
The Effect of Deep and Slow Breathing on Retention and Cognitive Function in the Elderly Population

Abstract
:1. Introduction
2. Materials and Methods
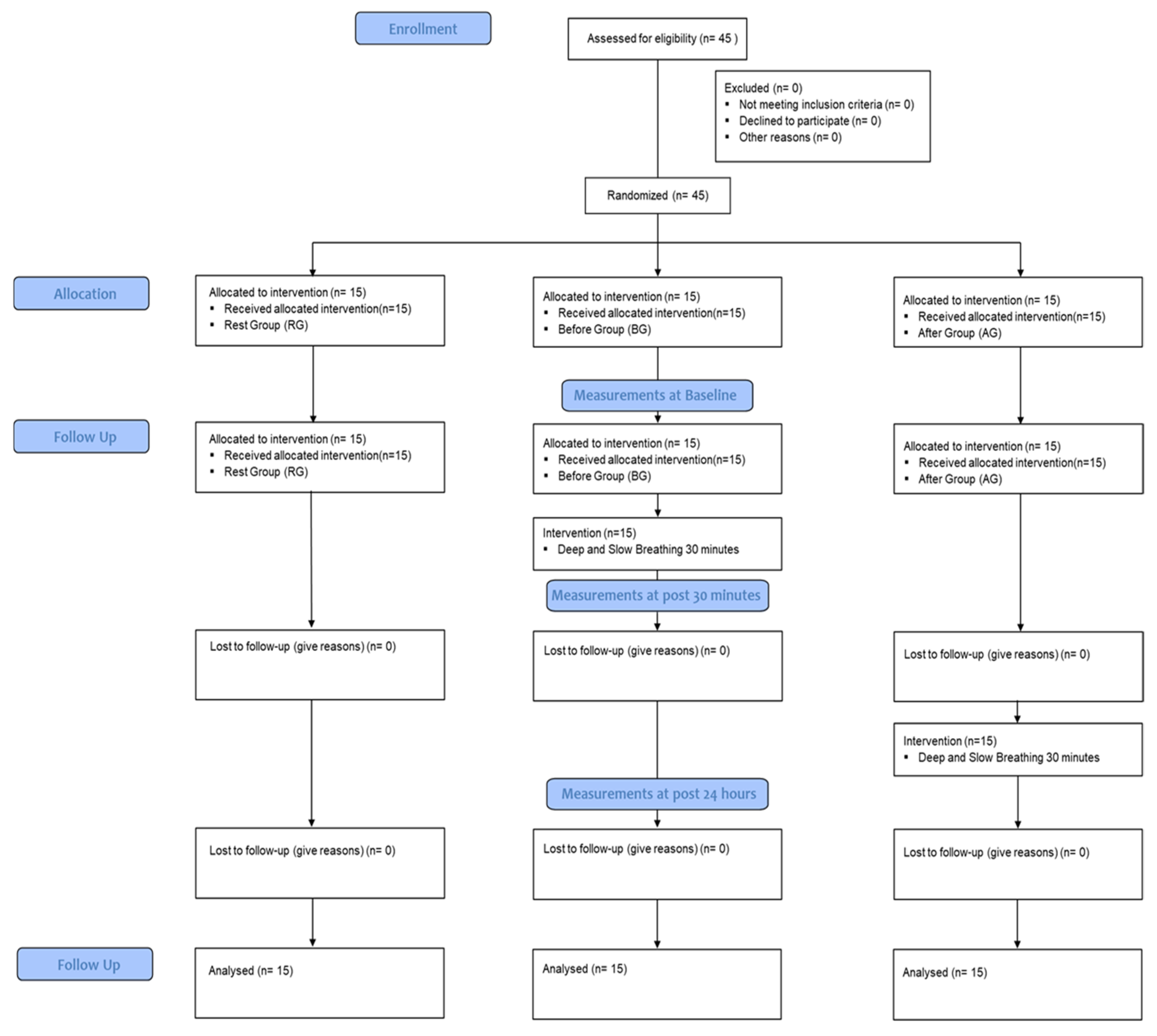
2.1. Participants
2.2. Procedures
2.2.1. Intervention with Cognitive Skill Tasks
2.2.2. Intervention with Deep and Slow Breathing
2.2.3. Measurement with New Cognitive Skills Retention
2.2.4. Measurement with Cognitive Function by Areas
N-Back Test
Go/No-Go Test
Mental Rotation Test
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Subjects
3.2. Change of New Cognitive Skills Retention
3.3. Change of Cognitive Function by Area
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McKay, L.; Evans, K.C.; Frackowiak, R.; Corfield, D. Neural correlates of voluntary breathing in humans. J. Appl. Physiol. 2003, 95, 1170–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.S.; Oh, Y.J. Health promoting lifestyle and need assessment of health promotion program for the rural elderly. J. Korean Acad. Community Health Nurs. 2004, 15, 5–17. [Google Scholar]
- Kwon, J.D. Diagnosis and Tasks of the Dementia Response System from the Perspective of Elderly Welfare Policy. J. Health Soc. Res. 2018, 38, 9–36. [Google Scholar] [CrossRef]
- Kim, E.J.; June, K.J. The Effects of Excercise Program on Cognitive Perception, Health Promotion Activity and Life Satisfaction of Elderly in Senior Citizen`s Center. J. Korean Acad. Community Health Nurs. 2000, 11, 80–89. [Google Scholar]
- Busch, V.; Magerl, W.; Kern, U.; Haas, J.; Hajak, G.; Eichhammer, P. The effect of deep and slow breathing on pain perception, autonomic activity, and mood processing—An experimental study. Pain Med. 2012, 13, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Floyer-Lea, A.; Matthews, P.M. Distinguishable brain activation networks for short- and long-term motor skill learning. J. Neurophysiol. 2005, 94, 512–518. [Google Scholar] [CrossRef]
- Yadav, G.; Mutha, P.K. Deep breathing practice facilitates retention of newly learned motor skills. Sci. Rep. 2016, 6, 37069. [Google Scholar] [CrossRef] [Green Version]
- Kiss, J.; Troncoso, E.; Djebbara, Z.; Vutskits, L.; Muller, D. The role of neural cell adhesion molecules in plasticity and repair. Brain Res. Rev. 2001, 36, 175–184. [Google Scholar] [CrossRef]
- Rothman, S.M.; Mattson, M.P. Activity-dependent, stress-responsive BDNF signaling and the quest for optimal brain health and resilience throughout the lifespan. Neuroscience. 2013, 239, 228–240. [Google Scholar] [CrossRef] [Green Version]
- Halamish, V.; Bjork, R.A. When does testing enhance retention? A distribution-based interpretation of retrieval as a memory modifier. J. Exp. Psychol. Learn. Mem. Cogn. 2011, 37, 801–812. [Google Scholar] [CrossRef] [PubMed]
- Gothe, N.; Pontifex, M.B.; Hillman, C.; McAuley, E. The acute effects of yoga on executive function. J. Phys. Act. Health 2013, 10, 488–495. [Google Scholar] [CrossRef]
- Sarang, S.P.; Telles, S. Immediate effect of two yoga-based relaxation techniques on performance in a letter-cancellation task. Percept. Mot. Ski. 2007, 105, 379–385. [Google Scholar] [CrossRef]
- Afsaneh, Z.; Alireza, Z.; Mehdi, T.; Farzad, A.; Reza, Z.M.; Mehdi, M.; Mojtaba, K.S. Assessment of Selective Attention with CSCWT (Computerized Stroop Color-Word Test) among Children and Adults. 2012; Online Submission. Available online: https://eric.ed.gov/?id=ED530676 (accessed on 17 January 2012)Online Submission.
- Barr, M.S.; Radhu, N.; Guglietti, C.L.; Zomorrodi, R.; Rajji, T.K.; Ritvo, P.; Daskalakis, Z.J. Age-related differences in working memory evoked gamma oscillations. Brain Res. 2014, 1576, 43–51. [Google Scholar] [CrossRef]
- Votruba-Drzal, E.; Coley, R.L.; Koury, A.S.; Miller, P. Center-based child care and cognitive skills development: Importance of timing and household resources. J. Educ. Psychol. 2013, 105, 821–838. [Google Scholar] [CrossRef]
- Mun, H.-J.; Ha, D.H. Componential analysis for sex differences in the performance of mental rotation task. Korean Educ. Psychol. Res. 2010, 24, 957–975. [Google Scholar]
- Piepmeier, A.T.; Etnier, J.L. Brain-derived neurotrophic factor (BDNF) as a potential mechanism of the effects of acute exercise on cognitive performance. J. Sport Health Sci. 2015, 4, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Skriver, K.; Roig, M.; Lundbye-Jensen, J.; Pingel, J.; Helge, J.W.; Kiens, B.; Nielsen, J.B. Acute exercise improves motor memory: Exploring potential biomarkers. Neurobiol. Learn. Mem. 2014, 116, 46–58. [Google Scholar] [CrossRef]
- Fumoto, M.; Sato-Suzuki, I.; Seki, Y.; Mohri, Y.; Arita, H. Appearance of high-frequency alpha band with disappearance of low-frequency alpha band in EEG is produced during voluntary abdominal breathing in an eyes-closed condition. Neurosci. Res. 2004, 50, 307–317. [Google Scholar] [CrossRef]
- Shimizu, T.; Komori, T.; Kugio, Y.; Fujimaki, Y.; Oyanagi, K.; Hayashi, H. Electrophysiological assessment of corticorespiratory pathway function in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2010, 11, 57–62. [Google Scholar] [CrossRef]
- Yu, X.; Fumoto, M.; Nakatani, Y.; Sekiyama, T.; Kikuchi, H.; Seki, Y.; Sato-Suzuki, I.; Arita, H. Activation of the anterior prefrontal cortex and serotonergic system is associated with improvements in mood and EEG changes induced by Zen meditation practice in novices. Int. J. Psychophysiol. 2011, 80, 103–111. [Google Scholar] [CrossRef]
- Park, Y.J.; Park, Y.B. Clinical utility of paced breathing as a concentration meditation practice. Complement. Ther. Med. 2012, 20, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Critchley, H.D.; Nicotra, A.; Chiesa, P.A.; Nagai, Y.; Gray, M.A.; Minati, L.; Bernardi, L. Slow breathing and hypoxic challenge: Cardiorespiratory consequences and their central neural substrates. PLoS ONE 2015, 10, e0127082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perciavalle, V.; Blandini, M.; Fecarotta, P.; Buscemi, A.; Di Corrado, D.; Bertolo, L.; Fichera, F.; Coco, M. The role of deep breathing on stress. Neurol. Sci. 2017, 38, 451–458. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | CG (n1 = 15) | BG (n2 = 15) | AG (n3 = 15) |
|---|---|---|---|
| Gender (male/female) | 7/8 | 9/6 | 8/7 |
| Age (years) | 71.10 ± 4.87 1 | 69.70 ± 5.10 | 71.30 ± 6.37 |
| Height (cm) | 168.54 ± 9.87 | 167.33 ± 6.75 | 168.93 ± 8.67 |
| Weight (kg) | 63.65 ± 9.65 | 67.39 ± 8.71 | 65.45 ± 7.65 |
| BMI | 22.55 ± 2.65 | 24.16 ± 2.49 | 23.19 ± 2.81 |
| MMES-K (score) | 25.43 ± 6.40 | 26.01 ± 5.01 | 25.09 ± 5.65 |
| Retention | TL | STT | LTT | Post hoc | F | ||
|---|---|---|---|---|---|---|---|
| Correct (%) | |||||||
| CG | 50 ± 12.69 1 | 59 ± 14.30 | 58.75 ± 19.27 | Time | 67.60 * | ||
| BG | 45 ± 4.71 | 81.5 ± 9.52 | 86.25 ± 7.29 | TL < STT, LTT | |||
| Time *Group | 14.53 * | ||||||
| AG | 51 ± 26.85 | 59 ± 20.11 | 89 ± 11.01 | TL, STT < LTT | |||
| Reaction Time (ms) | |||||||
| CG | 1052.13 ± 157.32 | 1160.95 ± 170.53 | 1186.16 ± 152.58 | TL < STT, LTT | Time | 48.44 * | |
| BG | 1088.16 ± 88.52 | 894.47 ± 84.89 | 916.49 ± 91.24 | STT, LTT < TL | |||
| Time *Group | 87.16 * | ||||||
| AG | 1093.84 ± 154.59 | 1094.22 ± 151.16 | 803.45 ± 157.58 | LTT < TL, STT | |||
| N-Back | TL | STT | LTT | Post hoc | F | ||
|---|---|---|---|---|---|---|---|
| Correct (%) | |||||||
| CG | 59.14 ± 17.97 1 | 40.27 ± 10.05 | 48.39 ± 14.31 | Time | 80.00 * | ||
| BG | 54.07 ± 24.99 | 70.78 ± 13.61 | 48.32 ± 13.87 | TL < STT, LTT | |||
| Time *Group | 34.70 * | ||||||
| AG | 60.73 ± 18.89 | 72.16 ± 12.79 | 82.37 ± 12.03 | TL, STT < LTT | |||
| Reaction Time (ms) | |||||||
| CG | 790.31 ± 88.83 | 1005.78 ± 116.46 | 1101.01 ± 121.39 | TL < STT, LTT | Time | 116.05 * | |
| BG | 784.19 ± 89.54 | 689.25 ± 65.32 | 1070.65 ± 75.69 | STT, LTT < TL | |||
| Time *Group | 83.41 * | ||||||
| AG | 815.47 ± 87.28 | 682.24 ± 69.35 | 634.57 ± 52.30 | LTT < TL, STT | |||
| Go/No-Go | TL | STT | LTT | Post hoc | F | ||
|---|---|---|---|---|---|---|---|
| Correct (%) | |||||||
| CG | 59.14 ± 17.97 1 | 40.27 ± 10.05 | 48.39 ± 14.31 | Time | 47.07 * | ||
| BG | 54.07 ± 24.99 | 70.78 ± 13.61 | 48.32 ± 13.87 | TL < STT, LTT | |||
| Time *Group | 34.27 * | ||||||
| AG | 60.73 ± 18.89 | 72.16 ± 12.79 | 82.37 ± 12.03 | TL, STT < LTT | |||
| Reaction Time (ms) | |||||||
| CG | 564.84 ± 120.56 | 774.93 ± 68.13 | 987.18 ± 138.84 | TL < STT, LTT | Time | 90.49 * | |
| BG | 563.61 ± 122.20 | 567.30 ± 43.32 | 1003.64 ± 137.37 | STT, LTT < TL | |||
| Time *Group | 62.13 * | ||||||
| AG | 557.01 ± 144.88 | 570.87 ± 51.00 | 534.26 ± 53.00 | LTT < TL, STT | |||
| Mental Rotation | TL | STT | LTT | Post hoc | F | ||
|---|---|---|---|---|---|---|---|
| Correct (%) | |||||||
| CG | 59.14 ± 17.97 1 | 40.27 ± 10.05 | 48.39 ± 14.31 | Time | 96.87 * | ||
| BG | 54.07 ± 24.99 | 70.78 ± 13.61 | 48.32 ± 13.87 | TL < STT, LTT | |||
| Time *Group | 70.75 * | ||||||
| AG | 60.73 ± 18.89 | 72.16 ± 12.79 | 82.37 ± 12.03 | TL, STT < LTT | |||
| Reaction Time (ms) | |||||||
| CG | 1298.84 ± 58.23 | 1409.59 ± 110.83 | 1455.36 ± 134.75 | TL < STT, LTT | Time | 76.59 * | |
| BG | 1329.98 ± 85.21 | 1151.42 ± 62.59 | 1463.40 ± 132.51 | STT, LTT < TL | |||
| Time *Group | 63.12 * | ||||||
| AG | 1306.20 ± 69.06 | 1175.39 ± 79.84 | 964.01 ± 48.00 | LTT < TL, STT | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-H.; Park, D.-S.; Song, C.-H. The Effect of Deep and Slow Breathing on Retention and Cognitive Function in the Elderly Population. Healthcare 2023, 11, 896. https://doi.org/10.3390/healthcare11060896
Lee S-H, Park D-S, Song C-H. The Effect of Deep and Slow Breathing on Retention and Cognitive Function in the Elderly Population. Healthcare. 2023; 11(6):896. https://doi.org/10.3390/healthcare11060896
Chicago/Turabian StyleLee, Su-Ha, Dae-Sung Park, and Chang-Ho Song. 2023. "The Effect of Deep and Slow Breathing on Retention and Cognitive Function in the Elderly Population" Healthcare 11, no. 6: 896. https://doi.org/10.3390/healthcare11060896