

The Reliability and Validity of Dental Indifference Scale among Romanian Young Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. The Psychometric Properties of the Dental Indifference Scale
3. Materials and Methods
3.1. The Translation and the Adaptation of the Scale
3.2. Ethical Consideration
3.3. Study Design and Participants
3.4. Measures
- oral hygiene behavior (the daily frequency of tooth brushing with two choices: 1—two or more times a day; or 2—once a day or more rarely);
- eating behavior (the frequency of daily snacks: 1—one-two snacks between meals; or 2—three or more snacks);
- attendance (1—between six months and a year; or 2—more than a year);
- flossing (1—once a day; or 2—less than once a day);
- self-assessment of oral health (1—better than the average; 2—average, 3—worse than average).
3.5. The Socio-Demographic Data Collected
3.6. The Statistical Analysis of the Data
4. Results
4.1. Socio-Demographic Characteristics
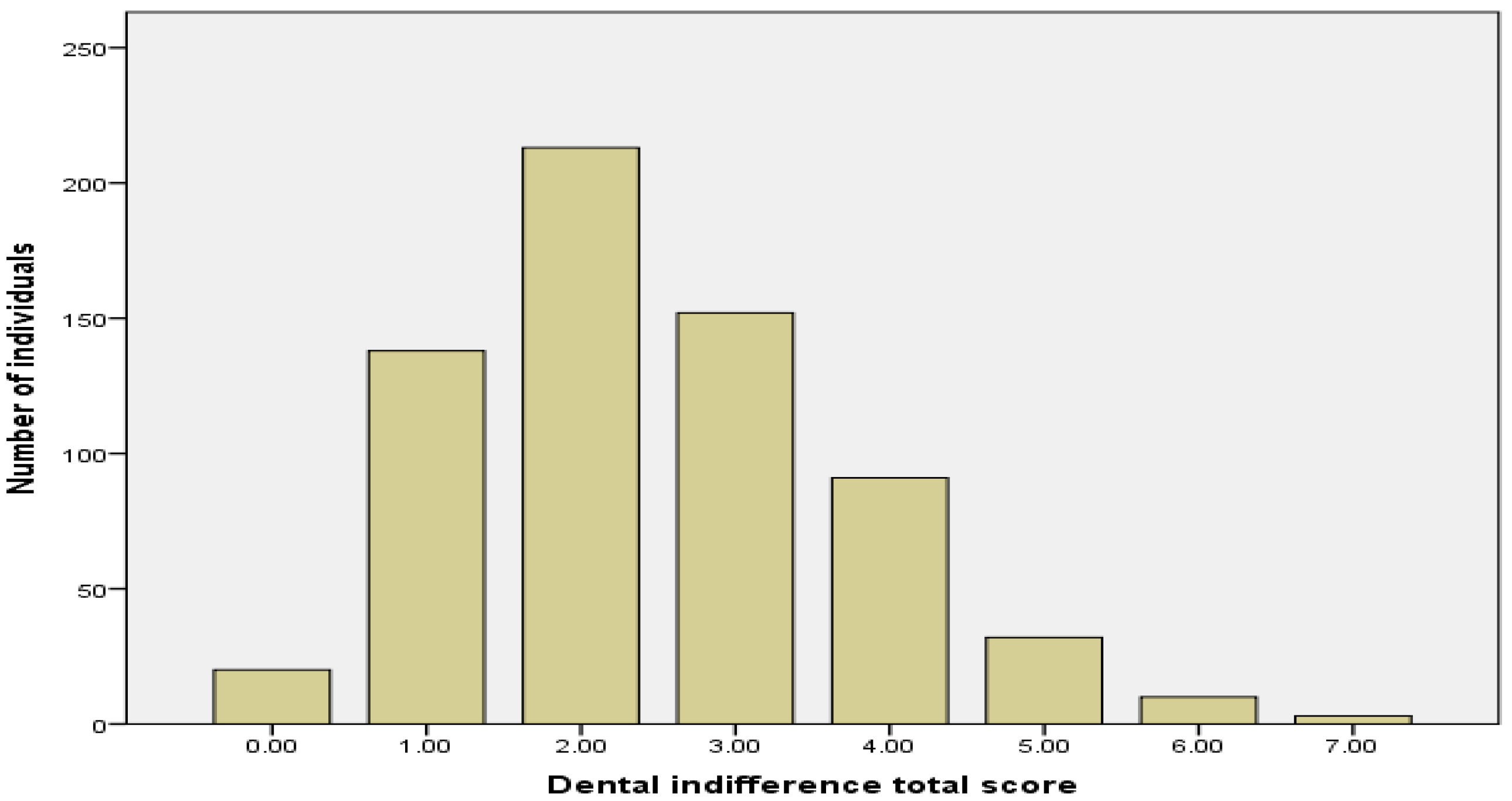
4.2. Descriptive Analysis
4.3. Reliability
4.4. Dental Indifference and Oral Health Behavior
5. Discussion
Limits of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Items from the Original English Version | Items from the Final Romanian Version |
|---|---|
1. I usually use:
| 1. Folosesc de obicei:
|
2. At present:
| 2. În momentul de față:
|
3. If I lost a filling in a back tooth and it did not hurt:
| 3. Dacă aș pierde o plombă de pe dintele din spate și nu mă doare:
|
4. I usually make an appointment to visit a dentist:
| 4. Îmi fac programare pentru a merge la medicul stomatolog:
|
5. If my gums bled, but they didn’t hurt:
| 5. Dacă gingiile mi-ar sângera, dar nu m-ar durea:
|
6. About all your dental appointments during the last 5 years:
| 6. Referitor la programările dvs. la cabinetul dentar din ultimii 5 ani, puteți spune că:
|
7. If I had a very painful back tooth:
| 7. Dacă aș avea un dinte din spate foarte dureros:
|
8. I would say that my main reason for not going to a dentist for a check-up would be:
| 8. Aș spune că principalul motiv pentru care nu merg la medicul stomatolog pentru control ar fi:
|
References
- Nuttall, N.M. Initial development of a scale to measure dental indifference. Community Dent. Oral Epidemiol. 1996, 24, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Pandey, V.; Chandra, S.; Dilip Kumar, H.P.; Gupta, A.; Bhandari, P.P.; Rathod, P. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment: A cross-sectional study. J. Int. Soc. Prev. Community Dent. 2016, 6, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enríquez-Campoverde, P. Indiferencia Al Tratamiento Odontológico en Adultos Jóvenes de 18 a 44 años Parroquia El Batán, Cuenca 2017. Bachelor’s Thesis, Universidad Catolica de Cuenca, Cuenca, Ecuador, 2017. [Google Scholar]
- Khajuria, A.K.; Singh, P.; Agarwal, G. Impact of dental neglect score on oral health among patients receiving fixed orthodontic treatment. Eur. J. Mol. Clin. Med. 2022, 9, 2080–2084. [Google Scholar]
- Hiraoka, T.; Chujo, T.; Tsuge, M.; Kondo, Y. Paediatric case of group A streptococcal pharyngitis, arthritis and osteomyelitis associated with dental neglect. BMJ Case Rep. 2021, 14, e239196. [Google Scholar] [CrossRef] [PubMed]
- Heredia, D.; Villavicencio, E.; Jaramillo, J. Indiferencia al tratamiento dental. Odontol. Act. Rev. Científica 2018, 3, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Pacheco Pacheco, J.S. Relación Entre la Indiferencia Dental Y la Adherencia Terapéutica en Pacientes de la Clínica Odontológica Especializada Pnp Angamos. Bachelor’s Thesis, Universidad Alas Peruanas, Lima, Peru, 2020. [Google Scholar]
- Jamieson, L.M.; Thomson, W.M. The Dental Neglect and Dental Indifference scales compared. Community Dent. Oral Epidemiol. 2002, 30, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Ayabaca Morocho, M.V. Relación Entre El Nivel de Instrucción Y la Indiferencia Dental en Personas de 45 a 65 años, de la Parroquia Huayna Cápac en la Ciudad de Cuenca, 2017. Bachelor’s Thesis, Universidad Católica de Cuenca, Cuenca, Ecuador, 2018. [Google Scholar]
- Skaret, E.; Raadal, M.; Kvale, G.; Berg, E. Reliability and validity of the Dental Indifference Scale in a population of 18-year-olds in Norway. Community Dent. Oral Epidemiol. 2000, 28, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Callalli, L.; Navarro, D.; Leon, X. Association between the level of indifference to dental treatment and habits of oral hygiene in adults. J. Oral Res. 2022, 11, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. 2020. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 20 January 2022).
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.A.; Barrett, K.C.; Leech, N.L.; Gloeckner, G.W. IBM SPSS for Introductory Statistics: Use and Interpretation, 6th ed.; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Peterson, R.A.; Kim, Y. On the relationship between coefficient alpha and composite reliability. J. Appl. Psychol. 2013, 98, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, W.M.; Spencer, A.J.; Gaughwin, A. Testing a child dental neglect scale in South Australia. Community Dent. Oral Epidemiol. 1996, 24, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Thomson, W.M.; Locker, D. Dental neglect and dental health among 26-year-olds in the Dunedin Multidisciplinary Health and Development Study. Community Dent. Oral Epidemiol. 2000, 28, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C.B.; Randall, C.L.; McNeil, D.W. Development and Validation of the Oral Health Values Scale. Community Dent. Oral Epidemiol. 2021, 49, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Etikan, I.; Alkassim, R.; Abubakar, S. Comparision of snowball sampling and sequential sampling technique. Biom. Biostat. Int. J. 2016, 3, 00055. [Google Scholar] [CrossRef] [Green Version]

| Items | M | Std.Dev | Min.–Max. | Skewness | Kurtosis |
|---|---|---|---|---|---|
| 1 | 0.87 | 0.32 | 0–1 | −2.32 | 3.43 |
| 2 | 0.51 | 0.50 | 0–2 | −0.03 | −1.91 |
| 3 | 0.16 | 0.37 | 0–2 | 2.00 | 2.56 |
| 4 | 0.30 | 0.45 | 0–1 | 0.87 | −1.24 |
| 5 | 0.36 | 0.48 | 0–1 | 0.56 | −1.68 |
| 6 | 0.06 | 0.24 | 0–1 | 3.56 | 10.74 |
| 7 | 0.10 | 0.30 | 0–1 | 2.63 | 4.95 |
| 8 | 0.06 | 0.24 | 0–1 | 3.61 | 11.11 |
| DIS total score | 2.45 | 1.32 | 0–7 | 0.56 | 0.22 |
| Mean Rank | Gender | Education | ||
|---|---|---|---|---|
| Males | Females | Secondary Level | University Level | |
| DIS total score | 345.72 | 324.62 | 280.64 | 247.73 |
| Mann-Whitney U | 43,157.00 | 26,259.00 | ||
| Test-Retest | N | Kappa Values | % Agreement | |
|---|---|---|---|---|
| 0 | 1 | |||
| DIS1 | 35 | 0.68 | 34 | 62 |
| DIS2 | 35 | 0.47 | 62 | 25 |
| DIS3 | 35 | 0.37 | 82 | 8 |
| DIS4 | 35 | 0.60 | 42 | 48 |
| DIS5 | 35 | 0.44 | 65 | 22 |
| DIS6 | 35 | −0.06 | 94 | 5 |
| DIS7 | 35 | 0.34 | 80 | 17 |
| DIS8 | 35 | 0.79 | 82 | 17 |
| DIS total score: α = 0.37 ω = 0.39 | ||||
| Oral Health Behavior | Mean DIS (Std.Dev.) | p< |
|---|---|---|
| Daily frequency of tooth brushing | ||
| Two or more times a day | 2.71 (1.30) | 0.001 |
| Once a day or more rarely | 3.43 (1.46) | |
| Eating behavior | ||
| Large number of snacks between meals | 2.71 (1.30) | 0.001 |
| Small number of snacks between meals | 2.10 (1.22) | |
| Dental attendance | ||
| 6 months–1 year | 2.22 (1.18) | 0.001 |
| More than a year | 3.37 (1.18) | |
| Flossing | ||
| Once a day | 1.92 (1.10) | 0.001 |
| Less than once a day | 2.71 (1.31) | |
| Self-assessment of oral health | ||
| Better than the average | 2.27 (1.22) * | 0.001 |
| Average | 3.31 (1.33) | |
| Worse than the average | 4.00 (0.80) ** | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sfeatcu, R.; Balgiu, B.A.; Băluță, A.; Gălbinașu, B.M.; Georgescu, C.E.; Ilici, R.R. The Reliability and Validity of Dental Indifference Scale among Romanian Young Adults. Healthcare 2023, 11, 876. https://doi.org/10.3390/healthcare11060876
Sfeatcu R, Balgiu BA, Băluță A, Gălbinașu BM, Georgescu CE, Ilici RR. The Reliability and Validity of Dental Indifference Scale among Romanian Young Adults. Healthcare. 2023; 11(6):876. https://doi.org/10.3390/healthcare11060876
Chicago/Turabian StyleSfeatcu, Ruxandra, Beatrice Adriana Balgiu, Andreea Băluță, Bogdan Mihai Gălbinașu, Carmen Elena Georgescu, and Roxana Romanița Ilici. 2023. "The Reliability and Validity of Dental Indifference Scale among Romanian Young Adults" Healthcare 11, no. 6: 876. https://doi.org/10.3390/healthcare11060876