

Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
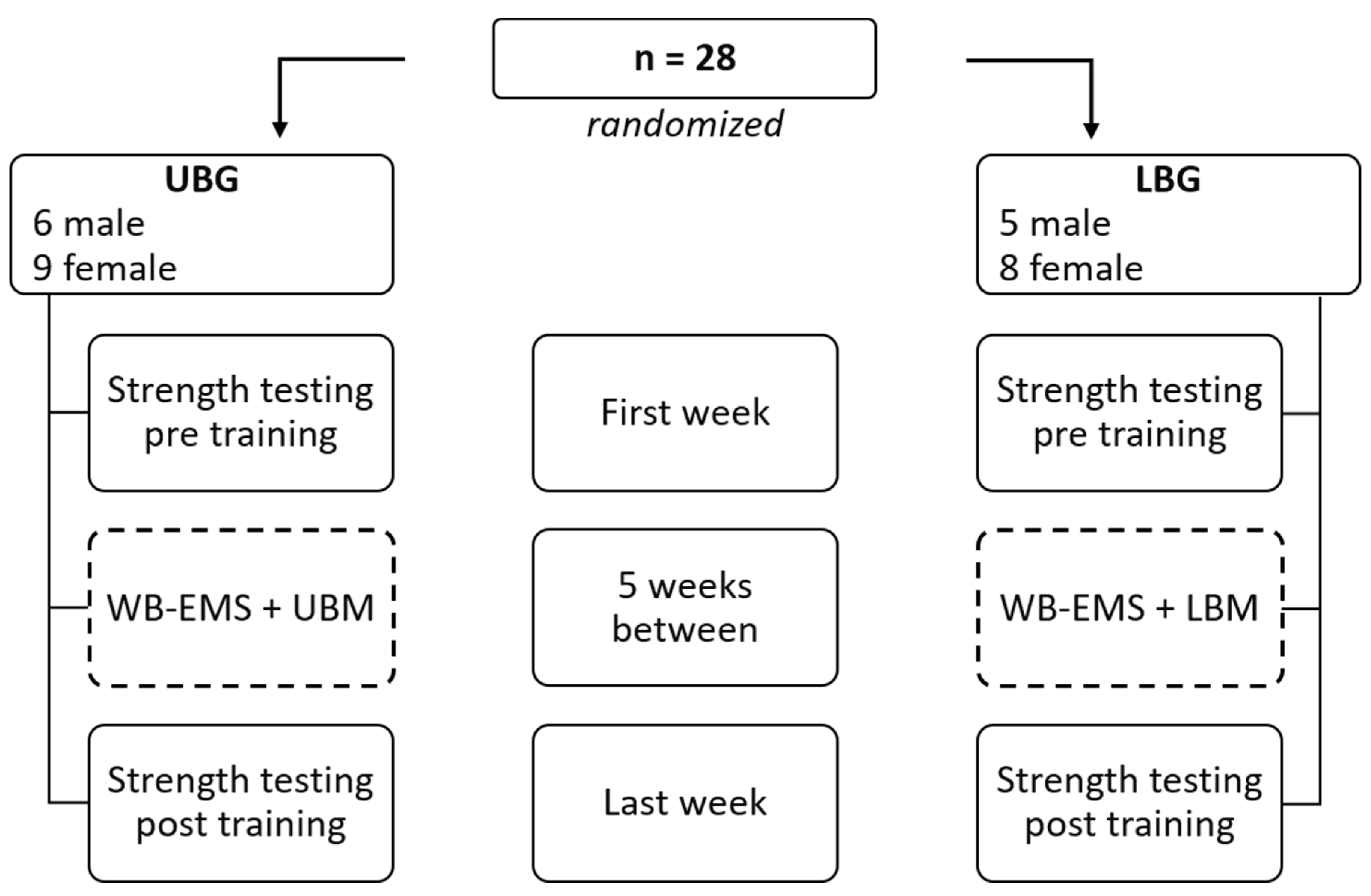
2.2. Experimental Design
2.3. WB-EMS Procedure
2.4. Exercise Procedure
2.5. Isometric Strength Testing Procedure
2.6. Statistical Analysis
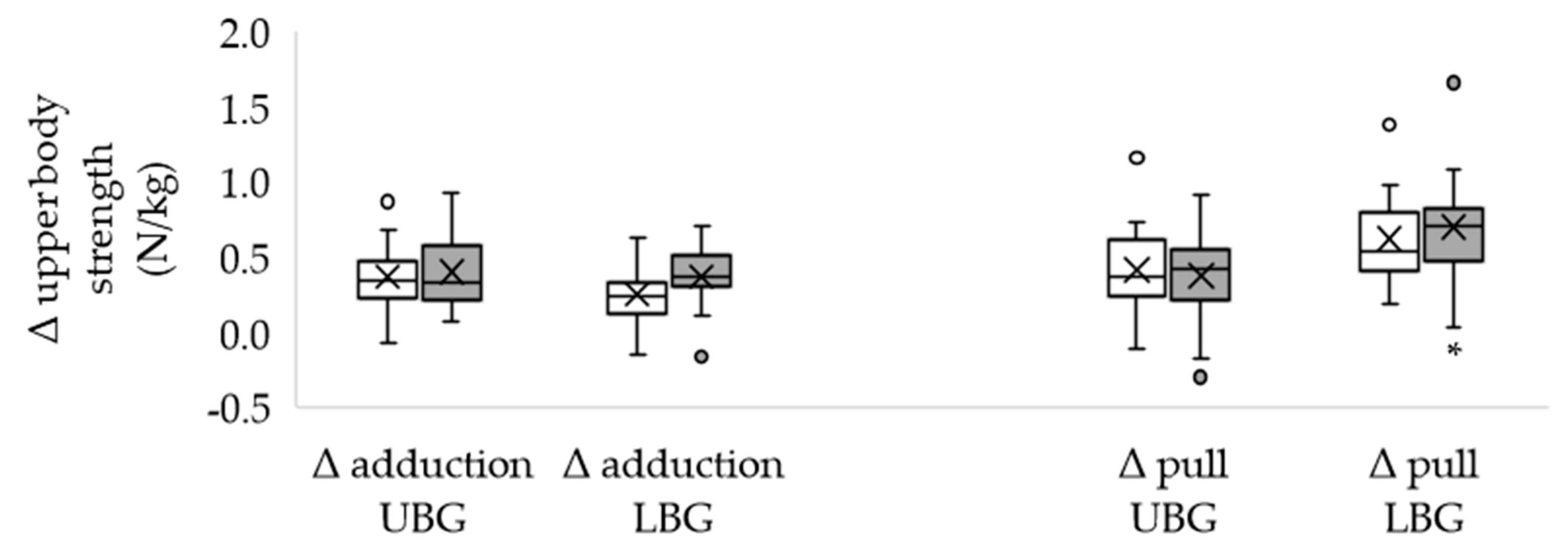
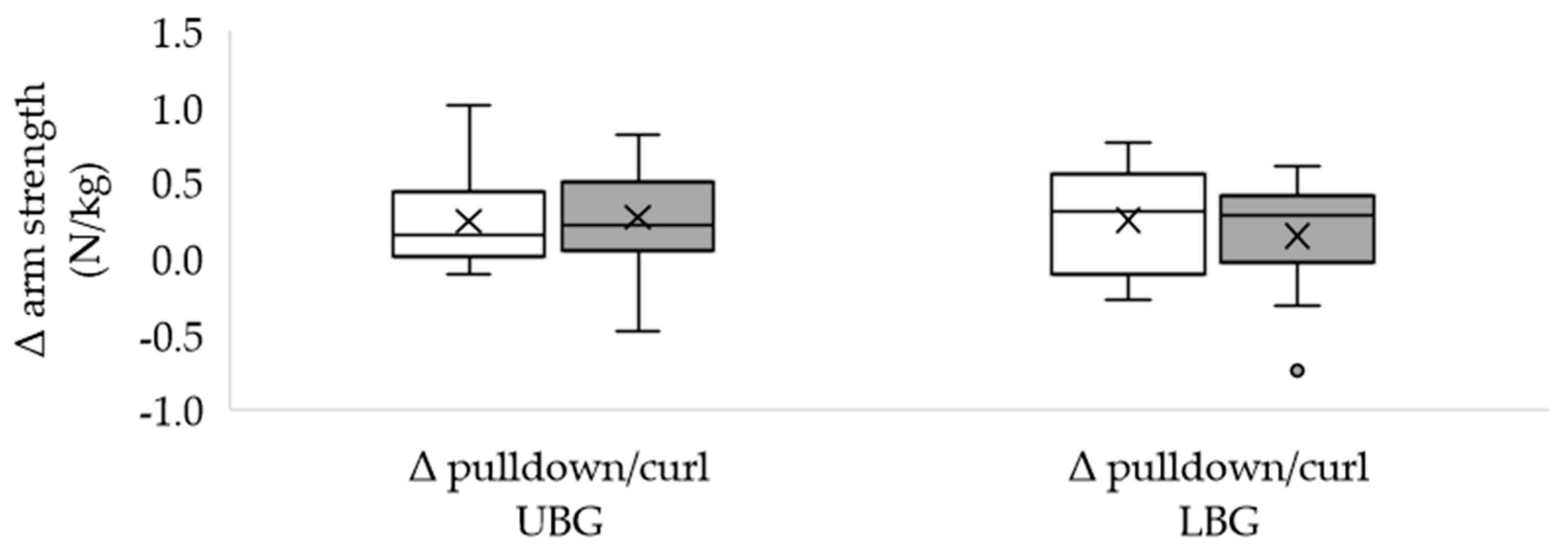
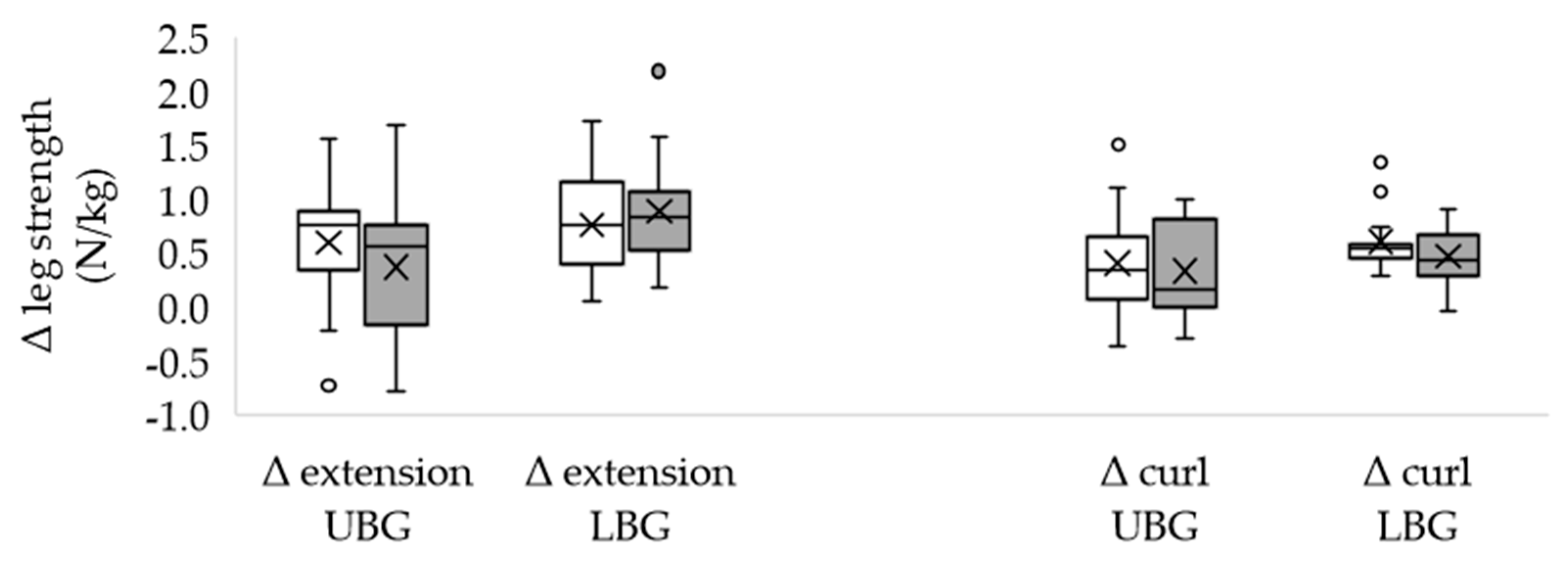
3. Results
4. Discussion
4.1. Overview
4.2. Accompanying Voluntary Activity
4.3. Training Models and Adaptations
4.4. Transferability
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berger, J.; Ludwig, O.; Becker, S.; Backfisch, M.; Kemmler, W.; Fröhlich, M. Effects of an Impulse Frequency Dependent 10-Week Whole-body Electromyostimulation Training Program on Specific Sport Performance Parameters. J. Sports Sci. Med. 2020, 19, 271–281. [Google Scholar]
- Jee, Y.S. The efficacy and safety of whole-body electromyostimulation in applying to human body: Based from graded exercise test. J. Exerc. Rehabil. 2018, 14, 49–57. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Froehlich, M.; Kohl, M.; von Stengel, S. Whole-Body Electromyostimulation Versus High Intensity (Resistance Exercise) Training—Impact on Body Composition and Strength. Dtsch. Z. Sportmed. 2015, 66, 321–327. [Google Scholar] [CrossRef]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernandez-Gonzalez, V.; Reverter-Masia, J. Effects of Whole-Body Electromyostimulation on Physical Fitness in Postmenopausal Women: A Randomized Controlled Trial. Sensors 2020, 20, 1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiorilli, G.; Quinzi, F.; Buonsenso, A.; Casazza, G.; Manni, L.; Parisi, A.; Di Costanzo, A.; Calcagno, G.; Soligo, M.; di Cagno, A. A Single Session of Whole-Body Electromyostimulation Increases Muscle Strength, Endurance and proNGF in Early Parkinson Patients. Int. J. Environ. Res. Public Health 2021, 18, 5499. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Teschler, M.; Weissenfels, A.; Bebenek, M.; von Stengel, S.; Kohl, M.; Freiberger, E.; Goisser, S.; Jakob, F.; Sieber, C.; et al. Whole-body electromyostimulation to fight sarcopenic obesity in community-dwelling older women at risk. Resultsof the randomized controlled FORMOsA-sarcopenic obesity study. Osteoporos. Int. 2016, 27, 3261–3270. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation--a systematic review of the influence of training regimens and stimulation parameters on effectiveness in electromyostimulation training of selected strength parameters. J. Strength Cond. Res. 2011, 25, 3218–3238. [Google Scholar] [CrossRef] [Green Version]
- Tiggemann, C.L.; Korzenowski, A.L.; Brentano, M.A.; Tartaruga, M.P.; Alberton, C.L.; Kruel, L.F. Perceived exertion in different strength exercise loads in sedentary, active, and trained adults. J. Strength Cond. Res. 2010, 24, 2032–2041. [Google Scholar] [CrossRef]
- Filipovic, A.; DeMarees, M.; Grau, M.; Hollinger, A.; Seeger, B.; Schiffer, T.; Bloch, W.; Gehlert, S. Superimposed Whole-Body Electrostimulation Augments Strength Adaptations and Type II Myofiber Growth in Soccer Players during a Competitive Season. Front. Physiol. 2019, 10, 1187. [Google Scholar] [CrossRef]
- Filipovic, A.; Bizjak, D.; Tomschi, F.; Bloch, W.; Grau, M. Influence of Whole-Body Electrostimulation on the Deformability of Density-Separated Red Blood Cells in Soccer Players. Front. Physiol. 2019, 10, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2021. [Google Scholar]
- Kemmler, W.; Froehlich, M.; von Stengel, S.; Kleinöder, H. Whole-Body Electromyostimulation—The Need for Common Sense! Rationale and Guideline for a Safe and Effective Training. Dtsch. Z. Sportmed. 2016, 67, 218–221. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Shojaa, M.; von Stengel, S.; Filipovic, A.; Kleinöder, H.; Berger, J.; Fröhlich, M. Efficacy and Safety of Low Frequency Whole-Body Electromyostimulation (WB-EMS) to Improve Health-Related Outcomes in Non-athletic Adults. A Systematic Review. Front. Physiol. 2018, 9, 573. [Google Scholar] [CrossRef]
- Micke, F.; Kleinöder, H.; Dörmann, U.; Wirtz, N.; Donath, L. Effects of an Eight-Week Superimposed Submaximal Dynamic Whole-Body Electromyostimulation Training on Strength and Power Parameters of the Leg Muscles: A Randomized Controlled Intervention Study. Front. Physiol. 2018, 9, 1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuhbeck, E.; Birkenmaier, C.; Schulte-Göcking, H.; Pronnet, A.; Jansson, V.; Wegener, B. The Influence of WB-EMS-Training on the Performance of Ice Hockey Players of Different Competitive Status. Front. Physiol. 2019, 10, 1136. [Google Scholar] [CrossRef]
- Ludwig, O.; Berger, J.; Schuh, T.; Backfisch, M.; Becker, S.; Fröhlich, M. Can A Superimposed Whole-Body Electromyostimulation Intervention Enhance the Effects of a 10-Week Athletic Strength Training in Youth Elite Soccer Players? J. Sports Sci. Med. 2020, 19, 535–546. [Google Scholar]
- Dörmann, U.; Wirtz, N.; Micke, F.; Morat, M.; Kleinöder, H.; Donath, L. The Effects of Superimposed Whole-Body Electromyostimulation during Short-Term Strength Training on Physical Fitness in Physically Active Females: A Randomized Controlled Trial. Front. Physiol. 2019, 10, 728. [Google Scholar] [CrossRef] [Green Version]
- Moritani, T.; deVries, H.A. Neural factors versus hypertrophy in the time course of muscle strength gain. Am. J. Phys. Med. 1979, 58, 115–130. [Google Scholar]
- Coburn, J.W.; Housh, T.J.; Malek, M.H.; Weir, J.P.; Cramer, J.T.; Beck, T.W.; Johnson, G.O. Neuromuscular responses to three days of velocity-specific isokinetic training. J. Strength Cond. Res. 2006, 20, 892–898. [Google Scholar] [CrossRef]
- Elgueta-Cancino, E.; Evans, E.; Martinez-Valdes, E.; Falla, D. The Effect of Resistance Training on Motor Unit Firing Properties: A Systematic Review and Meta-Analysis. Front. Physiol. 2022, 13, 817631. [Google Scholar] [CrossRef]
- Natsume, T.; Ozaki, H.; Kakigi, R.; Kobayashi, H.; Naito, H. Effects of training intensity in electromyostimulation on human skeletal muscle. Eur. J. Appl. Physiol. 2018, 118, 1339–1347. [Google Scholar] [CrossRef] [PubMed]
- Hortobágyi, T.; Maffiuletti, N.A. Neural adaptations to electrical stimulation strength training. Eur. J. Appl. Physiol. 2011, 111, 2439–2449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues-Santana, L.; Adsuar, J.C.; Denche-Zamorano, Á.; Vega-Muñoz, A.; Salazar-Sepúlveda, G.; Contreras-Barraza, N.; Galán-Arroyo, C.; Louro, H. Bibliometric Analysis of Studies on Whole Body Electromyostimulation. Biology 2022, 11, 1205. [Google Scholar] [CrossRef]
- von Stengel, S.; Kemmler, W. Trainability of leg strength by whole-body electromyostimulation during adult lifespan: A study with male cohorts. Clin. Interv. Aging 2018, 13, 2495–2502. [Google Scholar] [CrossRef] [Green Version]
- Reljic, D.; Konturek, P.C.; Herrmann, H.J.; Neurath, M.F.; Zopf, Y. Effects of whole-body electromyostimulation exercise and caloric restriction on cardiometabolic risk profile and muscle strength in obese women with the metabolic syndrome: A pilot study. J. Physiol. Pharmacol. 2020, 71, 89–98. [Google Scholar] [CrossRef]
- Evangelista, A.L.; Teixeira, C.V.S.; Barros, B.M.; de Azevedo, J.B.; Paunksnis, M.R.R.; Souza, C.R.; Wadhi, T.; Rica, R.L.; Braz, T.V.; Bocalini, D.S. Does whole-body electrical muscle stimulation combined with strength training promote morphofunctional alterations? Clinics 2019, 74, e1334. [Google Scholar] [CrossRef] [Green Version]
- Wirtz, N.; Zinner, C.; Doermann, U.; Kleinoeder, H.; Mester, J. Effects of Loaded Squat Exercise with and without Application of Superimposed EMS on Physical Performance. J. Sports Sci. Med. 2016, 15, 26–33. [Google Scholar]
- Kemmler, W.; Teschler, M.; von Stengel, S. Role of whole body-electromyostimulation—“A series of studies”. Osteologie 2015, 24, 20–29. [Google Scholar] [CrossRef]
- Kemmler, W.; Weissenfels, A.; Willert, S.; Fröhlich, M.; Ludwig, O.; Berger, J.; Zart, S.; Becker, S.; Backfisch, M.; Kleinöder, H.; et al. Recommended Contraindications for the Use of Non-Medical WB-Electromyostimulation. Dtsch. Z. Sportmed. 2019, 70, 278–282. [Google Scholar] [CrossRef]
- Stöllberger, C.; Finsterer, J. Side effects of and contraindications for whole-body electro-myo-stimulation: A viewpoint. BMJ Open Sport Exerc. Med. 2019, 5, e000619. [Google Scholar] [CrossRef]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Expert. Rev. Cardiovasc. Ther. 2019, 17, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Runkel, B.; Kappelhoff, M.; Hilberg, T. Complex strength performance in patients with haemophilia A. Method development and testing. Hamostaseologie 2015, 35 (Suppl. S1), S12–S17. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, M.; Tomczak, E. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trends Sport Sci. 2014, 1, 19–25. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Erlbaum: Hillsdals, NJ, USA, 1988; Volume 2. [Google Scholar]
- Hughes, D.C.; Ellefsen, S.; Baar, K. Adaptations to Endurance and Strength Training. Cold Spring Harb. Perspect. Med. 2018, 8, a029769. [Google Scholar] [CrossRef]
- Maffiuletti, N.A. Physiological and methodological considerations for the use of neuromuscular electrical stimulation. Eur. J. Appl. Physiol. 2010, 110, 223–234. [Google Scholar] [CrossRef]
- Martínez-Cava, A.; Hernández-Belmonte, A.; Courel-Ibáñez, J.; Morán-Navarro, R.; González-Badillo, J.J.; Pallarés, J.G. Bench Press at Full Range of Motion Produces Greater Neuromuscular Adaptations Than Partial Executions after Prolonged Resistance Training. J. Strength Cond. Res. 2022, 36, 10–15. [Google Scholar] [CrossRef]
- Pallarés, J.G.; Cava, A.M.; Courel-Ibáñez, J.; González-Badillo, J.J.; Morán-Navarro, R. Full squat produces greater neuromuscular and functional adaptations and lower pain than partial squats after prolonged resistance training. Eur. J. Sport Sci. 2020, 20, 115–124. [Google Scholar] [CrossRef]
- Omoto, M.; Matsuse, H.; Hashida, R.; Takano, Y.; Yamada, S.; Ohshima, H.; Tagawa, Y.; Shiba, N. Cycling Exercise with Electrical Stimulation of Antagonist Muscles Increases Plasma Growth Hormone and IL-6. Tohoku J. Exp. Med. 2015, 237, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Masayuki, O.; Matsuse, H.; Takano, Y.; Yamada, S.; Ohshima, H.; Tagawa, Y.; Shiba, N. Oxygen Uptake during Aerobic Cycling Exercise Simultaneously Combined with Neuromuscular Electrical Stimulation of Antagonists. J. Nov. Physiother. 2013, 3, 185. [Google Scholar] [CrossRef] [Green Version]
- Paillard, T. Training Based on Electrical Stimulation Superimposed Onto Voluntary Contraction Would be Relevant Only as Part of Submaximal Contractions in Healthy Subjects. Front. Physiol 2018, 9, 1428. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, P.; Zhou, S.; Crowley, Z.; Brooks, L.; Hooper, A. Effects of unilateral electromyostimulation superimposed on voluntary training on strength and cross-sectional area. Muscle Nerve 2009, 40, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Deley, G.; Cometti, C.; Fatnassi, A.; Paizis, C.; Babault, N. Effects of combined electromyostimulation and gymnastics training in prepubertal girls. J. Strength Cond. Res. 2011, 25, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Adams, V. Electromyostimulation to fight atrophy and to build muscle: Facts and numbers. J. Cachexia Sarcopenia Muscle 2018, 9, 631–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filipovic, A.; Kleinöder, H.; Plück, D.; Hollmann, W.; Bloch, W.; Grau, M. Influence of Whole-Body Electrostimulation on Human Red Blood Cell Deformability. J. Strength Cond. Res. 2015, 29, 2570–2578. [Google Scholar] [CrossRef] [Green Version]
- Filipovic, A.; Grau, M.; Kleinöder, H.; Zimmer, P.; Hollmann, W.; Bloch, W. Effects of a Whole-Body Electrostimulation Program on Strength, Sprinting, Jumping, and Kicking Capacity in Elite Soccer Players. J. Sports Sci. Med. 2016, 15, 639–648. [Google Scholar]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation--a systematic review of the effects of different electromyostimulation methods on selected strength parameters in trained and elite athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef] [Green Version]
- Kemmler, W.; Teschler, M.; Bebenek, M.; von Stengel, S. [(Very) high Creatinkinase concentration after exertional whole-body electromyostimulation application: Health risks and longitudinal adaptations]. Wien. Med. Wochenschr. 2015, 165, 427–435. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (m 11; f 17) | UBG (m 6; f 9) | LBG (m 5; f 8) | |
|---|---|---|---|
| Age [years] | 28 (20–36) | 32 (25–36) | 26 (20–35) |
| Height [cm] | 173.0 (159–186) | 174.0 (159.0–186.0) | 171.0 (160.0–186.0) |
| Body mass pre [kg] | 74.1 (47.4–114.3) | 78.3 (53.1–114.3) | 67.2 (47.4–100.3) |
| Body mass post [kg] | 74.4 (48.0–112.9) | 78.2 (52.8–112.9) | 68.0 (48.0–99.7) |
| BMI pre [kg/m2] | 25.33 (18.21–40.98) | 25.68 (19.27–40.98) | 23.88 (18.21–30.35) |
| BMI post [kg/m2] | 25.06 (18.08–38.57) | 25.63 (19.16–38.57) | 23.74 (18.08–30.65) |
| Number of sessions | 5 (3–6) | 5 (3–6) | 5 (3–6) |
| Test Position | Strength (N) Initial | Strength (N) Final | Significance | Effect Size r |
|---|---|---|---|---|
| Arm adduction right | 83.3 (44.8–143.0) | 116.2 (42.6–178.3) | 0.002 ** | 0.81 |
| Arm adduction left | 83.0 (44.8–124.4) | 124.4 (54.2–196.0) | <0.001 ** | 0.88 |
| Arm pull right | 173.0 (117.0–293.7) | 232.6 (124.7–331.6) | 0.001 ** | 0.84 |
| Arm pull left | 196.0 (114.1–331.7) | 242.2 (132.4–378.3) | 0.006 ** | 0.70 |
| Triceps pulldown | 253.0 (142.7–461.2) | 279.2 (149.6–510.4) | 0.012 * | 0.65 |
| Biceps curl | 308.5 (117.6–512.7) | 331.7 (143.6–528.2) | 0.008 ** | 0.69 |
| Leg extension right | 377.2 (196.7–697.4) | 404.8 (237.4–766.0) | 0.015 * | 0.63 |
| Leg extension left | 373.4 (130.9–682.5) | 403.3 (218.6–769.0) | 0.100 | 0.43 |
| Leg curl right | 184.6 (40.9–296.1) | 200.1 (71.2–447.5) | 0.005 ** | 0.72 |
| Leg curl left | 185.5 (48.0–296.5) | 186.9 (85.5–396.0) | 0.031 * | 0.56 |
| Test Position | Strength (N) Initial | Strength (N) Final | Significance | Effect Size r |
|---|---|---|---|---|
| Arm adduction right | 61.7 (28.8–127.4) | 84.9 (43.1–155.5) | 0.007 ** | 0.75 |
| Arm adduction left | 56.2 (29.0–111.3) | 85.1 (46.1–170.0) | 0.002 ** | 0.84 |
| Arm pull right | 140.0 (80.9–281.7) | 170.4 (145.0–362.2) | 0.001 ** | 0.88 |
| Arm pull left | 131.0 (94.9–216.8) | 167.9 (136.8–378.2) | 0.001 ** | 0.88 |
| Triceps pulldown | 178.0 (125.0–474.0) | 203.0 (140.2–474.2) | 0.039 * | 0.57 |
| Biceps curl | 215.3 (137.0–559.5) | 212.7 (167.9–531.0) | 0.221 | 0.34 |
| Leg extension right | 330.5 (218.2–725.0) | 385.6 (281.0–787.8) | 0.002 ** | 0.86 |
| Leg extension left | 304.0 (184.8–612.0) | 348.5 (228.1–704.9) | 0.001 ** | 0.88 |
| Leg curl right | 139.4 (104.6–268.7) | 170.0 (140.0–311.9) | 0.001 ** | 0.88 |
| Leg curl left | 127.0 (105.0–261.4) | 166.2 (132.0–287.9) | 0.002 ** | 0.86 |
| Test Position | Δ UBG (N) | Δ UBG (%) | Δ LBG (N) | Δ LBG (%) |
|---|---|---|---|---|
| Arm adduction right | 26.5 (−11.9–68.3) | 137.01 (83.43–175.63) | 12.6 (−13.9–44.3) | 120.68 (86.47–222.92) |
| Arm adduction left | 27.5 (5.6–83.3) | 131.70 (104.61–183.05) | 29.1 (−15.2–58.7) | 152.74 (84.85–244.67) |
| Arm pull right | 29.4 (−6.3–85.4) | 114.74 (96.14–149.36) | 32.5 (10.4–96.1) | 128.46 (105.28–182.82) |
| Arm pull left | 21.6 (−27.2–90.2) | 115.07 (84.68–144.24) | 41.4 (4.6–164.0) | 131.67 (102.47–176.56) * |
| Triceps pulldown | 11.7 (−9.0–89.5) | 105.88 (97.20–161.89) | 19.6 (−22.5–74.5) | 110.17 (93.72–130.56) |
| Biceps curl | 24.5 (−31.3–69.4) | 107.45 (88.79–139.86) | 21.2 (−45.1–40.7) | 108.82 (88.02–122.55) |
| Leg extension right | 52.0 (−90.7–141.2) | 117.40 (86.99–125.25) | 55.1 (−4.4–130.3) | 116.67 (98.94–135.90) |
| Leg extension left | 41.8 (−94.5–120.3) | 110.05 (80.11–167.00) | 56.0 (4.7–215.7) | 121.68 (101.14–144.09) |
| Leg curl right | 30.3 (−27.8–151.4) | 117.45 (79.41–185.79) | 37.1 (15.5–126.3) | 124.87 (111.12–168.34) |
| Leg curl left | 13.9 (−27.3–99.5) | 107.42 (88.28–178.13) | 39.7 (−1.7–70.7) | 131.41 (98.79–160.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stephan, H.; Wehmeier, U.F.; Förster, T.; Tomschi, F.; Hilberg, T. Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training. Healthcare 2023, 11, 741. https://doi.org/10.3390/healthcare11050741
Stephan H, Wehmeier UF, Förster T, Tomschi F, Hilberg T. Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training. Healthcare. 2023; 11(5):741. https://doi.org/10.3390/healthcare11050741
Chicago/Turabian StyleStephan, Holger, Udo Frank Wehmeier, Tim Förster, Fabian Tomschi, and Thomas Hilberg. 2023. "Additional Active Movements Are Not Required for Strength Gains in the Untrained during Short-Term Whole-Body Electromyostimulation Training" Healthcare 11, no. 5: 741. https://doi.org/10.3390/healthcare11050741