
Serious Long-Term Effects of Head and Neck Cancer from the Survivors’ Point of View
 , , , , ,
, , , , ,  ,
,  , , , , , , , , , , and add
Show full author list
, , , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods
3. Results
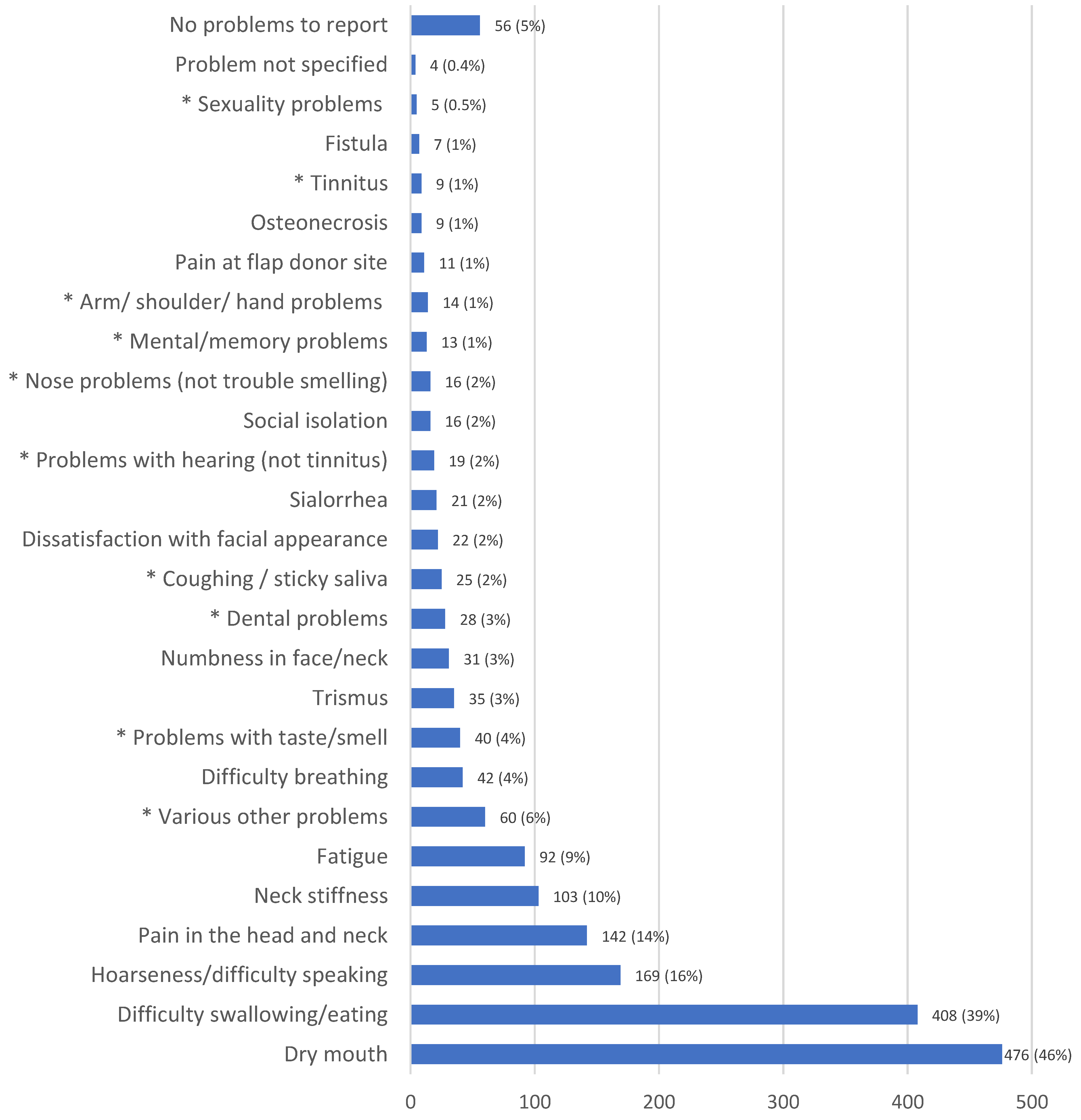
3.1. Frequency of Problems Reported
3.2. Associations of Four Most Frequently Mentioned Problems with Survivor Characteristics
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Pulte, D.; Brenner, H. Changes in survival in head and neck cancers in the late 20th and early 21st century: A period analysis. Oncologist 2010, 15, 994–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loorents, V.; Rosell, J.; Willner, H.S.; Borjeson, S. Health-related quality of life up to 1 year after radiotherapy in patients with head and neck cancer (HNC). Springerplus 2016, 5, 669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaelsen, S.H.; Gronhoj, C.; Michaelsen, J.H.; Friborg, J.; von Buchwald, C. Quality of life in survivors of oropharyngeal cancer: A systematic review and meta-analysis of 1366 patients. Eur. J. Cancer 2017, 78, 91–102. [Google Scholar] [CrossRef]
- Clasen, D.; Keszte, J.; Dietz, A.; Oeken, J.; Meister, E.F.; Guntinas-Lichius, O.; Pabst, F.; Büntzel, J.; Jenzewski, E.-M.; Singer, S.; et al. Quality of life during the first year after partial laryngectomy: Longitudinal study. Head Neck 2018, 40, 1185–1195. [Google Scholar] [CrossRef] [Green Version]
- Goyal, N.; Day, A.; Epstein, J.; Goodman, J.; Graboyes, E.; Jalisi, S.; Kiess, A.P.; Ku, J.A.; Miller, M.C.; Panwar, A.; et al. Head and neck cancer survivorship consensus statement from the American Head and Neck Society. Laryngoscope Investig. Otolaryngol. 2022, 7, 70–92. [Google Scholar] [CrossRef]
- Tribius, S.; Raguse, M.; Voigt, C.; Munscher, A.; Grobe, A.; Petersen, C.; Krull, A.; Bergelt, C.; Singer, S. Residual deficits in quality of life one year after intensity-modulated radiotherapy for patients with locally advanced head and neck cancer: Results of a prospective study. Strahlenther. Onkol. 2015, 191, 501–510. [Google Scholar] [CrossRef]
- Singer, S.; Danker, H.; Guntinas-Lichius, O.; Oeken, J.; Pabst, F.; Schock, J.; Vogel, H.J.; Meister, E.F.; Wulke, C.; Dietz, A. Quality of life before and after total laryngectomy: Results of a multicenter prospective cohort study. Head Neck 2014, 36, 359–368. [Google Scholar] [CrossRef]
- Nordgren, M.; Abendstein, H.; Jannert, M.; Boysen, M.; Ahlner-Elmqvist, M.; Silander, E.; Bjordal, K.; Hammerlid, E. Health-related quality of life five years after diagnosis of laryngeal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 1333–1343. [Google Scholar] [CrossRef]
- Magne, N.; Marcy, P.Y.; Chamorey, E.; Guardiola, E.; Pivot, X.; Schneider, M.; Demard, F.; Bensadoun, R.J. Concomitant twice-a-day radiotherapy and chemotherapy in unresectable head and neck cancer patients: A long-term quality of life analysis. Head Neck 2001, 23, 678–682. [Google Scholar] [CrossRef]
- Abendstein, H.; Nordgren, M.; Boysen, M.; Jannert, M.; Silander, E.; Ahlner-Elmqvist, M.; Hammerlid, E.; Bjordal, K. Quality of life and head and neck cancer: A 5 year prospective study. Laryngoscope 2005, 115, 2183–2192. [Google Scholar] [CrossRef]
- Kraaijenga, S.A.; Oskam, I.M.; van der Molen, L.; Hamming-Vrieze, O.; Hilgers, F.J.; van den Brekel, M.W. Evaluation of long term (10-years+) dysphagia and trismus in patients treated with concurrent chemo-radiotherapy for advanced head and neck cancer. Oral Oncol. 2015, 51, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Roick, J.; Danker, H.; Dietz, A.; Papsdorf, K.; Singer, S. Predictors of changes in quality of life in head and neck cancer patients: A prospective study over a 6-month period. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, K.; de Graeff, A.; Fayers, P.M.; Hammerlid, E.; van Pottelsberghe, C.; Curran, D.; Ahlner-Elmqvist, M.; Maher, E.J.; Meyza, J.W.; Bredart, A.; et al. A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. EORTC Quality of Life Group. Eur. J. Cancer 2000, 36, 1796–1807. [Google Scholar]
- Singer, S.; Hammerlid, E.; Tomaszewska, I.M.; Amdal, C.D.; Bjordal, K.; Herlofson, B.B.; Santos, M.; Silva, J.C.; Mehanna, H.; Fullerton, A.; et al. Methodological approach for determining the Minimal Important Difference and Minimal Important Change scores for the European Organisation for Research and Treatment of Cancer Head and Neck Cancer Module (EORTC QLQ-HN43) exemplified by the Swallowing scale. Qual. Life Res. 2022, 31, 841–853. [Google Scholar] [CrossRef]
- Evaluation Software Development Company. Computer-Based Health Evaluation System. Available online: https://ches.pro/ (accessed on 5 January 2023).
- Scott, S.I.; Kathrine, Ø.; Madsen, A.; Rubek, N.; Charabi, B.W.; Wessel, I.; Hadjú, S.F.; Jensen, C.V.; Stephen, S.; Patterson, J.M.; et al. Long-term quality of life & functional outcomes after treatment of oropharyngeal cancer. Cancer Med. 2021, 10, 483–495. [Google Scholar] [CrossRef]
- Nordgren, M.; Jannert, M.; Boysen, M.; Ahlner-Elmqvist, M.; Silander, E.; Bjordal, K.; Hammerlid, E. Health-related quality of life in patients with pharyngeal carcinoma: A five-year follow-up. Head Neck 2006, 28, 339–349. [Google Scholar] [CrossRef]
- Aggarwal, P.; Hutcheson, K.A.; Garden, A.S.; Mott, F.E.; Lu, C.; Goepfert, R.P.; Fuller, C.D.; Lai, S.Y.; Gunn, G.B.; Chambers, M.S.; et al. Determinants of patient-reported xerostomia among long-term oropharyngeal cancer survivors. Cancer 2021, 127, 4470–4480. [Google Scholar] [CrossRef]
- Halpern, M.T.; de Moor, J.S.; Yabroff, K.R. Impact of Pain on Employment and Financial Outcomes Among Cancer Survivors. J. Clin. Oncol. 2022, 40, 24–31. [Google Scholar] [CrossRef]
- van Leeuwen, M.; Kieffer, J.M.; Young, T.E.; Annunziata, M.A.; Arndt, V.; Arraras, J.I.; Autran, D.; Hani, H.B.; Chakrabarti, M.; Chinot, O.; et al. Phase III study of the European Organisation for Research and Treatment of Cancer Quality of Life cancer survivorship core questionnaire. J. Cancer Surviv. 2022. [Google Scholar] [CrossRef]
- Verdonck-de Leeuw, I.; Dawson, C.; Licitra, L.; Eriksen, J.G.; Hosal, S.; Singer, S.; Laverty, D.P.; Golusinski, W.; Machczynski, P.; Varges Gomes, A.; et al. European Head and Neck Society recommendations for head and neck cancer survivorship care. Oral Oncol. 2022, 133, 106047. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | % | |
|---|---|---|
| Gender | ||
| Male | 727 | 70% |
| Female | 306 | 30% |
| Age in years | ||
| <60 | 246 | 24% |
| 60–69 | 423 | 41% |
| 70–79 | 275 | 27% |
| 80+ | 89 | 9% |
| Geographic area | ||
| Northern Europe | 237 | 23% |
| Central/Western Europe | 440 | 43% |
| Southern Europe | 218 | 21% |
| Israel | 10 | 1% |
| Japan | 30 | 3% |
| Brazil | 98 | 9% |
| Tumor sub-site | ||
| Oropharynx | 366 | 35% |
| Oral cavity | 221 | 21% |
| Larynx | 188 | 18% |
| Nasopharynx | 79 | 8% |
| Salivary gland | 53 | 5% |
| Hypopharynx | 46 | 4% |
| Nasal cavity and sinuses | 34 | 3% |
| Unknown primary | 46 | 4% |
| Treatment | ||
| Surgery | 112 | 11% |
| RT | 118 | 11% |
| CRT | 302 | 29% |
| RT +/− CT and ND | 103 | 10% |
| Surgery and RT +/− CT | 397 | 38% |
| Unknown | 1 | 0% |
| UICC stage (Version 7) | ||
| I | 195 | 19% |
| II | 160 | 15% |
| III | 234 | 23% |
| IV | 416 | 40% |
| Missing/Unknown | 28 | 3% |
| Time since diagnosis (years) | ||
| 5 to 6 | 219 | 21% |
| 7 to 8 | 367 | 36% |
| 9 to 10 | 204 | 20% |
| >10 | 243 | 24% |
| Dry Mouth | Difficulty Swallowing/Eating | Hoarseness/ Difficulty Speaking | Pain in the Head and Neck | |||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Gender (reference = male) | ||||||||
| female | 1.3 | (1.0–1.8) | 1.1 | (0.9–1.5) | 1.2 | (0.8–1.8) | 0.8 | (0.5–1.2) |
| Age (reference = less than 60 years old) | ||||||||
| 60–69 years | 1.1 | (0.8–1.6) | 1.1 | (0.8–1.6) | 0.9 | (0.6–1.5) | 0.6 | (0.4–0.9) |
| 70–79 years | 1.0 | (0.7–1.5) | 1.5 | 1.0–2.3) | 1.4 | (0.8–2.3) | 0.4 | (0.2–0.6) |
| 80 years or older | 0.7 | (0.4–1.1) | 1.0 | (0.6–1.7) | 0.7 | (0.3–1.5) | 0.5 | (0.2–1.1) |
| Tumor subsite (reference = oropharynx) | ||||||||
| hypopharynx | 0.3 | (0.1–0.6) | 1.9 | (1.0–3.7) | 5.4 | (2.5–11.5) | 0.8 | (0.2–2.3) |
| larynx | 0.4 | (0.3–0.6) | 0.9 | (0.6–1.4) | 7.2 | (4.3–12.3) | 0.5 | (0.2–1.0) |
| nasal cavity and sinuses | 0.3 | (0.1–0.7) | 0.4 | (0.2–0.9) | 0.5 | (0.1–2.4) | 0.6 | (0.2–2.1) |
| nasopharynx | 0.9 | (0.5–1.5) | 0.6 | (0.3–1.0) | 0.5 | 0.2–1.9) | 2.3 | (1.0–5.1) |
| oral cavity | 0.6 | (0.4–0.9) | 0.9 | (0.6–1.4) | 1.5 | (0.8–2.7) | 1.1 | (0.6–1.9) |
| salivary gland | 0.6 | (0.3–1.1) | 0.4 | (0.2–0.9) | 0.6 | (0.2–1.9) | 1.2 | (0.6–2.7) |
| unknown primary | 1.2 | (0.6–2.4) | 1.0 | (0.5–2.0) | 0.8 | (0.2–3.8) | 0.6 | (0.2–1.8) |
| UICC stage (reference = UICC I) | ||||||||
| UICC stage II | 1.2 | (0.7–1.9) | 1.9 | (1.2–3.1) | 0.9 | (0.5–1.7) | 1.4 | (0.7–2.6) |
| UICC stage III | 0.8 | (0.5–1.3) | 1.7 | (1.0–2.7) | 1.8 | (0.9–3.4) | 1.0 | (0.5–2.0) |
| UICC stage IV | 0.9 | (0.6–1.4) | 1.9 | (1.2–3.0) | 1.0 | (0.6–1.9) | 1.2 | (0.6–2.2) |
| Treatment group (reference = surgery only) | ||||||||
| CRT | 4.7 | (2.5–9.0) | 2.1 | (1.1–3.9) | 0.3 | (0.1–0.6) | 0.2 | (0.1–0.5) |
| RT | 2.9 | (1.5–5.5) | 1.2 | (0.6–2.3) | 0.3 | (0.1–0.6) | 0.3 | (0.1–0.8) |
| RT +/− CT and ND | 2.0 | (1.0–4.0) | 1.9 | (0.9–3.8) | 0.2 | (0.1–0.6) | 1.0 | (0.4–2.4) |
| Surgery and RT +/− CT | 3.2 | (1.8–5.6) | 1.8 | (1.1–3.2) | 0.5 | (0.2–0.9) | 0.8 | (0.4–1.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, K.J.; Amdal, C.D.; Bjordal, K.; Astrup, G.L.; Herlofson, B.B.; Duprez, F.; Gama, R.R.; Jacinto, A.; Hammerlid, E.; Scricciolo, M.; et al. Serious Long-Term Effects of Head and Neck Cancer from the Survivors’ Point of View. Healthcare 2023, 11, 906. https://doi.org/10.3390/healthcare11060906
Taylor KJ, Amdal CD, Bjordal K, Astrup GL, Herlofson BB, Duprez F, Gama RR, Jacinto A, Hammerlid E, Scricciolo M, et al. Serious Long-Term Effects of Head and Neck Cancer from the Survivors’ Point of View. Healthcare. 2023; 11(6):906. https://doi.org/10.3390/healthcare11060906
Chicago/Turabian StyleTaylor, Katherine J., Cecilie D. Amdal, Kristin Bjordal, Guro L. Astrup, Bente B. Herlofson, Fréderic Duprez, Ricardo R. Gama, Alexandre Jacinto, Eva Hammerlid, Melissa Scricciolo, and et al. 2023. "Serious Long-Term Effects of Head and Neck Cancer from the Survivors’ Point of View" Healthcare 11, no. 6: 906. https://doi.org/10.3390/healthcare11060906