
Socioeconomic Status and Quality of Life: An Assessment of the Mediating Effect of Social Capital
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Socioeconomic Status
2.1.2. Quality of Life
2.1.3. Social Capital
2.1.4. Sociodemographic
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larnyo, E.; Dai, B.; Nutakor, J.A.; Ampon-Wireko, S.; Larnyo, A.; Appiah, R. Examining the impact of socioeconomic status, demographic characteristics, lifestyle and other risk factors on adults’ cognitive functioning in developing countries: An analysis of five selected WHO SAGE Wave 1 Countries. Int. J. Equity Health 2022, 21, 1–20. [Google Scholar] [CrossRef]
- Christian, A.K.; Sanuade, O.A.; Okyere, M.A.; Adjaye-Gbewonyo, K. Social capital is associated with improved subjective well-being of older adults with chronic non-communicable disease in six low-and middle-income countries. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Baum, F. The New Public Health/Fran Baum; Oxford University Press: New York, NY, USA, 2016. [Google Scholar]
- Bwalya, J.C.; Sukumar, P. The Relationship between Social Capital and Children’s Health Behaviour in Ireland. 2019. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3418320 (accessed on 12 March 2022).
- Addae, E.A. The mediating role of social capital in the relationship between socioeconomic status and adolescent wellbeing: Evidence from Ghana. BMC Public Health 2020, 20, 20. [Google Scholar] [CrossRef] [PubMed]
- Putnam, R.D. Bowling Alone: The Collapse and Revival of American Community; Simon and Schuster: New York, NY, USA, 2000. [Google Scholar]
- Bourdieu, P.; Richardson, J.G. Handbook of Theory and Research for the Sociology of Education. Forms Cap. 1986, 241, 258. [Google Scholar]
- Coleman, J.S. Social capital in the creation of human capital. Am. J. Sociol. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Buijs, T.; Maes, L.; Salonna, F.; Van Damme, J.; Hublet, A.; Kebza, V.; Costongs, C.; Currie, C.; De Clercq, B. The role of community social capital in the relationship between socioeconomic status and adolescent life satisfaction: Mediating or moderating? Evidence from Czech data. Int. J. Equity Health 2016, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Littlecott, H.J.; Evans, R.; Murphy, S.; Hewitt, G.; Fletcher, A. School composition, school culture and socioeconomic inequalities in young people’s health: Multi-level analysis of the Health Behaviour in School-aged Children (HBSC) survey in Wales. Br. Educ. Res. J. 2017, 43, 310–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, D.; Emeljanovas, A.; Mieziene, B.; Štefan, L.; Kawachi, I. How different contexts of social capital are associated with self-rated health among Lithuanian high-school students. Glob. Health Action 2018, 11, 1477470. [Google Scholar] [CrossRef] [Green Version]
- Alecu, A.; Helland, H.; Hjellbrekke, J.; Jarness, V. Who you know: The classed structure of social capital. Br. J. Sociol. 2022, 73, 505–535. [Google Scholar] [CrossRef]
- Kaur, M.; Chakrapani, V.; Newtonraj, A.; Lakshmi, P.V.M.; Vijin, P.P. Social capital as a mediator of the influence of socioeconomic position on health: Findings from a population-based cross-sectional study in Chandigarh, India. Indian J. Public Health. 2018, 62, 294. [Google Scholar] [PubMed]
- Cruz-Torres, C.E.; Martín Del Campo-Ríos, J. Social capital in Mexico moderates the relationship of uncertainty and cooperation during the SARS-COV-2 pandemic. J. Community Psychol. 2022, 50, 1048–1059. [Google Scholar] [CrossRef]
- Putnam, R.D. Who Killed Civic America. 1996. Available online: https://www.prospectmagazine.co.uk/magazine/whokilledcivicamerica (accessed on 28 June 2022).
- Coleman, J.S. Foundations of Social Theory; Belknap Press of Harvard University Press: Cambridge, UK, 1990. [Google Scholar]
- Ge, T. Effect of socioeconomic status on children’s psychological well-being in China: The mediating role of family social capital. J. Health Psychol. 2020, 25, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Inchley, J.; Currie, D. Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being; Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Xu, F.; Cui, W.; Xing, T.; Parkinson, M. Family socioeconomic status and adolescent depressive symptoms in a Chinese low–and middle–income sample: The indirect effects of maternal care and adolescent sense of coherence. Front. Psychol. 2019, 10, 819. [Google Scholar] [CrossRef] [PubMed]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Nutakor, J.A.; Dai, B.; Gavu, A.K.; Antwi, O.-A. Relationship between chronic diseases and sleep duration among older adults in Ghana. Qual. Life Res. 2020, 29, 2101–2110. [Google Scholar] [CrossRef] [PubMed]
- Nutakor, J.A.; Dai, B.; Zhou, J.; Larnyo, E.; Gavu, A.K.; Asare, M.K. Association between socioeconomic status and cognitive functioning among older adults in Ghana. Int. J. Geriatr. Psychiatry 2021, 36, 756–765. [Google Scholar] [CrossRef]
- Dai, B.; Nutakor, J.A.; Zhou, J.; Larnyo, E.; Asare, M.K.; Danso, N.A.A. Association between socioeconomic status and physical functioning among older adults in Ghana. J. Public Health 2022, 30, 1411–1420. [Google Scholar] [CrossRef]
- Luo, M.; Ding, D.; Bauman, A.; Negin, J.; Phongsavan, P. Social engagement pattern, health behaviors and subjective well-being of older adults: An international perspective using WHO-SAGE survey data. BMC Public Health 2020, 20, 99. [Google Scholar] [CrossRef]
- Da Rocha, N.S.; Power, M.J.; Bushnell, D.M.; Fleck, M.P. The EUROHIS-QOL 8-item index: Comparative psychometric properties to its parent WHOQOL-BREF. Value Health J. Int. Soc Pharm. Outcomes Res. 2012, 15, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Kennedy, B.P.; Lochner, K.; Prothrow-Stith, D. Social capital, income inequality, and mortality. Am. J. Public Health. 1997, 87, 1491–1498. [Google Scholar] [CrossRef] [Green Version]
- World Helath Organization. A Conceptual Framework for Action on the Social Determinants of Health. 2010. Available online: https://apps.who.int/iris/handle/10665/44489 (accessed on 12 June 2022).
- Uphoff, E.P.; Pickett, K.E.; Cabieses, B.; Small, N.; Wright, J. A systematic review of the relationships between social capital and socioeconomic inequalities in health: A contribution to understanding the psychosocial pathway of health inequalities. Int. J. Equity Health 2013, 12, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129 (Suppl. S2), 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpiano, R.M. Toward a neighborhood resource-based theory of social capital for health: Can Bourdieu and sociology help? Soc. Sci Med. 2006, 62, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Snelgrove, J.W.; Pikhart, H.; Stafford, M. A multilevel analysis of social capital and self-rated health: Evidence from the British Household Panel Survey. Soc. Sci. Med. 2009, 68, 1993–2001. [Google Scholar] [CrossRef]
- Kim, D.; Subramanian, S.V.; Kawachi, I. Social capital and physical health: A systematic review of the literature. In Social Capital and Health; Springer: New York, NY, USA, 2008; pp. 139–190. [Google Scholar]
- Ladin, K.; Wang, R.; Fleishman, A.; Boger, M.; Rodrigue, J.R. Does social capital explain community-level differences in organ donor designation? Milbank Q. 2015, 93, 609–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Wang, S.; Chen, L.; Luo, M.; Xue, L.; Cui, D.; Mao, Z. Socioeconomic status, social capital, health risk behaviors, and health-related quality of life among Chinese older adults. Health Qual. Life Outcomes 2020, 18, 291. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; Yang, S.; Liu, X.; Ren, X.; Liu, D.; Li, N. Association between social capital and quality of life among urban residents in less developed cities of western China: A cross-sectional study. Medicine 2018, 97, e9656. [Google Scholar] [CrossRef]
- Zhang, J.; Hong, L.; Ma, G. Socioeconomic Status, Peer Social Capital, and Quality of Life of High School Students During COVID-19: A Mediation Analysis. Appl. Res. Qual. Life 2022, 17, 3005–3021. [Google Scholar] [CrossRef]
- Wang, J.; Geng, L. Effects of socioeconomic status on physical and psychological health: Lifestyle as a mediator. Int. J. Environ. Res. Public Health. 2019, 16, 281. [Google Scholar] [CrossRef] [Green Version]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef]
- Daniel, H.; Bornstein, S.S.; Kane, G.C. Addressing Social Determinants to Improve Patient Care and Promote Health Equity: An American College of Physicians Position Paper. Ann. Intern. Med. 2018, 168, 577–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhammad, T.; Kumar, P.; Srivastava, S. How socioeconomic status, social capital and functional independence are associated with subjective wellbeing among older Indian adults? A structural equation modeling analysis. BMC Public Health 2022, 22, 1836. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Kong, Y.; Gao, W.; Mo, L. Effects of Socioeconomic Status, Parent–Child Relationship, and Learning Motivation on Reading Ability. Front. Psychol. 2018, 9, 1297. [Google Scholar] [CrossRef]
- Al-Omoush, K.S.; Ribeiro-Navarrete, S.; Lassala, C.; Skare, M. Networking and knowledge creation: Social capital and collaborative innovation in responding to the COVID-19 crisis. J. Innov. Knowl. 2022, 7, 100181. [Google Scholar] [CrossRef]
- Sengupta, N.K.; Osborne, D.; Houkamau, C.A.; Hoverd, W.J.; Wilson, M.S.; Greaves, L.M.; West Newman, T.; Barlow, F.K.; Armstrong, G.; Robertson, A.; et al. How much happiness does money buy? Income and subjective well-being in New Zealand. N. Z. J. Psychol. 2012, 41, 21–34. [Google Scholar]
- Puntscher, S.; Hauser, C.; Walde, J.; Tappeiner, G. The impact of social capital on subjective well-being: A regional perspective. J. Happiness Stud. 2015, 16, 1231–1246. [Google Scholar] [CrossRef]
- Gu, D.; Brown, B.L.; Qiu, L. Self-perceived uselessness is associated with lower likelihood of successful aging among older adults in China. BMC Geriatr. 2016, 16, 172. [Google Scholar] [CrossRef] [Green Version]
- Green, H.; Fernandez, R.; Moxham, L.; MacPhail, C. Social capital and wellbeing among Australian adults’ during the COVID-19 pandemic: A qualitative study. BMC Public Health 2022, 22, 2406. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency n = 1792 | % |
|---|---|---|
| Gender | ||
| Male | 890 | 49.67 |
| Female | 902 | 50.33 |
| Age | ||
| 18–24 | 136 | 7.59 |
| 25–34 | 195 | 10.88 |
| 35–44 | 236 | 13.17 |
| 45–54 | 314 | 17.52 |
| 55–64 | 474 | 26.45 |
| 65–74 | 288 | 16.07 |
| 75+ | 149 | 8.31 |
| Residence | ||
| Urban | 861 | 48.05 |
| Rural | 931 | 51.95 |
| Marital status | ||
| Never married | 234 | 13.06 |
| Currently married | 1023 | 57.09 |
| Cohabiting | 43 | 2.4 |
| Separated/Divorced | 241 | 13.45 |
| Widowed | 251 | 14.01 |
| Education | ||
| Less than primary school | 426 | 23.77 |
| Primary school completed | 442 | 24.67 |
| Secondary school completed | 472 | 26.34 |
| High school completed | 357 | 19.92 |
| University/Post graduate degree completed | 95 | 5.3 |
| Income quintile | ||
| Lowest | 692 | 38.62 |
| 2 | 155 | 8.65 |
| 3 | 267 | 14.9 |
| 4 | 373 | 20.81 |
| Highest | 305 | 17.02 |
| Variable | VIF |
|---|---|
| Socioeconomic status | 1.01 |
| Social capital | 1.01 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| B | SE | t | Lower | Upper | |
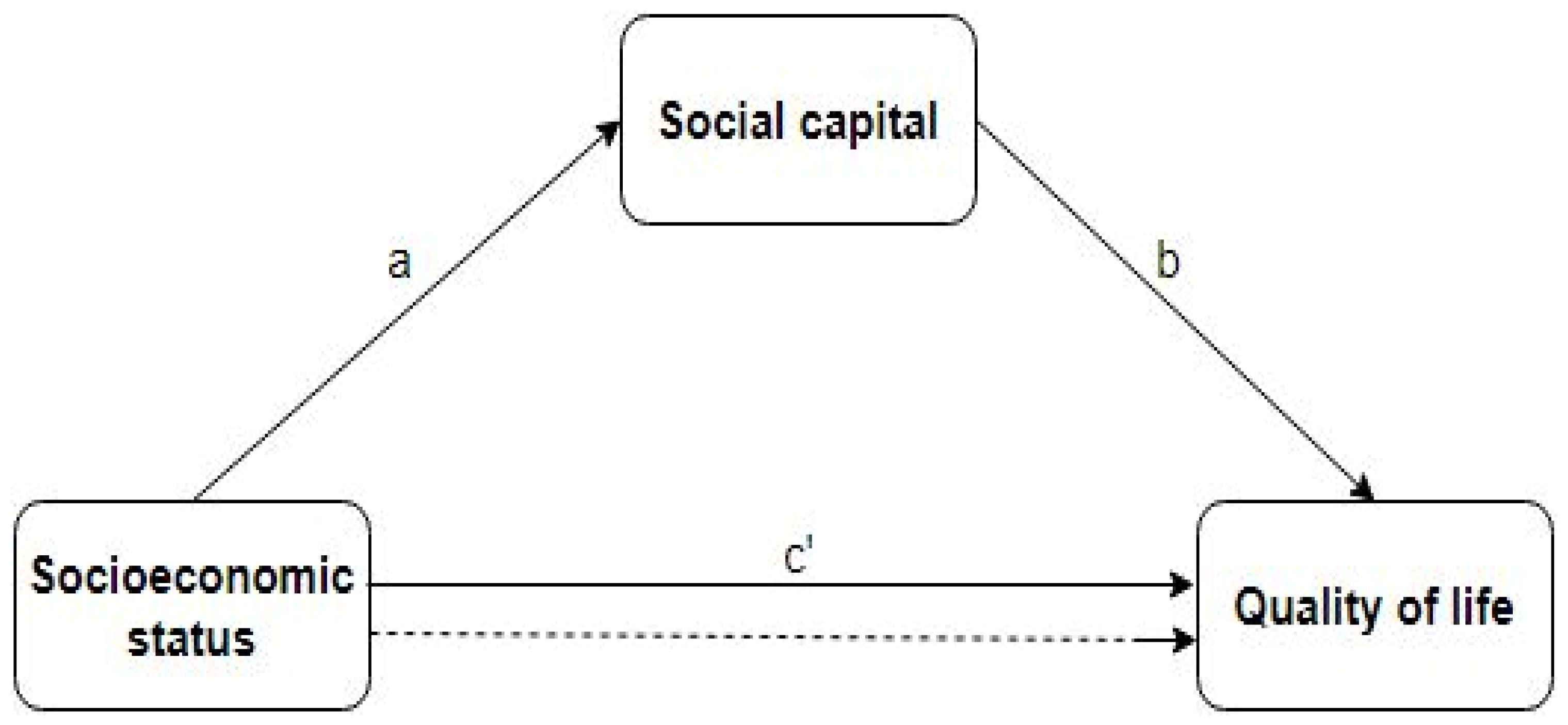
| Socioeconomic status → Quality of life | 0.21 * | 0.09 | 2.3 | 0.14 | 0.34 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| B | SE | M | Lower | Upper | |
| Social capital → Quality of life | 1.49 *** | 0.17 | 8.89 | 1.11 | 1.56 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| B | SE | t | Lower | Upper | |
| Socioeconomic status → Social capital | 0.06 *** | 0.01 | 4.55 | 0.03 | 0.08 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| B | SE | M | Lower | Upper | |
| Socioeconomic status → Social capital → Quality of life | 0.09 *** | 0.02 | 3.27 | 0.03 | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nutakor, J.A.; Zhou, L.; Larnyo, E.; Addai-Danso, S.; Tripura, D. Socioeconomic Status and Quality of Life: An Assessment of the Mediating Effect of Social Capital. Healthcare 2023, 11, 749. https://doi.org/10.3390/healthcare11050749
Nutakor JA, Zhou L, Larnyo E, Addai-Danso S, Tripura D. Socioeconomic Status and Quality of Life: An Assessment of the Mediating Effect of Social Capital. Healthcare. 2023; 11(5):749. https://doi.org/10.3390/healthcare11050749
Chicago/Turabian StyleNutakor, Jonathan Aseye, Lulin Zhou, Ebenezer Larnyo, Stephen Addai-Danso, and Debashree Tripura. 2023. "Socioeconomic Status and Quality of Life: An Assessment of the Mediating Effect of Social Capital" Healthcare 11, no. 5: 749. https://doi.org/10.3390/healthcare11050749