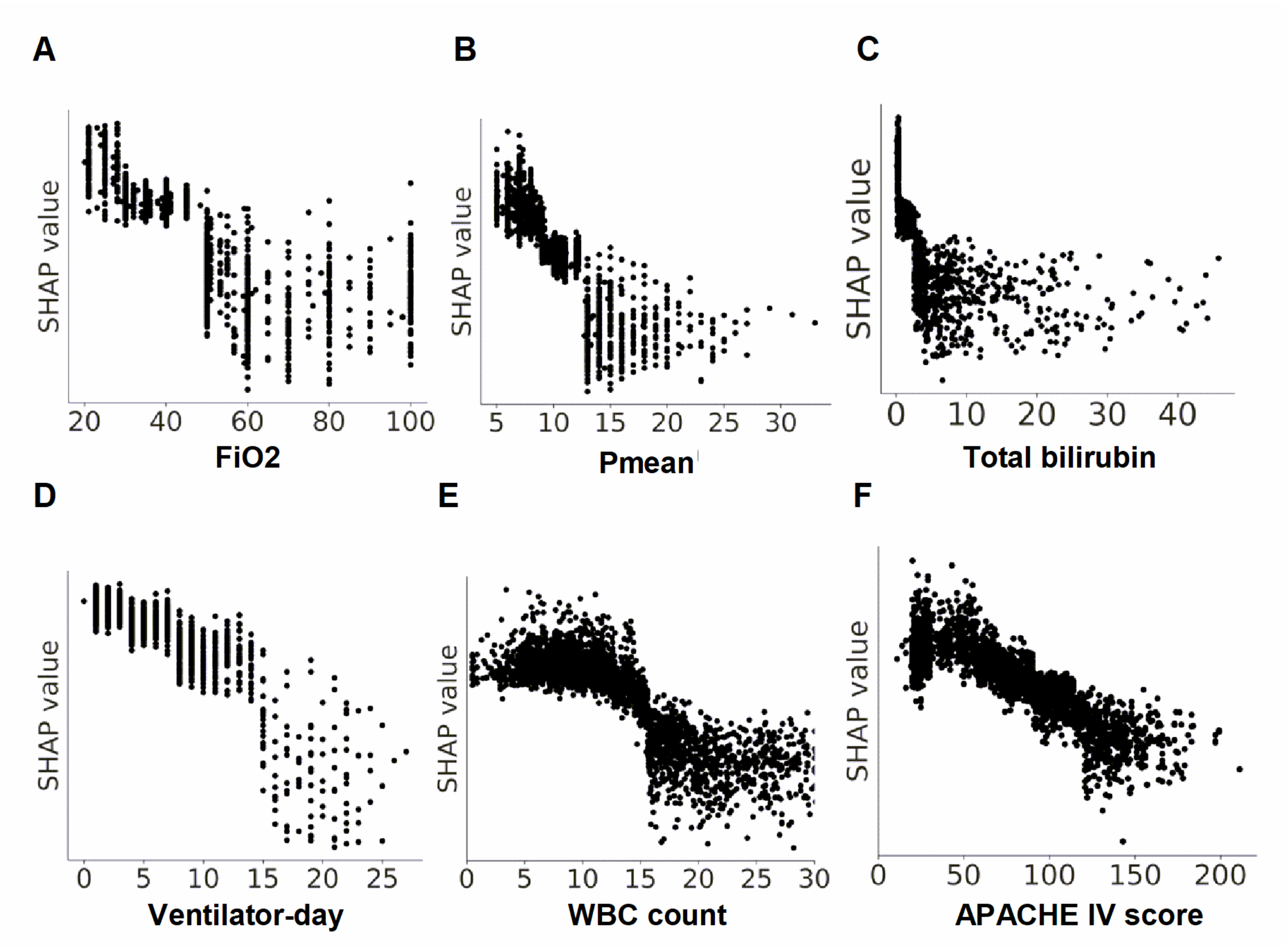
3.3. Global Explanation of the ML Model at the Clinical Domain and Feature Level
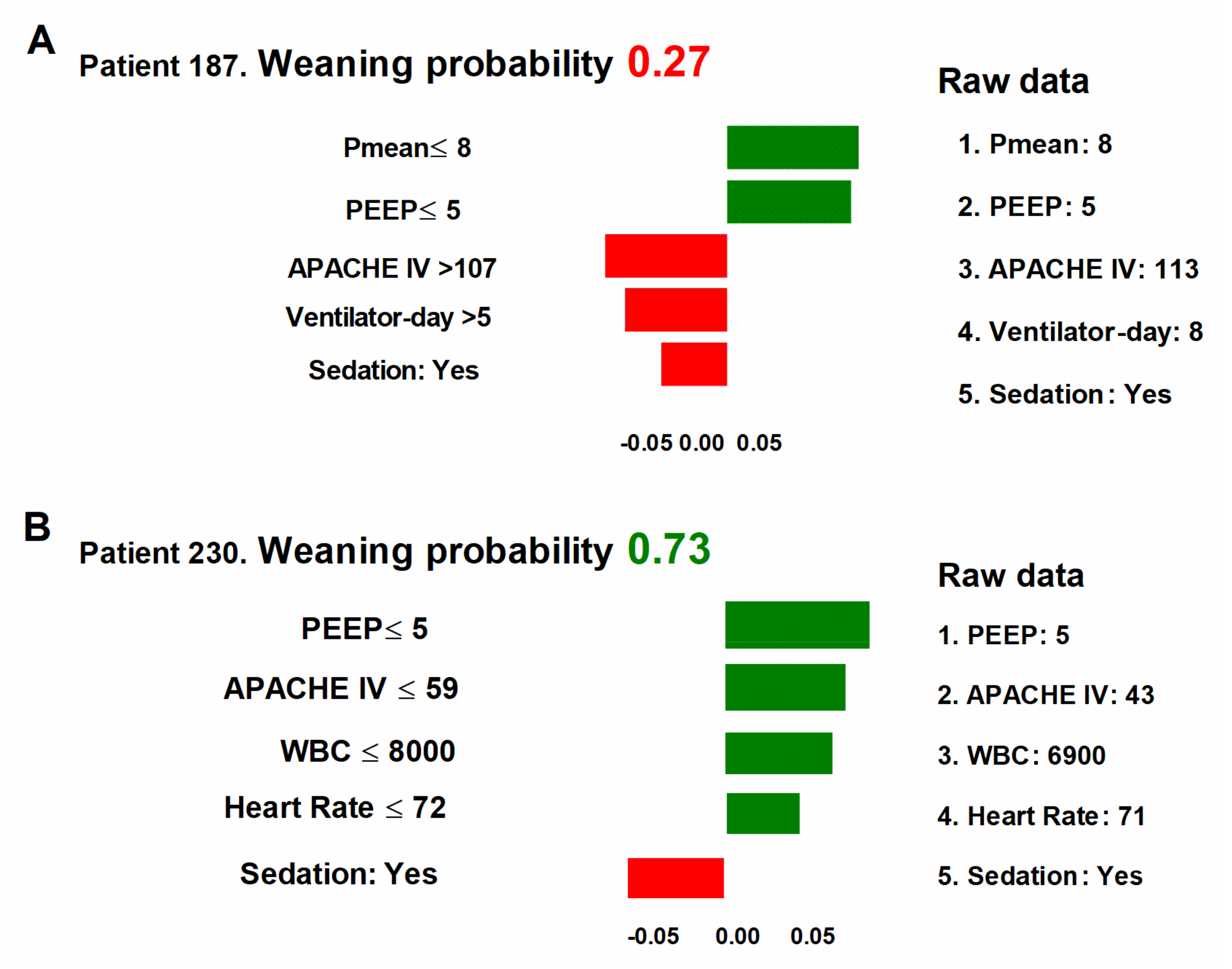
3.4. Local Explanation of the ML Model for Successful Extubation Prediction of the Individual Patient
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faubel, S.; Edelstein, C.L. Mechanisms and mediators of lung injury after acute kidney injury. Nat. Rev. Nephrol. 2016, 12, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Husain-Syed, F.; Slutsky, A.S.; Ronco, C. Lung-Kidney Cross-Talk in the Critically Ill Patient. Am. J. Respir. Crit. Care Med. 2016, 194, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Fleuren, L.M.; Dam, T.A.; Tonutti, M.; de Bruin, D.P.; Lalisang, R.C.A.; Gommers, D.; Cremer, O.L.; Bosman, R.J.; Rigter, S.; Wils, E.J.; et al. Predictors for extubation failure in COVID-19 patients using a machine learning approach. Crit. Care 2021, 25, 448. [Google Scholar] [CrossRef]
- Lin, M.Y.; Li, C.C.; Lin, P.H.; Wang, J.L.; Chan, M.C.; Wu, C.L.; Chao, W.C. Explainable Machine Learning to Predict Successful Weaning Among Patients Requiring Prolonged Mechanical Ventilation: A Retrospective Cohort Study in Central Taiwan. Front. Med. 2021, 8, 663739. [Google Scholar] [CrossRef]
- Liu, W.; Tao, G.; Zhang, Y.; Xiao, W.; Zhang, J.; Liu, Y.; Lu, Z.; Hua, T.; Yang, M. A Simple Weaning Model Based on Interpretable Machine Learning Algorithm for Patients With Sepsis: A Research of MIMIC-IV and eICU Databases. Front. Med. 2021, 8, 814566. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Hou, C.C.; Wu, V.C.; Lu, H.M.; Wang, C.Y.; Chen, L.; Kao, T.W. The impact of dialysis-requiring acute kidney injury on long-term prognosis of patients requiring prolonged mechanical ventilation: Nationwide population-based study. PLoS ONE 2012, 7, e50675. [Google Scholar] [CrossRef]
- Vieira, J.M., Jr.; Castro, I.; Curvello-Neto, A.; Demarzo, S.; Caruso, P.; Pastore, L., Jr.; Imanishe, M.H.; Abdulkader, R.C.; Deheinzelin, D. Effect of acute kidney injury on weaning from mechanical ventilation in critically ill patients. Crit. Care Med. 2007, 35, 184–191. [Google Scholar] [CrossRef]
- Datta, D.; Foley, R.J.; Wu, R.; Grady, J.; Scalise, P. Renal Function, Weaning, and Survival in Patients With Ventilator-Dependent Respiratory Failure. J. Intensive Care Med. 2019, 34, 212–217. [Google Scholar] [CrossRef]
- Vemuri, S.V.; Rolfsen, M.L.; Sykes, A.V.; Takiar, P.G.; Leonard, A.J.; Malhotra, A.; Spragg, R.G.; Macedo, E.; Hepokoski, M.L. Association Between Acute Kidney Injury During Invasive Mechanical Ventilation and ICU Outcomes and Respiratory System Mechanics. Crit. Care Explor. 2022, 4, e0720. [Google Scholar] [CrossRef]
- Hepokoski, M.; Englert, J.A.; Baron, R.M.; Crotty-Alexander, L.E.; Fuster, M.M.; Beitler, J.R.; Malhotra, A.; Singh, P. Ventilator-induced lung injury increases expression of endothelial inflammatory mediators in the kidney. Am. J. Physiol. Renal. Physiol. 2017, 312, F654–F660. [Google Scholar] [CrossRef] [Green Version]
- Hepokoski, M.; Wang, J.; Li, K.; Li, Y.; Gupta, P.; Mai, T.; Moshensky, A.; Alotaibi, M.; Crotty Alexander, L.E.; Malhotra, A.; et al. Altered lung metabolism and mitochondrial DAMPs in lung injury due to acute kidney injury. Am. J. Physiol. Lung Cell. Mol. Physiol. 2021, 320, L821–L831. [Google Scholar] [CrossRef]
- Pollard, T.J.; Johnson, A.E.W.; Raffa, J.D.; Celi, L.A.; Mark, R.G.; Badawi, O. The eICU Collaborative Research Database, a freely available multi-center database for critical care research. Sci. Data 2018, 5, 180178. [Google Scholar] [CrossRef]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Lehman, L.W.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [Green Version]
- The U.S. Food and Drug Administration. Good Machine Learning Practice for Medical Device Development: Guiding Principles; The U.S. Food and Drug Administration: Washington, DC, USA, 2021. [Google Scholar]
- Hu, C.A.; Chen, C.M.; Fang, Y.C.; Liang, S.J.; Wang, H.C.; Fang, W.F.; Sheu, C.C.; Perng, W.C.; Yang, K.Y.; Kao, K.C.; et al. Using a machine learning approach to predict mortality in critically ill influenza patients: A cross-sectional retrospective multicentre study in Taiwan. BMJ Open 2020, 10, e033898. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.C.; Pai, K.C.; Su, S.A.; Wang, M.S.; Wu, C.L.; Chao, W.C. Explainable machine learning to predict long-term mortality in critically ill ventilated patients: A retrospective study in central Taiwan. BMC Med. Inform. Decis. Mak. 2022, 22, 75. [Google Scholar] [CrossRef]
- Lundberg, S.M.; Lee, S.I. A Unified Approach to Interpreting Model Predictions. arXiv 2018, arXiv:1705.07874v2. [Google Scholar]
- Hvitfeldt, E.; Pedersen, T.L.; Benesty, M. lime: Local Interpretable Model-Agnostic Explanations. 2018. Available online: https://CRAN.R-project.org/package=lime (accessed on 1 February 2023).
- Joannidis, M.; Forni, L.G.; Klein, S.J.; Honore, P.M.; Kashani, K.; Ostermann, M.; Prowle, J.; Bagshaw, S.M.; Cantaluppi, V.; Darmon, M.; et al. Lung-kidney interactions in critically ill patients: Consensus report of the Acute Disease Quality Initiative (ADQI) 21 Workgroup. Intensive Care Med. 2020, 46, 654–672. [Google Scholar] [CrossRef] [Green Version]
- Van den Akker, J.P.; Egal, M.; Groeneveld, A.B. Invasive mechanical ventilation as a risk factor for acute kidney injury in the critically ill: A systematic review and meta-analysis. Crit. Care 2013, 17, R98. [Google Scholar] [CrossRef] [Green Version]
- Chao, W.C.; Tseng, C.H.; Wu, C.L.; Shih, S.J.; Yi, C.Y.; Chan, M.C. Higher glycemic variability within the first day of ICU admission is associated with increased 30-day mortality in ICU patients with sepsis. Ann. Intensive. Care 2020, 10, 17. [Google Scholar] [CrossRef] [Green Version]
- Hoong, C.W.S.; Yeo, X.E.; Lin, Y.; Ooi, S.T.; Yeoh, E. High glycaemic variability is associated with progression of COVID-19. Acta Diabetol. 2021, 58, 1701–1704. [Google Scholar] [CrossRef]
- Park, S.; Kim, W.J.; Cho, N.J.; Choi, C.Y.; Heo, N.H.; Gil, H.W.; Lee, E.Y. Predicting intradialytic hypotension using heart rate variability. Sci. Rep. 2019, 9, 2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorsen-Meyer, H.C.; Nielsen, A.B.; Nielsen, A.P.; Kaas-Hansen, B.S.; Toft, P.; Schierbeck, J.; Strom, T.; Chmura, P.J.; Heimann, M.; Dybdahl, L.; et al. Dynamic and explainable machine learning prediction of mortality in patients in the intensive care unit: A retrospective study of high-frequency data in electronic patient records. Lancet Digit. Health 2020, 2, e179–e191. [Google Scholar] [CrossRef]
- Teboul, J.L.; Monnet, X.; Chemla, D.; Michard, F. Arterial Pulse Pressure Variation with Mechanical Ventilation. Am. J. Respir. Crit. Care Med. 2019, 199, 22–31. [Google Scholar] [CrossRef]
- Bakker, J.; Kattan, E.; Annane, D.; Castro, R.; Cecconi, M.; De Backer, D.; Dubin, A.; Evans, L.; Gong, M.N.; Hamzaoui, O.; et al. Current practice and evolving concepts in septic shock resuscitation. Intensive Care Med. 2021, 48, 148–163. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; McIntyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- European Commission, Directorate-General for Communications Networks, Content and Technology. Ethics Guidelines for Trustworthy AI; European Commission: Brussels, Belgium, 2019. [Google Scholar]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonca, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Rostami, M.; Oussalah, M. A novel explainable COVID-19 diagnosis method by integration of feature selection with random forest. Inform. Med. Unlocked 2022, 30, 100941. [Google Scholar] [CrossRef]
- Yoon, J.H.; Pinsky, M.R.; Clermont, G. Artificial Intelligence in Critical Care Medicine. Crit. Care 2022, 26, 75. [Google Scholar] [CrossRef]
- Perren, A.; Brochard, L. The importance of timing for the spontaneous breathing trial. Ann. Transl. Med. 2019, 7, S210. [Google Scholar] [CrossRef]
- Fleuren, L.M.; Thoral, P.; Shillan, D.; Ercole, A.; Elbers, P.W.G. Right Data Right Now C. Machine learning in intensive care medicine: Ready for take-off? Intensive Care Med. 2020, 46, 1486–1488. [Google Scholar] [CrossRef]
- Rostami, M.; Muhammad, U.; Forouzandeh, S.; Berahmand, K.; Farrahi, V.; Oussalah, M. An effective explainable food recommendation using deep image clustering and community detection. Intell. Syst. Appl. 2022, 16, 200157. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Successful Weaning (−) | Successful Weaning (+) | p-Value | |
|---|---|---|---|---|
| N = 1789 | N = 1024 | N = 765 | ||
| Demographic data | ||||
| Age (years) | 62.1 ± 14.2 | 62.3 ± 14.1 | 61.8 ± 14.3 | 0.393 |
| Sex (male) | 1018 (56.9%) | 568 (55.5%) | 450 (58.8%) | 0.156 |
| Body weight (kg) | 88.2 ± 27.7 | 90.4 ± 29.8 | 85.4 ± 24.3 | <0.001 |
| Height (cm) | 169.6 ± 11.3 | 169.8 ± 11.8 | 169.4 ± 10.6 | 0.453 |
| End-stage renal disease | 530 (29.6%) | 229 (22.4%) | 301 (39.3%) | <0.001 |
| APACHE IV | 83.8 ± 37.2 | 89.9 ± 39.3 | 75.6 ± 32.4 | <0.001 |
| Ethnicity | 0.520 | |||
| African American | 254 (14.2%) | 144 (14.1%) | 110 (14.4) | |
| Asian | 17 (1.0%) | 8 (0.8%) | 9 (1.2%) | |
| Caucasian | 1094 (61.2%) | 644 (62.8%) | 450 (58.8%) | |
| Hispanic | 79 (4.4%) | 39 (3.8%) | 40 (5.2%) | |
| Native American | 28 (1.6%) | 22 (2.1%) | 6 (0.8%) | |
| Other | 317 (17.8%) | 167 (16.3%) | 150 (19.6%) | |
| Ventilatory parameters | ||||
| FiO2 (%) | 48.4 ± 19.2 | 52.0 ± 20.6 | 43.6 ± 16.0 | <0.001 |
| PEEP (cmH2O) | 6.1 ± 2.5 | 6.5 ± 2.9 | 5.5 ± 1.6 | <0.001 |
| VT (mL) | 482.1 ± 134.7 | 489.5 ± 124.5 | 472.1 ± 146.7 | 0.007 |
| Ppeak, (cmH2O) | 20.4 ± 5.2 | 21.2 ± 5.3 | 19.3 ± 4.8 | <0.001 |
| Pmean, (cmH2O) | 10.5 ± 3.2 | 11.1 ± 3.5 | 9.7 ± 2.4 | <0.001 |
| Laboratory data | ||||
| White blood cell count (count/μL) | 15.9 ± 10.2 | 17.3 ± 11.2 | 14.0 ± 8.3 | <0.001 |
| Hemoglobin (g/dL) | 9.9 ± 2.0 | 10.0 ± 2.0 | 9.9 ± 1.9 | 0.587 |
| Platelet (103/μL) | 181.8 ± 111.8 | 172.6 ± 111.2 | 194.1 ± 111.5 | <0.001 |
| Total bilirubin (mg/dL) | 2.3 ± 4.5 | 2.9 ± 5.2 | 1.6 ± 3.4 | <0.001 |
| Lactate (mmol/L) | 4.4 ± 4.1 | 5.1 ± 4.8 | 3.4 ± 2.7 | <0.001 |
| HCO3 (mmol/L) | 23.7 ± 4.7 | 23.1 ± 5.0 | 24.3 ± 4.2 | <0.001 |
| PaCO2 (cmH2O) | 44.7 ± 13.5 | 45.1 ± 14.3 | 44.2 ± 12.4 | 0.188 |
| Vital signs and fluid balance | ||||
| Systolic blood pressure (mmHg) | 118.5 ± 28.1 | 112.8 ± 26.3 | 126.1 ± 28.6 | <0.001 |
| Diastolic blood pressure (mmHg) | 61.9 ± 18.3 | 59.4 ± 16.7 | 65.3 ± 19.7 | <0.001 |
| Mean blood pressure (mmHg) | 78.1 ± 22.1 | 74.1 ± 19.4 | 83.5 ± 24.2 | <0.001 |
| Heart rate (per minute) | 90.8 ± 20.8 | 93.6 ± 21.2 | 87.1 ± 19.6 | <0.001 |
| Respiratory rate (per minute) | 17.8 ± 6.3 | 17.8 ± 6.5 | 17.9 ± 5.9 | 0.826 |
| Oxygen saturation (%) | 96.6 ± 6.1 | 96.1 ± 6.5 | 97.3 ± 5.6 | <0.001 |
| Daily input, mL | 1938.6 ± 1729.4 | 2112.7 ± 1832.7 | 1705.4 ± 1550.2 | <0.001 |
| Daily output, mL | 1096.6 ± 1677.2 | 1147.1 ± 1806.6 | 1029.0 ± 1484.0 | 0.141 |
| Ultrafiltration, mL | −2090.6 ± 1025.4 | −2058.4 ± 975.8 | −2133.8 ± 1086.8 | 0.51 |
| Outcome | ||||
| ICU length of stay (day) | 7.8 ± 7.9 | 9.5 ± 8.6 | 5.6 ± 6.2 | 0.118 |
| Ventilator day (day) | 6.0 ± 6.2 | 7.9 ± 7.3 | 3.4 ± 2.8 | 0.004 |
| Hospital stay (day) | 17.3 ± 16.7 | 17.8 ± 17.1 | 16.5 ± 16.1 | 0.747 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, M.-Y.; Chang, Y.-M.; Li, C.-C.; Chao, W.-C. Explainable Machine Learning to Predict Successful Weaning of Mechanical Ventilation in Critically Ill Patients Requiring Hemodialysis. Healthcare 2023, 11, 910. https://doi.org/10.3390/healthcare11060910
Lin M-Y, Chang Y-M, Li C-C, Chao W-C. Explainable Machine Learning to Predict Successful Weaning of Mechanical Ventilation in Critically Ill Patients Requiring Hemodialysis. Healthcare. 2023; 11(6):910. https://doi.org/10.3390/healthcare11060910
Chicago/Turabian StyleLin, Ming-Yen, Yuan-Ming Chang, Chi-Chun Li, and Wen-Cheng Chao. 2023. "Explainable Machine Learning to Predict Successful Weaning of Mechanical Ventilation in Critically Ill Patients Requiring Hemodialysis" Healthcare 11, no. 6: 910. https://doi.org/10.3390/healthcare11060910