
Bright Morning Lighting Enhancing Parasympathetic Activity at Night: A Pilot Study on Elderly Female Patients with Dementia without a Pacemaker
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
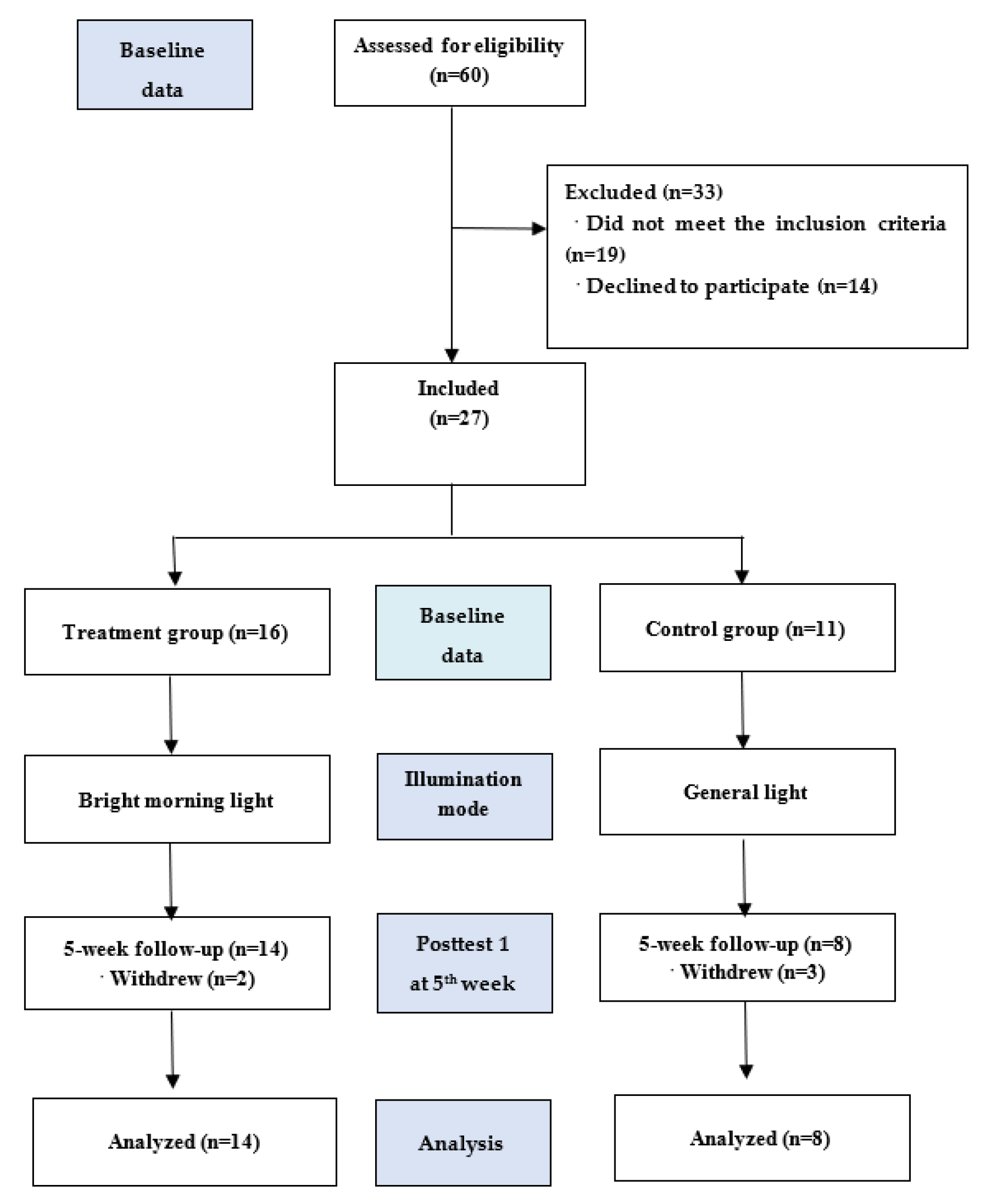
2.1. Study Design
2.2. Participants
2.3. Intervention Group
2.4. Instruments and Outcome Measures
Validity and Reliability of HRV Data
2.5. Statistical Analyses
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Primary Outcomes
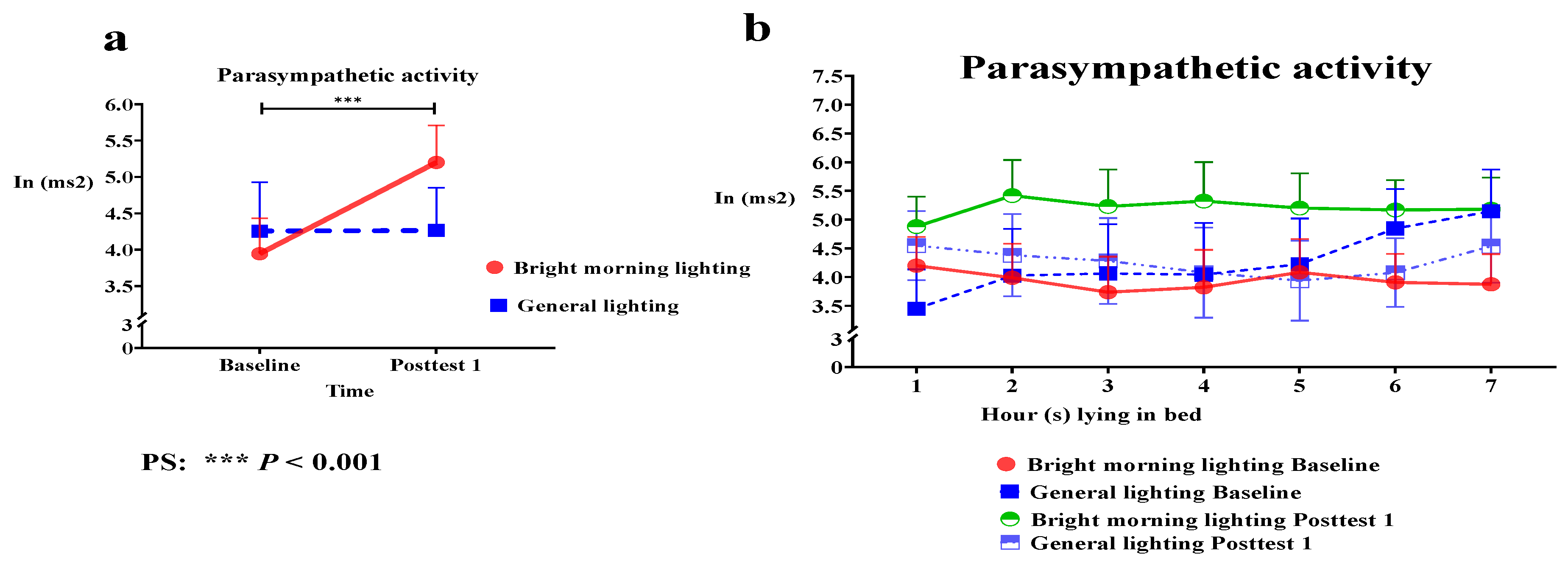
3.2.1. Effects of BML on PSNS Activity
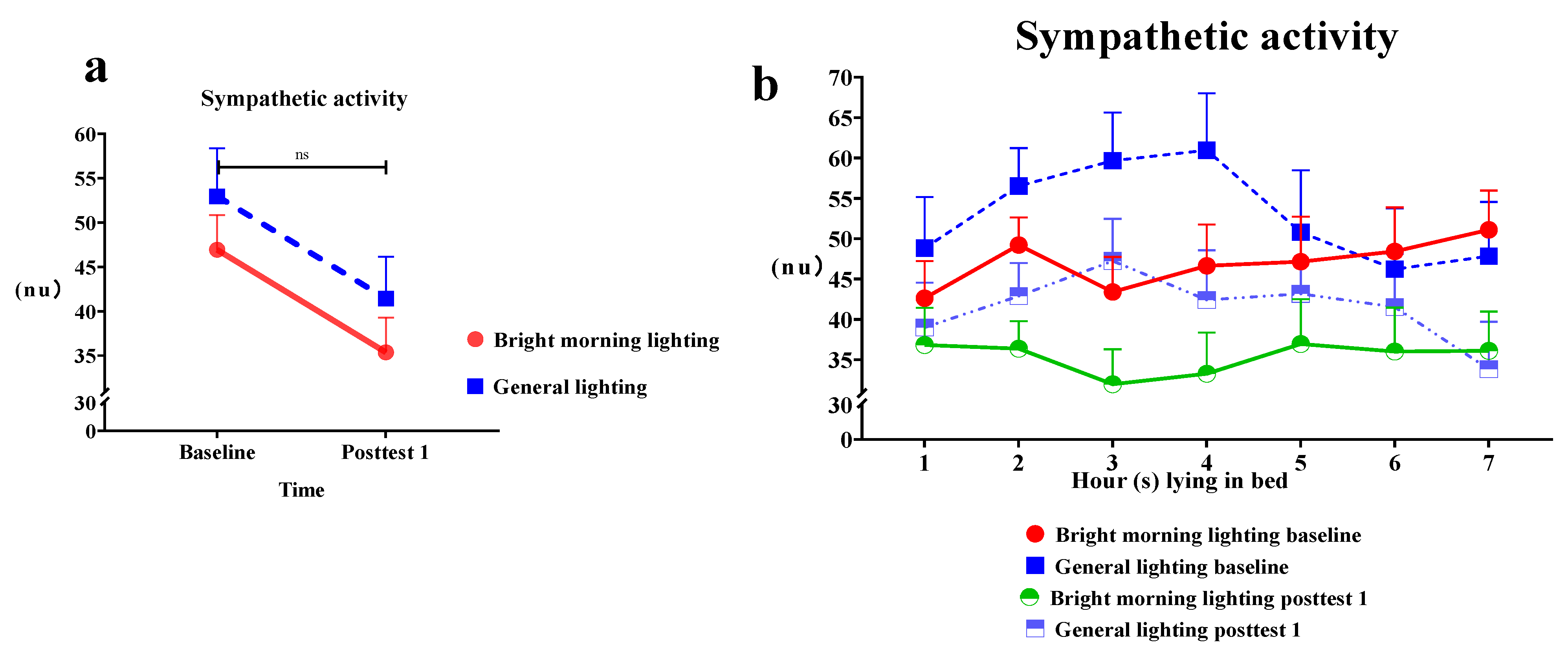
3.2.2. Effects of BML on SNS Activity
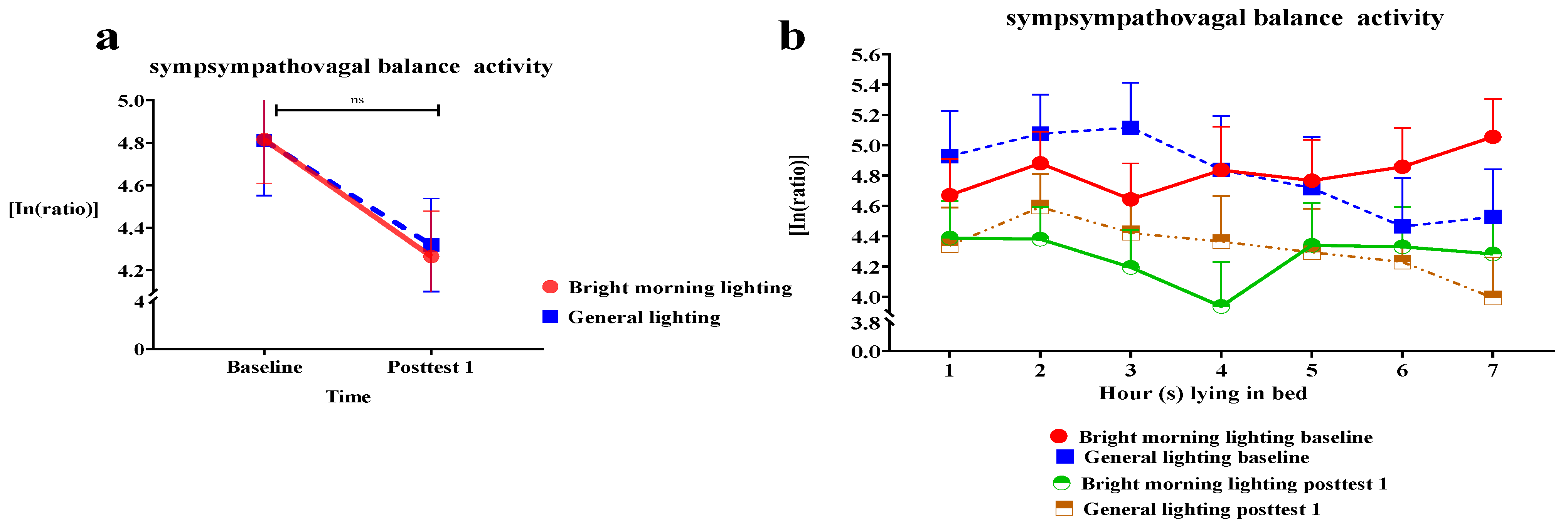
3.2.3. Effects of BML on Sympathovagal Balance
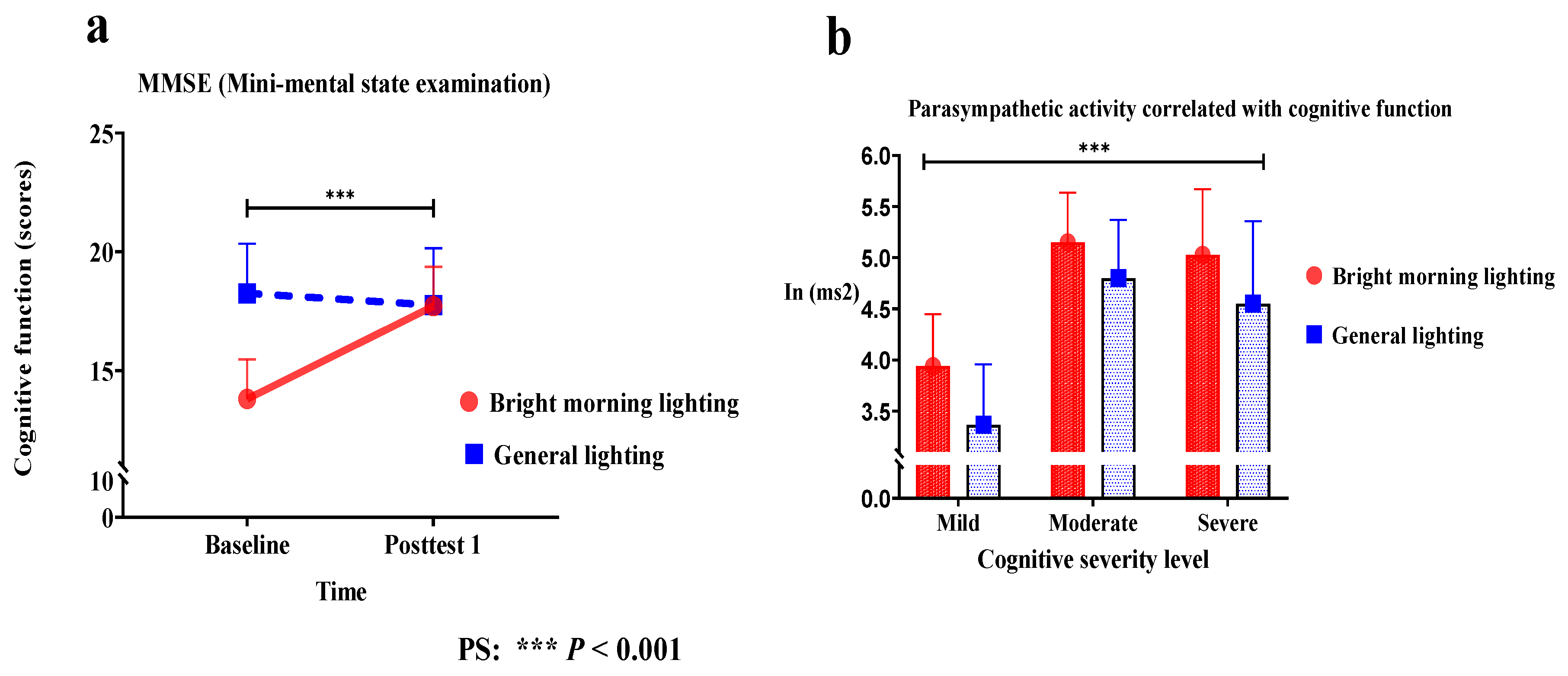
3.3. Secondary Outcomes
Effect of HF, LF%, and LF/HF on Cognitive Function
4. Discussion
4.1. BML Exposure Enabled Stable Circadian Rhythm and the Postponement of Dementia Disease Progression
4.2. BML Exposure Enhanced PSNS Activity to a Maximum at Night
4.3. BML Therapy Is More Effective for Severe Dementia-Enhanced PSNS Activity
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 2 September 2021).
- Coker-Ayo, O.O.; Nathaniel, S.I.; Poupore, N.; Bailey-Taylor, M.J.; Roley, L.T.; Goodwin, R.L.; McPhail, B.; Russ-Sellers, R.; Nathaniel, T.I. Sex Differences in Demographic and Pharmacological Factors in Alzheimer Patients with Dementia and Cognitive Impairments. Front. Behav. Neurosci. 2022, 16, 828782. [Google Scholar] [CrossRef]
- Rossi, A.; Mikail, N.; Bengs, S.; Haider, A.; Treyer, V.; Buechel, R.R.; Wegener, S.; Rauen, K.; Tawakol, A.; Bairey Merz, C.N.; et al. Heart-Brain Interactions in Cardiac and Brain Diseases: Why Sex Matters. Eur. Heart J. 2022, 43, 3971–3980. [Google Scholar] [CrossRef]
- Kong, S.D.X.; Hoyos, C.M.; Phillips, C.L.; McKinnon, A.C.; Lin, P.; Duffy, S.L.; Mowszowski, L.; LaMonica, H.M.; Grunstein, R.R.; Naismith, S.L.; et al. Altered Heart Rate Variability during Sleep in Mild Cognitive Impairment. Sleep. 2021, 44, zsaa232. [Google Scholar] [CrossRef]
- Abulafia, C.; Duarte-Abritta, B.; Villarreal, M.F.; Ladrón-de-Guevara, M.S.; García, C.; Sequeyra, G.; Sevlever, G.; Fiorentini, L.; Bär, K.J.; Gustafson, D.R.; et al. Relationship between Cognitive and Sleep-Wake Variables in Asymptomatic Offspring of Patients with Late-Onset Alzheimer’s Disease. Front. Aging Neurosci. 2017, 9, 93. [Google Scholar] [CrossRef] [Green Version]
- da Silva, V.P.; Ramalho Oliveira, B.R.; Tavares Mello, R.G.; Moraes, H.; Deslandes, A.C.; Laks, J. Heart Rate Variability Indexes in Dementia: A Systematic Review with a Quantitative Analysis. Curr. Alzheimer Res. 2018, 15, 80–88. [Google Scholar] [CrossRef]
- Forte, G.; Morelli, M.; Grässler, B.; Casagrande, M. Decision Making and Heart Rate Variability: A Systematic Review. Appl. Cogn. Psychol. 2022, 36, 100–110. [Google Scholar] [CrossRef]
- Ahmed, R.M.; Ke, Y.D.; Vucic, S.; Ittner, L.M.; Seeley, W.; Hodges, J.R.; Piguet, O.; Halliday, G.; Kiernan, M.C. Physiological Changes in Neurodegeneration—Mechanistic Insights and Clinical Utility. Nat. Rev. Neurol. 2018, 14, 259–271. [Google Scholar] [CrossRef]
- Zoccoli, G.; Amici, R. Sleep and Autonomic Nervous System. Curr. Opin. Physiol. 2020, 15, 128–133. [Google Scholar] [CrossRef]
- Sforza, E.; Pichot, V.; Cervena, K.; Barthélémy, J.C.; Roche, F. Cardiac Variability and Heart-Rate Increment as a Marker of Sleep Fragmentation in Patients with a Sleep Disorder: A Preliminary Study. Sleep 2007, 30, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Stein, P.K.; Pu, Y. Heart Rate Variability, Sleep and Sleep Disorders. Sleep Med. Rev. 2012, 16, 47–66. [Google Scholar] [CrossRef]
- Rubiño, J.A.; Gamundí, A.; Akaarir, M.; Canellas, F.; Rial, R.; Nicolau, M.C. Bright Light Therapy and Circadian Cycles in Institutionalized Elders. Front. Neurosci. 2020, 14, 359. [Google Scholar] [CrossRef]
- Liu, Y.L.; Gong, S.Y.; Xia, S.T.; Wang, Y.L.; Peng, H.; Shen, Y.; Liu, C.F. Light Therapy: A New Option for Neurodegenerative Diseases. Chin. Med. J. 2020, 134, 634–645. [Google Scholar] [CrossRef]
- Logan, R.W.; McClung, C.A. Rhythms of Life: Circadian Disruption and Brain Disorders across the Lifespan. Nat. Rev. Neurosci. 2019, 20, 49–65. [Google Scholar] [CrossRef]
- Tan, J.S.I.; Cheng, L.J.; Chan, E.Y.; Lau, Y.; Lau, S.T. Light Therapy for Sleep Disturbances in Older Adults with Dementia: A Systematic Review, Meta-analysis and Meta-regression. Sleep Med. 2022, 90, 153–166. [Google Scholar] [CrossRef]
- Missotten, P.; Farag, L.; Delye, S.; Muller, A.; Grotz, C.; Adam, S. Role of “Light Therapy” among Older Adults with Dementia: An Overview and Future Perspectives. Geriatr. Psychol. Neuropsychiatr. Vieil. 2019, 17, 83–91. [Google Scholar] [CrossRef]
- Liu, C.R.; Liou, Y.M.; Jou, J.H. Ambient Bright Lighting in the Morning Improves Sleep Disturbances of Older Adults with Dementia. Sleep Med. 2022, 89, 1–9. [Google Scholar] [CrossRef]
- Liu, C.R.; Liou, Y.M.; Jou, J.H. Pilot Study of the Effects of Bright Ambient Therapy on Dementia Symptoms and Cognitive Function. Front. Psychol. 2021, 12, 782160. [Google Scholar] [CrossRef]
- Yang, H.; Goldstein, M.R.; Vazquez, M.; Williams, J.P.; Mullington, J.M. Effects of Sleep and Sleep Deficiency on Autonomic Function in Humans. Curr. Opin. Endocr. Metab. Res. 2021, 18, 268–274. [Google Scholar] [CrossRef]
- Thome, J.; Densmore, M.; Terpou, B.A.; Théberge, J.; McKinnon, M.C.; Lanius, R.A. Contrasting Associations between Heart Rate Variability and Brainstem-Limbic Connectivity in Posttraumatic Stress Disorder and Its Dissociative Subtype: A Pilot Study. Front. Behav. Neurosci. 2022, 16, 862192. [Google Scholar] [CrossRef]
- Yeh, T.C.; Kao, L.C.; Tzeng, N.S.; Kuo, T.B.; Huang, S.Y.; Chang, C.C.; Chang, H.A. Heart Rate Variability in Major Depressive Disorder and after Antidepressant Treatment with Agomelatine and Paroxetine: Findings from the Taiwan Study of Depression and Anxiety (TAISDA). Prog. Neuropsychopharmacol. Biol. Psychiatry 2016, 64, 60–67. [Google Scholar] [CrossRef]
- Ferrer, I. Defining Alzheimer as a Common Age-Related Neurodegenerative Process Not Inevitably Leading to Dementia. Prog. Neurobiol. 2012, 97, 38–51. [Google Scholar] [CrossRef]
- Kalogeraki, L.; Michopoulos, I. [Hoarding Disorder in DSM-5: Clinical Description and Cognitive Approach]. Psychiatriki 2017, 28, 131–141. [Google Scholar] [CrossRef]
- Lin, F.V.; Heffner, K.; Gevirtz, R.; Zhang, Z.; Tadin, D.; Porsteinsson, A. Targeting Autonomic Flexibility to Enhance Cognitive Training Outcomes in Older Adults with Mild Cognitive Impairment: Study Protocol for a Randomized Controlled Trial. Trials 2021, 22, 560. [Google Scholar] [CrossRef]
- Kuo, T.B.; Yang, C.C. Scatterplot Analysis of EEG Slow-Wave Magnitude and Heart Rate Variability: An Integrative Exploration of Cerebral Cortical and Autonomic Functions. Sleep 2004, 27, 648–656. [Google Scholar] [CrossRef]
- Kuo, T.B.; Lin, T.; Yang, C.C.; Li, C.L.; Chen, C.F.; Chou, P. Effect of Aging on Gender Differences in Neural Control of Heart Rate. Am. J. Physiol. 1999, 277, H2233–H2239. [Google Scholar] [CrossRef]
- Silva, L.E.V.; Moreira, H.T.; de Oliveira, M.M.; Cintra, L.S.S.; Salgado, H.C.; Fazan, R., Jr.; Tinós, R.; Rassi, A.; Schmidt, A.; Marin-Neto, J.A. Heart Rate Variability as a Biomarker in Patients with Chronic Chagas Cardiomyopathy with or without Concomitant Digestive Involvement and Its Relationship with the Rassi Score. Biomed. Eng. OnLine 2022, 21, 44. [Google Scholar] [CrossRef]
- Chouchou, F.; Desseilles, M. Heart Rate Variability: A Tool to Explore the Sleeping Brain? Front. Neurosci. 2014, 8, 402. [Google Scholar] [CrossRef] [Green Version]
- Wahlstrom, J.; Skog, I.; Handel, P.; Khosrow-Khavar, F.; Tavakolian, K.; Stein, P.K.; Nehorai, A. A Hidden Markov Model for Seismocardiography. IEEE Trans. Biomed. Eng. 2017, 64, 2361–2372. [Google Scholar] [CrossRef]
- Cibeira, N.; Maseda, A.; Lorenzo-López, L.; González-Abraldes, I.; López-López, R.; Rodríguez-Villamil, J.L.; Millán-Calenti, J.C. Bright Light Therapy in Older Adults with Moderate to Very Severe Dementia: Immediate Effects on Behavior, Mood, and Physiological Parameters. Healthcare 2021, 9, 1065. [Google Scholar] [CrossRef]
- Yuksel, D.; Baker, F.C.; Goldstone, A.; Claudatos, S.A.; Forouzanfar, M.; Prouty, D.E.; Colrain, I.M.; de Zambotti, M. Stress, Sleep, and Autonomic Function in Healthy Adolescent Girls and Boys: Findings from the NCANDA Study. Sleep Health 2021, 7, 72–78. [Google Scholar] [CrossRef]
- Perneczky, R.; Wagenpfeil, S.; Komossa, K.; Grimmer, T.; Diehl, J.; Kurz, A. Mapping Scores onto Stages: Mini-Mental State Examination and Clinical Dementia Rating. Am. J. Geriatr. Psychiatry 2006, 14, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Magee, M.; Sletten, T.L.; Gordon, C.; Lovato, N.; Ambani, K.; Bartlett, D.J.; Kennaway, D.J.; Lack, L.C.; Grunstein, R.R.; et al. Light-based methods for predicting circadian phase in delayed sleep-wake phase disorder. Sci. Rep. 2021, 11, 10878. [Google Scholar] [CrossRef]
- Jou, J.H. Embracing Darkness; Business Weekly Publications: Taipei, Taiwan, 2021. [Google Scholar]
- Deboer, T. Sleep Homeostasis and the Circadian Clock: Do the Circadian Pacemaker and the Sleep Homeostat Influence Each Other’s Functioning? Neurobiol. Sleep Circadian Rhythm. 2018, 5, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, E.J.; Joyce, D.S.; Rissman, A.J.; Burgess, H.J.; Colwell, C.S.; Lack, L.C.; Gradisar, M. Electric Lighting, Adolescent Sleep and Circadian Outcomes, and Recommendations for Improving Light Health. Sleep Med. Rev. 2022, 64, 101667. [Google Scholar] [CrossRef]
- Montaruli, A.; Castelli, L.; Mulè, A.; Scurati, R.; Esposito, F.; Galasso, L.; Roveda, E. Biological Rhythm and Chronotype: New Perspectives in Health. Biomolecules 2021, 11, 487. [Google Scholar] [CrossRef]
- Chellappa, S.L. Individual Differences in Light Sensitivity Affect Sleep and Circadian Rhythms. Sleep 2021, 44, zsaa214. [Google Scholar] [CrossRef]
- Wirz-Justice, A.; Benedetti, F. Perspectives in Affective Disorders: Clocks and Sleep. Eur. J. Neurosci. 2020, 51, 346–365. [Google Scholar] [CrossRef]
- Boudreau, P.; Yeh, W.H.; Dumont, G.A.; Boivin, D.B. Circadian Variation of Heart Rate Variability across Sleep Stages. Sleep 2013, 36, 1919–1928. [Google Scholar] [CrossRef] [Green Version]
- McCurry, S.M.; Pike, K.C.; Vitiello, M.V.; Logsdon, R.G.; Larson, E.B.; Teri, L. Increasing Walking and Bright Light Exposure to Improve Sleep in Community-Dwelling Persons with Alzheimer’s Disease: Results of a Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2011, 59, 1393–1402. [Google Scholar] [CrossRef]
- Oldham, M.A.; Ciraulo, D.A. Bright Light Therapy for Depression: A Review of Its Effects on Chronobiology and the Autonomic Nervous System. Chronobiol. Int. 2014, 31, 305–319. [Google Scholar] [CrossRef]
- Freeman, M.Z.; Cannizzaro, D.N.; Naughton, L.F.; Bove, C. Fluoroquinolones-Associated Disability: It Is Not All in Your Head. NeuroSci 2021, 2, 235–253. [Google Scholar] [CrossRef]
- Nicolini, P.; Mari, D.; Abbate, C.; Inglese, S.; Bertagnoli, L.; Tomasini, E.; Rossi, P.D.; Lombardi, F. Autonomic Function in Amnestic and Nonamnestic Mild Cognitive Impairment: Spectral Heart Rate Variability Analysis Provides Evidence for a Brain-Heart Axis. Sci. Rep. 2020, 10, 11661. [Google Scholar] [CrossRef] [PubMed]
- Forte, G.; Favieri, F.; Casagrande, M. Heart Rate Variability and Cognitive Function: A Systematic Review. Front. Neurosci. 2019, 13, 710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, S.D.; Hoyos, C.M.; Phillips, C.L.; McKinnon, A.C.; Palmer, J.R.; Duffy, S.L.; Mowszowski, L.; Lin, P.; Gordon, C.J.; Naismith, S.L. Left Amygdala Volume Moderates the Relationship between Nocturnal High-Frequency Heart Rate Variability and Verbal Memory Retention in Older Adults with Amnestic Mild Cognitive Impairment: Biomarkers (Non-neuroimaging)/Novel Biomarkers. Alzheimers Dement. 2020, 16, e044608. [Google Scholar] [CrossRef]
- MacDonald, K.J.; Cote, K.A. Contributions of Postlearning REM and NREM Sleep to Memory Retrieval. Sleep Med. Rev. 2021, 59, 101453. [Google Scholar] [CrossRef]
- Walker, M.P. The Role of Slow Wave Sleep in Memory Processing. J. Clin. Sleep Med. 2009, 5 (Suppl. 34), S20–S26. [Google Scholar] [CrossRef] [Green Version]
- Cordone, S.; Annarumma, L.; Rossini, P.M.; De Gennaro, L. Sleep and β-Amyloid Deposition in Alzheimer Disease: Insights on Mechanisms and Possible Innovative Treatments. Front. Pharmacol. 2019, 10, 695. [Google Scholar] [CrossRef] [Green Version]
- Kuo, T.B.J.; Lai, C.T.; Chen, C.Y.; Lee, G.S.; Yang, C.C.H. Unstable Sleep and Higher Sympathetic Activity during Late-Sleep Periods of Rats: Implication for Late-Sleep-Related Higher Cardiovascular Events. J. Sleep Res. 2013, 22, 108–118. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Time | Treatment Group (n = 16) | Control Group (n = 11) | Chi-Square Test | Time | Treatment Group (n = 14) | Control Group (n = 8) | Chi-SquareTest | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | χ2 | p | n | (%) | n | (%) | χ2 | p | |||
| Educational level | Baseline | 2.52 | 0.47 | Posttest 1 | 0.55 | 0.90 | ||||||||
| 1. Literate | 6 | (37.5) | 2 | (18.2) | 5 | (35.7) | 2 | (25.0) | ||||||
| 2. Elementary School (≤6 years) | 5 | (31.3) | 3 | (27.2) | 4 | (28.6) | 2 | (25.0) | ||||||
| 3. Junior high school (7–9 years) | 3 | (18.7) | 2 | (18.2) | 3 | (21.4) | 2 | (25.0) | ||||||
| 4. Senior high school or college (10–12 years) | 2 | (12.5) | 4 | (36.4) | 2 | (14.3) | 2 | (25.0) | ||||||
| Marital status | 2.18 | 0.33 | 1.62 | 0.43 | ||||||||||
| 1. Unmarried | 2 | (12.5) | 0 | (0.0) | 2 | (14.3) | 0 | (0.0) | ||||||
| 2. Married | 3 | (18.8) | 4 | (36.4) | 3 | (21.4) | 3 | (37.5) | ||||||
| 3. Widowed | 11 | (68.7) | 7 | (63.6) | 9 | (64.3) | 5 | (62.5) | ||||||
| Dementia type | 6.80 | 0.079 | 0.73 | 0.69 | ||||||||||
| 1. Alzheimer | 14 | (87.4) | 10 | (90.9) | 12 | (85.8) | 7 | (87.5) | ||||||
| 2. Vascular dementia | 1 | (6.3) | 1 | (9.1) | 1 | (7.1) | 1 | (12.5) | ||||||
| 3. Frontotemporal lobe | 1 | (6.3) | 0 | (0.0) | 1 | (7.1) | 0 | (0.0) | ||||||
| Severity of dementia | 1.08 | 0.58 | 0.10 | 0.94 | ||||||||||
| 1. Mild | 3 | (18.8) | 4 | (36.4) | 6 | (42.8) | 4 | (50.0) | ||||||
| 2. Moderate | 8 | (50.0) | 4 | (36.4) | 4 | (28.6) | 2 | (25.0) | ||||||
| 3. Severe | 5 | (31.2) | 3 | (27.2) | 4 | (28.6) | 2 | (25.2) | ||||||
| Source | 1.16 | 0.28 | 2.16 | 0.14 | ||||||||||
| 1. Community | 10 | (62.5) | 9 | (81.8) | 8 | (57.1) | 8 | (87.5) | ||||||
| 2. Nursing home | 6 | (37.5) | 2 | (18.2) | 6 | (42.9) | 1 | (12.5) | ||||||
| Step | HF a Mean/SE | Roy’s Largest Root h/t i | LF% b Mean/SE | Roy’s Largest Root h/t i | LF/HF c Mean/SE | Roy’s Largest root h/t i | MMSE Score d Mean/SE | Wald χ2 j /t i | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Exp e | Con f | Diff g | p Value | Exp e | Con f | Diff g | p Value | Exp e | Con f | Diff g | p Value | Exp e | Con f | Diff g | p Value | |
| Week 0 k | 3.9 0.48 | 4.2 0.67 | −0.3 | 0.54 i | 47.0 3.91 | 52.9 5.40 | −5.9 | −0.98 i | 4.8 0.20 | 4.8 0.25 | 0.0 | −0.87 i | 13.80 1.66 | 18.25 2.09 | −4.45 | 1.38 i |
| 0.59 | 0.33 | 0.38 | 0.41 | |||||||||||||
| Week 5 l | 5.2 0.50 | 4.2 0.58 | 1.0 | 35.3 3.91 | 41.4 4.71 | −6.1 | 4.2 0.21 | 4.3 0.21 | −0.1 | 17.71 1.65 | 17.75 2.39 | −0.04 | ||||
| Group m | 4.7 0.31 | 4.2 0.38 | 0.5 | 1.49 h | 39.3 3.78 | 45.1 4.36 | −5.1 | 2.9 h | 4.5 0.13 | 4.6 0.13 | −0.1 | 1.63 h | 16.97 | 18.47 | −1.50 | −4.45 j |
| 0.21 | 0.25 | 0.16 | 0.09 | |||||||||||||
| Group × time n | 1.62 h | 0.25 h | 0.24 h | 4.41 j | ||||||||||||
| 0.001 *** | 0.31 | 0.16 | 0.001 *** | |||||||||||||
| Group × HRV × Cognitive function o | 1.41 h | 0.31 h | 0.16 h | |||||||||||||
| 0.001 *** | 0.20 | 0.34 | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-R.; Kuo, T.B.J.; Jou, J.-H.; Lai, C.-T.L.; Chang, Y.-K.; Liou, Y.M. Bright Morning Lighting Enhancing Parasympathetic Activity at Night: A Pilot Study on Elderly Female Patients with Dementia without a Pacemaker. Healthcare 2023, 11, 793. https://doi.org/10.3390/healthcare11060793
Liu C-R, Kuo TBJ, Jou J-H, Lai C-TL, Chang Y-K, Liou YM. Bright Morning Lighting Enhancing Parasympathetic Activity at Night: A Pilot Study on Elderly Female Patients with Dementia without a Pacemaker. Healthcare. 2023; 11(6):793. https://doi.org/10.3390/healthcare11060793
Chicago/Turabian StyleLiu, Chuen-Ru, Terry B. J. Kuo, Jwo-Huei Jou, Chun-Ting Lai Lai, Yu-Kai Chang, and Yiing Mei Liou. 2023. "Bright Morning Lighting Enhancing Parasympathetic Activity at Night: A Pilot Study on Elderly Female Patients with Dementia without a Pacemaker" Healthcare 11, no. 6: 793. https://doi.org/10.3390/healthcare11060793